
Abstract
Background:
Hallux valgus (HV) is commonly treated with proximal or distal first metatarsal osteotomy. Despite good correction, these procedures have inherent risks such as malunion, nonunion, metatarsal shortening, loss of fixation, and avascular necrosis. Suture button fixation has been used for HV treatment. It avoids the risks of corrective osteotomies while maintaining reduction of the intermetatarsal angle (IMA). The goal of this study was to assess the radiographic and functional outcomes of patients undergoing HV correction with a distal soft tissue procedure and proximal suture button fixation.
Methods:
The authors retrospectively reviewed the charts and radiographs of 22 patients who had undergone HV correction using a distal soft tissue correction and proximal fixation with a miniature suture button device (Mini TightRope; Arthrex, Inc, Naples, FL). Mean follow-up was 27.7 months. The IMA, hallux valgus angle (HVA), and sesamoid station were measured on radiographs obtained preoperatively as well as in the immediate postoperative period and at final follow-up. Preoperative and postoperative Short Form-36 (SF-36) and Foot and Ankle Ability Measure (FAAM) scores were collected. Postoperative complications, and any additional operative procedures performed were also recorded.
Results:
The mean preoperative IMA and HVA were 16.9 and 32.6 degrees, respectively. The mean immediate postoperative IMA was 5.2 degrees (P < .0001) and the mean HVA was 9.8 degrees (P < .0001). At final follow-up, the mean IMA was 8.2 degrees (P < .0001) and the mean HVA was 16.7 degrees (P < .0001). The average change in HVA from preoperative to final follow-up was 16.0 degrees and the average change in IMA from preoperative to final follow-up was 8.6 degrees (P < .0001). Sesamoid station assessment at the 2-week follow-up showed that 22 patients (100%) were in the normal position group; at final follow-up, 17 patients (77%) had normal position and 5 patients (23%) had displaced position. Although there were no clinically symptomatic recurrences, asymptomatic radiographic recurrence was noted in 5 patients (23%) who had a final HVA >20 degrees. All components of the FAAM and the SF-36 showed improvement from preoperative to final follow-up, although these changes were not statistically significant. Three patients experienced complications, including an intraoperative second metatarsal fracture, a postoperative second metatarsal stress fracture, and a postoperative deep vein thrombosis.
Conclusion:
The use of a distal soft tissue procedure in conjunction with proximal suture button fixation is a safe and effective procedure for treating symptomatic HV deformity. Our results show that this technique can correct the IMA, HVA, and sesamoid station without the need for osteotomy.
Level of evidence:
Level IV.
Introduction
Hallux valgus (HV) is one of the most common forefoot conditions. 1,4,12,16 Operative treatment options for HV include soft tissue procedures with medial eminence resection, osteotomies, and arthrodesis of the metatarsophalangeal (MTP) or tarsometatarsal (TMT) joints. 5,16 More than a 100 different procedures have been described to address and treat HV. Nevertheless, there is no single gold standard treatment. 1,4
Despite the ability to achieve good correction with proximal and distal osteotomies, these procedures have inherent risks such as malunion, nonunion, metatarsal shortening, transfer metatarsalgia, loss of fixation, and avascular necrosis of the first metatarsal head. 7,2 In addition, these procedures are designed to alter osseous alignment and, in the case of osteotomies, entail extra-articular correction of an intra-articular deformity. It has been argued, however, that HV is primarily due to soft tissue contracture and attenuation, resulting in malalignment at the articular level. 7 “Metatarsal suspension” techniques avoid corrective osteotomies and close the intermetatarsal angle (IMA) with distal soft tissue releases and the use of a nonabsorbable suture between the first and second metatarsals. The potential benefits of avoiding an osteotomy include decreased recovery time, smaller incisions, earlier weightbearing, and avoiding complications associated with osteotomies. 7,2 Several authors have examined the outcomes of suture suspension HV correction techniques. 7,8,11,13 Most recently, a series was on 14 patients who experienced a decrease in the IMA and hallux valgus angle (HVA) when treated with a modified suture button construct (Arthrex Mini TightRope). 7
The goal of the current study was to assess the outcomes of HV correction using a distal soft tissue procedure combined with proximal miniature suture button device (Mini TightRope; Arthrex, Inc, Naples, Florida).
