
Abstract
Background:
Stiff equinocavus deformities of the foot are challenging to treat, often requiring extensive soft tissue dissection and bone removal. These procedures frequently yield suboptimal results and not infrequently amputation. Minimally invasive surgery using a circular external fixator potentially avoids the trauma to the soft tissue and may lead to improvement in outcomes and a lower amputation rate. The objective of this study was to evaluate the efficacy of minimally invasive surgery using a circular external fixator and limited soft tissue release to correct stiff equinocavus deformities.
Methods:
The treatment outcome of 29 patients (31 feet) with stiff equinocavus deformities of the foot and ankle treated with minimally invasive surgery and circular external fixation were reviewed after a mean follow-up period of 63 months. Patients’ demographics and cause of the deformities were recorded. Weight bearing radiographs of the foot were compared pre and postoperatively.
Results:
Outcome was satisfactory (plantigrade foot with improvement/resolution of pain) in 21 of 31 extremities, fair in 6 of 31 extremities, and poor in 4 of 31 extremities. In the majority of patients, a significant improvement in the equinocavus deformities was achieved with a statistically significant improvement in calcaneus and navicular height. Two patients with Charcot-Marie-Tooth and severely insensate feet had a poor outcome, resulting in transtibial amputation.
Conclusion:
Minimally invasive surgery with gradual correction of neglected stiff equinocavus deformities using a modular circular external fixator is a reliable initial limb salvage strategy. Minimally invasive surgery and gradual correction of neglected severe stiff equinocavus deformities using the modular circular external fixator to gradually correct neglected severe stiff equinocavus deformities, is a safe initial limb salvage strategy which may simplify secondary procedures such as arthrodesis.
Level of evidence:
IV.
Keywords
Introduction
Severe neglected stiff foot and ankle deformities are still an unfortunate reality in developing countries, where access to medical care is not always readily available. Road traffic accidents are quite common in developing nations, as pedestrians, bicycles, motorcycles, and all other vehicles share the same road with little policing. The lower limbs are especially exposed to trauma in these situations. 1,14 Chronic neglected medical conditions involving the peripheral or central nervous system are also a source of foot and ankle deformities. 16,17,31 The lack of timely and adequate medical treatment and rehabilitation can lead to severe sequelae. 16,31
Conventional operative techniques to treat severe foot and ankle deformities involve a 1-stage procedure intended to address all the components of the deformity. 3,9,25,26,28,33 Such procedures are associated with a high risk of vascular and soft tissue complications, because deep scarring and retraction involving the posterior-medial neurovascular bundle of the foot and ankle from previous surgeries are common. 3,22,27,33 Arthrodesis with deformity correction usually involves extensive dissection of soft tissue, multiple osteotomies removal of large bone wedges, with increased risk of skin and bone necrosis and/or infection, 10,24,25,27 as well as excessive shortening of the foot and limb, leading to imbalance on the contralateral side. 2,3,5,20,25
Stiff equinovarus deformities (ECDs) of the foot are mostly caused by neglected trauma, 14,29 burns, 19,27 compartment syndrome of the leg, 5,14,16 peripheral nerve injury, 31 and central nervous system lesions. 2,23,26,30 These cosmetically challenging and functionally incapacitating deformities are common in developing countries. Moreover, because of the equinus position, these deformities are often associated with chronic metatarsalgia and/or forefoot plantar ulcers, especially in those patients with reduced sensitivity, increasing the risks of infection and amputation. 17,31 This is particularly true in cases where there is scarring, shortening, and adhesions of the posteromedial neurovascular bundle of the foot, such as after severe lower extremity trauma, compartment syndrome, 1,5,14 -16 burns, 19,27 previous surgeries, 5,19 late effects of paralytic disease, 9,17,20,24,30,32 and chronic vascular disease. 1,6,25 Poor skin quality/multiple scars, joint stiffness secondary to arthrofibrosis, shortening of the foot, claw toes, and neglected or mistreated childhood osteoarticular deformities can further complicate efforts to achieve a plantigrade foot. 1,2,3,5,10 -13,18,19,22,23 -26,28,29
Gradual and progressive correction of these severe deformities, using the distraction-osteogenesis principle proposed by Ilizarov 21 delivered through an external circular fixator, is a less invasive, yet highly effective, alternative in such cases. 5,12,13,15 According to Ilizarov, both soft tissue and bone can grow in response to gradual progressive controlled distraction force. 21 Daily adjustments to the rods that connected the rings allow controlled accommodation of the tarsal bones after they had been disimpacted, without requiring any osteotomy, as long as there is sufficient space within the joints. 4,12,13,15
The objective of this retrospective chart review was to evaluate the efficacy in achieving satisfactory correction of severe neglected stiff equinocavus deformities with minimally invasive surgery using a circular external fixator and limited soft tissue release.
