
Abstract
Prosthetic instability is one of the most challenging complications to manage when considering reverse shoulder arthroplasty (RSA). Additional tools are available to improve accuracy in planning and execution of arthroplasties, such as 3-dimensional (3D) virtual planning based on computer tomography (CT) scan and intra-operative navigation. We report a case of an 84-year-old male treated for RSA prosthetic instability combined with severe glenoid deformity and bone loss, and subclinical periprosthetic joint infection (PJI). The definitive surgery consisted in implanting a customized metaglene component realized on the basis of the bone defect detected in the 3D-CT scan and implanted with the aid of computer-assisted intra-operative navigation. The patient was periodically followed-up for a year with clinical and radiological evaluations with the absence of further prosthetic dislocations nor PJI, a good overall satisfaction, a satisfying range of motion, and acceptable functional scores (American Shoulder and Elbow Surgeons Score 62, Constant-Murley Score 36). This is the first description, to our knowledge, of a customized glenoid baseplate implanted with the aid of intraoperative navigation. The combined use of 3D-CT planning and intra-operative computer-assisted navigation allows to manage complex cases of prosthetic revision surgery even where extensive bone defects are present.
Keywords
Introduction
Reverse shoulder arthroplasties (RSAs) are burdened by a fairly high rate of complications, with studies showing variable percentages up to 68%.1–3 Instability or dislocation of the implant is the most common complication with an estimate rate ranging from 1.5% to 31%. 2 There are multiple factors that can contribute to a raised risk of instability, but more often instability is primarily determined by a biomechanical issue: loss of compression, loss of containment or impingement.2–4 Chronic or acute periprosthetic joint infection (PJI) is the second most common cause of recurring or irreducible dislocations,2,3,5 with rates ranging from 2.9% in primary RSA to 15.4% in revision surgeries. 6 When combined with altered workloads on the prosthetic components due to malpositioning or improper planning, polyethylene (PE) premature wear or baseplate mobilization may occur. This can further exacerbate the soft tissue damage, massive bone remodeling, and severe humeral and glenoid bone loss, which will eventually worsen an already present prosthetic instability.3,7 Fortunately, in recent years 3-dimensional (3D) virtual planning based on computer tomography (CT) scan, intra-operative navigation, and patient-specific instrumentation (PSI) have been developed and employed as additional tools to improve accuracy in planning and execution of arthroplasties, both anatomic and RSA.8–13 Specifically, a more precise glenoid and screw positioning, as well as bone stock preservation have been demonstrated. 13 This technology may be also useful for the management of complex cases of revision surgery where a customized component is needed, and the residual bone stock should be spared.
The purpose of this case report is to provide the first description of the diagnostic and therapeutic management of a patient who underwent revision surgery due to chronic RSA instability with the implant of a custom-made glenoid baseplate realized on the basis of the 3D CT-based planning and intra-operative navigation.
At our institution, no ethical committee nor Institutional Review Board approval is necessary for case reports, and the patient gave his informed consent to data collection and their anonymous use for scientific and teaching purposes. This study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Case Report
In November 2020, an 84-year-old right-handed man with a history of recurring RSA dislocations and multiple revision surgeries presented to our attention with the dislocated RSA. In 2018, the patient underwent left RSA for end-stage cuff arthropathy at another hospital. Two years later, in September 2020, the patient underwent the first revision surgery due to a dislodged glenosphere from the metaglene component (Figure 1). The damaged glenosphere and PE insert were replaced. About 20 days post-operatively, a first irreducible atraumatic RSA dislocation episode occurred, and therefore a further revision surgery was necessary. The implant was reduced, and the PE insert was replaced. In November 2020, the patient was referred to our emergency department because he suddenly presented an extremely limited range of motion (ROM) of the shoulder (abduction 20°, forward elevation 20°, rotations 0°). There were no neurovascular deficits, neither sign of surgical wound infection on clinical examination. Plain radiographs showed antero-inferior dislocation of the left RSA (Figure 2). The limb was immobilized in arm sling and the patient was admitted to the orthopedic ward to complete pre-operative evaluation. Our decision-making process was the following. First, an electromyography to evaluate the integrity of the axillary nerve and exclude a possible atrophy of the deltoid was performed. In addition, all the information regarding the implant and its measures (Medacta Shoulder System Reverse, Medacta International, Castel San Pietro, Switzerland), as well as any critical issue in the soft tissues were collected. Our aim was to identify any causes of prosthetic instability already present and choose the most appropriate treatment. Pre-operative planning highlighted an insufficient implant lateralization which determined an inadequate glenoid wrapping and a consequent scarce component coaptation. Also, an unsatisfactory humeral version (20° antiverted) which could predispose to future dislocations was present. Inflammatory markers were within normal range.