Methods
Institutional review board approval was obtained for this research. We performed a retrospective cohort study of 22 nonconsecutive patients who underwent HV correction with an extensive lateral release, medial eminence resection and capsular imbrication, and proximal fixation using a miniature suture button device (Mini TightRope; Arthrex) device. Mean follow-up was 27.7 months (range, 12-63 months). The average age at surgery was 60.6 years (range, 42-75 years) with 22 females and no males. Surgeries were performed between 2012 and 2015, and a total of 46 patients underwent bunion correction with a miniature suture device, leaving a follow-up rate of 48% (22/46). Inclusion criteria were as follows: older than 18 years, failed nonoperative care, and HV correction performed with the use of a mini suture device. Exclusion criteria were as follows: prior bunion surgery, inflammatory arthritis, and follow-up of less than 1 year. There was no exclusion for degree of preoperative deformity or metatarsal adductus. Patients with mild, moderate, or severe HV deformity, an incongruent first MTP joint, and an increased yet flexible IMA were included in the study. The flexibility of the IMA was assessed manually in the office and also intraoperatively, both before and at the conclusion of the lateral release. Contraindications included an intermetatarsal facet between the lateral base of the first metatarsal and medial base of the second metatarsal, an os intermetatarseum, rigid intermetatarsal deformity, first MTP arthritis, first TMT arthritis, and a congruent deformity. For patients with rigid metatarsal primus varus, a proximal osteotomy was performed, and for first TMT arthritis or instability, a first TMT fusion was performed. These patients were not included in the study. Minimum follow-up was 1 year.
Operative Technique
All surgeries were performed by one of the senior authors (E.M.B., C.P.C., J.T.S.). First, an extensive lateral release of the metatarsophalangeal joint complex was performed. Through a dorsal incision, the adductor tendon, intermetatarsal ligament, metatarsal-sesamoid ligament, and lateral joint capsule were completely released (Figure 1). The lateral capsule was not pie-crusted, but instead incised sharply. Care was taken to fully release the plantar lateral aspect of the joint, such that a freer elevator could be swept from plantar to dorsal around the metatarsal head. Next, the medial aspect of the joint was exposed through a separate, medial longitudinal incision. The medial capsule was then opened in line with the skin incision taking care to protect the dorsal medial cutaneous nerve. Following resection of the medial eminence, a capsular repair was performed by advancing the plantar flap proximally and securing this with oblique mattress stitches. Fluoroscopy was then used to confirm that the HVA was corrected as well as the sesamoid station (Figure 2).

Case steps for using Mini TightRope. (A). Standard incisions when using Mini TightRope. (B). Placement of guidewire. (C). Passing through of Mini TightRope from lateral side. (D). Mini TightRope passed. (E). Tightening of Mini TightRope on medial side. (F) Final position of hallux.

Radiographic images taken during use of Mini TightRope. (A) Placement of Guidewire for Mini TightRope. (B) Cannulated drill for Mini TightRope. (C) Final position of Mini TightRope.
The suture button construct was then inserted. An approximately 2-cm longitudinal incision was made between the second and third metatarsals. Distally, this incision began at the level of the proximal extent of the lateral release incision. It extended 1 to 2 cm proximally. The lateral aspect of the second metatarsal shaft was exposed and a 1.1 mm suture passer/guide wire advanced first through the second metatarsal and then through the first metatarsal, exiting through the medial diaphysis just proximal to the first metatarsal head. Care was taken to capture 4 cortices with the suture passer to minimize the chance of suture cut-out. The trailing edge of the guidewire has a loop that is used to pull the suture from lateral to medial. The lateral button sits on the lateral aspect of the second metatarsal. The suture was then pulled out of the medial aspect of the first metatarsal. It was tensioned and then tied over a medial button.