Material and Methods
Over a 17-year period (1993-2010), 54 patients (60 feet) with severe neglected stiff equinocavus deformities were surgically treated at a tertiary care teaching institution. Only patients with a minimum follow-up period of 12 months who were treated after skeletal maturity were included in the study.
A total of 29 patients (31 feet), 18 males and 11 females, met the inclusion criteria. The mean age of the studied population at the time of surgery was 32 years (range 18-54 years). The mean postoperative follow-up period was 63 months (range 12-218 months). A variety of etiologies were present in the studied population (Table 1).
Patient Demographics, Early Complications, and Final Outcome.
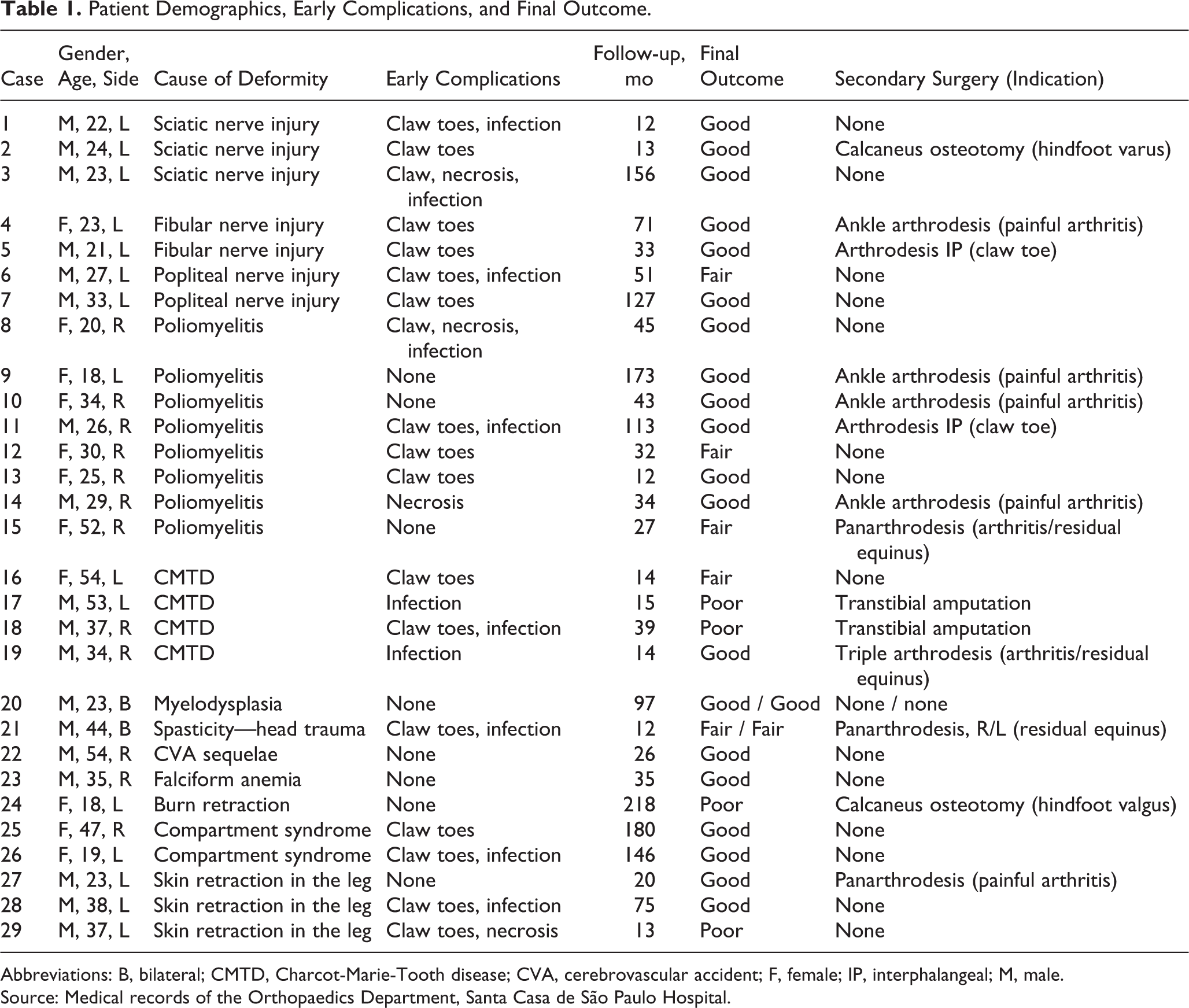
Abbreviations: B, bilateral; CMTD, Charcot-Marie-Tooth disease; CVA, cerebrovascular accident; F, female; IP, interphalangeal; M, male.
Source: Medical records of the Orthopaedics Department, Santa Casa de São Paulo Hospital.
Radiographic Assessments
The magnitude of the equinus and cavus deformities and treatment outcome were assessed on a weight-bearing lateral radiograph of the foot, using the following parameters developed by the authors : (1) calcaneus-to-ground distance—the distance, in centimeters, between the inferior cortex of the posterior calcaneus and the ground (Figure 1); and (2) height of the navicular—the distance, in centimeters, between the perpendicular line drawn from the inferior cortex of the navicular bone to the line drawn from the inferior aspect of the calcaneal tuberosity to the center of the head of the first metatarsal bone (Figure 1). A calcaneus-to-ground distance >4.0 cm indicated severe equinus deformity and was an inclusion criterion for this study (Figure 1). A height of the navicular >3.0 cm indicated severe cavus deformity; this, however, was not an inclusion criterion.

