
Abstract
Displaced calcaneal fractures encompass a spectrum of fracture patterns, many of which are associated with soft tissue complications. Displaced tongue-type calcaneal fractures often cause pressure on the posterior heel skin, particularly when treatment is delayed. Resultant partial- or full-thickness skin necrosis presents significant challenges to the treating surgeon. In this article, the authors report on a case of full-thickness skin necrosis associated with a displaced tongue-type calcaneus fracture. The authors describe the use of a specialized heel window casting technique, which eliminates posterior heel pressure and greatly facilitates soft tissue surveillance and local wound care. The article also reviews the literature on soft tissue complications associated with displaced calcaneus fractures.
Introduction
Tongue-type calcaneal fractures represent 14% to 20% of all calcaneus fractures. 8,10 They can occur as an isolated fracture line or as part of a more complex, intra-articular calcaneus fracture pattern. These injuries require urgent reduction and fixation in order to minimize soft tissue compromise from the pressure of the displaced tuberosity fragment on the posterior heel skin. 10,18
If presentation, diagnosis, or surgical intervention is delayed, resultant partial- or full-thickness skin necrosis can lead to devastating complications, including amputation. 10 After reduction and fixation, the surgeon must balance the need for close soft tissue surveillance and wound care with the need for immobilization to facilitate bone and soft tissue healing. Short-leg casts, splints, and removable prefabricated braces all limit access to the posterior heel and can apply pressure to the already tenuous posterior soft tissues. This is exacerbated by the fact that traditional techniques employed by patients to elevate the foot or ankle typically involve resting the injured limb on a stack of pillows or blankets.
We present a case report and technical description of a novel short-leg casting technique that relieves posterior heel pressure while adequately immobilizing the foot and providing access to the heel for soft tissue monitoring and wound management.
Case Description
A 39-year-old 1-pack-per-day smoker was transferred to our hospital with a left displaced tongue-type calcaneus fracture (Figure 1A). The injury occurred when he landed on his feet after falling from a height of 10 feet. There was ecchymosis at the fracture site, and the posterior heel skin was taut but intact. He underwent percutaneous reduction and internal fixation using two 4.5-mm fully threaded cortical screws placed using lag technique with washers (Figure 1B). He was discharged to home on postoperative day 2 in a bulky padded short-leg splint with the ankle in a resting equinus position. A skin check prior to discharge revealed a small fracture blister but otherwise viable skin over the posterior heel. Smoking cessation was strongly recommended in order to maximize his likelihood of soft tissue and fracture healing.

(A) Lateral radiograph of the patient’s left foot on the date of injury, demonstrating a displaced tongue-type calcaneus fracture. (B) Immediate postoperative radiograph showing anatomic reduction and fixation with 2 fully threaded 4.5-mm cortical screws with washers.
At his first scheduled appointment on postoperative day 10, he admitted to having fallen at home on the day of discharge. A 1.5-cm × 2-cm area of full-thickness skin necrosis was noted at the posterior heel (Figure 2A). Radiographs were obtained and revealed loss of fixation (Figure 2B). He was taken to the operating room urgently for revision percutaneous reduction and fixation using two 6.5-mm partially threaded cannulated screws with washers (Figure 2C). With the ankle in resting plantarflexion, he was placed into a modified short-leg plaster splint with a posterior heel window and plaster strut that permitted the heel to rest free of pressure (Figure 3A–C). On postoperative day 2, a skin check revealed a stable area of skin necrosis, and he was placed into a modified short-leg fiberglass cast with a posterior heel window and fiberglass-wrapped aluminum strut to entirely eliminate heel pressure (Figure 4). The ankle remained in a position of resting plantarflexion, and a borderless Mepilex AG (Mölnlycke, Norcross, GA) dressing was applied to the posterior heel.
