
Abstract
Background:
Metal component failure in total ankle arthroplasty (TAA) is difficult to treat. Traditionally, conversion to an arthrodesis has been advocated. Revision TAA surgery has become more common with availability of revision implants and refinement of bone-conserving primary implants. The goal of this study was to analyze the clinical results and patient-reported outcomes for patients undergoing revision total ankle arthroplasty.
Methods:
We retrospectively reviewed prospectively collected data on 52 patients with a mean age of 63.5 ± 9.6 years who had developed loosening or collapse of major metal components following primary TAA. These patients were compared to a case-matched control group of 52 primary TAAs performed at the host institution with a minimum of 2 years’ follow-up. Cases of isolated polyethylene exchange, infection, or extra-articular realignment procedures were excluded. The American Orthopaedic Foot & Ankle Society (AOFAS) hindfoot score, Short Form 36 (SF-36), Short Musculoskeletal Function Assessment (SMFA), and pain scores were prospectively collected. Clinical data was collected through review of the electronic medical record to identify reasons for clinical failure, where clinical failure was defined as second revision or conversion to arthrodesis or amputation.
Results:
The identified causes of failure of primary TAA were aseptic loosening of both components (42%), talar component subsidence/loosening (36%), coronal talar subluxation (12%), tibial loosening (8%), and talar malrotation (2%). Thirty-one patients (59.5%) underwent revision of all components, 20 (38.5%) just the talar and polyethylene components, and one (2%) the tibial and polyethylene components. The average time to revision was 5.5 years ± 5.4 with a follow-up of 3.1 years ± 1.5 after revision. Eleven (21.2%) revision arthroplasties required further surgery: 6 required conversion to arthrodesis and 5 required second revision TAA. Pain scores, SF-36 scores, SMFA scores, and AOFAS Hindfoot scores all improved after revision surgery but never reached the same degree of improvement seen after primary TAA.
Conclusions:
Clinical and patient-reported outcomes of revision ankle arthroplasty after metal component failure significantly improved after surgery, although the recovery time was longer. In this series, 21.2% of revision TAAs required a second revision TAA or arthrodesis surgery. Various prostheses performed similarly when used for revision surgery. Revision TAA can offer significant improvements postoperatively.
Level of Evidence:
Level III, therapeutic.
Introduction
The number of total ankle replacements being performed in the United States is on the rise. 8 Studies demonstrating better joint motion and overall function with equivalent pain relief have led to an increase in the numbers of total ankle arthroplasties (TAAs) being performed each year with a steady rate of ankle arthrodesis. 8,23 -25,30 With the numbers of ankle arthroplasty on the rise, revision total ankle arthroplasty is also increasing. 6,18,33 What was once considered the gold-standard salvage procedure for failed TAA, the ankle arthrodesis leaves patients dissatisfied and with functional deficits. 5,22,24 A systematic review of the Scandinavian Total Ankle Replacement system demonstrated a 10.7% revision rate at 64 months. 7,9,10,20 The salvage procedures for failed total ankle replacement include revision with or without cement, conversion to arthrodesis (including use of structural graft), cement arthroplasty, and amputation. 13,19,26
Literature on outcomes of revision ankle arthroplasty surgery is remarkably sparse and patient reported outcomes from these revision surgeries is even more rare. A classification system for reporting failures in TAA was created to describe failure types, and the associated numeric classification from this system is included for reader reference (VG-# is used for this identification). 31 The goals of this study were to provide patient-reported outcomes from revision total ankle replacement and to document intermediate-term clinical outcomes from an increasingly more common and necessary procedure.
Materials and Methods
We conducted an Institutional Review Board (IRB) approved, retrospective chart review of prospectively collected data reviewing all revision total ankle arthroplasties done between September 2007 and March 2016 at one institution. Three high-volume ankle replacement surgeons performed the revision surgeries. Revision total ankle arthroplasties involving cyst debridement (VG-8) and bone grafting with polyethylene exchange/VG-6 and those being done during treatment of infection (VG-10 and VG-11) were excluded from the cohort. Those patients with major metal component failure with a minimum of 2 years of follow-up after revision surgery were included in the study. In addition, a control group was established consisting of 52 consecutive primary TAAs (performed between July 2013 and June 2015) with a minimum of 2 years follow-up. These patients were pulled from a prospective database at the host institution. The control group was matched with the revision TAA group for age as well as implant used.
