
Abstract
Congenital dislocation of the fifth metatarsophalangeal (MTP) joint can cause significant limitations in a patient’s ability to wear a closed shoe. Historic treatment has involved amputation of the digit or attempts at reconstruction. These techniques have had limited success with unreliable correction and/or unacceptable cosmesis. The authors present a detailed, methodical approach to reconstruction of this deformity with a stepwise algorithm that addresses both the bony and soft tissue components of the deformity. With this modern technique, reliable and satisfactory results can be expected.
Introduction
It is difficult to ascertain the prevalence of congenital dislocation of the fifth metatarsophalangeal (MTP) joint because symptoms are so variable. It has been described as being asymptomatic in up to 50% of patients born with the anomaly. 20,29,32 However, when it is symptomatic, the pain can be chronic and severe, and the correction is difficult.
The deformity of congenital dislocation of the fifth MTP joint is complex. It is multiplanar, consisting of adduction of the fifth toe, varus at the MTP joint, and severe dorsiflexion of the MTP joint, with variable degrees of dorsal subluxation to the extreme of an irreducible, fixed, and complete dislocation. There is always multi-planar soft tissue contracture of the MTP joint capsule and both the flexor and extensor tendons. 6 Less well described is the dysmorphism of the osseous structures, and the attenuation or loss of the plantar plate, as demonstrated in the illustrative case provided below.
Chronic, congenital dislocation of the fifth MTP joint may present in adulthood as a result of the difficulty the patient has with the pressure of shoes against the elevated toe. The diagnosis is typically made by the clinical appearance of the toe in a dorsally dislocated, varus position with crossover of the fourth toe. The diagnosis is then confirmed with weightbearing anteroposterior (AP), oblique, and lateral radiographs of the foot. These radiographs must be closely inspected for abnormal morphology of the fifth metatarsal head, dorsal migration of the proximal phalanx, and varus alignment of the MTP joint. In children, conservative treatment with stretching and taping has had mild success and there are reports of percutaneous techniques for reduction. 11,22 However, in adults, the options are either shoe modification or operative reconstruction. 19,32
Multiple operative techniques for treatment of a symptomatic congenital dislocation of the fifth toe have been described. In the past, amputation was offered as a simple operative solution. However, this was not without sequelae. Beyond aesthetic concerns, patients could develop painful callus under the deformed metatarsal head, valgus drift of the lesser toes, lesser toe hammering, and/or lesser toe metatarsalgia. 14 Other operative techniques have been developed to attain a better functional and cosmetic result. These techniques have focused on soft tissue release alone and have not been demonstrated to have long-term success and reproducibility. We present a stepwise approach to the operative correction of chronic, congenital dislocation of the fifth MTP joint in an adult patient that focuses on the principles of deformity correction through contracture release, soft tissue balancing, and osseous decompression of the dysplastic fifth MTP joint.
Technique
The patient is placed supine with a bump under the ipsilateral hip. The foot and ankle are prepped and draped in a typical, sterile fashion. An Esmarch bandage is used as a tourniquet above the malleoli. A single, curvilinear incision from distal to the proximal interphalangeal (PIP) joint with oblique or transverse central section at level of MTP joint is recommended to reduce dorsal contracture. Following subcutaneous dissection, the PIP joint is resected (both the proximal and middle phalanges articular facets) with a micro-oscillating saw, adjusting alignment of the toe through position of saw cuts as needed. An open tenotomy of the flexor digitorum longus is performed through this space. Fixation of the PIP arthrodesis is performed with a pair of 0.035-inch (0.89-mm) Kirschner wires for rotational control. The pins are placed antegrade through the middle phalanx and then retrograde into the proximal phalanx. Fluoroscopic control is used to ensure acceptable alignment.
Attention is then turned to the MTP joint. A Z-lengthening of the extensor tendon is performed, followed by a proximal, transverse incision of the periosteum of the distal fifth metatarsal shaft, and continuing with elevation of the capsule of the fifth MTP joint in order to leave this cuff of tissue attached to the dorsum of the base of the proximal phalanx. The fifth metatarsal head is inspected for shape and condition of the articular cartilage. Release is done with a gouge-shaped elevator. If there is severe loss of cartilage and an irregularly shaped metatarsal, reshaping with a rongeur to a more rounded configuration may be done.