Postoperatively, patients were kept heel weightbearing for a period of 6 weeks in a postoperative shoe. Weightbearing was then progressed in a sneaker for an additional 2 weeks.
Radiographic Evaluation
The IMA, HVA, and sesamoid station were measured on anteroposterior weightbearing radiographs preoperatively and at the final follow-up visit. The initial postoperative radiographs were non-weightbearing. The HVA was measured as the angle subtended by a line formed from the long axis of the first metatarsal and the long axis of the proximal phalanx. The IMA was measured by the angle subtended by the long axis of the first metatarsal and second metatarsal. Recurrence was defined as an HV angle of greater than 20 degrees at final follow-up. 11
Sesamoid station was determined by assessing the relationship of the tibial sesamoid to the long axis of the first metatarsal on the anteroposterior (AP) radiograph. Sesamoid station was classified as grade I, II, III, IV, V, VI, or VII. Sesamoid station of grade IV or less was classified as normal sesamoid position and grade V or greater as lateral displacement of the sesamoid (Figure 3). 13 Standing weight bearing radiographs were obtained at final follow-up (Figure 4).
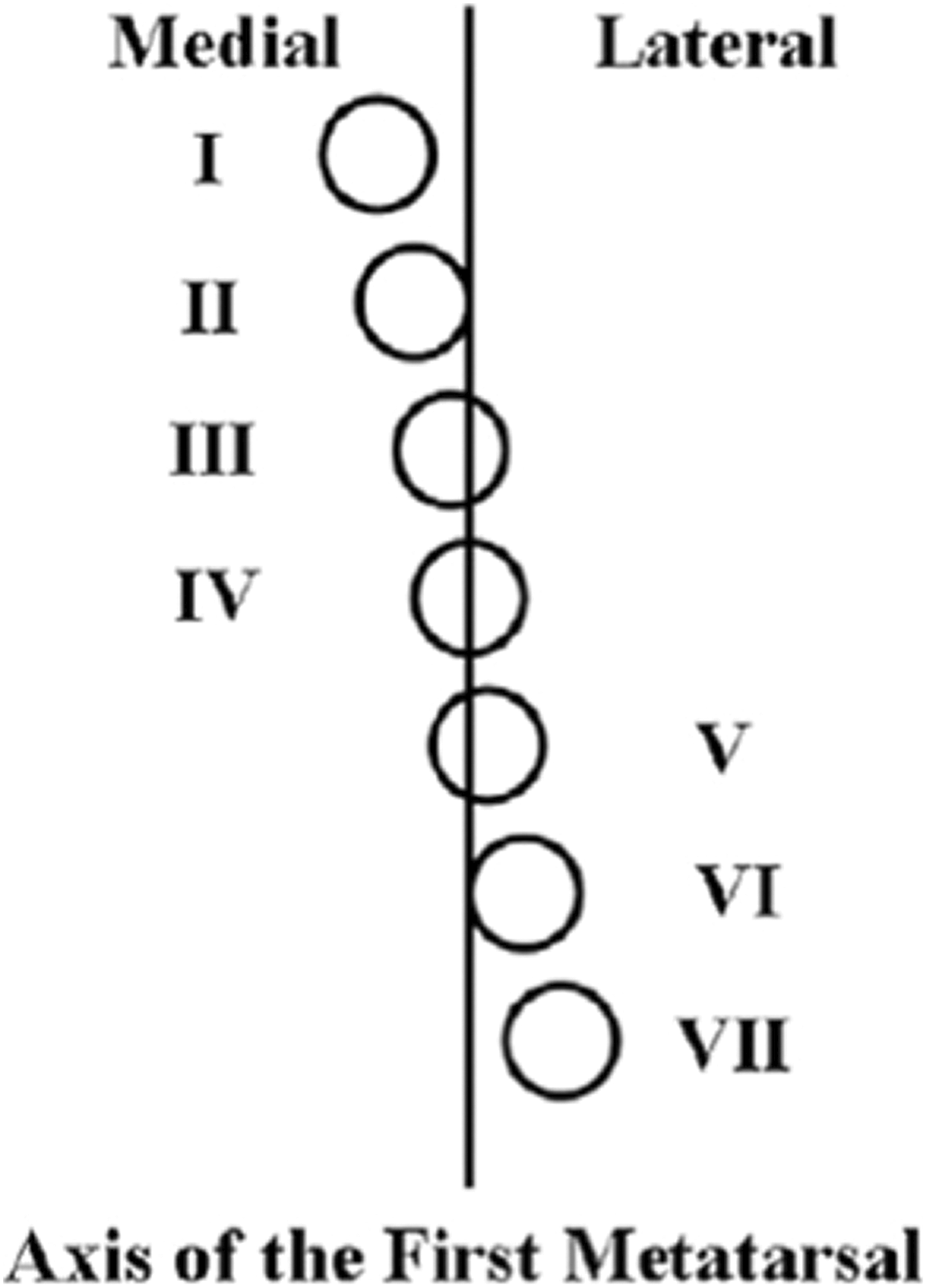
Sesamoid station is determined by the position of the tibial sesamoid relative to the mid-axis of the first metatarsal, as defined by Hardy and Clapham. 6

Preoperative and postoperative radiographs in 2 patients. (A) Preoperative radiograph in patient 1 with elevated intermetatarsal angle. (B) Preoperative radiograph in patient 2 with elevated intermetatarsal angle. (C) Three-year postoperative radiograph in patient 1. (D) Four-year postoperative radiographs in patient 2.
Additional procedures performed at the time of HV correction included gastrocnemius recession, hammertoe correction, lesser metatarsal shortening osteotomy, Akin osteotomy, metatarsal head resection, and metatarsal open reduction internal fixation (Table 1).
Additional Procedures Performed at Time of HV Correction.

