
Abstract
Adult-acquired flatfoot deformity (AAFD) comprises a wide spectrum of ligament and tendon failure that may result in significant deformity and disability. It is often associated with posterior tibial tendon deficiency (PTTD), which has been linked to multiple demographic factors, medical comorbidities, and genetic processes. AAFD is classified using stages I through IV. Nonoperative treatment modalities should always be attempted first and often provide resolution in stages I and II. Stage II, consisting of a wide range of flexible deformities, is typically treated operatively with a combination of soft tissue procedures and osteotomies. Stage III, which is characterized by a rigid flatfoot, typically warrants triple arthrodesis. Stage IV, where the flatfoot deformity involves the ankle joint, is treated with ankle arthrodesis or ankle arthroplasty with or without deltoid ligament reconstruction along with procedures to restore alignment of the foot. There is limited evidence as to the optimal procedure; thus, the surgical indications and techniques continue to be researched.
Keywords
Adult-acquired flatfoot deformity (AAFD) comprises a wide spectrum of ligament and tendon failures, resulting in significant deformity and disability. Although there are no large-scale epidemiological studies, reported rates are >3% in women over the age of 40 years and >10% of all adults over the age of 65 years. 69,72 In adults, this deformity is commonly associated with posterior tibial tendon deficiency (PTTD). In PTTD, involvement of the posterior tibial tendon (PTT) is associated with failure of surrounding ligamentous structures and resulting bony deformity, which may be instigated by repetitive loading and degeneration, inflammatory arthropathy, acute injury, or preexisting abnormality.
Over the past 3 decades, there have been numerous advances in the treatment and surgical techniques for this complex disorder. This review aims to provide an overview of adult flatfoot deformity, including the pathophysiology, clinical evaluation, and treatment.
Pathophysiology
The PTT is a powerful plantarflexor and inverter of the hindfoot. It passes posterior and medial to the subtalar axis, acting across the transverse tarsal (talonavicular and calcaneocuboid) joints. 47 During the early stance phase of normal gait, the foot is everted, placing the transverse tarsal joints parallel to each other, creating mobility through the hindfoot. During midstance, the PTT pulls the foot into inversion, which causes the axes of the transverse tarsal joints to diverge from each other so that the hindfoot becomes rigid during late stance. 98 The rigid foot allows the Achilles tendon to be effective in propulsion.
The etiology of PTTD is most commonly attributed to a degenerative process in which the micromechanical trauma of repetitive loading leads to tendon dysfunction. 31,47,87,115 Cadaveric studies have shown that the PTT courses sharply around the medial malleolus as it inserts onto the medial and plantar foot. 115 As a result, the PTT is under increased tension at this location and is therefore susceptible to more resistance and friction. 115 This retromalleolar region is hypovascular and is vulnerable to tendinopathy and eventual rupture. 82 Once the PTT becomes insufficient, the foot is subject to the unopposed pull of the peroneus brevis, resulting in increased hindfoot valgus and abduction. 47,66 The static restraints of the medial arch—primarily the spring ligament, as well as the interosseous talocalcaneal ligament—become stretched and the vector of the gastrocnemius-soleus complex becomes altered, leading to worsening valgus deformity. 71 In later stages, the deltoid ligament may fail, causing ankle instability and talar tilt. 17
There are myriad factors implicated in the development of AAFD, although many can be conceptualized as falling into 2 broad categories: extrinsic factors that exert more physical force on the tendon and intrinsic factors that weaken the tendon and make it more susceptible to degeneration. Extrinsic factors such as obesity, foot shape, acute traumatic injury, and equinus contracture can increase the force experienced by the PTT, exposing it to more mechanical trauma. 31,47,63,87,115 In addition, preexisting deformity, such as asymptomatic flexible pes planus, accessory navicular, or valgus orientation of the subtalar joint, can also make the foot more susceptible to AAFD. 40,47,72,81,88,100 Intrinsic factors can predispose the tendon to attenuation and degeneration. PTTD may be instigated or accelerated by inflammatory disorders (such as rheumatoid arthritis or seronegative spondyloarthropathy), hypertension, diabetes mellitus, and steroid use. 40,47,63,72,81,88,100 Furthermore, polymorphisms at genes involved in collagen degradation and remodeling—such as matrix metalloproteinase (MMP)–13 and MMP-18—may play a role, although these factors are still being investigated. 29,51 The relative effect of many of these factors is still not well understood.
Finally, although AAFD is commonly linked to PTTD, there a number of other etiologies for AAFD in which patients with a normal PTT can develop AAFD. 95,114,121 Failure of the spring (calcaneonavicular) ligament has been identified as a potential cause of AAFD in patients in whom the PTT is normal based on imaging and intraoperative exploration. 95,114,121 However, details about the incidence and pathophysiology in such cases are unknown.
Evaluation
Clinical
The diagnosis of flatfoot consists of clinical and radiographic evaluation. The typical patient with AAFD is a woman with obesity in her sixth decade of life. 31 Symptomatic flatfoot is associated with elevated body mass index (BMI). 99 Patients may complain of pain along the medial foot due to tenosynovitis or deformity. 31 In more severe stages of AAFD, symptoms may include lateral pain as well. This is often attributed to talocalcaneal impingement at the angle of Gissane, fibular impingement against the calcaneus, subtalar arthritis, and peroneal tendonitis or tears due to subfibular impingement. 41 It has been proposed that the hindfoot valgus associated with flatfoot leads to talocalcaneal subluxation and narrowing of the sinus tarsi, causing abnormal bony contact and impingement. 80 The duration of symptoms, aggravating and ameliorating factors, attempted prior therapies, and functional/employment status may aid in assessing severity of disease.
Visually, the arch may appear flattened (midfoot planus) with a valgus heel. The “too many toes” sign—in which a patient viewed from behind has more than 2 toes visible lateral to the hindfoot—is indicative of forefoot abduction (Figure 1). Although the too many toes sign is not specific for flatfoot deformity, it may assist in diagnosis. 69 Patients often have tenderness and swelling posterior to the medial malleolus, but this may occur anywhere along the course of the tendon. 68,69 Later in the disease, patients may actually have less pain after the PTT has elongated or ruptured, and thus the absence of pain does not preclude the diagnosis. 119

“Too many toes” sign. When the feet are examined from behind a patient with flatfoot deformity, more toes may be visible laterally (seen on the right foot, arrow) indicating forefoot abduction. Heel valgus is also seen.
