
Abstract
Background:
Total ankle arthroplasty (TAA) provides a surgical alternative to tibiotalar arthrodesis when treating end-stage ankle arthritis. TAA preserves range of motion at the tibiotalar joint leading to improved postoperative function. Many patients who undergo TAA wish to maintain a high level of activity, including participation in low-impact sports such as golf. There are several studies in the total hip and total knee arthroplasty literature that have looked at the effect of total joint arthroplasty on golf handicap. We hypothesized that similar to hip and knee arthroplasty research, TAA is likely to result in a postoperative increase in golf handicap.
Methods:
After obtaining institutional review board approval, we retrospectively identified 60 patients (from 140 consecutive TAAs performed between August 2016 and February 2017) who had undergone TAA, played golf pre- and postoperatively, and had at least 1 year of postoperative follow-up. The average postoperative follow-up for the cohort was 28.1 months. Variables including preoperative and postoperative golf handicaps, swing laterality, age, gender, surgical laterality, implant used, and operating surgeon were recorded.
Results:
The average preoperative and postoperative handicaps were 19.7 and 17.9, respectively, which did not represent a statistically significant difference (P = .07). Patients who played 3 or more rounds per week had better preoperative and postoperative handicaps compared to patients who played 2 rounds or less; however, the change in their handicap following TAA and the number of rounds played per week was not affected. There was no association between the change in handicap and the follow-up period, handedness of golf shot, surgical laterality, implant used, or the operating surgeon.
Conclusion:
Our findings showed that golf handicap was not negatively affected following TAA in this series.
Level of Evidence:
Level IV, case series.
Introduction
End-stage ankle arthritis (ESAA) is a disabling condition with patient morbidity approaching that of other debilitating disorders, including end-stage hip arthritis, congestive heart failure, and end-stage kidney disease. 4,27 Total ankle arthroplasty (TAA) was developed in the 1970s 23,26 and provides a surgical alternative to tibiotalar arthrodesis when treating ESAA. TAA preserves range of motion at the tibiotalar joint, leading to improved postoperative function. 5 Many authors have demonstrated superiority of TAA to arthrodesis with respect to postoperative function and patient reported outcomes. 8,19,24,25 Many patients who undergo TAA wish to maintain an active lifestyle including participation in low-impact sports such as golf, a sport that is played by 28 million American adults each year. 6 The majority of orthopedic surgeons have no objections to patients returning to golfing activities following total joint replacement 12,13,16 and active golfing has not been associated with an increased risk of postoperative complications. 1 The progressive inability to actively participate in sport is often cited as the main reason to pursue total joint arthroplasty. 12,13 For golfers undergoing total joint replacement, there is often a concern that the procedure will limit their participation in the sport or negatively affect their performance. 1 There are several studies in the total hip and total knee arthroplasty literature that have assessed the effect of total joint arthroplasty on golf participation, driving distance, and handicap. 1,6,12,13,17,28 The effect of total joint arthroplasty on postoperative handicap has been mixed, with some authors reporting a decrease in postoperative handicap 1,6,9,18 and others finding the postoperative handicap to increase. 1,12,13 We sought to determine the impact of TAA on postoperative golf handicap.
Materials and Methods
After obtaining institutional review board approval, we retrospectively identified 60 patients (from 140 consecutive TAAs performed between August 2016 and February 2017) who had undergone TAA, played golf pre- and postoperatively, and had at least 1 year of postoperative follow-up (Tables 1 and 2). Based on previous literature relating to golf performance and changes in handicap following total joint arthroplasty, a change of 2 strokes was deemed significant. Sample size analysis determined that 60 patients were required to achieve a power of 0.80 to detect this difference at a significance of .05. Variables including preoperative and postoperative golf handicaps (which patients self-reported from memory or by accessing their own scores through national databases), age, gender, swing laterality, surgical laterality, implant used and operating surgeon were recorded for each patient. Patients who had undergone associated simultaneous procedures at the time of TAA were excluded. Differences in categorical variables (gender, surgical laterality, swing laterality, surgeon) were compared using the chi-square test whereas differences in continuous variables (age, preoperative handicap, postoperative handicap, change in handicap, or frequency of play) were assessed using Student t test and 1-way analysis of variance. A P value less than .05 was considered statistically significant.
Patient Demographic Dataa

a Values are n (%) unless otherwise noted.
Patient Demographics and Preoperative Handicap.