Abbreviations: HV, hallux valgus; ORIF, open reduction internal fixation.
Patient-Reported Outcomes
Preoperative Short Form-36 (SF-36) scores and Foot and Ankle Ability Measure (FAAM) scores were collected in the majority of patients. At final follow-up, patients completed a SF-36 and FAAM. 10,11
Statistical Analysis
Means and standard deviations are presented for continuous measurements, including degrees of deformity, changes in degrees of deformity, FAAM, and SF-36. We performed further statistical tests to determine whether the change in continuous measurements was different from zero. First, we used histograms and Q-Q plots to assess the normality of the measurements. Paired t tests were used for measurements with normal distribution. If measurements were skewed, the nonparametric Wilcoxon signed-rank test was used instead. Frequencies and percentages were presented for the categorical measurement sesamoid station grade. In addition, we defined recurrence of radiographic deformity by evaluating the degree of deformity at final follow-up; recurrence was defined as degree of deformity greater than 20 for HVA. All analyses were conducted using SAS software version 9.4 (SAS Institute, Cary, NC).
Results
All patients had non-weightbearing radiographs at 2 to 6 weeks postoperatively and weightbearing radiographs at the final follow-up visit. There was a statistically significant (P < .001) decrease in both IMA and HVA when comparing the preoperative and the immediate postoperative radiographs (Table 2). The average change in HVA was 22.8 degrees, and the average change in IMA was 11.7 degrees. There was also a statistically significant (P < .001) decrease in both the HVA and IMA from preoperative to final follow-up. The average change in HVA from preoperative to final follow-up was 16.0 degrees, and the average change in IMA from preoperative to final follow-up was 8.6 degrees (Table 2).
Radiographic HVA and IMA Preoperatively, at Initial Follow-up, and at Final Follow-up.