Equinus contracture or tightness of the gastrocnemius-soleus complex is typically observed. 2,37 Gastrocnemius-soleus tightness can lead to laxity and collapse in the arch and supporting structures of the midfoot, as well as forefoot abduction. 16,57,113 Equinus contracture limits ankle dorsiflexion, forcing the foot to evert and dorsiflex through the talonavicular or midfoot joints to continue the gait cycle. Normal ankle dorsiflexion is 20 degrees with the knee flexed or extended. Gastrocnemius contracture is typically revealed with a Silfverskiold test, in which ankle dorsiflexion is tested with the knee in extension and then in flexion while maintaining the hindfoot in a neutral position. 36 Dorsiflexion <10 degrees with the knee extended that corrects with the knee flexed or a difference of >10 degrees between knee flexed and extended is a criterion. Equinus in extension that corrects with knee flexion indicates gastrocnemius tightness as opposed to Achilles contracture. 119
Flexibility of the foot as well as strength and function of the PTT can be determined with a single-limb heel raise. When a normal heel raise is performed, the hindfoot inverts. However, in flatfoot, the PTT cannot invert the foot and subtalar joint in order to lock the transverse tarsal joints, and therefore they cannot function as a stable lever arm for raising the heel off the ground. 31,69 In milder forms of flatfoot, the single-limb heel raise can result in pain but the patient may still be able to invert the hindfoot, or the patient may accomplish the heel raise via the Achilles without the hindfoot inverting. The critical threshold for PTTD is the inability to invert the heel. Patients with severe arthritis, talonavicular or subtalar fusion, or Achilles tendon rupture may find it difficult to heel-raise but should be differentiated from flatfoot based on history, physical examination, and imaging. 31 In addition, the examiner should prevent the patient from pushing up from a surface with his or her hands, which can cause a false-negative test.
Flexibility of the foot deformity should also be assessed by the examiner. The examiner should test if the flatfoot deformity can be corrected through inversion at the subtalar joint and adduction at the talonavicular joint. 119 The flexibility assessment may need to be performed in plantarflexion in case of equinus contracture.
Radiographic
Weightbearing radiographs of the foot and ankle are essential. On the anteroposterior (AP) radiograph, the relationships between the talus, navicular, and first metatarsal are evaluated. The AP talo–first metatarsal angle compares the long axis of the talus to that of the first metatarsal and is elevated in flatfoot (normal, 7 degrees; flatfoot, 16 degrees). 124 The talonavicular coverage angle (normal, <15-20 degrees; flatfoot, >20 degrees) represents forefoot abduction and is formed by the lines of the articular surfaces of the talus and navicular (Figure 2). 103,122 Talar uncoverage can also be expressed by the percentage of the talus that is not in contact with the navicular medially (Figure 2). 103,122 Increased values indicate forefoot abduction, with 30% representing a clinically important threshold that may affect management. 33 The talar incongruency angle, a newer marker for forefoot abduction (normal, 6 degrees; flatfoot, >50 degrees), increases dramatically between substages of flatfoot and may guide treatment (Figure 3). 22,43

Common radiographic parameters in a stage IIb flatfoot patient measured on weightbearing anteroposterior radiograph. (A) Talonavicular coverage angle, measured as the angle between a line connecting the articular surface of the talus and a line connecting the articular surface of the navicular. (B) Talonavicular uncoverage percentage, measured as the percentage of the talar head articular surface not covered by the navicular (dashed line) over the entire extent of the talar head articular surface. (C) Talo–first metatarsal angle, which is the angle between the axis of the first metatarsal and the axis of the talus.

Talar incongruency angle. The talar incongruency angle is formed by 2 lines: a line between the most lateral point of the articular surfaces of the talus (point A) and the navicular (point B), as well as a line drawn from the lateral aspect of the talar neck at its narrowest segment (point C) to the lateral point of the talar articular surface (point A). This measurement is shown in a normal patient (left) and a flatfoot patient (right). Arrowheads point to the area of the talar head uncovered by the navicular. (Printed with permission from Ellis et al. 43 )
On the lateral radiograph, the talo–first metatarsal angle (Meary’s angle; Figure 4) should measure 0 ± 10 degrees and is elevated in flatfoot deformity (often >20 degrees, apex directed plantarly). 43,124 Arch height is frequently measured, but studies have shown that the distance between the medial cuneiform and the base of the fifth metatarsal may be more clinically useful to differentiate between normal feet (17 mm) and flatfeet (6 mm). 43,124 Calcaneal pitch is formed by the line parallel to the ground and the line along the inferior inclination axis of the calcaneus, and it is decreased in flatfoot (normal, 8 degrees; flatfoot, 4 degrees). 43,124
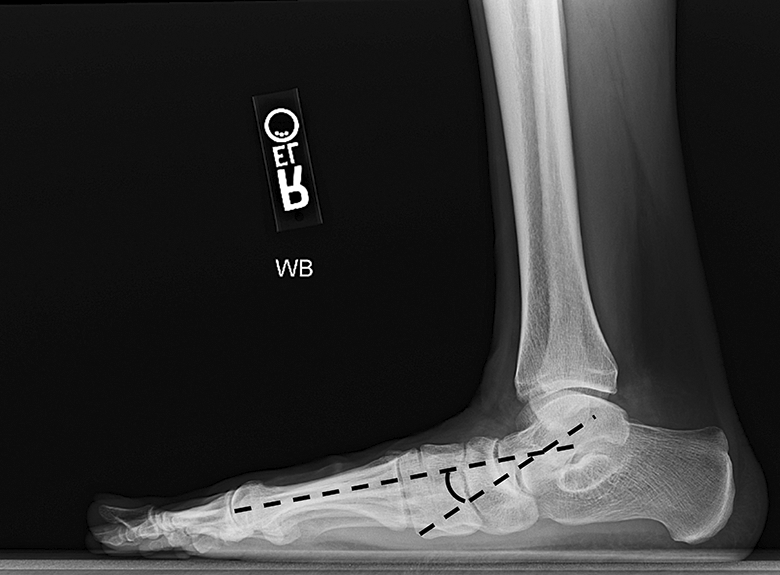
Meary’s angle, or the lateral talar–first metatarsal angle, is formed by the lines of the axis of the first metatarsal and the talus. In flatfoot, the apex of the angle is directed in the plantar direction.
