
Abstract
Background:
There is substantial variability in the operative treatment of hallux valgus despite the existence of high quality evidence to guide treatment decisions. The purpose of this study was to determine the current trends in the treatment of mild, moderate, and severe hallux valgus and if greater degrees of consensus correlate with the presence of higher-level evidence.
Methods:
Members of the American Orthopaedic Foot & Ankle Society completed a 14-item survey. A total of 131 (14%) of 922 members completed the survey. Three cases representing 3 stages of HV were presented, and respondents selected their preferred treatment. Preferred forms of proximal and distal metatarsal osteotomies, as well as mode of fixation for each, were inquired.
Results:
In the treatment of mild hallux valgus without second metatarsalgia, 80% of those surveyed chose a distal metatarsal osteotomy, while, if second metatarsalgia was present, 56% chose a distal metatarsal osteotomy with a second metatarsal-shortening osteotomy. In the treatment of moderate hallux valgus, there was generally less consensus, while, in the treatment of severe hallux valgus, a majority of those surveyed chose a Lapidus procedure, with the addition of a second metatarsal-shortening osteotomy in the presence of second metatarsalgia. The most popular distal and proximal metatarsal osteotomies, respectively, were chevron osteotomy (80%) and opening wedge osteotomy (33%). The presence of Level I evidence did not significantly correlate with higher degrees of consensus.
Conclusion:
Despite the existence of high-quality evidence supporting the use of certain procedures in the treatment of HV, there exists an apparent lack of consensus among surgeons about the choice of surgical procedures. Moreover, higher-level evidence was not correlated with greater consensus in hallux valgus.
Level of Evidence:
Level II.
Introduction
Hallux valgus (HV) is the most common deformity of the forefoot, although there is little consensus in terms of optimal surgical treatment with more than 200 different operative treatments described. 4,12 As a generalization, treatment decisions are influenced by the severity of the deformity, which can be generally graded as mild, moderate, and severe. 20 The amount and quality of evidence comparing procedures for each of these degrees of deformity varies considerably, with prospective Level I evidence often lacking. In 2006, a group of surgeons responsible for resident education were surveyed to determine the standard of practice for “mild” and “severe” forms of HV. 17,18 They found that in mild HV, there was a high degree of consensus that a distal chevron osteotomy is the optimal treatment. In contrast, there was no consensus regarding the optimal treatment for severe HV as surgeons were divided between 3 options: a metatarsal osteotomy, a metatarsal phalangeal joint arthrodesis, and a Lapidus procedure.
Since 2006, a considerable number of studies have been published that provide Level I evidence for various operative procedures for the treatment of HV. 4,11,19,22,24 However, the degree to which this data has created a consensus regarding what procedures are best suited for the treatment of HV of various severities is unknown. Thus, the purpose of this study was to determine in which stages of HV there exists a consensus regarding optimal treatment and to assess if the presence of higher levels of evidence is correlated with greater degrees of consensus. We hypothesized that stages of HV for which Level I studies exist would correlate with greater degrees of consensus and that stages of HV for which new Level I research has been published since 2006 would exhibit higher degrees of consensus compared to more than a decade ago.
Methods
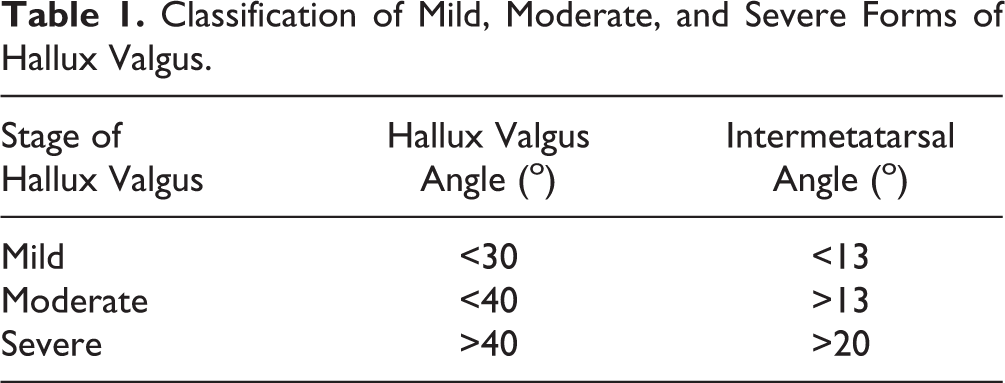
A total of 922 members of the American Orthopaedic Foot & Ankle Society (AOFAS) were contacted by e-mail to participate in this study. Participants were e-mailed a unique anonymous link to a 14-item survey. Severities of HV were defined by intermetatarsal and hallux valgus angles (IMA and HVA) (Table 1). 20 The first case in the survey was that of a hypothetical 50-year-old woman with a left forefoot deformity with no second ray symptoms. Films were provided that showed a mild HV deformity. Participants were then asked to select which treatment they would choose from a list of options provided. A variation of this case was then provided in which the difference in the clinical vignette was that the patient had second metatarsalgia (SM). Although there are a host of factors that influence operative decision making in hallux valgus, we wanted to limit the variables to some degree for the purposes of the survey, and we felt that SM was a sufficiently common problem so as to warrant inclusion. Participants were given a more extensive list of potential treatment options when SM was present (Table 2).