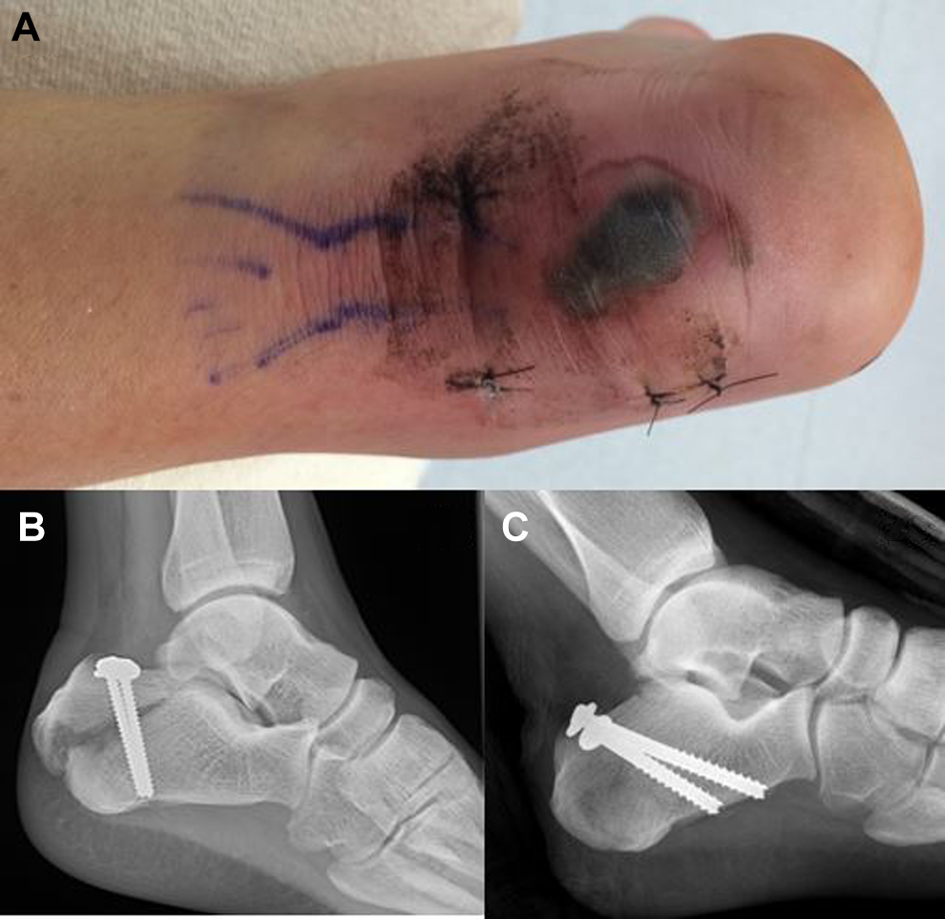
(A) Clinical photograph and (B) lateral radiograph of the patient’s left heel 10 days after index fixation. The patient admitted to having fallen at home on the day of discharge. (C) Immediate postoperative lateral radiograph after revision percutaneous reduction and internal fixation with 2 partially threaded 6.5-mm cannulated screws.

Technique for applying the modified short-leg splint/cast with posterior heel window and strut (A-C, splinting; D-I, casting). (A) A towel is used to create a potential space over the posterior heel that allows application of a plaster posterior slab splint with the heel free. (B) A window in Jones cotton and Webril padding is made to keep the heel uncovered. (C) The towel is removed once the plaster hardens, leaving a strut to protect the posterior heel. (D) Stockinette is placed proximally and distally and wrapped with cast padding. (E) A large stack of 4″ × 4″ gauze is positioned over the posterior heel wound and wrapped with additional cast padding. (F) The desired position of the ankle is maintained while fiberglass cast material is applied, along with the addition of a foot plate. (G) Once the fiberglass has hardened, a posterior cast window is cut at the margins of the gauze bulge. (H) After the gauze is removed and tape is used to cover the cut fiberglass edges, 2-inch-wide aluminum splinting material is contoured to provide a supporting strut posterior to the heel. (I) The aluminum is overwrapped with fiberglass casting material and then secured to the cast proximally and distally with additional fiberglass.

Clinical photograph of the patient’s left heel after application of a modified short leg cast with a posterior heel window and fiberglass-wrapped aluminum strut, which entirely eliminates heel pressure.