Standing ankle radiographs may reveal lateral talar tilt and ankle arthritis, which can occur in the later stages of flatfoot deformity. 17,18,90 Moreover, it can be beneficial to obtain full-length radiographs of the lower extremity to rule out other causes of deformity. For example, arthritis, trauma, or deformity of the knee or tibia can affect interpretation of foot and ankle imaging.
Hindfoot alignment radiographs, most frequently Saltzman views, can quantify hindfoot valgus and guide operative planning. 101 The hindfoot moment arm is measured by the shortest distance between the midtibial axis and the most inferior portion of the calcaneus (normal, –3 mm [varus]; flatfoot, >+10 mm [valgus]). 23,64,101 The hindfoot alignment angle is formed by the intersection of the longitudinal axis of the tibial shaft and the axis of the calcaneal tuberosity (normal, 5 degrees; flatfoot, 22 degrees). 122 This angle is reliable and strongly correlates with the hindfoot moment arm, allowing for planning of intraoperative correction of hindfoot valgus (Figure 5).

The hindfoot alignment angle. The hindfoot alignment angle, as measured on Saltzman hindfoot radiographs, is formed by the intersection of the longitudinal axis of the tibial shaft and the axis of the calcaneal tuberosity. (A) Measurement in flatfoot patient; (B) measurement in a normal control. (Printed with permission from Williamson et al. 122 )
Although not universally available, multiplanar imaging modalities like weightbearing computed tomography (CT) and magnetic resonance imaging (MRI) are increasingly being used to understand the extent of the flatfoot deformity and aid with surgical planning. Weightbearing CT provides additional parameters used to quantify flatfoot deformity and may identify underlying anatomic variants in the subtalar joint that predispose to peritalar subluxation and flatfoot (Figure 6). 11,60,78 Weightbearing CT may help identify specific locations of deformity (eg, medial arch collapse at the talonavicular or naviculocuneiform joint) and localize impingement, arthritis, or severe calcaneal subluxation, which may need to be addressed with hindfoot (ie, subtalar) fusion. 60 CT can assess the specific source of lateral hindfoot pain, such as focal impingement between the lateral process of the talus and the anterior calcaneus. 41 MRI can identify soft tissue pathology inherent to flatfoot—primarily PTT insufficiency but also disruption of the spring or deltoid ligaments. 35,78 Bony edema on MRI, especially when seen focally between the lateral process of the talus and the anterior calcaneus at the angle of Gissane, may indicate impingement due to flatfoot (Figure 7). 119

X-ray and weightbearing computed tomography (CT) in a flatfoot patient. This patient underwent weightbearing CT, which demonstrated flatfoot deformity with severe lateral subtalar impingement. Cystic formation and bone contact are seen at the angle of Gissane. Subluxation of the calcaneus relative to the talus is also seen on the coronal image; in such cases, fusion may be needed to address the subluxation.

Magnetic resonance image of the same patient from Figure 6 demonstrated lateral subtalar impingement with hyperintensity and reactive bony edema.
Diagnosis/Stages
AAFD is divided into stages that guide treatment (Table 1). Early descriptions of PTT rupture and proposed treatments based on severity of deformity were described in 1983, and a classification using 3 stages was detailed in 1989. 68,69 In 1997, a fourth stage indicating tibiotalar joint involvement was added. 17,90 In 2007, stage II was subdivided into types IIA and IIB based on the amount of talonavicular uncoverage. 33 Although the reliability of this classification has not been formally studied, it is still regularly cited in flatfoot literature and used clinically. 3
Stages of Adult-Acquired Flatfoot Deformity.a

Abbreviations: FDL, flexor digitorum longus; LCL, lateral column lengthening; MCO, medial calcaneal osteotomy; MRI, magnetic resonance imaging; NSAID, nonsteroidal anti-inflammatory drug; PT, physical therapy; PTT, posterior tibial tendon; TMT, tarsometatarsal.
Stage I
Stage I is the mildest form of PTT dysfunction. Patients may have a history of tenosynovitis or tendinosis with mild to moderate pain over the course of the tendon. The hindfoot is mobile with normal alignment. 69 On the single-heel raise, the PTT is still able to invert and lock the hindfoot, allowing the patient to rise up onto the toes. Radiographs can be normal, although MRI may show PTT inflammation or early signs of degeneration. 49
Stage II
Stage II represents the development of deformity and abnormal function. The deformity is still flexible, however, and passive correction can be performed via adduction at the talonavicular joint and inversion at the subtalar joint. As the PTT degenerates and elongates, the foot is less able to actively invert, which precludes the ability to lock the transverse tarsal joints and rise onto the toes. 69 Subsequently, the bones distal to the talus (calcaneus, cuboid, navicular) rotate laterally and the talonavicular joint subluxates, leading to hindfoot valgus and forefoot abduction. 3,69 Unsupported, the talus now plantarflexes. These changes increase the lateral talo–first metatarsal (Meary’s) angle and decrease the coverage of the talar head by the navicular. At some point, attenuation of the spring ligament may also occur and can contribute to worsening deformity. 93
Stage IIA deformity is characterized by minimal abduction at the midfoot with less than 30% talonavicular uncoverage on the standing AP radiograph. 33 At stage IIB, the deformity is still flexible, but there is greater forefoot abduction (>30% talonavicular uncoverage). The difference in IIA and IIB may assist in determining treatment, such as the use of lateral column lengthening (Figure 8).