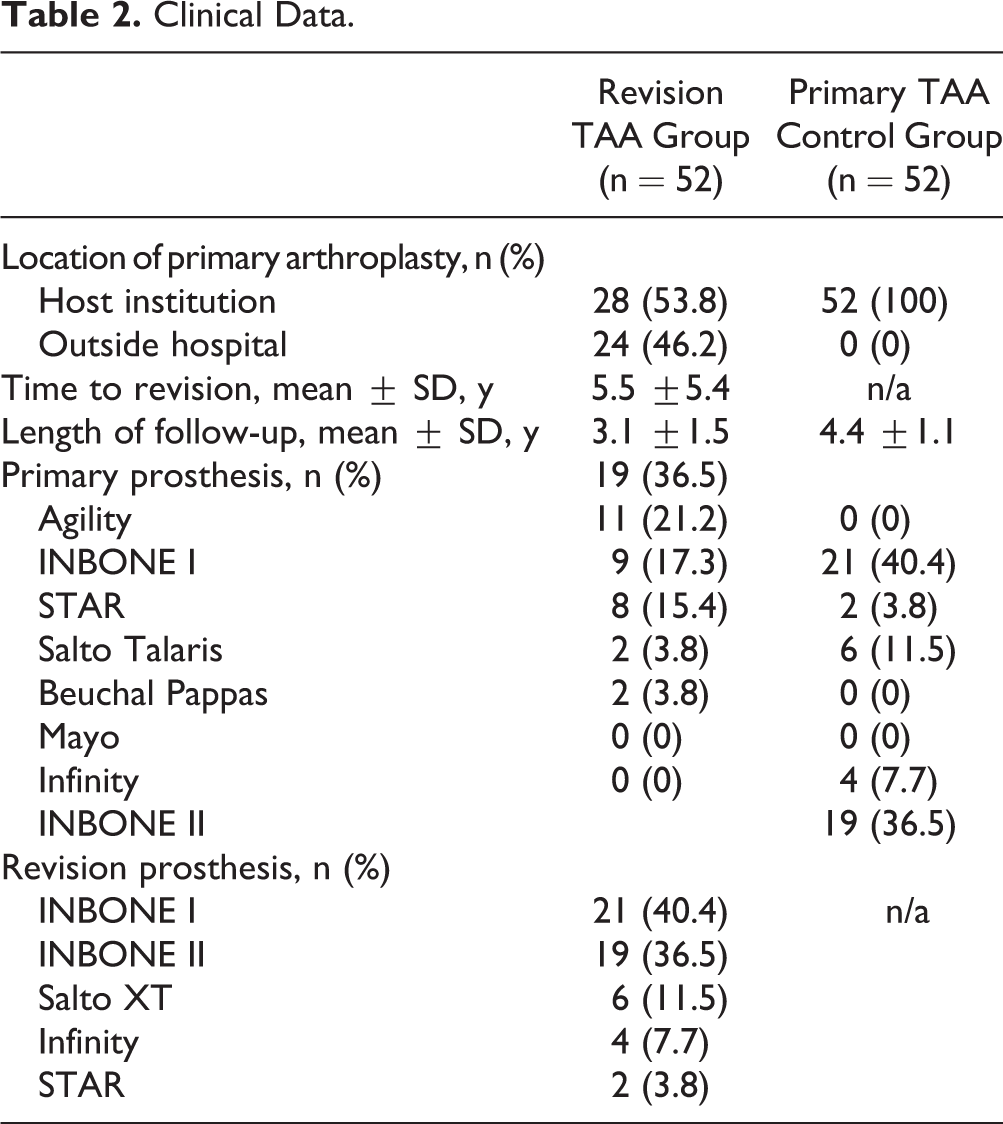
Fifty-two primary total ankle arthroplasties requiring revision (52 patients [27 female, 51.9%, and 25 male, 48.1%]) met the inclusion criteria for this study. The mean age (and standard deviation) of the patients was 63.5 ± 9.6 years (range 39-83 years). Twenty-eight of the ankles (53.8%) had their primary surgery at the revision institution while 24 ankles (46.2%) represented referrals from outside institutions. On average, revision total ankle arthroplasty occurred at 5.5 ± 5.4 years (range 0.6-35 years). The mean duration of follow-up after revision TAA was 3.1 ± 1.5 years (range 2.0-10.3 years). There was no difference in demographics, clinic data, or implants used between the revision TAA group and the control primary TAA group (see Table 1 for complete demographic information).
Demographic Data.

Patients completed outcomes questionnaires preoperatively before revision TAA, then at 6 months, and then on an annual basis postoperatively after both primary and revision TAA where applicable. Each patient filled out the American Orthopaedic Foot & Ankle Society (AOFAS) hindfoot score, pain score of maximum pain level over the previous week, Short Form 36 (SF-36), and the Short Musculoskeletal Function Assessment (SMFA) questionnaires at the above intervals.
