
Abstract
Purpose
To compare outcomes, between stemmed and stemless reverse shoulder arthroplasty (RSA) at a minimum follow-up of 5 years.
Methods
The authors retrospectively assessed a consecutive series of 45 patients that underwent RSA between September 2014 and October 2018 (23 stemless and 22 stemmed). All patients underwent plain anteroposterior and scapular Y-view radiographs for assessment immediately post-operatively and at final follow-up. At a minimum follow-up of 5 years, an independent observer assessed the clinical scores, including Constant score, QuickDASH score, and American Shoulder and Elbow Surgeons score.
Results
Of the 45 patients that underwent RSA, 5 patients died (11%), 2 were revised due to infection (4%), and 4 patients were lost to follow-up (9%). This left a final cohort of 34 patients (18 stemless and 16 stemmed). Significant differences between groups were found immediately post-operatively for lateralisation shoulder angle (LSA) (p = 0.021), but at 5 years post-operative for distalisation shoulder angle (DSA) (p = 0.017) and QuickDASH scores (p = 0.041) (Table 4), while the outcomes were comparable for absolute Constant scores, ASES score, and range of motion. Finally, stemless RSA had a 17% complication rate, while stemmed RSA had a 31% complication rate.
Conclusion
Stemless RSA had significantly more lateralisation, and significantly less distalisation, compared to stemmed RSA. Furthermore, at a 5-year follow-up, stemless RSA granted significantly greater QuickDASH scores. Finally, stemless RSA had comparable complication rates as stemmed RSA. The clinical relevance of this study is that stemless RSA is a safe alternative to stemmed RSA, while granting comparable or greater scores.
Introduction
Reverse shoulder arthroplasty (RSA) is increasingly performed, with a 200% increase from 2011 to 2015,1,2 for indications such as glenohumeral osteoarthritis, irreparable rotator cuff tear, or cuff tear arthropathy.3–7 The design of RSA is continuously evolving by shortening the humeral stem to reduce complications related to periprosthetic fractures, stem loosening, and malposition.4,7–10 Additionally, removal of the stem during revision surgery was often challenging as it could lead to humeral fractures and potential bone loss caused by ingrowth.7,11–13
Recently, following the success of stemless anatomic shoulder arthroplasty, stemless RSA has been introduced to overcome the complications related to the stem and facilitate revision surgery.13,14 Furthermore, the advantages of stemless RSA include increased bone preservation, as well as reduced stress shielding, surgical time and blood loss.5,6,9,13,15–20 Nonetheless, certain risks remain, namely poor fixation to early loosening, instability due to reduced bone contact area, intra-operative fractures6,15 or inadequate inclination.5,6 Due to the novelty of this type of implant, there are limited studies directly comparing the outcomes to stemmed RSA at medium-term follow-up.
The present study aims to compare functional, clinical, and radiological outcomes, at a minimum follow-up of 5 years, between stemmed and stemless RSA. The hypothesis is that stemless RSA yields comparable results to stemmed RSA.
Methods
The authors retrospectively assessed a consecutive series of 45 patients (45 RSAs) that underwent surgery between September 2014 and October 2018 at 2 centres by 3 senior surgeons (Figure 1). Of the 45 RSAs, 23 were performed using stemless RSA (EasyTech Reversed, FX Shoulder Solutions, Viriat, France) (Figure 2), and 22 using stemmed RSA (Figure 3). The most common indications for surgery were primary or secondary osteoarthritis due to massive rotator cuff tear (mRCT). Indications also include mRCT or osteonecrosis. No exclusion criteria were used for this study. Patients were routinely assigned to stemmed RSA at initial patient inclusion period. As standard procedure evolved, and the surgeons modernised their practice during the inclusion period, routine assignment gradually shifted to stemless RSA. Informed consent for the use of personal data for research was obtained for every participant, and the study was approved by the ethical board in advance (IRB approval number: IRB #: 098 DRC 210 DA03 001).

Flowchart.
