
Abstract
Background:
Individuals with limited health literacy often struggle in effectively communicating with their physicians and may lack the skills needed to make informed health decisions. It is therefore important that providers have insight into patients’ baseline medical knowledge, as this can help physicians customize their approach to, and conversations with, each patient. As such, this study evaluated the foot and ankle–specific knowledge of patients seeking care for various foot and ankle ailments.
Methods:
An unvalidated survey developed by our study group was distributed to 206 patients, assessing their knowledge of foot and ankle anatomy, terminology, conditions, treatment, and perioperative issues. Performance was evaluated as a function of participants’ demographic factors.
Results:
Participants performed significantly worse on the conditions and treatment questions as compared to the anatomy, terminology, and perioperative considerations subsections. Significantly better performance correlated with education (≥college), visit type (preoperative evaluation), a current or previous health care occupation, and prior orthopedic surgeon evaluation.
Conclusions:
Patients’ knowledge of foot and ankle anatomy, terminology, conditions, treatment, and perioperative issues correlates with certain patient characteristics and demographics. With enhanced insight into the risk factors for limited knowledge, education campaigns can be designed to target those most in need.
Introduction
Health literacy is a measure of one’s ability to obtain and process the basic health information and services needed to make informed health decisions. 2,10 Unfortunately, an estimated 33% to 68% of Americans have inadequate health literacy, which is troubling as limited health literacy impedes the effective dissemination and comprehension of relevant health information, and also complicates communication, compromises care, and leads to poorer outcomes. 1,7,9,10 In addition, poor health, worse control of chronic conditions, prolonged hospitalizations, the infrequent use of preventive services, an increased use of emergency services, and early death have also been associated with limited literacy. 10 Conversely, patients with adequate health literacy experience more effective and meaningful interactions with their physicians and are better equipped to make informed and appropriate treatment decisions. 3,14
Recent literature has demonstrated that many patients struggle with musculoskeletal-specific health literacy, which is defined by different competencies than those required for general health literacy; its terminology, conditions, and treatment modalities mandate an enhanced set of skills that include, but also exceed, those needed for general health literacy. 4,12,15 -17 Despite this, there are currently no studies evaluating specialty-specific knowledge in a foot and ankle population. 1,7,9,15 -18,19
Through the use of a questionnaire, this study investigated foot and ankle patients’ knowledge in the categories of foot and ankle–related terminology, anatomy, conditions, treatment, and perioperative considerations. It also evaluated the relationship between patients’ demographic factors and foot and ankle–specific knowledge. We hypothesized that age, education, race, health care experience, visit type, and prior visits to providers for foot and ankle complaints would influence questionnaire performance.
Methods
Following institutional review board approval, questionnaires were distributed to English-speaking adults (aged 18 years or older) presenting to the practices of our senior authors and our institutional Foot and Ankle Medicaid/Medicare Ambulatory Care Center (ACC) between October 1 and November 3, 2015. Inclusion was not limited to new patients, but also included individuals presenting for preoperative evaluations, postoperative visits, and nonoperative follow-up. Patients were informed of the study’s purpose and benefits of participation. It was emphasized that participation was voluntary, unrelated to the care they would receive, and that all results were anonymous. Patients were excluded if they did not meet the aforementioned criteria, if they had cognitive impairment, or were unable to read or write in English. Patients amenable to participation completed the survey in examination rooms, prior to being seen by a physician. Two hundred and six patients completed the Foot and Ankle Literacy Survey (FALS) (Figure 1). Table 1 summarizes subject demographic and baseline characteristics.