Each patient had erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) blood tests to screen for infection. If either of these were mildly elevated, a frozen section of synovial tissue was obtained intraoperatively to look for white blood cells (WBCs) per high-powered field (HPF). Patients with suspected infection (ie, elevated WBC per HPF) were excluded from this study. Patients were evaluated for revision based on clinical examination as well as implant appearance on radiographs and advanced imaging.
The Student t test was used to compare findings for preoperative and postoperative outcome scores and 1-way analysis of variance was used for comparisons of more than 2 means. All statistical analysis was performed using SPSS 22 (IBM Corp, Armonk, NY) by a professional with expertise in statistics.
Results
The average length of follow-up after revision TAA was 3.1 ± 1.5 years (range 2 years to 10.3 years). The Agility prosthesis was the most frequently revised (19/52, 36.5%) in this study, followed by the INBONE I (11/52, 21.1%), STAR (9/52, 17.3%), Salto Talaris (8/52, 15.4%), Beuchal Pappas (2/52, 3.8%), and Mayo (2/52, 3.8%) prostheses, respectively. The most commonly used prostheses in revision situations were the INBONE I (21/52, 40.4%), INBONE II (Wright Medical Technologies, Arlington, TN; 19/52, 36.5%), Salto XT (Integra, Plainsboro, NJ; 6/52, 11.5%), Infinity (Wright Medical Technologies; 4/52, 7.7%), and STAR (2/52, 3.8%), respectively (Table 2).
Clinical Data.
In the revision TAA cohort, the diagnosis at the time of primary total ankle arthroplasty was post-traumatic in 32 ankles (61.5%), primary osteoarthritis in 9 ankles (17.3%), inflammatory arthritis in 6 ankles (11.5%), and gouty arthritis in 5 ankles (9.6%). The most common indication for revision TAA was aseptic loosening of both talus and tibia (VG-12.3) (22/52, 42.3%) followed by talar subsidence or loosening (VG-12.2) (19/52, 36.5%), coronal talar subluxation (6/52, 11.5%), tibial loosening (VG-12.1) (4/52, 7.7%), and talar malrotation (1/52, 1.9%), respectively (Table 3). Talar subsidence was diagnosed either on plain lateral radiographs demonstrating progressive distal migration of the talar component, or through single-photon emission computed tomography (SPECT). Coronal talar subluxation is a phenomenon related to the “saddle” talar component in the INBONE I prosthesis. This component does not prevent subluxation medially or laterally in the coronal plane as successfully as the “sagittal sulcus” talar component present in the INBONE II prosthesis. Talar malrotation occurred intraoperatively during the primary TAA, where the talar prosthesis was placed in an externally rotated position. In 31 patients (59.6%), all components were revised (tibia, talus, and polyethylene). Twenty patients (38.5%) had only the talar and polyethylene components revised, whereas 1 patient (1.9%) had only the tibial and polyethylene components revised.
Indications for Primary and Revision Total Ankle Arthroplasty.

At the time of the most recent follow-up, 41 patients (78.8%) retained their initial revision implants, 5 patients (9.6%) went on to require a second revision TAA (VG-12.3) and 6 patients (11.5%) required conversion to tibiotalar arthrodesis (VG-12.4). The average time to second revision after first revision was 24 ± 4.7 months. Of the 5 patients requiring second revision surgery, 2 patients had wound complications requiring debridement and polyethylene exchange with additional soft tissue coverage procedures (VG-9), 2 patients required gutter debridement with polyethylene exchange (VG-5 and VG-6), and 1 patient required subtalar arthrodesis with gutter debridement and polyethylene exchange (VG-3, VG-5, and VG-6). The overall failure rate in this cohort was 21.2%. None of the patients in this cohort had a periprosthetic joint infection around their revision TAA, and there were no perioperative fractures.
The average improvement in pain score for the control group after primary TAA in our study was 61.1 (from 70.6 to 9.5). The average improvement in pain score after revision TAA was 49.7 (from 64.8 to 15.1). This difference was significant (P = .05). Significant differences were also seen in the changes between the control group preoperatively to postoperatively and the revision cohort, with respect to SF-36 (Mental P = .03, Physical P = .04), and SMFA (Function P = .04, Bother P = .05), but not in the AOFAS hindfoot scores (P = .57) in this study.
The maximum improvement achieved after primary TAA in the control group was greater than those achieved in the revision TAA group for all measures except the AOFAS hindfoot score. The change from preoperative to postoperative scores for both the primary group and the revision group were significant but the magnitude of improvements seen after primary TAA were greater than the revision group.