Profile (A) and lateral (B) photographs and radiographs of the left foot of patient 28, who presented a severe and stiff equinocavus deformity as a sequelae of poliomyelitis. Lines H and h marked on the radiographs (B and D) and on the photograph (C) represent the calcaneus-to-ground distance and the height of the navicular, respectively. These measurements were used to assess the severity of the deformity.
Outcome Measures
A successful outcome comprised the following: (1) patients achieved a plantigrade foot; (2) the heel was completely in contact with the ground and there was a significant visual clinical improvement in gait (improvement in limp and ability to bear weight on the entire foot sole); and (3) the equinocavus deformity was corrected; that is, the radiographic calcaneus-to-ground distance became zero (to the ground) and there was a reduction in the navicular height of at least 1.0 cm. The first 2 variables were examiner dependent; the third variable was obtained by comparing the pre- and postoperative weight-bearing radiographs.
The treatment outcome was categorized as good when all 3 outcome variables were achieved successfully, fair when 2 of the 3 outcome variables were achieved, and poor if only 1 or no outcome variables were successfully achieved.
Minor complications commonly reported in the treatment of foot and ankle deformities with an external fixator, 7,12,13 such as pin tract infection, skin necrosis with distraction, and claw toe deformity, were also noted.
Surgical Technique
Surgical treatment consisted of (1) a percutaneous tenotomy of the Achilles and tibialis posterior tendons, and plantar fascia and short plantar muscle release, (2) a transverse osteotomy of the midfoot via a single dorsal longitudinal incision performed in case of ankylosis or previous midtarsal joint fusion (talonavicular, calcaneocuboid and/or intercuneiforms), and (3) gradual realignment of the foot and ankle using a standard circular foot frame with 3 independent segments interconnected by rods—one for the leg, one for the hindfoot, and another one for the forefoot 12 -14 (Figure 2).