Classification of Mild, Moderate, and Severe Forms of Hallux Valgus.
Treatment Options Presented for Hallux Valgus.
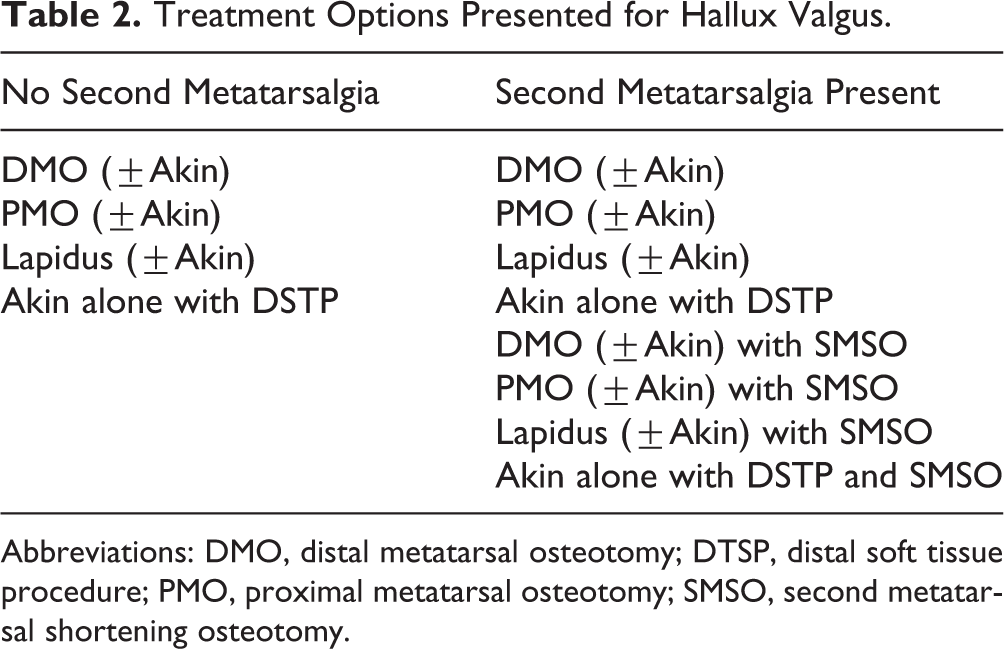
Abbreviations: DMO, distal metatarsal osteotomy; DTSP, distal soft tissue procedure; PMO, proximal metatarsal osteotomy; SMSO, second metatarsal shortening osteotomy.
Two subsequent cases were provided of 58- and 62-year-old females with films displaying moderate and severe HV, respectively, neither of which had a hypermobile first ray. Variations of each case with and without SM were provided as in the first mild case. The format of the survey and images used for the 3 stages of HV are available in the appendix.
Further questions not presented in the form of a case regarding physician operative preference were also included. Participants were asked to name their distal metatarsal osteotomy (DMO) and proximal metatarsal osteotomy (PMO) of choice if and when they perform each, as well as the type of fixation that they would use in each from a list of options (Table 3). Participants were permitted to enter choices separate from those provided for fixation type. Preferred fixation in a Lapidus procedure was also assessed. Participants were asked if they had completed a foot and ankle fellowship after residency, and what percentage of their practice is specific to foot and ankle surgery.