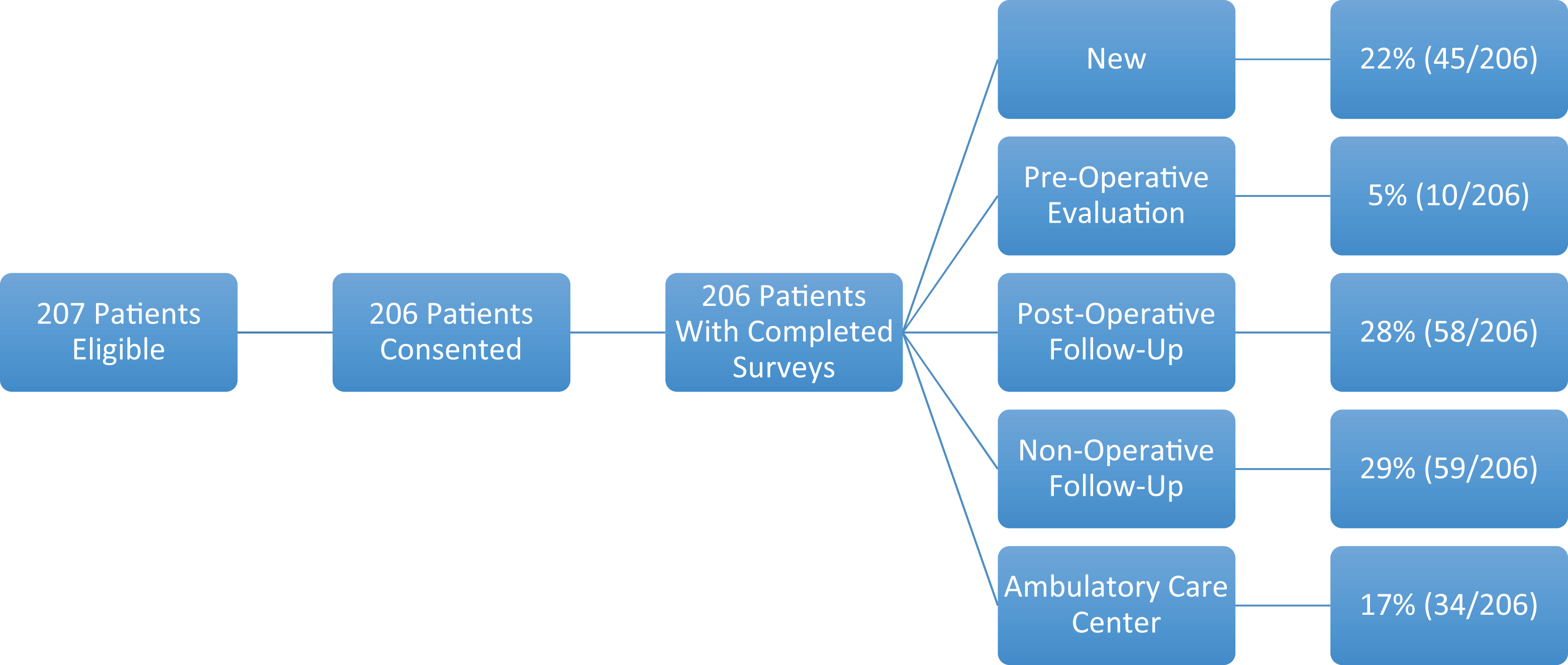
The breakdown of study participants’ visit types.
Participants’ Demographics and Baseline Characteristics.
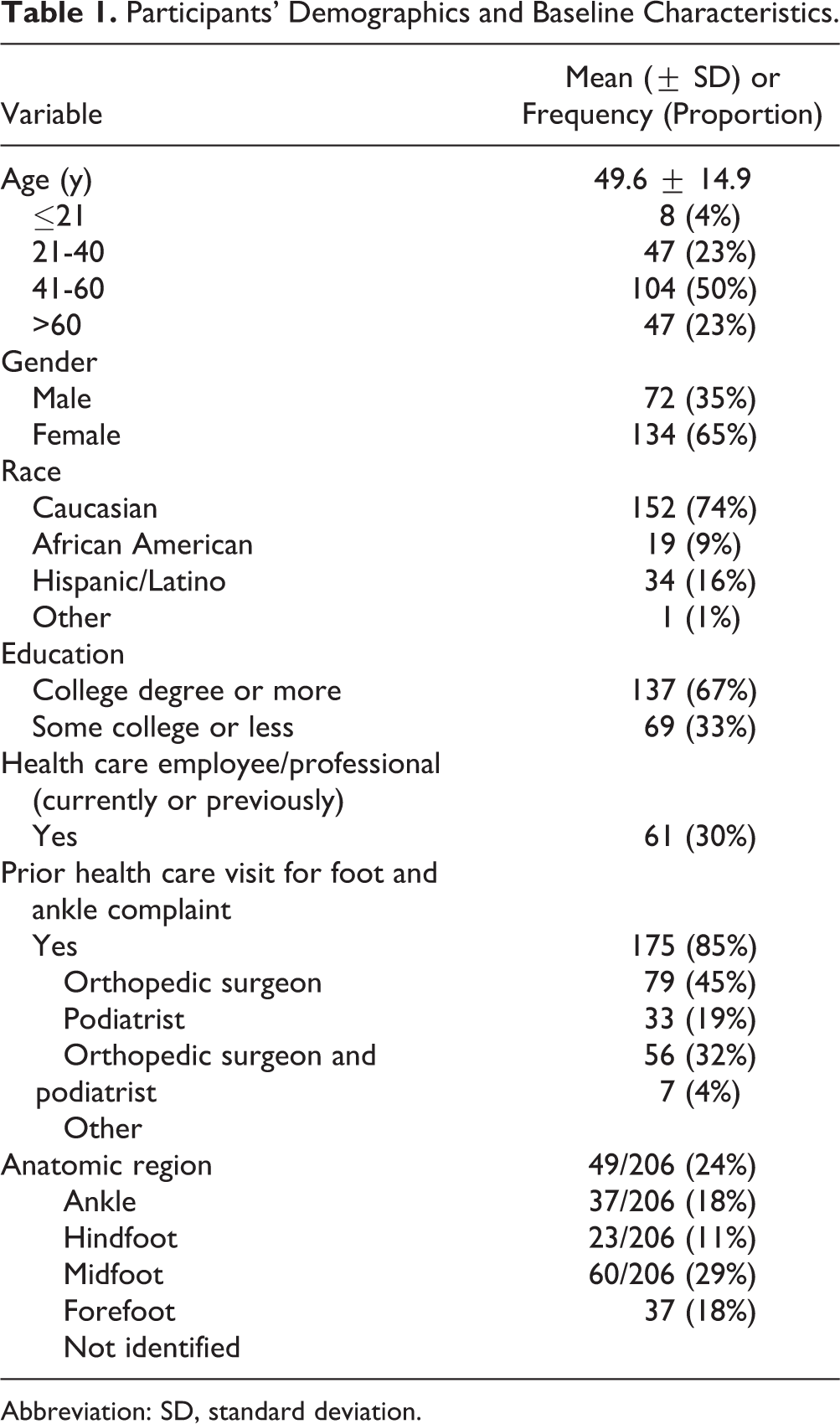
Abbreviation: SD, standard deviation.
Foot and Ankle Literacy Survey
The questionnaire, referred to as the Foot and Ankle Literacy Survey, was developed by our study group and was composed of 2 components. The first was a demographic section consisting of questions regarding age, gender, race, level of education, employment status, visit type (new patient, preoperative evaluation, postoperative visit, nonoperative follow-up, ACC), symptomatic anatomic region (ankle, hindfoot, midfoot, forefoot), and whether the patient had been seen previously by a health care provider for foot and ankle complaints.
The second component of the FALS consisted of 14 questions assessing patients’ foot and ankle knowledge (Figure 2). Questions were based on the following 4 categories, though were presented in mixed order: terminology, anatomy, conditions and treatment, and perioperative considerations (Table 2). These categories were chosen following our study group’s review of the most commonly emphasized themes within the American Orthopaedic Foot & Ankle Society’s (AOFAS’s) Internet-based patient education website, FootCareMD.org. 8 This approach to questionnaire design was derived from a prior study describing the development and validation of a musculoskeletal-specific health literacy assessment tool. 17 Of note, the FALS was written at a Microsoft Word–determined Flesch-Kincaid grade level of 4.5, as health care organizations such as the National Work Group on Cancer and Health, American Medical Association, and National Institutes of Health recommend the readability of patient education material to be no higher than a sixth-grade level. 5,13

The Foot and Ankle Literacy Survey (FALS). Questions 1, 5, 7, and 13 assessed patients’ knowledge of foot and ankle terminology. Questions 2, 4, 8, and 9 evaluated knowledge of conditions and treatment. Anatomy was assessed in questions 3, 6, and 14. Perioperative considerations were evaluated in questions 10, 11, and 12.
A Listing of Each Question, Corresponding Theme and Percentage of Respondents Who Answered It Correctly (n = 206).