Lateral photographic view of the left foot of patient 28 in the immediate postoperative period of the CEF device placement for correction of the deformities (A and C) and after 3 months of progressive correction (B and D).
Postoperative Protocol
Correction was started 7 to 10 days after surgery. Patients remained hospitalized to allow adjustments of the setting twice a day. To prevent any complication during the entire period of treatment, the speed of the deformity correction was adjusted according to the symptoms the patient reported and medical judgment, following 3 subjective clinical parameters such as pain, edema, and ischemia of the toes. Patients also underwent daily physical therapy consisting of ambulation with crutches without weight bearing to avoid contractures of the knee and hip during the entire period of foot and ankle distraction treatment. After 8 to 10 weeks, patients were reassessed clinically, and a goniometer was used to establish if the angle between the longitudinal axis of the leg and the plantar surface of the foot had achieved the target of 90°.
At this point, any additional correction in the rotational alignment of the mid- and forefoot (pronation and supination deformities) and/or correction of claw toes was carried out under anesthesia. To achieve correction of the rotational deformities, the lateral rods connecting to the half rings of the forefoot and hindfoot were temporarily released and the foot was manipulated into a slightly hypercorrected position. The lateral rods were then reconnected and an additional anterior rod was placed connecting the leg rings to the foot half rings to lock the frame, which stabilized the correction achieved and closed the leg-hindfoot-forefoot-leg connection (Figure 2). Clawing of the toes was corrected through percutaneous tenotomy of the flexor tendons (Figure 3).

Frontal photographic view of the right foot of patient 13 showing the alignment achieved after correction of the claw toe deformity with percutaneous tenotomy of the flexor tendons and internal fixation with Kirschner wires.
Following this procedure, patients were released from the hospital and observed at 4 weekly follow-ups. The frame was in place for an average of 12 weeks. Weight bearing was not allowed during the entire corrective period because the equinus deformity did not allow the heel to touch the ground until it was completely corrected. After removal of the external fixator, the extremity was immobilized in a short leg plaster cast with full weight bearing as tolerated for 6 weeks, followed by a molded rigid thermoplastic foot and ankle orthosis for an additional 6 months.
Statistical analysis was carried out to compare the pre- and post-operative radiographic results using Wilcoxon test, with the significance level established at P <.05.
Results