Flatfoot stages IIA and IIB. In patients with stage II flatfoot, substages IIA and IIB are denoted by the amount of talar head uncoverage on the weightbearing anteroposterior radiograph (dashed line), divided by the total surface of the talar articular surface (solid line + dashed line). Typically, 30% is the threshold used, in which patients with >30% talonavicular uncoverage are deemed stage IIB. This patient with bilateral flatfoot deformity has stage IIB on the left and stage IIA on the right.
Stage III
Stage III signifies a more rigid deformity, in which the malalignment at the triple joint complex (talonavicular, calcaneocuboid, and subtalar joints) cannot be corrected past neutral with passive inversion. 31,69 The hindfoot is in a fixed valgus position and forefoot abduction is present. Clinically, the PTT may be completely disrupted and therefore less painful; pain may be more severe laterally near the sinus tarsi due to impingement or arthritis. 41 Patients may have degenerative changes in the triple joint complex with arthritic radiographic signs, including joint space narrowing and osteophyte formation. 3
Stage IV
The involvement of the ankle joint is what differentiates stage IV deformity from other stages. In stage IV, the deltoid ligament is insufficient, leading to lateral talar tilt and tibiotalar valgus deformity. 17,18,90 Although some patients have tibiotalar involvement with a flexible flatfoot (denoted stage IVa), most have a rigid foot deformity in the setting of ankle joint involvement (denoted stage IVb). 17 In addition to tibiotalar deformity, ankle arthritis may also be present. 17,18
Treatment
Nonoperative
Nonoperative treatment should be attempted first, although its success has been described primarily in less severe stages of deformity. 5,75,92 In mild cases, activity modification and nonsteroidal anti-inflammatory drugs (NSAIDs) may provide symptomatic relief and allow the PTT tendonitis to resolve. 92 For patients with acute symptoms, a short period of immobilization may be provided using a boot or, in severe cases, a cast. 9 After immobilization, or for patients with chronic symptoms, patients may be transitioned to a custom brace or orthosis and a rehabilitation program.
There are a variety of orthotic options for flatfoot patients. Due to difficulty with patient compliance with the bulkier custom orthoses, many surgeons may opt to use traditional off-the-shelf ankle braces, which may provide lateral stability but do not provide as much arch support. 65 By contrast, the University of California Biomechanics Laboratory (UCBL) orthosis is a custom in-shoe orthosis that can help support the arch and stabilize hindfoot alignment. 65 The Arizona brace is a custom orthosis that combines an in-shoe brace with a leather laced-up upper portion and can also maintain midfoot height, although with less effect on the calcaneus. 65 The Arizona brace has been described in all stages of deformity, but its rigidity may limit functional activity. 65 A custom or off-the-shelf ankle-foot orthosis (AFO) with an articulation at the ankle (hinged supramalleolar orthosis [SMO], or Richey brace) permits more dorsiflexion/plantarflexion and has been associated with successful nonsurgical treatment. 65,92 A rigid AFO may be recommended in more severe stages of flatfoot (stages III-IV). 9
Structured physical therapy may also be beneficial. Rehabilitation protocols aim to mechanically strengthen ankle inversion, stretch the Achilles and gastrocnemius, improve proprioception, and ideally minimize further tendon lengthening and foot deformity. 75 In one series of patients with stage I to II deformity, a structured nonoperative protocol consisting of an orthosis and aggressive exercise/stretching resulted in improved function and satisfaction in nearly 90% of patients, with only 11% requiring surgery in the 2-year study period. 5 The protocol included a short articulated orthosis along with high repetition exercises, plantarflexion, Achilles tendon stretching, and a home regimen. 5 After completion, patients had improvement in strength and ambulation, satisfaction, and pain (change in median pain scores from 8/10 to 1/10). 5 A randomized controlled trial of stage I to II patients found that the combination of orthoses, stretching, and eccentric exercise reduced pain and improved perceived function. 75 An additional study found that after 27 months of nonoperative care, only 12.5% of patients with AAFD had surgery. 92 Whether these protocols help patients avoid surgery completely or just prolong the time until eventual operative treatment is still unknown. Obesity has been linked to an increased likelihood of failing nonoperative care, but contributing factors have not been fully elucidated. 92
Operative
Operative intervention is recommended for patients who remain symptomatic after exhausting 6 months of nonoperative treatment, though this time period may be shorter or longer depending on the patient's deformity and planned surgery. Surgery can improve pain, function, and quality of life with continued improvement demonstrated at a 2-year follow-up. 27 A myriad of surgical options exist. The deformity type, as well as surgeon familiarity and preference, dictates the particular procedure (or combination of procedures) chosen. Operative strategies are summarized below and in Table 2. The surgeon should be familiar with each strategy, because the choice of procedures must depend on the specific deformity being addressed.
Goals of Frequently Used Surgical Options for Flatfoot Treatment.