Abbreviations: HV, hallux valgus; IM, intermetatarsal.
*P values are based on Wilcoxon signed-rank test. Wilcoxon signed-rank test is a paired t test for nonparametric data.
Sesamoid station was preoperatively classified as grade V or greater in all 22 patients. Postoperatively, patients were divided into 2 groups, those with normal sesamoid position (grade IV or less) and those with persistent sesamoid displacement (grade V or greater). At the initial follow-up, 22 patients (100%) were in the normal position group. At the time of final follow-up, 17 patients (77%) were in the normal position group and 5 patients (23%) were in the displacement group (Table 3).
Distribution of Sesamoid Station Preoperatively, at Initial Follow-up, and at Final Follow-up.

Three patients had complications, including 1 intraoperative second metatarsal fracture, a postoperative second metatarsal stress fracture, and a postoperative deep vein thrombosis. The intraoperative fracture was treated with K-wire fixation, which was removed at 8 weeks. This patient did very well and healed without further intervention or complication. The metatarsal stress fracture occurred at 8 weeks postoperatively in the context of the patient’s dog jumping on her foot. This was treated nonoperatively with a walking boot and successfully united. The deep vein thrombosis was treated with anticoagulation and had no other associated complications. No patients required revision surgery or developed hallux varus.
Radiographic recurrence occurred in 5 patients (23%). 11 Nevertheless, these patients did well and were asymptomatic. BMI, age at time of surgery, preoperative HVA, and preoperative IMA did not correlate with postoperative HV recurrence (Table 3).
Preoperative FAAM scores were available in 68% of cases. Postoperative FAAM scores were available in 100% of patients. There was no statistically significant difference between the pre- and postoperative FAAM or SF-36 scores (Tables 4 and 5)
Preoperative and Postoperative FAAM Scores.

*P values are based on Wilcoxon signed-rank test. Wilcoxon signed-rank test is a paired t test for nonparametric data.
Preoperative and Postoperative SF-36 Scores.
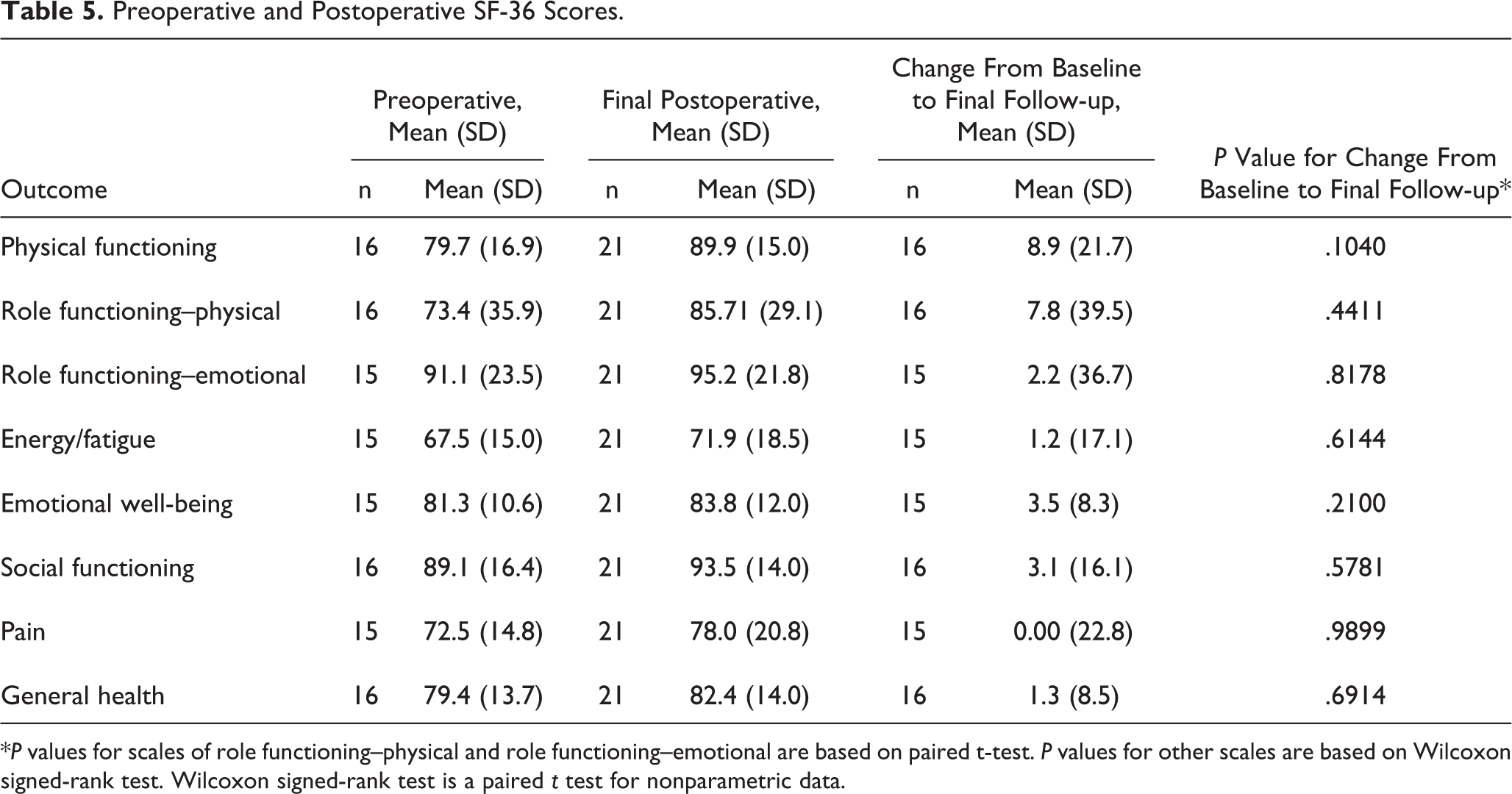