Serial skin checks were performed weekly for the first 3 weeks, and a new borderless Mepilex AG dressing was applied each week. At the 3-week postoperative appointment, the patient was transitioned to a new modified fiberglass cast with a similar posterior heel window and strut, but this time with the ankle in neutral dorsiflexion. Weekly dressing changes were continued at home. At his 5-week postoperative appointment, the area of posterior heel necrosis was diminishing in size, the eschar had fallen off spontaneously, and there was vital-appearing granulation tissue at the wound base (Figure 5A). Radiographs at that time demonstrated interval fracture healing. A borderless Mepilex AG dressing was again applied to the wound, and he was placed into a well-padded fiberglass cast and allowed to initiate through-heel weightbearing. Progressive fracture healing and posterior heel epithelialization was seen at the 8-week postoperative appointment (Figure 5B), and the patient was transitioned to weight-bearing as tolerated in a walking boot with weekly borderless Mepilex AG dressing changes. By the 12-week postoperative visit, the posterior heel skin had fully epithelized and radiographs showed complete fracture healing (Figure 5C, D). The patient was transitioned to dry gauze dressings daily as needed and permitted to wear normal shoes. At 7 months postsurgery, he had full ankle range of motion, his posterior heel skin had fully epithelialized, and radiographs showed complete healing of the fracture (Figure 6A–D).

(A-C) Clinical photographs demonstrating progressive healing of the posterior soft tissue injury at 5, 8, and 12 weeks following revision percutaneous reduction and internal fixation. (D) Lateral radiograph at the 12-week mark demonstrating stable fixation and progressive fracture healing.

(A, B) Clinical photographs demonstrating the patient’s left ankle range of motion in maximum active dorsiflexion and plantarflexion. (C, D) Clinical photograph and radiograph of the patient’s left heel 7 months after revision fixation demonstrating complete soft tissue and bony healing.
Description of Casting Technique
Written informed consent to present radiographs and clinical pictures was obtained from the patient. The casting technique is depicted in Figure 3D–I. Stockinette is placed proximally and distally and wrapped with cast padding (Figure 3D). A large stack of 4″ × 4″ gauze is positioned over the posterior heel wound and wrapped with additional cast padding (Figure 3E). The desired position of the ankle is maintained while the padding is applied. The leg is wrapped with fiberglass casting material with the addition of a foot plate (Figure 3F). Once the fiberglass has hardened, a posterior cast window is cut at the margins of the gauze bulge (Figure 3G). After the gauze is removed and tape is used to cover the cut fiberglass edges, 2-inch-wide aluminum splinting material is contoured to provide a supporting strut posterior to the heel (Figure 3H). The aluminum is overwrapped with fiberglass casting material and then secured to the cast proximally and distally with additional fiberglass (Figure 3I). The rigid posterior supporting strut protects the heel soft tissues from pressure and contact.
A modification of this casting technique using plaster can be applied in the operating room, as depicted in Figure 3A–C. Jones cotton was applied to the leg and a posterior window was made in the cotton over the heel. A rolled-up towel was used to create a potential space over the heel. A posterior plaster splint is applied and molded over the towels, maintaining the ankle in plantarflexion (Figure 6A). The towel roll is then removed, leaving a plaster strut with no pressure on the heel (Figure 3B, C).