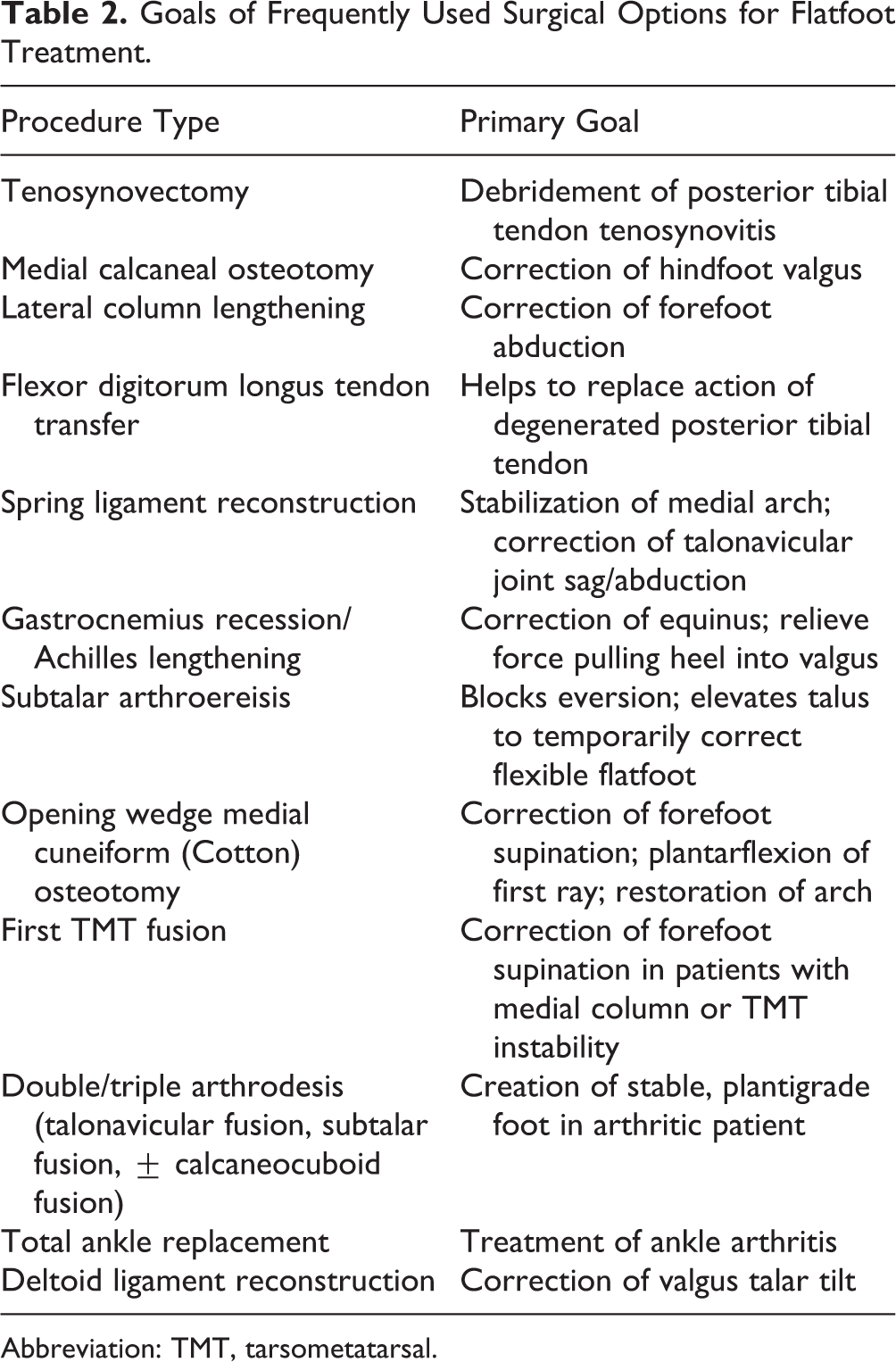
Abbreviation: TMT, tarsometatarsal.
Hindfoot Valgus
Medializing Calcaneal Osteotomy
Medializing calcaneal osteotomy (MCO) is a commonly employed technique to correct hindfoot valgus. Using a lateral approach, the calcaneus is osteotomized and the posterior segment is translated medially and fixed in place. 23 This decreases strain on the medial-sided foot ligaments and arch and repositions the axis of action of the Achilles tendon, providing correction of hindfoot valgus and improved inversion. 6,7,23,125 MCO is commonly combined with tendon transfer and can provide clinically significant improvement in pain and function at more than 10 years postoperatively. 21 When compared to other patient factors and procedures, including sex, calcaneal pitch, first tarsometatarsal (TMT) fusion, and spring ligament reconstruction, only MCO was a significant predictor of postoperative hindfoot alignment. 23 The ideal amount of translation can be calculated using a literature-based equation to achieve a slight hindfoot varus moment arm radiographically. Using this method, each additional millimeter of medial translation performed corresponds to a 1.52-mm change in moment arm. 23,26 The optimal postoperative radiographic hindfoot alignment is in mild varus (hindfoot moment arm 0-5 mm), which is associated with better clinical outcomes. 26 There are various types of fixation used in MCO, but regardless of method, union rates after MCO are high, with studies reporting rates up to 97% to 100% with comparable rates of return to activity, hardware removal, and functional outcomes. 1,73,105,107
One risk of MCO is neurovascular injury. A lateral incision is usually placed directly over the planned osteotomy site, and one study showed a safe zone using a reference point that is one-third the distance from the tip of the lateral malleolus to the posterior inferior margin of the calcaneus. 48 Appropriate skin incision placement and meticulous dissection may avoid laceration of the sural nerve and subsequent complications (painful neuroma or loss of sensation). 48 Radiographic safe zones in the calcaneus may avoid injury to the sural and medial and lateral plantar nerves, although the lateral and medial calcaneal nerves may still be at risk. 110 Some authors advocate minimally invasive techniques, citing decreased wound complications, infection rates, and nerve injury. 70,118 This has not yet been confirmed in large direct comparison studies.
Arthroereisis
Subtalar arthroereisis has been used in pediatric patients, but there is limited evidence of its utility in adults as an adjunct for additional correction. 50 An implant is placed in the sinus tarsi, with the goal of blocking physiologic eversion and elevating the talus. This procedure is minimally invasive and has produced improvements in clinical outcomes and deformity measurements but also has a high incidence of complications, especially sinus tarsi pain and need for implant removal. 91,96,106,126 Implant removal rates for symptomatic hardware range from 11% to 46%. 91,96,106 Due to the high rate of complications, most surgeons elect to correct deformity using other procedures.
Lateral Column Lengthening
Lateral column lengthening (LCL) can also provide correction of hindfoot valgus, but this is in addition to its function as a powerful mode to address forefoot abduction.
Forefoot Abduction
Lateral Column Lengthening
LCL can correct forefoot abduction, restore the medial arch, and improve talonavicular coverage (Figure 9). However, it may result in stiffness, lateral column overload, and fifth metatarsal stress fractures. 22,31,33 LCL can be achieved via osteotomy and graft or implant at the anterior calcaneus or distraction arthrodesis at the calcaneocuboid (CC) joint. Although CC distraction arthrodesis can provide substantial correction, it has largely been abandoned due to stiffness and high rates (up to 40%) of nonunion. 55 In a retrospective comparison study, patients who underwent osteotomies had better outcomes and lower rates of hardware removal than those who had CC arthrodesis. 59

Pre- and postoperative anteroposterior and lateral weightbearing radiographs of a patient who underwent lateral column lengthening and medializing calcaneal osteotomy for flatfoot (in addition, the patient underwent first tarsometatarsal fusion, flexor digitorum longus tendon transfer, and gastrocnemius recession).