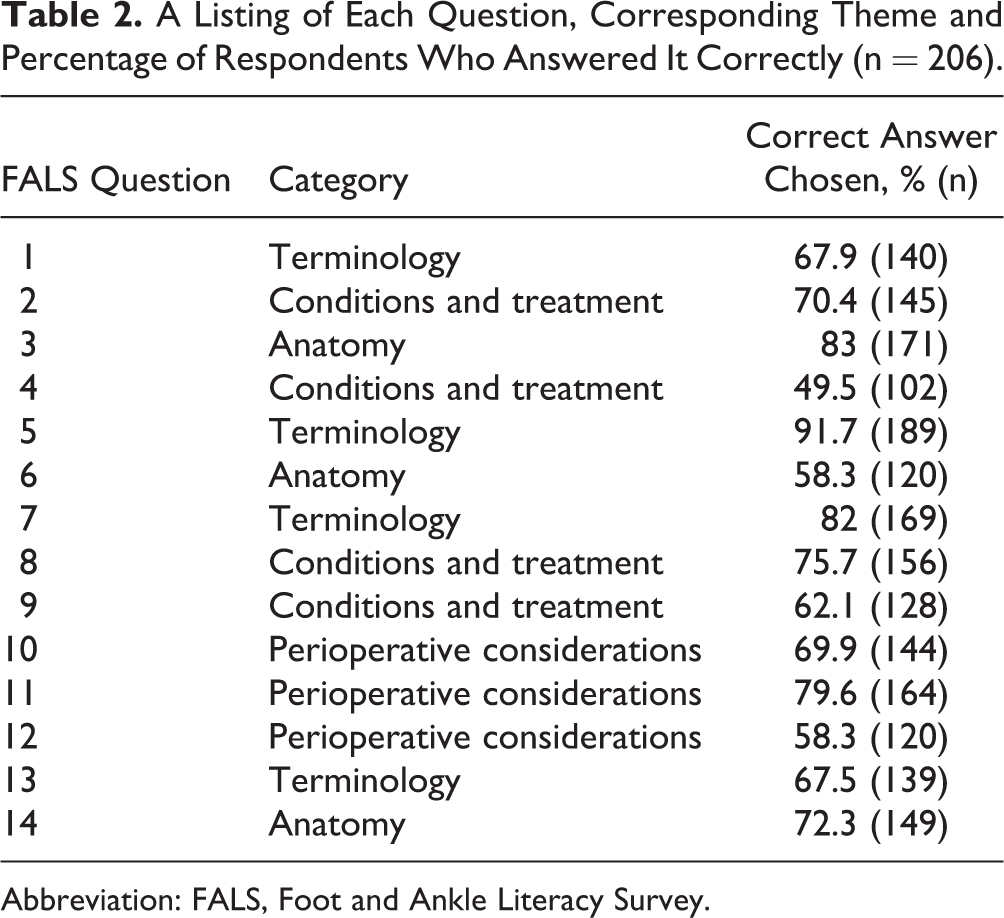
Abbreviation: FALS, Foot and Ankle Literacy Survey.
Statistical Analysis
Statistical analysis was performed with assistance from our institution’s clinical data analysts. Participants’ overall and categorical performance (eg, terminology, anatomy, conditions and treatment, perioperative considerations) on the FALS were determined. The total and categorical scores were then evaluated as a function of patients’ demographic traits. Significant differences between FALS performance and demographic characteristics were assessed via Wilcoxon rank sum and Kruskal-Wallis testing, depending on the number of variables within each demographic category. McNemar’s test with a Bonferroni correction was used to determine if statistically significant differences were present between categorical scores, independent of demographic attributes. The level of significance for all tests was set at P <.05.
Results
The overall mean FALS score was 9.9 ± 2.7 out of a possible 14 points. The percentage of correct answers for each question is listed in Table 2. McNemar’s testing revealed that participants performed significantly worse on the conditions and treatment subsection compared with the terminology, anatomy, and perioperative considerations subsections (P < .0001, P = .0001, P = .0049, respectively). There were no significant differences between scores in the other subsections (P > .05).
The relationship between participants’ demographic characteristics and overall FALS performance is presented in Table 3. Significantly better performance correlated with race (white, P < .001), higher levels of education (≥college, P < .001), patient type (preoperative visit, P < .002), and a current or previous health care occupation (P = .008). Additionally, of those patients who had previously seen a provider, a significant difference in performance was observed based on provider type (P = .008); patients who saw an orthopedic surgeon or an orthopedic surgeon and podiatrist scored higher than those who only saw a podiatrist or other type of provider.