Fixation Choices Given for Proximal and Distal Metatarsal Osteotomies, and Lapidus Procedure.

Physicians were sent a reminder e-mail 2 weeks and 1 month after the initial e-mail if they did not complete the survey. Incomplete surveys or surveys where typed responses were invalid were excluded, as well as surveys where participants selected that 0% of their practice involved foot and ankle surgery.
A literature search was conducted on MEDLINE in order to determine the number of studies constituting Level I evidence pertaining to mild, moderate, or severe HV, as well as the efficaciousness of different forms of DMOs and PMOs. This was done by using the keywords “(bunion OR hallux valgus) AND (mild OR moderate OR severe) OR (proximal OR distal) AND metatarsal osteotomy).” Studies were excluded that did not constitute Level I evidence as defined by the Journal of Bone & Joint Surgery (American Volume) in 2003, studies that did not analyze cohorts of patients separated by severity of HV according to the classifications of mild, moderate, and severe, and studies that did not analyze osteotomies according to their anatomical location of proximal or distal. 26 Analysis of correlation of the presence (yes/no) of Level I studies pertaining to each of these 3 forms of HV (mild, moderate, severe) and the 2 osteotomies (DMOs, PMOs) was then conducted with respect to the presence of a greater than 50% consensus being reached by respondents for 1 answer choice in each of these 5 categories. It was also assessed whether Level I evidence was associated with the most popular answer choice being of a higher magnitude.
Statistical analyses were performed using SAS (version 9.1; SAS, Inc, Cary, NC). Correlations between categorical and continuous variables were conducted via chi-square analysis and Pearson correlation coefficient, respectively. Significance was set at a P value of 0.05.
Results
A total of 189 surgeons completed part or all of the survey for a response rate of 20%. From these 189 responses, 50 responses were excluded due to an incomplete survey. There were 8 entries in which participants indicated that 0% of their practice included foot and ankle surgery and were thus excluded. This left 131 surveys for analysis, yielding a response rate of 14%. A foot and ankle fellowship had been completed by 80% of respondents. On average, 68% ± 33% (median: 85%) of respondents’ practice was specific to foot and ankle.
“Mild” Hallux Valgus
When no SM was present 80% of respondents chose a DMO with or without (±) an Akin procedure as their preferred treatment. When SM was present, a DMO ± Akin procedure with a second metatarsal–shortening osteotomy (SMSO) was selected as the most appropriate treatment by 56% of respondents (Table 4).
Treatments Selected for Mild, Moderate, and Severe Hallux Valgus With and Without Second Metatarsalgia.

Abbreviations: DMO, distal metatarsal osteotomy; DTSP, distal soft tissue procedure; PMO, proximal metatarsal osteotomy; SMSO, second metatarsal shortening osteotomy.
“Moderate” Hallux Valgus
The most common treatment choice, a PMO ± Akin procedure, was chosen by 52% of respondents. When SM was present in moderate HV, none of the treatment options were chosen by more than half of the respondents, with a PMO ± Akin procedure with a SMSO being the most common choice by 34% of respondents (Table 4).
“Severe” Hallux Valgus
A greater than 50% consensus was only reached when no SM was present. When no SM was present, 53% of surgeons chose a Lapidus procedure ± Akin procedure. When SM was present, 48% of respondents chose a Lapidus procedure ± Akin procedure with a SMSO (Table 4).
Distal Metatarsal Osteotomies
A chevron osteotomy was favored by 80% of surgeons when performing a DMO, followed by a Mitchell osteotomy. The most frequently preferred fixation for DMOs were noncannulated headed screws by 33% of surgeons, followed by cannulated headless screws by 28% of surgeons (Table 5).
Distal and Proximal Metatarsal Osteotomies: Preferred Techniques and Fixation.

Abbreviations: CH, cannulated headed; CHL, cannulated headless; DMO, distal metatarsal osteotomy; K, Kirschner; NCH, noncannulated headed; NCHL, noncannulated headless; PMO, proximal metatarsal osteotomy.
Proximal Metatarsal Osteotomies
The most commonly chosen PMO was an opening wedge osteotomy (33%), followed by a scarf osteotomy (23%). The most commonly preferred fixation for PMOs was plate osteosynthesis by 39% of surgeons, followed by noncannulated headed screws by 24% of surgeons.