Results
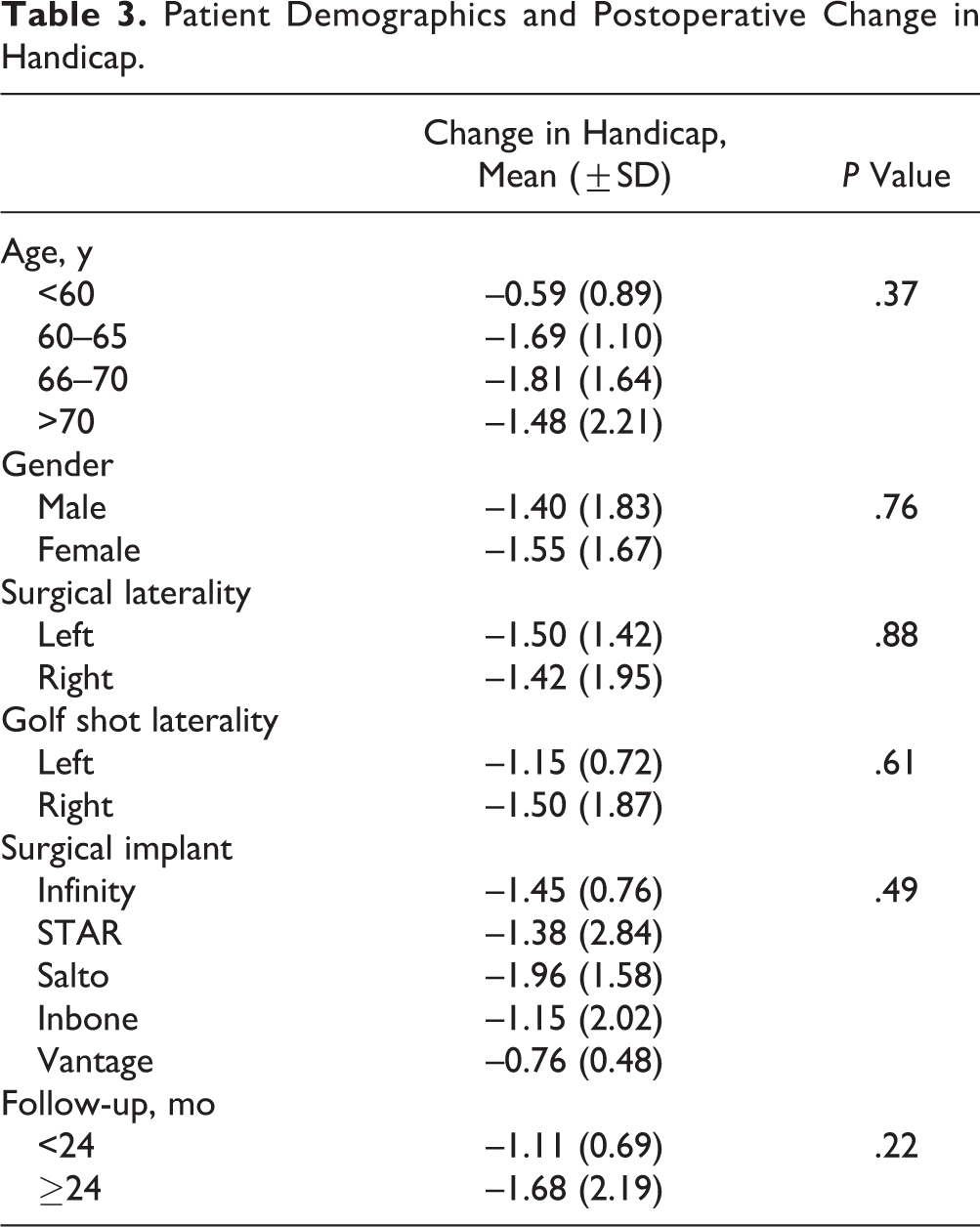
The average preoperative handicap was 19.68 (±5.69) and following TAA, the postoperative handicap was 18.22 (±5.21). Although a negative trend was observed, the difference did not reach statistical significance (P = .07). There were 5 total ankle systems used in this cohort: 20% of implants were the Scandinavian Total Ankle Replacement System (STAR; Stryker, Mahwah, NJ), 33.3% Salto Talaris (Integra LifeSciences, Plainsboro, NJ), 16.7% Vantage (Exactech Inc, Gainesville, Florida), 16.7% Infinity (Wright Medical Technology, Memphis, TN), and 13.3% were INBONE (Wright Medical, Memphis, TN) implants. There was no association between patient age, gender, golf shot laterality, surgical laterality, implant system, surgeon, and the change in handicap (Table 3). Although the average number of rounds played preoperatively and postoperatively were similar at 2.58 (±0.67) and 2.83 (±0.87), respectively (P = .08), there was a statistically significant association between the number of rounds played and the preoperative and postoperative handicaps. Patients who played more than 2 rounds per week had lower preoperative and postoperative handicaps compared to patients who played 2 rounds or fewer (see Table 4). However, there was no difference in the change in handicap between these 2 groups.
Patient Demographics and Postoperative Change in Handicap.
Handicap and Rounds per Week (Mean [±SD]).

*P < .05.