The traditional calcaneal osteotomy was the Evans opening wedge osteotomy. 45 Using a lateral approach, an osteotomy is made in the anterior calcaneus approximately 10 to 15 mm proximal to the CC joint. Interpositional bone graft or implant is used to fill an opening wedge in the space. 14,45,86 Autograft and allograft (often tricortical iliac crest graft) have both been described; there is no definite consensus from the literature regarding which leads to better union and outcomes. 39,53,89 As an alternate to bone graft, studies have reported that porous titanium wedges also provide good correction with low nonunion rates. 54,84 Optimal LCL graft size may be determined by literature-based formulas, in which each additional millimeter of lengthening performed corresponds to a 6.8-degree change in lateral incongruency angle. 22 The amount of graft is typically 4 to 8 mm, the amount required to correct forefoot abduction without losing all eversion.
While the Evans osteotomy is performed between the anterior and medial subtalar facets, the Hintermann calcaneal osteotomy is performed along the anterior border of the posterior facet, at the angle of Gissane. 62 Bone graft is inserted to restore the medial longitudinal arch, with the graft slightly wider at the cranial side to account for the plantarflexion of the anterior calcaneus that occurs with lengthening. If needed, the osteotomy and graft can be secured with a screw. 62 This technique allows the osteotomy to be closer to the talonavicular axis, which is considered the center of rotation of the subtalar joint. 62 In a cadaveric study comparing the two, the Hintermann osteotomy resulted in lower rates of damage to the anterior and medial articular facets as well as the peroneus longus tendon, although there was a higher risk of sural nerve injury. 44
In addition to the Evans and Hintermann osteotomies, there is increasing use of the “Z-type” or “step-cut” lengthening osteotomy. 116 The osteotomy is performed in the anterior calcaneus, with 3 step-cuts made (distal vertical, horizontal, and proximal vertical) to form a Z-shaped pattern. The distal portion can then be rotated and lengthened to create an opening lateral wedge effect. Graft can be placed in the vertical limbs, but osteotomy healing is dependent on the horizontal limb. 34,116 Preliminary work has shown that patients who undergo this osteotomy have excellent healing and correction with few of the complications inherent to traditional LCL, although there is a risk of peroneal tendon injury due to the proximal osteotomy. 34,104
MCO and LCL produce similar improvements in stride length, cadence, and walking speed, as well as comparable radiographic measurements of the AP and lateral talo–first metatarsal angle and calcaneal pitch. 83 In 1 study, MCO resulted in better first ray plantarflexion and varus, while LCL produced greater improvement in heel inversion. 83 However, another study reported that LCL achieved nearly 3 times greater correction of the lateral talo–first metatarsal angle and produced more lasting correction compared to MCO. 20 In a cadaveric study, LCL produced significantly greater correction than MCO with concomitant flexor digitorum longus (FDL) transfer in the lateral and AP talo–first metatarsal angles. 125
For stage IIA deformities with minimal forefoot abduction, MCO in concert with other adjunct procedures may be sufficient. 31 In more severe deformities, when forefoot abduction is severe and talonavicular uncoverage exceeds 30%, LCL may be beneficial to achieve the necessary correction. 22,31,67 MCO and LCL can be combined to achieve large amounts of correction. 86,108 Biomechanically, this is advantageous because it provides enhanced deformity correction and reduces lateral foot pressures that may cause pain or other lateral column complications. 14 In the case of both MCO and LCL, there are no studies in the literature investigating the optimal order of procedures; either MCO or LCL may be performed first. When the MCO is done first, the heel position is set initially, and the eversion potential of the hindfoot is decreased. 12 Afterward, LCL can be added if further correction of forefoot abduction is needed. If the LCL is performed first, the surgeon can assess for concomitant correction of hindfoot valgus, which may affect the need for or extent of MCO.
Spring Ligament Reconstruction
The spring (calcaneonavicular) ligament is a primary static stabilizer of the medial arch. In a cadaveric study, spring ligament reconstruction corrected midfoot deformity, which may avoid further osteotomies or fusions. 13 Multiple techniques have been described for spring ligament reconstruction, including allograft, autograft (such as peroneus longus), and synthetic materials. 27,120 However, there are insufficient data to support which, if any, technique should be employed.
Forefoot Supination
Cotton Osteotomy or First TMT Fusion
Residual forefoot supination may be present after the hindfoot is corrected. Supination occurs in the setting of longstanding deformity as the forefoot attempts to compensate for hindfoot valgus and arch collapse to maintain plantigrade position. The plantarflexion opening wedge medial cuneiform (Cotton) osteotomy can address this aspect of the flatfoot deformity. 28 The medial cuneiform is osteotomized from dorsal to plantar, and the plantar hinge of cortex is left intact. 123 Allograft or autograft or an implant of approximately 4 to 8 mm is inserted to correct supination and achieve plantarflexion of the first ray. 123 Although graft size was traditionally determined by intraoperative clinical judgment, there is interest in using linear-based equations to dictate graft size based on radiographic parameters. 76
In patients with stable first TMT joints, the osteotomy can correct forefoot varus deformity and medial arch height. 4,19 However, patients with concomitant instability in the medial column or first TMT may experience excessive motion (namely, dorsiflexion with weightbearing) despite this plantarflexion osteotomy. As a result, these patients are typically treated with TMT fusion instead. 4,19,57
Equinus Contracture
Gastrocnemius Recession/Achilles Tendon Lengthening
Equinus contracture is a common pathology observed in AAFD and can lead to worsening hindfoot valgus or exacerbation of flatfoot deformity. 2,37 To address the problem, many surgeons use gastrocnemius recession or Achilles tendon lengthening. 74 Based on the preoperative and intraoperative Silfverskiold test, either a gastrocnemius recession (for isolated gastrocnemius tightness) or Achilles lengthening (for gastrocnemius-soleus tightness) is performed. 119 These are both adjunct procedures for AAFD and are not done in isolation. 74
PTT Insufficiency
Although surgery is not commonly performed in the first stage (PTT tenosynovitis or tendinosis), it may be indicated in patients who fail conservative management and are still symptomatic. Possible soft tissue procedures include tenosynovectomy, PTT repair, and tendon transfer. 49,90,112 Some surgeons believe that soft tissue procedures alone are insufficient and also recommend the addition of a medial calcaneal osteotomy, but this has not been studied for cases without deformity.