Lapidus Fixation
When asked what their preferred fixation type was for a Lapidus procedure, the respondents made the following selections: plate osteosynthesis (43%), noncannulated headed screws (24%), cannulated headed screws (20%), cannulated headless screws (5%), does not do procedure (5%), and screw with plate (3%).
Literature Search
A total of 5 Level I studies were ultimately included for analysis. 4,11,19,22,24 Two of these studies pertained to mild HV, 2 pertained to DMOs, and 2 pertained to PMOs. None of the studies specifically analyzed moderate or severe HV.
Correlative Analysis
In the analysis of whether presence of Level I evidence was correlated with the presence of a greater than 50% consensus on one answer choice for questions pertaining to treatment preferences of mild, moderate, or severe HV, as well as PMOs and DMOs, chi-square analysis revealed that a statistically significant association did not exist (P = .47). Pearson correlation analysis similarly revealed no significant correlation between the presence of Level I evidence and a higher raw percentage value for the most popular answer choice (r = 0.33, P = .43).
Discussion
Hallux valgus is a common disease for which surgeons employ many and various treatments. Similar to other diseases that fall along a continuum in orthopedics and lack standardized treatment algorithms, this study found that the stages of HV that have the greatest controversy with respect to optimal operative treatment are those in the middle of the spectrum. Higher-level evidence does not necessarily correspond with higher degrees of clinical consensus among surgeons. For each stage of HV, a panoply of procedures have been described, implemented, and studied. 4 Each of these procedures is different in design, indications, and level of evidence as related to outcomes. In 2006, the state of practice of a group of 128 foot and ankle surgeons was assessed with respect to 2 forms of HV: mild and severe. 17,18 In the 11 years since that study, a host of studies and systematic reviews have been published, and a select number of guidelines for the treatment of HV have been proposed. 15,24 The purpose of this study was to provide an updated perspective from a larger group of surgeons than previously studied on the current trends in the treatment of HV among foot and ankle surgeons and to assess if the presence of higher-level evidence corresponded with greater consensus.
Mild Halux Valgus
When treating a patient presenting with a mild form of HV, a majority of surgeons (80%) prefer a DMO to any other operative intervention. This result is similar to that of a previous survey in which 87% of surgeons surveyed elected to employ a distal chevron osteotomy for mild HV. Our results are not surprising as DMOs have been shown to be capable of achieving acceptable angular correction of the deformity, generally maintain the length of the great toe, and are viewed as technically less complex than PMOs. 2,13 Furthermore, of the 3 categories of HV, mild HV is the sole category that has specific Level I evidence evaluating operative treatments. Although the presence of Level I evidence did not significantly correlate with greater degrees of consensus, the sample size of this study for this correlative analysis was small, and it is nevertheless notable that mild HV was also the form of HV with the greatest degree of consensus at 87%.
Moderate Halux Valgus
Compared to mild HV, the treatment for moderate HV engenders a higher level of disagreement. When no SM was present, a PMO was the most favored procedure in moderate HV (52%) and was closely followed by a DMO or Lapidus procedure (24%). When SM was present, there was a relatively uniform shift in response choices to include an SMSO with each procedure. Unlike mild HV, there are no Level I studies that have evaluated moderate HV. The difficulty sometimes seen in grading a moderate HV as distinct from a mild or severe one may explain this lower level of consensus, but the nature and findings of the studies that do exist likely provide a better explanation. Within the prospective comparative procedural studies that do exist, conflicting results between studies have often been found. 4,6,7,15,19
Severe Halux Valgus
In the treatment of severe HV, surgeons appear evenly split between 2 treatment choices: a Lapidus procedure and PMO. This result is similar to that of a previous survey study, where 50% of surgeons opted for a PMO, 24% for a Lapidus procedure, and 26% for a metatarsophalangeal fusion. 18 We believe the split of opinions is not surprising and may, as in moderate HV, similarly be due to the nature and findings of current research. The lack of popularity of DMOs is expected, as DMOs provide less correction of the IMA. 16 No Level I evidence has been produced comparing PMOs to a Lapidus procedure in severe HV in the last decade. However, several retrospective studies have been published that compare the Lapidus procedure to PMOs in severe HV. 7,10 Overall, maintenance of correction and complication rates appears roughly equal between the two.