Discussion
Revision total ankle arthroplasty for failed primary TAA was successful in 41 of the 52 ankles (78.8%) and of the eleven failures, 5 underwent successful repeat revision and had their prosthesis in place at the time of conclusion of this study. Overall, these 46 patients had significant improvement in VAS, SF-36, SMFA, and AOFAS hindfoot scores when compared to prerevision questionnaires (Table 4). Though significant improvement was noted in all outcome measures after revision TAA, the magnitude of improvement did not reach those achieved after primary TAA.
Clinical Outcome Scores From Primary and Revision TAA.

Failure rates and rates of reoperation in this study were comparable with those following both primary total ankle replacement and tibiotalar arthrodesis. 1,4,12,15 -17 The rate of reoperation or additional surgery after tibiotalar arthrodesis with block allograft salvage of failed TAA is notable because of nonunion rates and adjacent joint arthritis. 2,3,12,14,29,32 In the current study, the overall failure rate was 21.2% (11 of 52 ankles) during an average follow-up period of 3.1 years. Of the 11 patients who failed revision TAA, 6 were converted to arthrodesis/VG-12.4 and 5 of 6 had talar subsidence listed as the reason for failure of primary TAA. These 5 patients had revision TAA with the INBONE prosthesis and all developed some grade of talar avascular necrosis precluding a second revision TAA. This phenomenon has been demonstrated in a cadaveric model while drilling through the subtalar drill hole in the INBONE prosthesis and cited a 75% (3 of 4 specimens) rate of transection of the artery of the tarsal canal. 27 When the 6 patients who underwent salvage arthrodesis are excluded from the results, 46 patients (41 with one revision and 5 who required second revision TAA) had a reoperation rate of 19.8%, most commonly for gutter debridement and polyethylene exchange.
The studies detailing results of revision total ankle arthroplasty are limited. Reoperation rates range from 15% to 24% most commonly for gutter debridement. Failure rates in these previous cohorts are as high as 17%. 6,11 There are very few reports of below knee amputation in the available studies. 6 Both of these previous studies conclude that proper patient selection improves outcomes and revision TAA can be done successfully in the right patients.
Custom prostheses were not used in any of the revision surgeries in this study. They are no longer available for use in the United States at the time of this study. All patients in this study underwent revision for either metal component loosening/subsidence or component malalignment.
The reason for the differences between patient-reported outcomes after primary and revision TAA is unclear. The authors speculate that factors including bone loss, raising or lowering the joint line, and case duration among others could account for this difference. Our results indicate that revision arthroplasty should be considered in place of tibiotalar arthrodesis for failed TAA where possible, due to the comparable rates of reoperation and failure for each surgery.
There were limitations in this study. The patient-reported outcomes measures were collected prospectively but the study was retrospective. There is a potential selection bias when indicating a patient with a failed TAA for revision arthroplasty instead of tibiotalar arthrodesis. 21,28 Though aseptic loosening accounted for most revision TAAs, there was a total of 6 different indications for revision surgery. Additionally, the INBONE I and II were far and away the most frequently used prosthesis during revision, which could be seen as a limitation. Three other prostheses were also included in the study to diversify the cohort. Also, the control group was matched for basic demographics and implants used but some differences between the groups, including preoperative diagnosis, could not be controlled. The heterogeneity between the control group and the revision TAA group is another limitation. Another reasonable option for a control group would be to compare the revision cohort to all primary total ankle replacements contained in the database. The authors chose a case-matched control group to minimize differences in implants and follow-up times.
In conclusion, the results for revision total ankle arthroplasty performed for metal component failure show promising trends. Patient-reported outcomes improve significantly after revision surgery and, though these results are less in magnitude than those after primary TAA, health-related quality of life and function benefit greatly from this procedure. The information from this cohort may help surgeons set accurate expectations for recovery after revision TAA. With a failure rate of 21.2%, case by case evaluation is required to determine the best revision surgery for failed total ankle arthroplasty.
Supplemental Material
Supplemental Material, FAO813026-ICMJE - Revision Surgery for Metal Component Failure in Total Ankle Arthroplasty
Supplemental Material, FAO813026-ICMJE for Revision Surgery for Metal Component Failure in Total Ankle Arthroplasty by James R. Lachman, Jania Arcia Ramos, Samuel B. Adams, James A. Nunley, Mark E. Easley, and James K. DeOrio in Foot & Ankle Orthopaedics
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: James A. Nunley, MD, and James K. DeOrio, MD, report personal fees from Wright Medical Technologies, personal fees from Stryker, personal fees from Integra LifeScience, outside the submitted work. Mark E. Easley, MD, reports other from Stryker Orthopaedics- STAR development team, outside the submitted work. In addition, Drs. Nunley, DeOrio, and Easley have a patent Vantage Total Ankle System-Exactech, Inc. with royalties paid. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.