Easytech® Reversed Implant (FX Shoulder Solutions)

Humelock®, Humeris®, and Humelock II® Implants (FX Shoulder Solutions)
Surgical Technique
All surgeries were performed in the beach chair position under general anesthesia and interscalene block. All patients underwent the delto-pectoral approach (Table 2), while in one patient the antero-superior approach was performed due to the presence of a pacemaker. Tenotomy of the subscapularis muscle was performed by peeling, and a tenotomy on the long head of the biceps tendon was performed, granting visibility on the gleno-humeral joint. Stemmed implant placement on the humeral bone was prepared by manual reaming of the bone, once the final size was achieved, the humeral stem was placed in the bone. Stemless implant placement was prepared by selecting the largest insertion site possible for the best peripheral support, and ensuring pins did not rest in the humeral cortex. The humeral component was then impacted into the bone. The glenoid preparation was the same for both the stemmed and stemless implants. Trial inlays were then used to select the optimal height for the humeral cup. Mobility and implant stability were tested before reattachment of the subscapularis muscle by anchors in a neutral position.
Post-Operative Care
Cryotherapy was performed immediately after surgery. Patients were immobilised for 3 weeks, positioning the arm in internal rotation. Gentle passive range of motion and pendulum exercises were allowed immediately following surgery under the supervision of a physiotherapist for 2 to 4 weeks. Active range of motion exercises were allowed 6 weeks following surgery.
Radiologic Assessment
Following surgery, every patient underwent plain anteroposterior and scapular Y-view radiographs for assessment immediately post-operatively and at final follow-up, which were used to determine scapular notching according to the Sirveaux-Nérot classification. 21 Radiologic measurements were performed by one surgeon (AQ), and included the Neck Shaft Angle (NSA), Gleno-Metaphyseal Angle (GMA), glenoid inclination, Lateralisation Shoulder Angle (LSA), Distalisation Shoulder Angle (DSA) (Figure 4), and the acromio-humeral distance. Finally, the Teissier lateralisation, 22 Werthel lateralisation, 23 Lädermann's lowering of the acromio-implant distance, 24 inferior overhang (Figure 5), and Nourissat pentagon 25 were assessed (Figure 6).
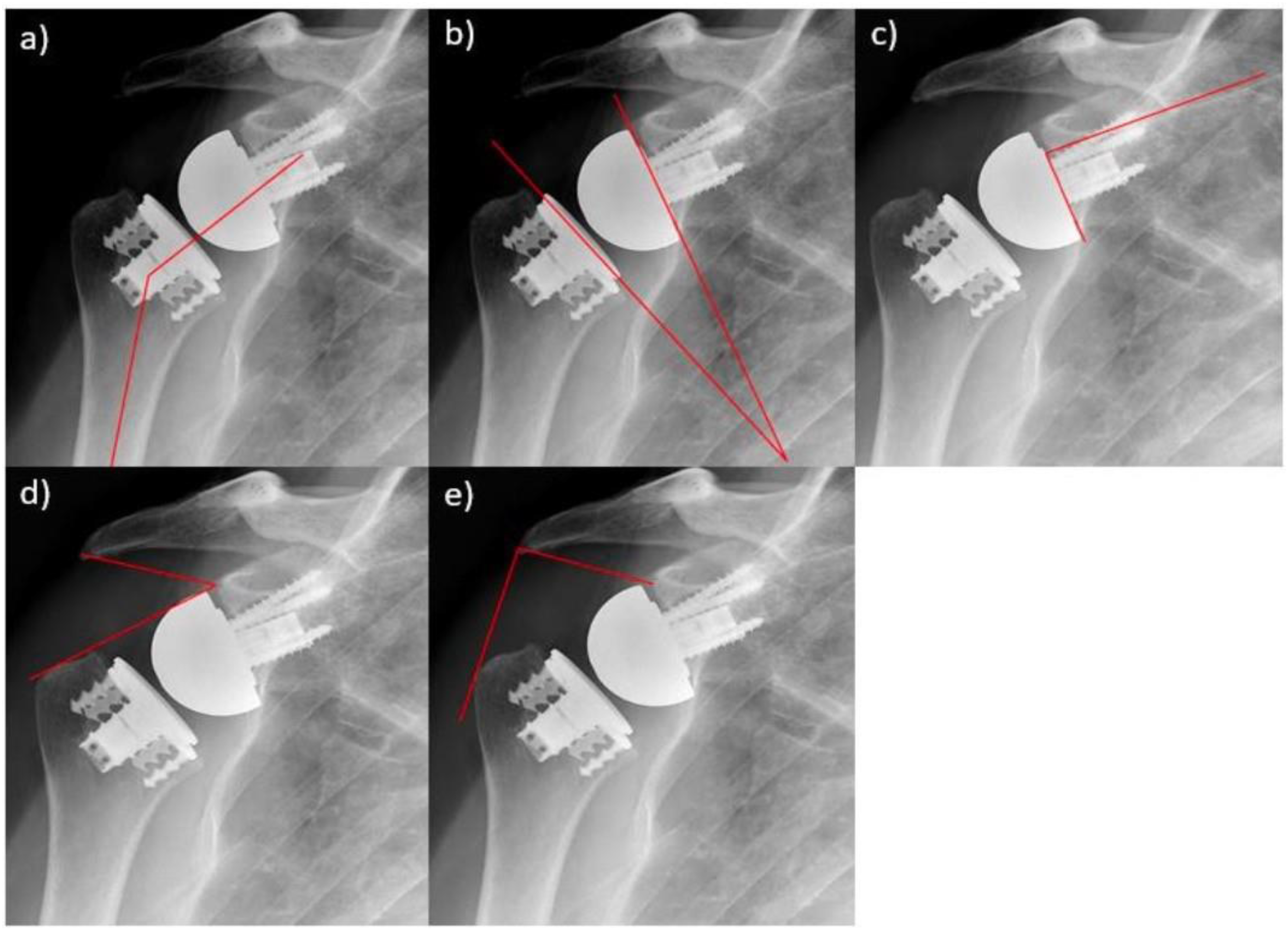
a) Neck Shaft Angle (NSA); b) Gleno-metaphyseal Angle (GMA); c) Glenoid Inclination; d) Distalisation Shoulder Angle (DSA); e) Lateralisation Shoulder Angle (LSA)

a) Lowering ; b) Inferior overhang; c) Lh + Lg = Werthel Lateralisation (Lh, Humerus lateralisation; Lg, Glenoid lateralisation); d) Teissier Lateralisation

Nourissat Pentagon