FALS Performance Among Study Participants as a Function of Demographic Characteristics.a

Abbreviations: FALS, Foot and Ankle Literacy Survey; SD, standard deviation.
aThese variables represent demographic categories with significant (P < .05) differences in knowledge.
The relationship between participants’ demographics and categorical performance is presented in Table 4. Age, gender, and anatomic region did not have significant associations with performance in any of the categories. Race and education were associated with significantly improved performances in the terminology, conditions and treatment, and perioperative considerations categories (white, P = .008, .002, .032, respectively; ≥college, P = .019, <.001, <.001, respectively). Individuals who identified as either currently or previously being employed in a health care field performed significantly better in the perioperative consideration questions (P = .01). Visit type correlated with significantly improved performance in the anatomy and conditions and treatment sections (preoperative evaluation, P = .023, .002, respectively). Patients who previously saw a provider for a foot and ankle symptom performed significantly better in the terminology section (P = .027).
Participants’ Categorical Performance on the FALS as a Function of Demographic Characteristics.a
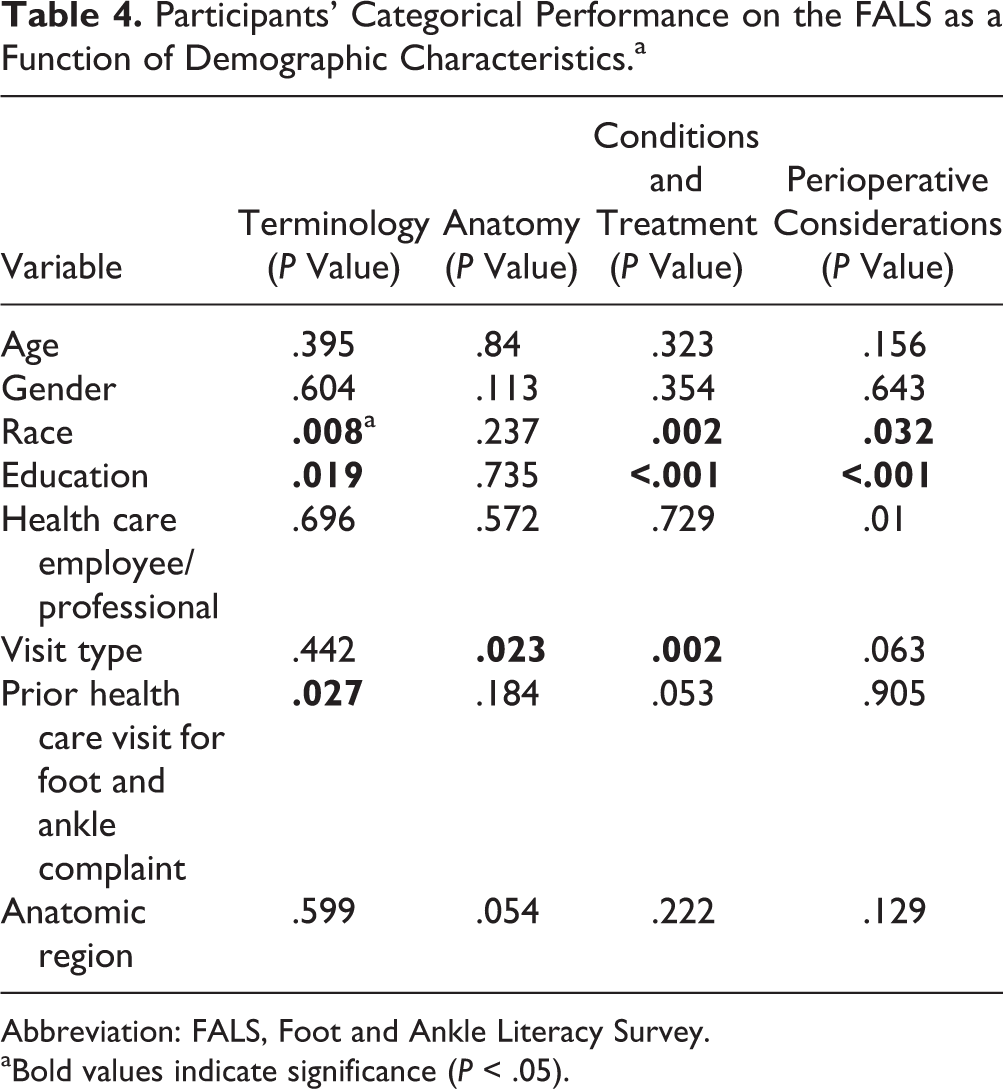
Abbreviation: FALS, Foot and Ankle Literacy Survey.
aBold values indicate significance (P < .05).