Discussion
Golf is a low-impact sport that can contribute to cardiovascular health, endurance, and flexibility. 10,21 Although total joint replacement has been shown to improve function and patient satisfaction, previous reports in the arthroplasty literature have found that golf handicaps can increase up to 5 strokes following lower extremity joint replacement (Table 5). 1,6,13 In contrast, in this current cohort, we found that golf handicaps were not negatively influenced following TAA and actually demonstrated a trend toward improvement. A possible explanation for this difference between our results and previous findings in the total knee arthroplasty (TKA) and total hip arthroplasty (THA) literature may be the importance of hip and knee motion relative to ankle motion in the recreational golfer. The hips internally and externally rotate during the backswing, generating up to 20% of the overall work, 17 and the new hip joint following THA may not be able to re-create the golfer’s learned preoperative mechanics—leading to altered swing mechanics, decreased accuracy and distance, and as a result, an increase in postoperative handicap. In addition, electromyographic studies have shown greater activation in the buttock and thigh muscles during a golf swing when compared to the muscles acting about the ankle, and this difference was greater in the high-handicap recreational golfer. 14 Significant rotational torque occurs about both knees during the golf swing and is highest about the leading knee at the time of impact. 13 In addition, following TKA, a significant proportion of patients experience midround pain. Taken together, these findings may explain the rise in handicap seen in the THA and TKA patient population and the relative increase in handicap following TKA performed on the leading knee when compared to the trailing knee. 12 Two studies looking at postoperative golf handicap following shoulder arthroplasty (TSA) found that players improved their handicap by 1.4 to 5 strokes. 9,18 The modern golf swing is described as being high-torque and relying on a large shoulder turn. In addition, unskilled golfers utilize their upper limb to a greater extent when compared to their low-handicap counterparts. 11,15 The ankles are typically planted and relied on for balance, allowing the upper extremity to perform a greater percentage of the total swing. These findings may explain why elderly, recreational golfers may be able to maintain or improve their postoperative handicaps following TAA and TSA but tend to experience an increase in handicap following THA and TKA.
Studies Addressing Total Joint Replacement and Change in Golf Handicap.

Abbreviations: THA, total hip arthroplasty; TKA, total knee arthroplasty; TSA, total shoulder arthroplasty.
We did not encounter any patients who were not able to return to golf following TAA and the number of rounds played per week did not change. In contrast, 10% and 33% of patients undergoing THA and TKA, respectively, were unable to return to play following total joint arthroplasty. 1 -3,22 This difference may be explained by residual discomfort and pain following THA and TKA or by the general health of patients undergoing TAA compared to patients undergoing TKA and THA. Ankle arthritis is usually post-traumatic in origin and, as a result, patients undergoing TAA may be younger and have fewer comorbidities restricting participation in sports following joint replacement. 4,20 This may also explain why TAA patients were able to return to the sport with a greater frequency compared to patients after TKA and THA.
Our results showed that in this patient population, preoperative and postoperative handicap and the change in handicap were not affected by the age of the patient. This is in keeping with previous studies which found that although relatively younger adults were shown to have greater club head speed compared to older adults, this did not translate to a difference in baseline handicap. 7 In addition, our study found that on average, patients who played more than twice per week had better handicaps compared to players who played less than 2 rounds. This difference was found both pre- and postoperatively. Although we know that increased practice and repetition improves performance, these findings are the first to show that elderly recreational golfers who play more frequently have, on average, better handicaps. More importantly, however, this study shows that following TAA, both groups of patients are able to return to the same frequency of play and can expect their handicaps to return to preoperative levels.
There are several limitations to this study: although our sample size was larger than several previously published reports, 1,9,12,13,18 a larger study group and increased statistical power may have been able to detect a significant improvement in postoperative handicap. In addition, a larger group may have been able to better detect an association between the change in handicap and the follow-up period, surgical laterality or the implant used. Furthermore, our study did not involve a control group. It may be interesting to compare the change in golf handicap following TAA versus the change seen following ankle arthrodesis or comparing fixed and mobile bearing total ankle implants. Radiographic and clinical outcomes could be considered and compared between golfers and nongolfers to determine whether playing golf has any impact on loosening rates, postoperative pain, or function. In addition to documenting the change in handicap, we could question patients on the use of a golf cart, their pain while playing and after playing, or the ease of a shot based on the club used. We did not question patients on their preoperative and postoperative satisfaction with respect to golf and their handicap, but this may be important future consideration. Patients were asked their handicap during their follow-up clinical visit and although we did not verify their scores through national databases, 83.3% of patients recorded their scores following each round. Regardless, there is always the possibility for recall bias or even that the patient would want to embellish their scores.
Conclusion
In summary, for the recreational golfer undergoing TAA, handicap and playing frequency do not appear to be negatively affected.
Supplemental Material
Supplemental Material, FAO790094-ICMJE - Keeping It in the Fairway: Golf Handicap Following Total Ankle Arthroplasty
Supplemental Material, FAO790094-ICMJE for Keeping It in the Fairway: Golf Handicap Following Total Ankle Arthroplasty by Michel A. Taylor, James R. Lachman, Samuel B. Adams, James A. Nunley, and James K. DeOrio in Foot & Ankle Orthopaedics
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: James K. DeOrio, MD, reports personal fees from Wright Medical and Exactech, during the conduct of the study. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.