Clinical Assessment
Pre-operatively, an independent observer assessed the Constant score 26 and age-/sex-adjusted Constant score. 27 At a minimum follow-up of 5 years, an independent observer assessed the clinical scores, including Constant score, age-/sex-adjusted Constant score, QuickDASH 28 score (MCID of 15 points), 29 and American Shoulder and Elbow Surgeons (ASES) 30 score. In addition, range of motion was assessed, including active forward elevation (AFE), external rotation with the elbow at the side (ER1), internal rotation (IR), and abduction. All intra- and post-operative complications were noted.
Statistical Analysis
Descriptive statistics were used to summarise the findings, and Shapiro–Wilk tests were used to assess the normality of data distributions. For normally distributed continuous data, differences between the stemmed and stemless RSA were evaluated using unpaired t-tests. For categorical variables, differences were between the stemmed and stemless RSA were evaluated using the Chi-squared tests. P values <0.05 were considered significant. Statistical analyses were performed using R version 4.2.3 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Of the 45 patients that underwent RSA, 5 patients died (11%), 2 were revised due to infection (4%), and 4 patients were lost to follow-up (9%) (Figure 1). The final stemless RSA group comprised 18 patients, aged 68.7 ± 7.2 (range, 57 to 79), with a BMI of 30.0 ± 3.9 (range, 23 to 36), with 10 women (56%), and 2 smokers (11%). The final stemmed RSA group comprised 16 patients, aged 72.6 ± 8.4 (range, 51 to 85), with a BMI of 26.3 ± 3.6 (range, 19 to 32), with 12 women (75%), and 3 smokers (19%) (Table 1). There were no significant differences between the groups in terms of indications for arthroplasty, or glenoid Walch classification as assessed intra-operatively (Table 2).
Demographics.

Intraoperative.

Complications and Adverse Events
Of all included patients receiving a stemless RSA, 1 experienced an acromial stress fracture (ASF) (6%), and 2 experienced periprosthetic fracture (11%) (Table 3). Of all included patients receiving a stemmed RSA, 1 experienced a greater tubercule fracture (6%), 1 experienced glenoid fracture (6%), 1 suffered musculo-cutaneous nerve damage (6%), 1 experienced glenoid loosening (6%), and finally 1 contracted an infection (6%). There were no significant differences found between the groups in terms of complications. One patient experienced a grade 1 notch at 5 post-operative years in the stemless group (6%). Spur occurred in 1 patient from the stemless group (6%), versus in 2 from the stemmed group (13%). Stage 1 and stage 2 radiolucent lines were observed on the humeral side around the stem in 3 patients respectively in the stemmed group (19% and 19%).