*P values for scales of role functioning–physical and role functioning–emotional are based on paired t-test. P values for other scales are based on Wilcoxon signed-rank test. Wilcoxon signed-rank test is a paired t test for nonparametric data.
Discussion
The results of our study show that the use of a suture button device is a viable option to treat HV deformity. In our study we reported an average preoperative IMA and HVA of 16.9 and 32.6 degrees, respectively, and there was a statistically significant decrease in both IMA and HVA at final follow-up to 8.2 degrees (P < .0001) and 16.7 degrees (P < .0001).
In our series, there was one patient who sustained an acute, intraoperative fracture successfully managed with K-wire fixation. Another patient sustained a postoperative fracture due to unexpected trauma and was successfully treated with a walking boot.
Our study found a final HVA, IMA, complication rate, and radiographic recurrence rate that are similar to those reported in the literature. A recent report on 5 patients undergoing HV correction with the original Mini TightRope device reported statistically significant reductions in IMA and HVA when comparing preoperative, immediate postoperative, and 20-month postoperative measurements. They did observe loss of correction of both the IMA and HVA between the immediate and long-term postoperative time points, although these changes were not statistically significant. They also reported that 3 of the 5 patients (60%) required removal of the device because of complications (fractured second metatarsal, fourth metatarsal stress fracture, and hallux varus). 15
Subsequently, another clinical study reported the clinical results of 44 cases of moderate to severe HV deformities corrected with the original version of the device. 9 Thirty-three patients also underwent an osteotomy of the distal metatarsal or the proximal phalanx. In this series, the average HVA improved from 32.2 to 15.2 degrees. The average first IMA improved from 14.6 degrees to 8.2 degrees. Complications included 2 stress fractures of the second metatarsal and 2 instances in which the button pulled through the cortex of either the first or second metatarsal.