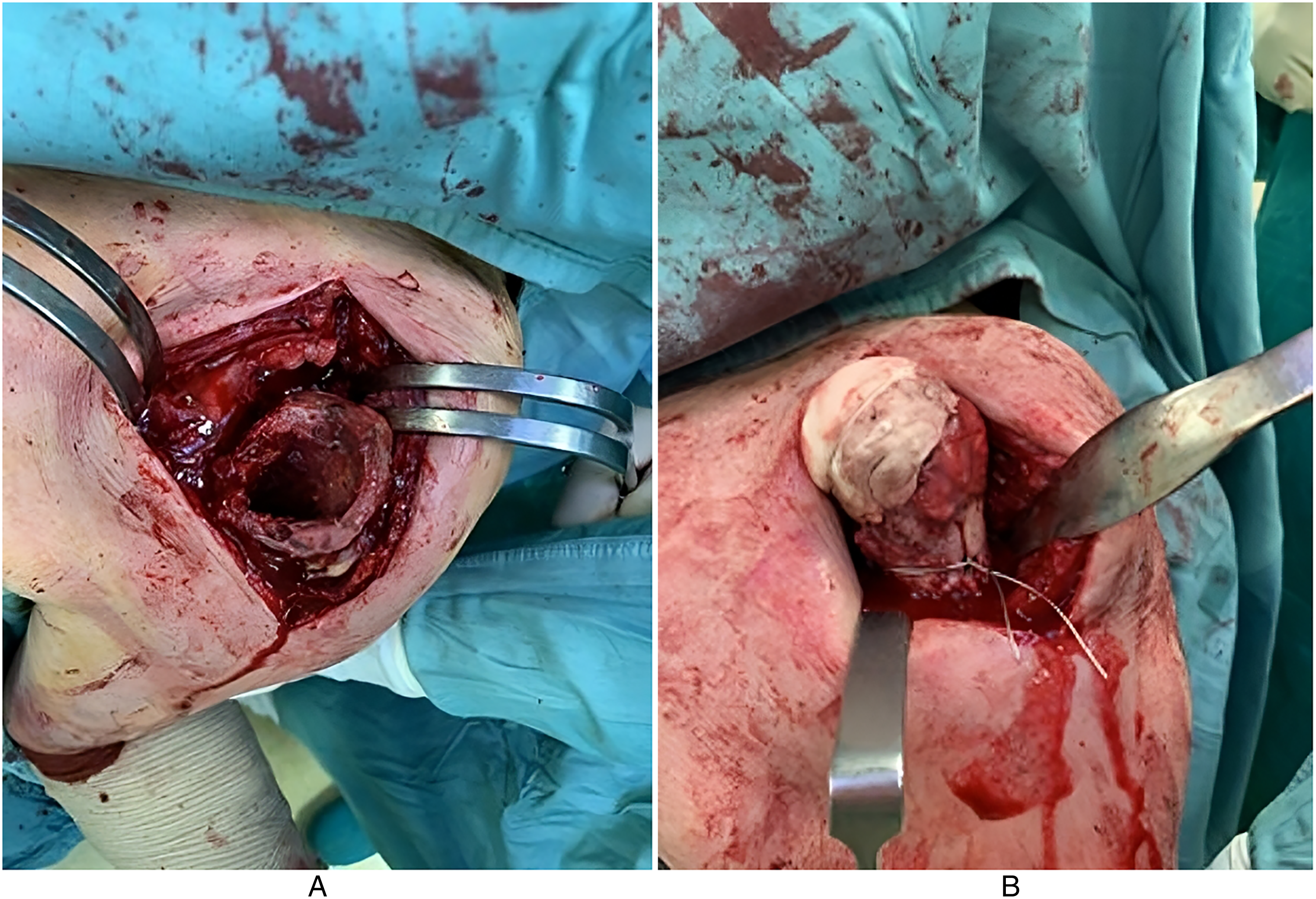
Antero-posterior radiographs showing dislodgment of the glenoid component (A), and the intra-operative findings with PE wear (B).