Complications and adverse events.

Radiological Outcomes
Immediately post-operative, there were significant differences between the stemless and stemmed groups in terms of GMA (28.4°±16.0° and 39.5°±12.6°; p = 0.033), LSA (86.4°±9.0° and 79.3°±6.7°; p = 0.021), Teisser lateralisation (51.6 ± 6.2 and 46.5 ± 7.1; p = 0.032), and Lädermann's lowering of the acromio-implant distance (29.8 ± 8.6 and 35.3 ± 5.9; p = 0.042). At 5 years post-operative, it was only significantly different for DSA (44.2 ± 6.7 and 51.1 ± 8.8; p = 0.017) (Table 4).
Radiological outcomes.

Clinical Outcomes
Pre-operatively, compared to patients that underwent stemmed RSA, those with stemless RSA had significantly greater absolute Constant scores (23.8 ± 7.5 and 32.4 ± 6.5; p = 0.003), as well as adjusted Constant scores (33.3 ± 11.2 and 43.3 ± 8.5; p = 0.031). At a minimum follow-up of 5 years, there was a significant difference between the stemless and the stemmed groups in terms of QuickDASH scores (24.4 ± 8.8 and 30.8 ± 7.1; p = 0.041), however, the difference of 6 points might not be clinically relevant. The outcomes for absolute and age-/sex-adjusted Constant scores, ASES score, and range of motion were comparable. (Table 5).
Clinical and functional outcomes.

Discussion
The most important findings for this study are that post-operative radiographs revealed that compared to stemmed RSA, stemless RSA had significantly more lateralisation immediately post-operatively (79.3°±6.7 vs 86.4°±9.0; p = 0.021), and significantly less distalisation at 5 years post-operative (51.1°±8.8 vs 44.2°±6,7; p = 0.017). Furthermore, at a minimum 5-year follow-up, compared to stemmed RSA, stemless RSA granted significantly greater QuickDASH scores. It is worth noting, however, that even though there were statistically significant differences in LSA, DSA, and QuickDASH, they may not be clinically relevant and further studies may be required to assess the long-term relevance. Furthermore, the groups had comparable absolute Constant scores, age-/sex-adjusted Constant scores, and ASES scores. Finally, stemless RSA had a 17% complication rate, while stemmed RSA had a 31% complication rate. While the hypothesis that stemless RSA yields comparable results to stemmed RSA is confirmed for the majority of clinical scores, it granted better radiographic outcomes. The clinical relevance of this study is that stemless RSA is a safe alternative to stemmed RSA, while granting comparable or better outcomes.
The non-anatomical (reverse) approach to shoulder arthroplasty was developed in 1985 by Grammont for cuff tear arthropathy. This approach tended to medialise and distalise the gleno-humeral centre of rotation.9,16,17,19 However, as high complication rates were reported,4,10 many implant designs have followed in the attempt to improve outcomes of shoulder arthroplasty.6,15 In fact, medialised position did not improve active external rotation, and excessive distalisation could lead to neurologic injuries. 31 Nowadays, lateralisation is recommended to minimise torque on the glenoid component and scapular notching.22,32 In a study by Boutsiadis et al, 31 it was determined that AFE was greater when the DSA was between 40° and 65°, and external rotation was greater when the LSA was between 75° and 95°. In the present study, both the stemmed and stemless RSA groups fall into the aforementioned range for DSA and LSA. Patients included in the stemless RSA group had a significantly greater LSA immediately after surgery, and a significantly lower DSA at 5 post-operative years. Statistically significant differences in LSA and DSA between the stemless and stemmed groups may be due to the conservation of bone stock required for the stemless implant, however, further studies with bigger cohorts should investigate this. Furthermore, the change in LSA and DSA between immediate post-operative and at 5 years may be due to the angle at which the radiograph was taken. While no significant difference was observed in ROM, the stemless RSA group tended to have more ROM than the stemmed RSA group, which could be due to the minimal cut and lower deltoid tension.