Most recently, a retrospective study was performed with 14 patients undergoing HV correction using the second-generation Mini TightRope device using a 1.1-mm suture passer and no drill bit. These authors reported statistically significant decreases in both IMA and HVA from the preoperative status to 1-week postoperative. The mean 1-week postoperative decrease in IMA and HVA when compared with preoperative was 9 and 28 degrees, respectively. At 6 months, the mean IMA and HVA reductions were 6 and 19 degrees, respectively. There were 2 minor soft tissue complications and 1 intraoperative second metatarsal fracture. 7
Although 5 patients had a radiographic recurrence of HVA in our study, all SF-36 and FAAM scores showed improvement from the preoperative period to final follow-up. In the patients with recurrence, the IM angle was maintained and thus we feel the recurrence occurred at the MTP joint. This may be due to recurrent capsular failure or pronation of the metatarsal that was not addressed at the time of surgery. However, our postoperative HV radiographic results are consistent with those in the literature, especially those that examine radiographic recurrence rather than just clinical recurrence. Examining recurrence after distal chevron osteotomy, one study found a radiographic recurrence rate of 73% at a mean of 7.9 years; however, none of the recurrences were painful. 14 Another study reported a 54% recurrence rate (HV > 15 degrees) in their randomized trial of scarf versus chevron osteotomy in 96 patients. Despite this recurrence, American Orthopaedic Foot & Ankle Society (AOFAS) scores were improved in both groups at final follow-up. 3 Taken together, these studies, as well as ours, suggest that radiographic parameters for HV do not always correlate with clinically symptomatic recurrence. 3,14
We also assessed sesamoid station in addition to looking at changes in HVA and IMA. There is a high correlation between the lateral displacement of the sesamoids and the degree of HV deformity. 13 Many believe that reduction of the sesamoids relative to the long axis of the first metatarsal is necessary to achieve a good outcome and prevent HV recurrence. 6,13
Using the method to measure sesamoid station described by Hardy and Clapham (Figure 3), we assessed the grade of medial and lateral sesamoid displacement preoperatively, immediately postoperatively, and at final follow-up. 6 Our data showed that despite having an initial adequate reduction of the sesamoids (100% < Grade V), 5 patients (23%) had a recurrence of sesamoid displacement. Four of these had asymptomatic radiographic recurrence of their HV angle to greater than 20 degrees; however, none of these patients recurred to their prior level and all had a lower sesamoid grade than preoperatively. These radiographic parameters again did not correlate with clinical significance.
Limitations of this study include the small cohort size, lack of a control group, and low follow-up rate. Patients were asked to come in for a clinical examination and additionally have investigational radiographs for the purpose of this study. We believe that this may have led to the low rate of follow-up. Outcome scores were not available for all patients, and therefore our analysis of functional outcome is somewhat limited. Lastly, all patients in this cohort were women, raising the question of generalizability of the results to men. That being said, we have no reason to believe that men respond differently to this technique.
Conclusion
The use of a distal soft tissue procedure in conjunction with a suture button device appears to be a safe and effective procedure for treating symptomatic HV deformity. Our results show that this technique can correct the IMA, HVA, and sesamoid station with results, complications, and recurrence that are similar to other reported techniques while avoiding an osteotomy.
Supplemental Material
Supplemental Material, FAI806951-ICMJE - Treatment of Hallux Valgus Deformity Using a Suture Button Device: A Preliminary Report
Supplemental Material, FAI806951-ICMJE for Treatment of Hallux Valgus Deformity Using a Suture Button Device: A Preliminary Report by Tyler A. Gonzalez, Jeremy T. Smith, Eric M. Bluman, Lauren V. Ready, William Ciurylo, and Christopher P. Chiodo in Foot & Ankle Orthopaedics
Footnotes
Acknowledgment
We thank Jamie Collins and Ying Heidi Yang for their help with the statistical analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Christopher P. Chiodo, MD, reports grants from Arthrex (educational support), outside the submitted work. ICMJE forms for all authors are available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.