Discussion
The soft tissue challenges and complications of calcaneus fractures have been well described for displaced intra-articular fractures. 15,24 However, the subset of tongue-type fractures has received less attention in the literature. For many displaced intra-articular calcaneus fractures, the degree of soft tissue swelling requires delaying definitive fixation until swelling subsides. 20 On the other hand, tongue-type calcaneus fractures, like displaced tuberosity avulsion fractures, often require urgent operative intervention to alleviate pressure on the threatened posterior heel skin. 10,13,17
The operative treatment of displaced tongue-type calcaneus fractures by percutaneous techniques has been well described. 23 This approach minimizes further injury to threatened soft tissues. However, soft tissue compromise can still occur. In a series of 139 operatively treated tongue-type calcaneus fractures, 21% had some degree of soft tissue compromise. 10 Factors associated with soft tissue compromise included degree of displacement, smoking status, and referral from another institution. Soft tissue complications after delayed treatment of calcaneal tuberosity fractures have also been described in the literature. 11,13,16 In a series of 33 operatively and nonoperatively treated calcaneal tuberosity avulsion fractures, 39% had soft tissue complications, and 27% of operatively treated fractures had fixation failure. 11
There is paucity of literature describing management strategies for threatened posterior heel skin associated with tongue-type calcaneus fractures. A case report from 1969 describes a walking cast with a heel window and metal stirrup to protect a calcaneus fracture while weight-bearing, but this technique was not designed to address posterior heel soft tissue compromise, and the area off-loaded by the stirrup was the plantar surface of the heel, not the posterior heel. 5 The benefit of a posterior heel window for soft tissue surveillance in the treatment of calcaneal tuberosity fractures has been described, but no specific techniques for cast application or posterior soft tissue pressure relief are provided. 3 In the care of diabetic foot ulcers, a walking cast utilizing an off-loading plantar window has been shown to produce improved outcomes compared to removable off-loading devices. 6,12 Similarly, metal stirrups have been used as a modification to a total contact cast to allow weight-bearing in the cast while unloading a plantar diabetic ulcer. 22 Our technique is unique in that it off-loads the skin over the posterior heel and calcaneal tuberosity to allow effective extremity elevation and soft tissue surveillance. External fixation techniques have likewise been described to protect soft tissue reconstruction procedures about the heel, 7,19 but considerations including cost, complications, and necessity for removal in the operating room make these techniques less favorable.
Soft tissue complications are common after fixation of calcaneus fractures, affecting 18% to 33% of intra-articular calcaneal fractures treated operatively. 1,2,9 Although tongue-type calcaneus fractures are often classified with intra-articular fractures, these injuries share soft tissue considerations similar to those encountered in the treatment of calcaneal tuberosity fractures, which have a soft tissue complication rate of nearly 40%. 11 Fractures of the calcaneal tuberosity tend to occur from low-energy mechanisms in older diabetic patients with osteoporotic bone, 4 whereas tongue-type fractures commonly occur in the setting of high-energy trauma. 10 Nevertheless, both fracture patterns are associated with high rates of soft tissue complications, specifically involving the posterior heel tissues.
Our case highlights important considerations in the management of both tongue-type calcaneus fractures and calcaneal tuberosity fractures. Percutaneous techniques for fixation were employed to minimize further injury to the threatened posterior soft tissues. 23 Unfortunately, fixation failure occurred in our patient, presumably after a low-energy fall at home with subsequent delay in presentation and diagnosis. A review of 139 tongue-type calcaneus fractures did not comment on loss of fixation, 10 but a case series of 22 operatively treated calcaneal tuberosity fractures reported a 27% rates of fixation failure. 11 Our patient was successfully treated with revision percutaneous fixation and frequent, diligent posterior soft tissue wound management and pressure relief, which was facilitated by the described casting technique. Since the successful treatment of this patient, we have applied the same casting technique in several other patients with compromised posterior heel soft tissues resulting from trauma.
Although some authors advocate for early range of motion without immobilization following operative treatment of tongue-type calcaneus fractures, 23 our case illustrates a situation in which immobilization and soft tissue access for wound management were critical. The described casting technique provides appropriate immobilization while simultaneously permitting access to the posterior heel soft tissues for wound surveillance and management. In addition, it provides a strut that allows patients to elevate the injured extremity on a pillow without direct pressure on the heel. This is in contrast to a dorsal plantarflexion splint, which would eliminate heel pressure from a cast but would leave the posterior heel unprotected and at risk for further injury, particularly when the leg is elevated on a stack of blankets or pillows. Our technique also allows for the effective use of a silicone-layered foam dressing impregnated with silver, which has been shown to be an effective modality in the prevention and treatment of pressured-related heel ulcers. 14,21,22 Modifications of this casting technique may prove useful for other calcaneal fracture patterns as well as hindfoot soft tissue reconstructions, postoperative Achilles wound complications, and diabetic foot care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.