Removing the stem of the implants for RSA was driven by the aim to facilitate adjusting the degree of LSA and DSA, but also to preserve the bone stock and achieve metaphyseal fixation while minimising bone resection.5,6,13,15 While stemless RSA versus stemmed RSA remains sparsely covered in literature, stemless TSA versus stemmed TSA has been widely discussed and compared in existing literature.33–35 In a systematic review by Peng et al 35 comparing effectiveness of stemless versus stemmed implants for regular TSA, clinical scores for both implant categories were compared. While both techniques yielded satisfactory results, none surpassed the other, therefore justifying expectations of comparability between techniques for RSA.
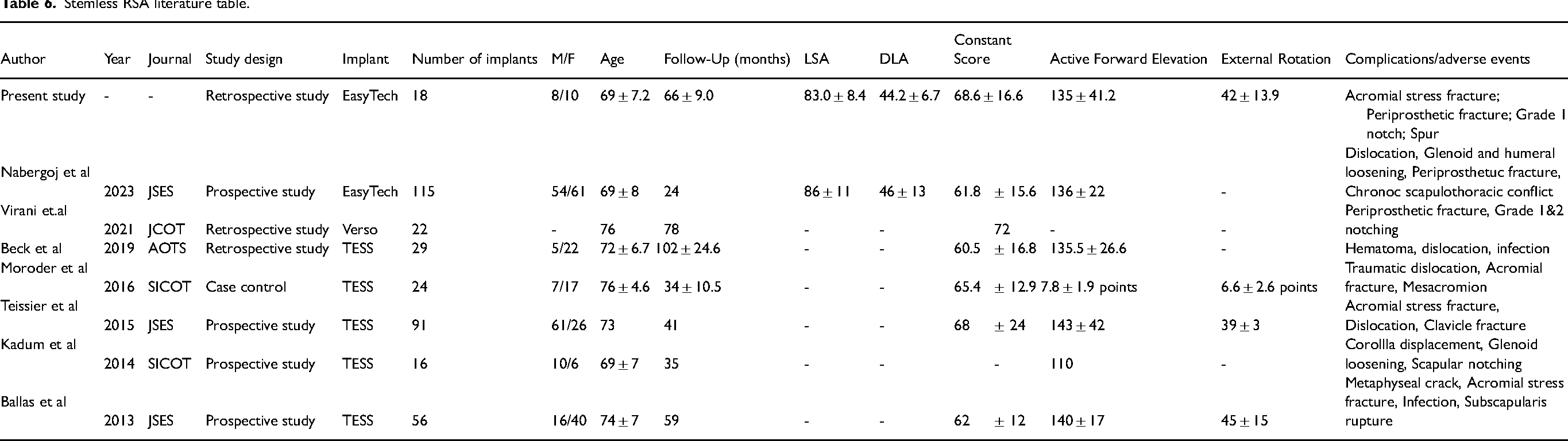
In a prospective study by Ballas et al, 8 participants underwent stemless RSA (TESS implant) with a 58 month follow-up, and found post-operative Constant scores of 62 ± 12, AFE of 140°±17, and external rotation of 45°±15 (Table 6). Another prospective study by Teissier et al 22 (TESS implant) yielded similar Constant scores (68 ± 12), and external rotation (39 ± 3). Compared to the study of Ballas et al 8 and Teissier et al, 22 the patients in the present study had comparable ROM post-operatively (AFE, 135°±41.2, external rotation, 42°±13.9), but had slightly better Constant scores (68.6 ± 16.6). Furthermore, there was no significant difference for glenoid Walch classification, even though there tended to be more shoulders with type A1 glenoids in the stemless group, and type B2 glenoids in the stemmed group. It is worth noting that, during RSA surgery, the glenoid anatomy is modified to accommodate the glenoid component, and therefore, the pre-operative glenoid morphology should not impact post-operative clinical scores. Most importantly, the present study tended to show higher scores for patients in the stemless group than patients in the stemmed group, once again demonstrating the non-inferiority of stemless RSA.
Stemless RSA literature table.