Twenty-one of the 31 (68%) extremities with severe stiff equinocavus deformity had a good outcome (Figure 4), 6 (19%) had a fair outcome, and 4 (13%) had a poor outcome. Two of the 4 feet with poor outcomes were amputated because of complex regional pain syndrome.
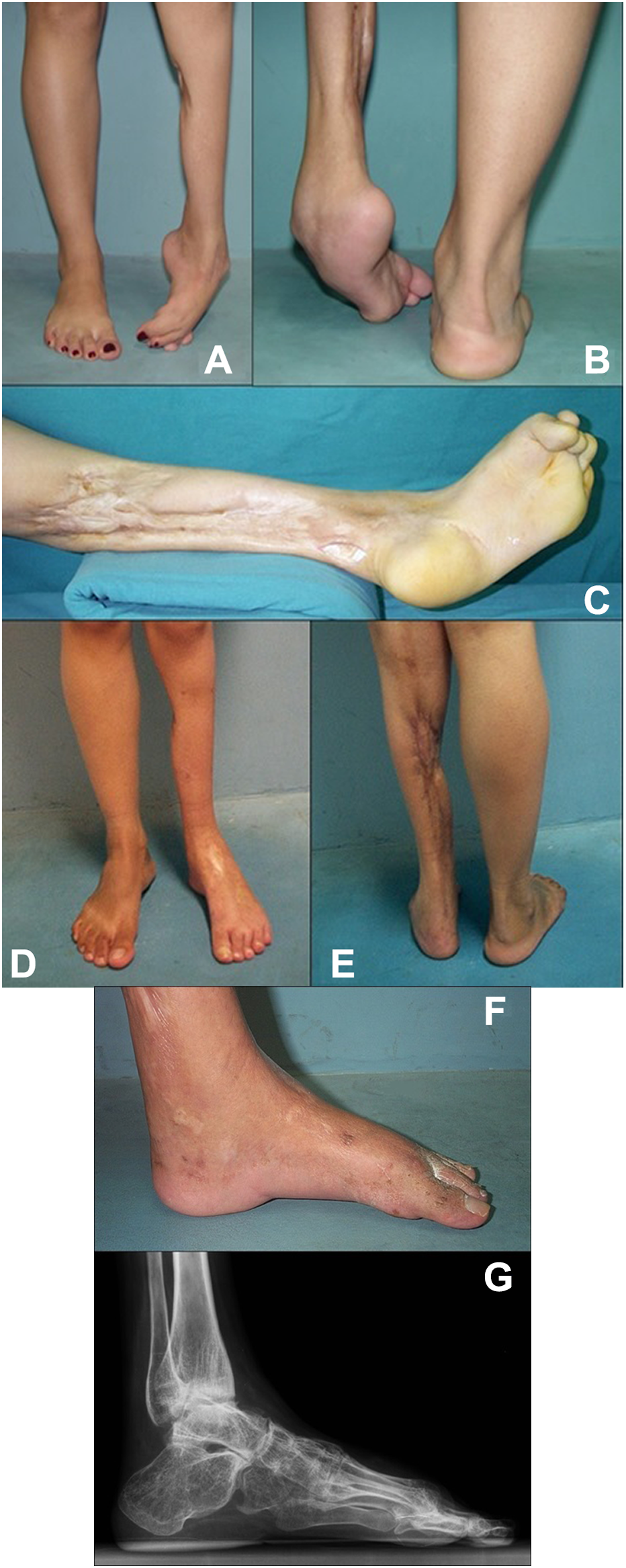
(A-E) Preoperative photographs of a patient with a left leg sequelae of compartment syndrome caused by snake bite (case 26). One may note on the frontal (A) and posterior (B) views, that the left foot is plantigrade. Panel C shows a severe scar retraction of the posterior calf. At 48 months after treatment with the circular external fixator, the left foot is plantigrade (D, E). (F, G) At 48 months after treatment with the circular external fixator, the left foot is plantigrade (F). The lateral radiograph (G) shows a satisfactory alignment in the plantigrade position of the foot and a global reduction in the joint spaces of the ankle and tarsal joints characterizing global ankyloses.
A statistically significant improvement in the equinus deformity was observed by the difference between the preoperative (median 10 ± 2.9 cm, range 4.0-15.0 cm) and postoperative (median 0.4 ± 0.8 cm, range 0-4.0 cm) radiographic calcaneus-to-ground distance (P < .001). The same was observed for the correction of the cavus deformity, as measured by the radiographic navicular height (median preoperative, 4.2 ± 1.1 cm, range 3.5-7.0 cm; median postoperative 3.6 ± 1.1 cm, range 0-5.4 cm) (P < .001).
Postoperative radiographs revealed that at the completion of treatment 13 of the extremities had developed signs of extensive spontaneous ankylosis involving either the foot or the ankle. The reason for these findings was not completely understood, because no operative intervention was made to fuse any foot and ankle joint during the course of the treatment.
Secondary surgeries were necessary in 14 of 31 feet, half for minor residual deformities and the other half for symptomatic late arthritis (Table 1, Figure 5). Five of the major joint fusions were indicated to treat residual pain associated with late arthritis on average 68 months (range 20-173) after the index treatment. Another 4 feet required major joint fusion to correct minor residual deformity, 2 of these also had painful arthritis. The later feet were operated on average 16 months (range 12-27) after the index procedure.

Preoperative photographs (A and B) and lateral radiograph (C) of the right foot and ankle of case 15, who presented sequelae of poliomyelitis. Note that the patient only bears weight on the plantar surface of the forefoot. Following 27 months of treatment with the circular external fixator, the foot is plantigrade with a mild residual equinus deformity (D and E). On the lateral view radiograph, one can observe a reduction in the joint spaces of the ankle and midfoot (F). This patient underwent a modeling panarthrodesis; panels G and H show the result after 60 months of this additional corrective procedure, whereas panel I shows the lateral radiographic image with complete pantalar fusion.