Correlation of Operative Procedure With Level of Evidence
Our investigation found that a large majority (80%) of surgeons preferred a distal chevron osteotomy as their DMO of choice. This level of consensus is the second largest seen in this study, and similarly pertains to a clinical scenario that has Level I evidence available. 22 The distal chevron osteotomy’s ubiquity in particular is likely not only due to the quality of evidence available but also to the frequency that it is taught to those in training and its relative technical ease. Finally, recent studies have found similarly equivalent results between the DMOs studied. 6,8,14
PMOs were not characterized by a degree of consensus similar to that of DMOs, despite their existing Level I evidence: the top 3 PMOs were opening wedge (33%), scarf (23%), and Ludloff (10%). Although the question was not provided in the setting of a clinical case, the opinions expressed by the respondents are potentially in contrast to the highest level evidence available. In 2013, a systematic review examined the angular correction and complications reported for PMOs. 23 Upon publication, the only PMOs with available Level I or II evidence were crescentic (I/II), proximal chevron (I), closing wedge (II), and Ludloff (II). With respect to HVA, crescentic osteotomy yielded the best correctional results, followed by Ludloff and proximal chevron. When complications were accounted for, the proximal chevron was deemed the procedure with the most favorable results. The relative technical ease of the opening wedge osteotomy may have a relatively large influence on surgeon preference. 5
The current study also assessed surgeon preferences with respect to fixation in 3 categories of surgeries: DMOs, PMOs, and a Lapidus procedure. Responses varied accordingly by procedure. In DMOs, 70% of surgeons opted for a screw of some variation as the mode of fixation. This is to be expected given that a distal chevron osteotomy was the most common DMO, and it has been shown that screw fixation is superior in this procedure. 1,11,25 In a PMO, the majority of surgeons also chose some variation of a screw as the mode of fixation, followed by a plate. These selections also are in line with the recommended mode of fixation for the procedures that were most popular in the PMO group. 5,25 In a Lapidus procedure, the nearly even split between a plate or variation of a screw reflects that both have been shown to be effective in the literature, although there is evidence to indicate that screws may be superior. 3,9
Limitations
There are several limitations to our study. First, the low response rate in this study may indicate that it is not a representative sample of the population of surgeons studied and also hampers its statistical utility. However, the number of surgeons surveyed is still greater than the number surveyed in previous studies on similar topics. 17,18 Second, the radiographic classification system used in this study, like many radiographic classifications, is not perfect. 20 It is possible that the interobserver reliability of the assessment of the IMA is imprecise and could thus influence our results. 21 However, the definitions used in this study are both widely used and accepted, and were useful in delineating 3 separate stages of HV. Third, in certain questions on the survey, there were a limited number of predetermined response choices. Although this limits how precisely the study allows readers to understand what the state of practice is, it allowed for comparisons between our results and Level I studies to be made, which often focused on these broader categories. Fourth, clinical decisions are made with more than radiographs and charts. It was not possible to capture an entire patient interaction in this study, and that is an inherent limitation to survey-based studies. Finally, we did not assess how dogmatic surgeons are in their approach; some surgeons have one type of HV operation that they vary to some degree based on the individual patient, whereas others do several different types of operations based on many factors.
Conclusion
The purpose of this study was not to determine the ideal treatment for each stage of HV; rather, we sought to evaluate the current trends in treatment of HV based upon degree of severity among a population of foot and ankle surgeons. We found that the degree to which practice is influenced by the most robust evidence available varies in the different stages of HV. The greatest consensus on appropriate treatment and specific operative technique appears to exist in mild HV and DMOs; there is also Level I evidence to support the treatments and techniques chosen. The presence of Level I evidence however did not uniformly translate to greater degrees of consensus in HV. This study should serve as a guide for future research with the aim of producing literature that addresses the areas of greatest controversy in the treatment of HV.
Supplemental Material
Supplemental Material, FAO800239-ICMJE - Evidence Versus Practice: Operative Treatment Preferences in Hallux Valgus
Supplemental Material, FAO800239-ICMJE for Evidence Versus Practice: Operative Treatment Preferences in Hallux Valgus by Peter C. Noback, David P. Trofa, and J. Turner Vosseller in Foot & Ankle Orthopaedics
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.