Tendon Transfer
Tendon transfers are widely favored techniques for treatment of flatfoot deformity. The most frequent choices are FDL, flexor hallucis longus (FHL), and, less commonly, peroneus brevis. 14,21,52,56,61 FDL may be favored because the tendon courses adjacent to the PTT (facilitating the approach), it is straightforward to locate anatomically, and its function is more expendable than great toe function; however, it is biomechanically weaker than the FHL. 8,52,109 The FHL has a larger size and was superior in a biomechanical study, although this has not been demonstrated in clinical scenarios. 8,109
In either case, tendon transfer alone is weak biomechanically and does not change the medial longitudinal arch height or hindfoot valgus deformity. 61,77 However, there is biomechanical and clinical success when FDL/FHL tendon transfer is combined with bony realignment procedures (commonly, MCO). 56,61 There are multiple techniques for tendon transfer with various proponents. Options for treatment include removal of the diseased PTT or augmentation of a weakened tendon, although these have not been directly compared in the literature. Some surgeons first remove the diseased PTT before proceeding with FDL or FHL transfer, since the PTT can be a major source of pain. 8,10 Other surgeons may keep the PTT because of the strength of the tibialis posterior muscle as well as the chance that pain may improve once alignment is changed. 8,10 The optimal location of FDL transfer has also been discussed, with options including the navicular, medial cuneiform, or PTT. 117 Although it was believed that tenodesis to the PTT was more physiologic while transfer to the navicular or medial cuneiform provided more secure fixation, these locations were biomechanically similar in a cadaveric study. 117
Rigid Deformity of the Foot
Double/Triple Arthrodesis
In rigid deformity of the foot, arthrodesis is usually indicated (Figure 10). In a study of patients with longstanding AAFD and rigid deformity, triple arthrodesis (talonavicular, subtalar, and calcaneocuboid joints) led to improvements in pain, function, and clinical outcomes scores. 24 A triple arthrodesis is best used in fixed flatfoot deformity but also may be used to treat severe flexible deformity where the spring ligament is severely compromised, in lieu of a spring ligament reconstruction. The patient’s age may be considered as well, as older patients with lower demands may be better off with one definitive surgery. However, there are no studies showing worse outcomes of reconstruction based on age, and the patient’s functional level should also be considered.

Pre- and postoperative weightbearing anteroposterior and lateral radiographs of a patient with stage III flatfoot deformity who underwent subtalar and talonavicular fusion (the patient also underwent medializing calcaneal osteotomy).
A dual-incision approach, with a longitudinal medial incision between the anterior and posterior tibial tendons for talonavicular exposure and a lateral incision from the tip of the fibula to the base of the fifth metatarsal, has traditionally been favored due to the complexity of the deformity. 24 In a cadaveric study, a dual-incision approach allowed better access to the calcaneocuboid joint with less vascular disruption to the talus compared to a single medial incision approach. 97 Other surgeons prefer a lateral-only incision, which has rates of deformity correction, wound complications, and pain comparable to the dual-incision approach. 85,94
Given the concern for postoperative rigidity as well as the risk of nonunion, some surgeons have tried to spare the calcaneocuboid joint. In patients whose calcaneocuboid joints are not involved in their primary disease, a double arthrodesis still provides improvement in pain, function, satisfaction, cosmesis, and shoewear. 15,102 Unfortunately, even in a double arthrodesis, patients still are at increased risk for adjacent joint (ankle, midfoot, calcaneocuboid) arthritis. 102 In addition, if there is severe hindfoot valgus, an MCO can be performed in conjunction with a double or triple arthrodesis. 111 An Achilles lengthening or gastrocnemius recession is typically needed as well. 46 It is imperative to correct the hindfoot to neutral, as the deltoid ligament may otherwise fail in a poorly positioned fusion. 79
Ankle Deformity
There is a paucity in the literature regarding surgical techniques, algorithms, and outcomes for stage IV deformity, which is characterized by deltoid ligament failure and involvement of the ankle joint. 18 Ultimately, in stage IV patients with deltoid ligament failure, it is important to determine 2 factors: the presence of ankle arthritis and whether the hindfoot is flexible.
Deltoid Ligament Reconstruction
If the foot deformity is flexible (stage IVa), joint-sparing procedures may be considered. The foot can be reconstructed using the previously described osteotomies and soft tissue procedures rather than fusion. In such cases, the ankle may be treated by reconstruction of the deltoid ligament (Figure 11). 17,32,42,58 When used as a supplement to other reconstructive procedures, deltoid reconstruction resulted in improved clinical outcomes as well as correction of valgus talar tilt by 5 degrees. 32,42 Deltoid ligament reconstruction techniques using peroneus longus autograft and anterior tibial tendon graft have been described. 32,42,58 The use of deltoid ligament reconstruction in ankle arthritis and in conjunction with ankle arthroplasty is still debated. 30

Pre- and postoperative radiographs of a patient with stage IV flexible flatfoot. The patient underwent reconstructive procedures in the foot (lateral column lengthening, medializing calcaneal osteotomy, flexor digitorum longus tendon transfer, first tarsometatarsal fusion, spring ligament reconstruction, and Achilles lengthening) and also had deltoid ligament reconstruction.
Ankle Arthroplasty/Arthrodesis
If the ankle is arthritic, however, ankle arthroplasty is usually considered. 17,32,42,58 In rigid deformity with ankle involvement (stage IVb), a double or triple arthrodesis with ankle replacement or pantalar fusion is used (Figure 12). 17 However, the optimal use of either procedure has not been well studied. There are anecdotal descriptions of staged procedures (ie, reconstructive procedures in the foot and deltoid ligament reconstruction first, followed by total ankle replacement), 30,38 but there are no studies supporting or refuting this.