Discussion
This study found that patients seeking foot and ankle care may have inadequate baseline knowledge, particularly with regard to conditions and treatment. This is concerning, as this section of the FALS evaluated a patient’s knowledge of the disorders that may have led them to initially seek orthopedic foot and ankle care, and the possible therapeutic interventions needed.
More than 40% of the subjects were unfamiliar with the adverse effects of cigarette smoking in the setting of foot and ankle surgery, which was a perioperative considerations-themed question. This was surprising, as we had a largely educated cohort, with 67% of our participants having earned at least a college degree. Some of the anatomy questions were also challenging for participants, and more than 40% of them struggled with proper identification of the foot’s bones. Without knowledge of basic anatomy, it may be difficult for patients to actively participate in discussions regarding their care. Additionally, more than 30% of participants did not know that an orthopedic foot and ankle surgeon is different from a podiatrist, which was a terminology-themed question. This finding has tremendous implications with regard to the orthopedic foot and ankle surgeon–patient relationship, as it suggests that many of our patients are unclear as to the specific type of health care provider caring for them, and that they may not comprehend what orthopedic foot and ankle surgeons are and the training involved in becoming one.
Although we expected race and employment to correlate with FALS performance, we did not hypothesize that preoperative patients would outperform the other visit types. Instead, we thought that patients presenting for postoperative follow-up would have had the best performance on the FALS, as they would have had the most interactions with providers regarding their given condition. However, it is possible that patients presenting for their preoperative evaluations had been using other resources to learn about foot and ankle conditions, their specific diagnosis, and planned interventions, which could have contributed to their higher FALS scores.
Previous studies are consistent with our findings, as they have identified poor postoperative comprehension in patients following orthopedic surgery. 6,11 In a prospective evaluation of patient comprehension of informed consent, Crepeau et al found that patients had low comprehension and recall immediately following a discussion of the consent form, and that it further deteriorated by the first postoperative visit. 6 Kadakia et al also found limited postoperative comprehension among orthopedic trauma patients, who demonstrated a limited understanding of their injuries, surgeries, and postoperative instructions. 11
Our study’s limitations include its cross-sectional design and cohort composed of individuals from a single academic medical center, which may limit the generalizability of our results. Additionally, we failed to assess the influence of confounding variables, such as socioeconomic status, on the relationship between race and FALS performance. Further, the FALS included a variety of topics, and patients may only have a familiarity with their specific ailment or treatment. As such, condition-specific surveys may be of utility in future investigations on knowledge. Despite being informed of confidentiality, response bias could have occurred if some patients were reluctant to truthfully answer questions regarding educational background. Admittedly, some may also critique the FALS questions and respective themes. However, as previously discussed, we incorporated those topics most emphasized on FootCareMD.org, and included questions that prior to this work, we expected most patients to answer correctly. 8
Although we cannot refute the importance of survey validation, this was not our study’s purpose. Validation is critical when a questionnaire’s intended use is for the objective determination of comprehension, or another outcome, based on a specific score or performance. There is no specific FALS score that is indicative of adequate or inadequate knowledge, and at no point in this work did we suggest differently. If such inferences were to be made from FALS performance, validation would be mandatory. Instead, we set out to gain uncomplicated insight into participants’ knowledge of foot and ankle–related topics and to enhance our understanding of the relationship between demographics and performance.
One’s ability to make informed health-related decisions relies on health literacy, the ability to comprehend basic health information, and an underlying foundation of knowledge. 2,10 This work demonstrated the use of a questionnaire to enhance our understanding of what foot and ankle patients do, and do not, know. Our study suggests that patients may lack important foot and ankle–specific knowledge, and that demographic variables may correlate with performance. A validated foot and ankle–specific survey should be created, as this may help optimize the study of this complex topic. With such an instrument, we could further delineate risk factors for limited comprehension and health literacy, assess the benefits of currently available and more novel patient education resources, and determine if limited patient comprehension adversely affects outcomes. With this continued investigation and emphasis on health literacy and comprehension, patients may be optimally positioned to make decisions about their foot and ankle health, an approach that we hope will enhance physician–patient interactions and improve outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.