To adequately realign the MTP joint, the joint must be decompressed and the insufficient plantar plate must be addressed. This technique involves a shortening metatarsal osteotomy and direct repair of the plantar plate. 12,17,25 A modified Weil osteotomy is performed with an oscillating saw and a section of the bone is removed to offset the plantar displacement that occurs as the metatarsal head is shifted proximally at the osteotomy.
The plantar plate is inspected. In the setting of chronic dislocation, the plantar plate tissue will be attenuated or fibrotic. The remnant of the plantar plate is reconstructed using two 2-0 nonabsorbable sutures passed twice through medial and lateral sides of the distal plantar plate, and then through 2 vertical drill tunnels in the medial and lateral corners of the base of the proximal phalanx. 5,9,24,25,33
The length of the metatarsal is determined by the tension of the soft tissues, judged after the sutures are tied to secure the plantar plate to the proximal phalanx. The osteotomy is fixed with a 2.0-mm cortical screw. Reconstruction of the capsule is then done, also using 2-0 nonabsorbable suture. Medial and lateral pants-over-vest sutures are placed from the plantar capsular tissue to the cuff of tissue attached to the dorsum of the phalanx, or to drill holes in the phalanx.
Next, the previously tenotomized flexor digitorum longus is identified at the level of the proximal phalanx through the original dorsal dissection. It is retrieved and transferred to the base of the proximal phalanx and sutured to the extensor hood and dorsal soft tissue. This adds a plantar-directed force to hold the phalanx reduced on the metatarsal. The extensor tendon is then repaired at its new length with 2-0 absorbable suture (Figure 1).
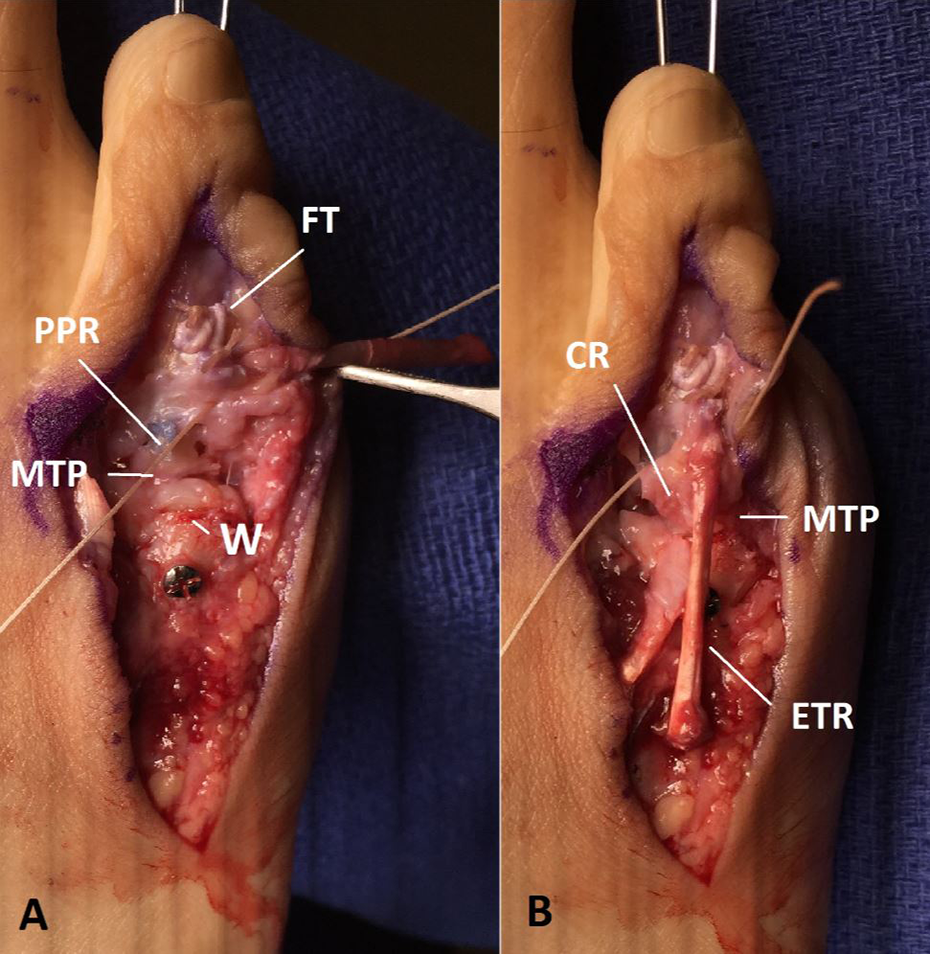
(A) Intraoperative photograph of the reduced fifth metatarsophalangeal MTP joint after Weil osteotomy (W), plantar plate reconstruction (PPR), and flexor transfer. (B) To complete the procedure, a capsular reconstruction (CR) is performed and the extensor tendon is repaired (ETR). FT, flexor transfer; MTP, metatarsophalangeal.