Shoulder arthroplasty remains an evolving technique as complications are frequent due to the anatomical complexity of the shoulder joint, but also the movement and stress applied on a daily basis. As a result, is it not uncommon to identify cases of glenoid loosening, nerve damage, migration or infections in cases of stemmed arthroplasty a seen in a systematic review by Kent et al. 36 In another systematic review by Reahl et al 37 comparing stemmed RSA to stemmed TSA, complication rates for RSA were 6%, while they were 9% for TSA, taking into consideration the heterogeneity of the included studies. These findings are substantially better than the reported complication rates in the present study, with the stemmed group reaching a complication rate of 31%. The nature of the complications, however, mirror the systematic reviews as cases of greater tubercule fracture, glenoid fracture and loosening, nerve damage and infections were observed. In comparison, the stemless RSA group had a complication rate of 17% with observed cases of periprosthetic fracture and ASFs, which are a result of excessive lateralisation. In a systematic review by Liu et al, 5 on stemless RSA, complication rates reached 12% and included cases of periprosthetic fractures, glenoid loosening and dislocations. Some of the encountered displacements however were a consequence of poor bone stock quality which constitutes a contraindication for stemless RSA as fixation would not be stable. Stemless RSA fixation is dependent on the available bone quality, as low bone mass density may affect resorption and stability, potentially requiring revision surgery. A study by Ritter et al 38 investigated the evaluation of bone density using computed tomography, and found that this imaging modality would allow objective assessment of the bone, and assist in decision-making before performing stemless RSA.
The findings of this study should be interpreted with the following limitations in mind. Firstly, even though the study evaluates stemless RSA at mid-term follow-up, the cohort remains relatively small with considerable rates of loss to follow-up and revision, and therefore may not accurately represent the population of interest. Secondly, the authors did not collect pre-operative range of motion, which does not allow for comparisons of the groups before surgery. Thirdly, only one surgeon performed the radiographic measurements using a standardised method, and therefore the authors did not remeasure the angles. Finally, even though authors did not select type of implant based on pre-operative characteristics, significant differences at baseline in BMI and Constant scores, added to the small cohort, may create bias in final results as the study cohorts may not be sufficiently comparable or powered. Nevertheless, the main strength of this study is that it is one of the first to directly compare stemmed and stemless RSA at a medium-term follow-up.
Conclusion
Stemless RSA had significantly more lateralisation, and significantly less distalisation, compared to stemmed RSA. Furthermore, at a minimum 5-year follow-up, compared to stemmed RSA, stemless RSA granted significantly greater QuickDASH scores, and comparable absolute Constant scores, age-/sex-adjusted Constant scores, and ASES scores. Finally, stemless RSA had comparable complications rates as stemmed RSA. The clinical relevance of this study is that stemless RSA is a safe alternative to stemmed RSA, while granting comparable or greater scores.
- NG reports fees from FX Shoulder Solutions and SBM outside of the submitted work. Furthermore, NG reports royalties from FX Shoulder Solutions and SBM. - AM reports fees from FX Shoulder Solutions outside of the submitted work. Furthermore, AM reports royalties from FX Shoulder Solutions. - HH reports fees from FX Shoulder Solutions and Smith & Nephew outside of the submitted work. Furthermore, HH reports royalties from FX Shoulder Solutions. - OL reports fees from FX Shoulder Solutions. Elsevier and Evolutis outside of the submitted work. Furthermore, OL reports royalties from FX Shoulder Solutions, Medartis, Kerimedical, TBF, Evolutis and Branchet.
Footnotes
Authors’ Contributions
QA Study design, data collection, interpretation of findings and manuscript writing.
DA Study design, data collection, interpretation of findings and manuscript editing.
RS Study design, data collection, interpretation of findings and manuscript editing.
AA Study design, data collection, interpretation of findings and manuscript editing.
PA Study design, data collection, interpretation of findings and manuscript editing.
NG Study design, data collection, interpretation of findings and manuscript editing.
AM Study design, data collection, interpretation of findings and manuscript editing.
HH Study design, data collection, interpretation of findings and manuscript editing.
CA Methodology, data curation, formal analysis, statistical analysis, manuscript writing.
FVR Methodology, data curation, formal analysis, statistical analysis, manuscript writing.
OL Procurement of funding, study design, data collection, interpretation of findings and manuscript writing.
All authors approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
All patients provided informed consent for the use of their data for research and publications and the institutional review board approved this study in advance (IRB #: 098 DRC 210 DA03 001).
Funding
The author(s) are grateful to “FX Shoulder Solutions” for funding the statistical analysis and manuscript preparation for this study.