Discussion
Surgical treatment in this extremely challenging patient population can be somewhat daunting. Traumatic nerve injury can cause paralysis of distinct muscle groups of the leg and is commonly associated with selective loss of the protective sensation of the foot leading to chronic ulcers. 14,31 This insensitivity is an additional risk factor when using the external fixator for correction of the resulting equinocavus deformity, as pin tract infections tend to be more frequent. 7,12,13 This partial loss of sensitivity in the extremity caused by incomplete nerve injury can be associated with chronic pain and complex regional pain syndrome. 31
Neglected deformities in patients who had high-energy trauma with extensive skin loss/degloving of the leg and foot with sequelae of compartmental syndrome including severe muscular retractions and extensive circumferential scars adhered to deep layers of tissue usually are elective for below-the-knee amputation because conventional operative treatment involves too many variables and delivers disappointing outcomes. 8,14,20 It has been speculated that the quality of life and clinical outcome of patients with severe sequelae from trauma to the lower extremity are better treated with transtibial amputation than in those treated with salvage surgery, 8,14,20 and the functional performance of an individual with a stiff foot is worse than that of an amputee using a leg prosthesis. 8,20 However, one must also take into account the smaller energy requirement for gait and the patient’s self-image with a preserved limb. In developing countries, the cost of acquiring and maintaining the leg prosthesis must also be considered, in addition to the aspects involving the cultural notion of disability that amputation may afford in some cultures. 14 Further scarring and fibrosis involving the anterior and posterior tibial arteries poses an enormous challenge for conventional operative approaches, especially when significant bone must be removed to achieve correction of the deformities. 25,26,28,32 The use of the circular external fixator in such cases allows gradual daily distraction of the soft tissue, including the blood vessels, thus minimizing such risks. Based on these limited series of cases, one can offer an alternative treatment option for patients with stiff equinocavus deformity as encouraging positive clinical results have been found. Because the correction of severe deformities was achieved through minimal invasive surgery using circular external fixator with low major complications rates, it is possible to consider this treatment option relatively safe and reliable.
Minimally invasive surgery with percutaneous Achilles tenotomy and plantar fasciotomy followed by progressive joint and soft tissue distraction with circular external fixation achieved full correction of the severe and stiff equinocavus deformities, with a good outcome in 68% (21/31) of the extremities, partial correction and a fair outcome in 19% (6/31) of the treated extremities, and a poor outcome in 13% (4/31) of the extremities.
After the index equinocavus deformity correction using minimal invasive surgery with circular external fixation, additional procedures were occasionally necessary in the following cases: (1) patients who achieved satisfactory correction of the deformities and plantigrade foot but developed symptomatic arthritis requiring arthrodesis, either in situ or with minimal bone resection; (2) patients who did not achieve complete correction of the deformities and plantigrade foot and required some deformity correction with arthrodesis; (3) patients who had their limb amputated because of a poor functional outcome or a complication of the underlying medical condition.
Although secondary surgeries were common, they were far less extensive than would be needed without the fixator. These results are especially satisfying when one takes into consideration the severity of the baseline deformities. The radiographic improvement was also significant for both the calcaneus-to-ground distance and the height of the navicular bone. The correction of the equinus deformity with the CEF was dramatic, but the correction of the cavus (although statistically significant) was visibly subtle.
Conclusion
Minimally invasive surgery with gradual correction of neglected stiff equinocavus deformities using a modular circular external fixator is a reliable primary limb salvage strategy which may simplify secondary procedures such as arthrodesis.
Supplemental Material
Supplemental Material, FAO789370-ICMJE - Minimally Invasive Surgery Using the Circular External Fixator to Correct Neglected Severe Stiff Equinocavus Foot Deformities
Supplemental Material, FAO789370-ICMJE for Minimally Invasive Surgery Using the Circular External Fixator to Correct Neglected Severe Stiff Equinocavus Foot Deformities by Ricardo Cardenuto Ferreira, Marco Túlio Costa, Cleber Lotti, and Lysie Pistorello in Foot & Ankle Orthopaedics
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.