The tourniquet is released and hemostasis obtained to prevent dorsal hematoma. The skin is closed using inverted, interrupted, deep dermal 3-0 monofilament, absorbable suture followed by 3-0 nonabsorbable monofilament for the skin. A soft compression dressing is applied and the patient placed into a protective postoperative shoe. Preoperative and postoperative radiographs are demonstrated in Figures 2 and 3, respectively. A stepwise summary of the procedure is included as Figure 4.

Preoperative lateral (A), anteroposterior (B), and oblique (C) radiographs of a patient with a chronic dislocation of his fifth MTP. There is dorsal dislocation of the fifth MTP joint with varus and adduction deformity. There is a dysmorphic appearance of the metatarsal head. MTP, metatarsophalangeal.

Postoperative lateral (A), anteroposterior (B), and oblique (C) radiographs after successful reconstruction of the fifth MTP joint at 4 wk. MTP, metatarsophalangeal.

Diagram of a stepwise approach for reconstruction of a congenital dislocation of the fifth MTP joint. MTP, metatarsophalangeal.
At the end of procedure the reconstructed toe may remain pale due to spasm of the digital vessels caused by lengthening of the chronic deformity. Reperfusion may take a few minutes and the authors recommend patience. If the toe does not return to similar rubor of the adjacent digits, placing the patient in a reverse Trendelenburg position can encourage dependent flow to the digits. Warming blankets can be applied over the foot to also encourage reperfusion.
If the toe fails to reperfuse after these measures, the dressing should be released to ensure it was not placed too tightly. Topical calcium channel blockers or nitroglycerine paste may be applied directly to the digit to encourage local vasodilation. There is no specific literature regarding the efficacy of such topical vasodilators in this clinical situation. However, there is evidence of a vasodilatory benefit from such topical agents in animal models, diabetic wound healing, and microvascular surgery management of vasospasm. Further study in this patient population is warranted, but is difficult due to the infrequent nature of persistent digital ischemia. 3,13,26,31,34,35
Ultimately, if the toe continues to remain poorly perfused, consideration can be given to removing the K-wire. The authors urge patience and have not experienced issues with failure of reperfusion in a healthy adult that does not have significant microvascular disease.
Postoperative Protocol
The patient is kept full time in the rigid postoperative shoe and non-weightbearing protection for 4 weeks. The pins are removed from the toe at 6 weeks, followed by gradual resumption of wide and open shoes to minimize pressure on the operative area.
Discussion
Congenital dislocation of the fifth MTP joint is a complex deformity that requires meticulous and thoughtful operative technique. In comparison to treatment of traumatic dislocations, operative correction of chronic deformity is difficult and the results less reliable. 15 Dysplasia of the fifth metatarsal head adds to the difficulty of achieving a durable and concentric reduction. Chronic dislocation leads to a variable combination of a dysmorphic metatarsal head, contracted capsule, plantar plate insufficiency, and contracted flexor and extensor tendons. These deforming forces contribute to superior, varus, and rotational deformity of the MTP and potential rigid hammering of the digit. Our described technique addresses these concerns through contracture release and soft tissue balancing, but also relies on the necessary decompression of the joint itself with shortening of the metatarsal. Historic techniques have focused on soft tissue releases, which are largely inadequate in the setting of prolonged, chronic deformity.