Pre- and postoperative weightbearing radiographs of a patient who had previously undergone triple arthrodesis and deltoid reconstruction, who then developed severe ankle arthritis. The patient subsequently underwent total ankle arthroplasty to address the ankle arthritis. In addition, tarsometatarsal fusion and medializing calcaneal osteotomy were performed to balance the foot and stabilize the first ray. Screws were placed in the medial malleolus to prevent stress fracture in this high-risk patient.
Authors’ Preferred Operative Treatment
Stage II
The senior author will typically treat stage II or greater deformity surgically when conservative care fails. Patients should be counseled that deformity is likely to progress over time, which can make reconstruction efforts more difficult. Gastrocnemius recession or Achilles lengthening is performed based on the preoperative and intraoperative Silfverskiold test. Even in cases with minimal contracture, gastrocnemius recession is performed because it has relatively low morbidity and can minimize the deforming force of a tight calf.
A medial curvilinear incision is made slightly plantar to the course of the PTT, and the posterior tibial tendon is inspected. If the caliber and consistency of the tendon appear normal, it is left intact. If there is evidence of tendon abnormality—thickening, tears, or degeneration—it is excised. In either case, the senior author will then proceed to FDL harvest and transfer. The FDL and FHL are identified distal to the knot of Henry and tenodesed distally to the knot with a nonabsorbable suture to preserve some flexion force. 109 The FDL is then transected proximal to this location but distal to the knot of Henry. This allows sufficient length for the FDL tendon to be transferred to the navicular, where it is secured through a drill hole.
Next, MCO is performed and fixed with two 4.5-mm cannulated screws. Amount of translation is determined using a literature-based equation and is usually approximately 1 cm. 23,26 Eversion potential is then assessed clinically. If stiff, LCL is avoided, even if forefoot abduction is present. If there is >10 degrees of passive eversion and >30% of forefoot abduction, the senior author will perform an Evans LCL with allograft and fix with a lateral compression plate, taking care to maintain eversion potential. In our experience, LCL of less than 8 mm is recommended, as it may decrease the incidence of lateral overload. We aim to slightly undercorrect abduction on simulated weightbearing fluoroscopy, which has been shown to lead to better clinical results. 22,25
Correction for residual forefoot supination is then assessed clinically. In the presence of a hypermobile first ray, plantar sagging of the first TMT joint on preoperative weightbearing lateral x-rays, or significant hallux valgus deformity, a first TMT fusion is performed. Otherwise, a Cotton osteotomy is performed, typically using an allograft size between 4 and 10 mm, fixed with a screw or compression staple.
The spring ligament may be reconstructed to further improve deformity correction (namely talonavicular abduction or sag). This decision is made based on preoperative MRI assessment of the ligament, intraoperative visualization, and correction obtained by LCL/MCO. 120 If the talonavicular joint has severe arthritis, however, the senior author will usually elect to fuse the talonavicular joint instead.
Stage III
The senior author will routinely perform a double arthrodesis (subtalar and talonavicular fusion) and leave the calcaneocuboid joint intact, unless it is severely arthritic or symptomatic. This is done through a combined lateral sinus tarsi incision (subtalar joint) and medial incision between the anterior and posterior tibial tendons (talonavicular joint). We routinely perform a concomitant MCO, because correcting the hindfoot valgus through the subtalar joint is difficult and may cause excessive forefoot supination. Two 6.5-mm cannulated screws may fix both the MCO and subtalar joint fusion concomitantly. Forefoot supination is addressed after the double arthrodesis using a Cotton osteotomy or first TMT fusion. Achilles lengthening or gastrocnemius recession is typically performed as well.
Stage IV
For the cases without ankle arthritis, a deltoid reconstruction is performed at the same time the foot is addressed. 32 For cases with ankle arthritis, the authors generally perform a staged total ankle replacement with a stemmed implant and then 6 weeks later will address the foot. The choice of deltoid reconstruction in this case is controversial. In our experience, the use of a stemmed tibial implant with a relatively larger polyethylene insert allows us to adequately balance the ankle. Other surgeons may elect to reconstruct the deltoid in addition to replacing the ankle. Flexibility of the hindfoot will dictate whether a reconstruction or double arthrodesis is performed in either ankle scenario.
Conclusions
Adult-acquired flatfoot deformity is most commonly associated with posterior tibial tendon insufficiency. The etiology of AAFD is not completely understood but may be due to underlying medical comorbidities, hypovascularity, genetics, foot morphology, or trauma. Characteristic clinical and radiographic findings are used to confirm the diagnosis. The staging system for flatfoot describes the deformity and can guide treatment. Nonoperative treatment with NSAIDs, immobilization, bracing, and physical therapy should be attempted in all stages and may provide long-term symptom relief in early stages of flatfoot. Nonsurgical treatment is typically all that is required for stage I flatfoot. Stage II deformities are flexible but have increasing hindfoot valgus and forefoot abduction. In this stage, a wide variety of procedures are employed, including medial calcaneal osteotomy, FDL or FHL tendon transfer, lateral column lengthening, and gastrocnemius recession or Achilles tendon lengthening. Both medial calcaneal osteotomies and lateral column lengthening provide significant correction but may provide correction predominantly in hindfoot valgus and forefoot abduction, respectively. When the flatfoot progresses to a fixed deformity in stage III, double or triple arthrodesis is recommended. Stage IV flatfoot may be flexible or rigid but is characterized by ankle joint involvement and lateral talar tilt. Ankle salvage or reconstructive procedures, such as deltoid ligament reconstruction, joint arthrodesis, or total ankle arthroplasty, may be required in addition to corrective hindfoot procedures.
Supplemental Material
Supplemental Material, FAO820847-ICMJE - Adult-Acquired Flatfoot Deformity
Supplemental Material, FAO820847-ICMJE for Adult-Acquired Flatfoot Deformity by Jensen K. Henry, Rachel Shakked, and Scott J. Ellis in Foot & Ankle Orthopaedics
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Scott J. Ellis, MD, reports personal fees from Wright Medical, outside the submitted work. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.