In 1940, Lantzounis proposed an operative correction aimed at rebalancing the soft tissues via capsulotomy and lengthening of the extensor tendon and plantar capsulorraphy. This was performed in mostly pediatric patients, and he reported varied success. 20 The DuVrie’s procedure uses a dorsal incision at the fourth webspace and release of the medial capsule, extensor tendon, and dorsal skin. It is only practical in minor deformity and does not adequately correct severe disease that results in a dysplastic, tight MTP joint. 6,10 In 1942, Lapidus described soft tissue release and transfer of the extensor tendon to the abductor digiti quinti to balance the deformity. 21 Butler’s operation for this condition was developed in the 1960s, which involved a double-limbed dorsal and plantar incision with extensor lengthening and relocation of the toe. 4 This procedure may be satisfactory in children whose contractures are not as severe and tissue may be more accommodating. 2,7 Zanoli’s procedure involves dorsal soft tissue release and transfer of the fifth extensor to the fourth. Minimal data exist to show its efficacy in severe, chronic deformity. 8 Other modifications have been made to address such a fifth toe deformity by soft tissue release alone and have not been shown to have long-term success or reproducibility. All of these procedures address soft tissue contracture and do not address any of the resultant bony deformity that results after years of chronic deformity. 1,18,27,30
The Ruiz-Mora procedure has also been described for correction of overriding fifth toe deformity. 28 It involves resection of the proximal phalanx and subsequent soft tissue balancing to reduce the symptoms of a dorsally migrating fifth toe. One study reported on 31 Ruiz-Mora procedures performed for painful dorsal fifth PIP corns. It observed great relief of their presenting pain, but many patients developed fifth metatarsalgia, bunionette deformity, or adjacent hammering of the fourth digit. 16 Another study reported on the long-term results of this procedure in 12 patients. The procedure was successful at symptom relief; however, there was significant dissatisfaction because of the cosmesis of the shortened digit. 11 Although the technique uses osseous decompression, resection of the phalanx rather than shortening of the metatarsal can cause excessive shortening, and floppiness of the toe, which have been shown to have negative cosmetic results and possible subsequent painful deformity.
The described technique in this manuscript allows for adjustable decompression of the joint because the metatarsal osteotomy can be variably shortened, making more accurate the rebalancing of the soft tissue. We have had excellent cosmetic and functional results in 4 toes (2 patients) using this technique without any recurrence of deformity or symptoms. This technique can be broadly applied to other chronic, lesser MTP dislocations with modifications as needed per each individual deformity.
Prior reports of operative correction have not used nonabsorbable suture. Nonabsorbable synthetic suture has been shown to have a significantly higher load to failure than commonly used braided, absorbable suture. 23 The authors recommend use of deep, nonabsorbable suture as we believe this stronger suture has the potential to improve long-term satisfaction and prevent future recurrence of the deformity. Prospective research is warranted to validate its benefit in forefoot surgery, but we believe it may contribute to a more reliable, long-term outcome.
Operative correction of this deformity requires meticulous handling of the soft tissues, thorough understanding of the soft tissue and bone deformities, and attention to detail. We believe the stepwise approach described addresses the critical components of this deformity. Contracture release and soft tissue reconstruction is not adequate for severe and chronic deformity that results in a dysplastic MTP joint. The key components of this deformity correction include capsular contracture release, extensor tendon lengthening, redirection of the flexor tendon, plantar plate reconstruction, and joint decompression. All of these factors must be considered and addressed to obtain correction of the deformity and achieve satisfactory symptom relief and cosmetic result.
Conclusion
Reconstruction of congenitally dislocated fifth toe is a technically challenging procedure. We propose a new, thorough stepwise approach to include decompression by metatarsal shortening, combined with direct plantar plate reconstruction, and soft tissue balancing that applies new methods to this age-old operative conundrum.
Supplemental Material
Supplemental Material, FAO782488-ICMJE - Congenital Dislocation of the Fifth Metatarsophalangeal Joint in Adults: Operative Technique
Supplemental Material, FAO782488-ICMJE for Congenital Dislocation of the Fifth Metatarsophalangeal Joint in Adults: Operative Technique by David E. Jaffe and James W. Brodsky in Foot & Ankle Orthopaedics
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.