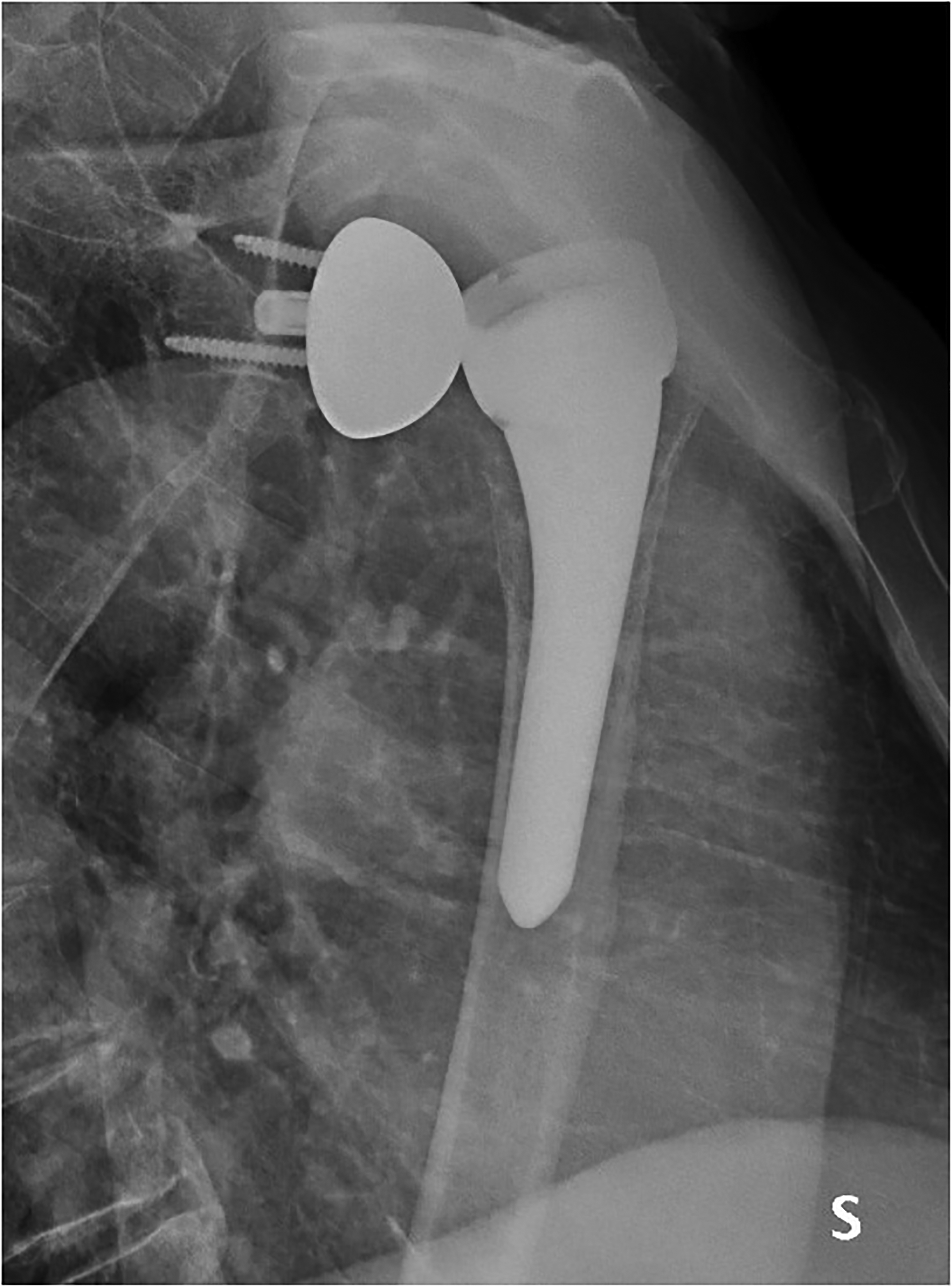
Axillary view of the dislocated RSA.
The patient underwent surgery on day 6th from admission. Under general anesthesia, a deltopectoral approach on the previous incision with the patient in a beach-chair position was performed. All adhesions were removed, including a voluminous inelastic posterior subdeltoid scar that could limit ROM and predispose to new dislocations through an indirect lever mechanism. Five samples of periprosthetic material were taken for microbiological analysis, as per existing practice for each revision procedure. The stability of the humeral stem and glenoid baseplate were verified and, after that, the glenosphere (from 39 mm standard to 39 mm lateralized), the PE insert (from +6 mm to +3 mm) and the humeral metaphyseal component (from +9 mm and 20° anteverted to +0 mm and 20° retroverted) were replaced. Intra-operative stability tests and ROM were proven to be optimal. The subscapularis was re-attached with multiple non-reabsorbable stitches, and the wound was closed in layers. To control bleeding, in the absence of contraindications, tranexamic acid was administered both intravenously and locally, as previously described. 14 The arm was placed in a sling (0° abduction and 30°internal rotation) to be maintained for 30 days to promote soft tissue healing and scar formation on the anterior capsule that could maintain the prosthesis in place. Microbiological examination resulted negative on all samples.
Shortly afterwards, a new atraumatic dislocation occurred. A subclinical PJI was then suspected and the patient underwent a 2-stage revision procedure. During the first phase of the procedure, the implant was removed, collected, and processed with the MicroDTTect® system (NovaHealth, Cazzago San Martino, Brescia, Italy) to degrade any bacterial biofilm formed on the surfaces and thus increase the accuracy of the examination. An antibiotic-loaded spacer was then implanted and an excessive humeral component anteversion was detected (Figure 3). Microbiological cultures resulted positive for Staphylococcus capitis, so the patient was subjected to targeted antibiotic therapy for 6 weeks and underwent periodic blood tests (erythrocyte sedimentation rate, C-reactive protein, fibrinogen, and white cell blood count) to monitor the infection. A CT scan with 3D reconstruction was performed to gain a clearer understanding of the altered patient's anatomy (Figure 4). A severe glenoid deformity and significant bone loss classified as severe-combined according to Antuna 15 were demonstrated. Therefore, in our opinion, an adequate management of the bone defect with the achievement of a stable fixation with bone grafts or augmented baseplates would not have been possible. As a result, it became necessary to employ a customized glenoid component (Osteobionix—Instituto Tecnológico de Canarias, Spain) that would fit the patient's anatomy impeccably allowing a correct anchoring to the poor bone stock available and avoiding additional bone loss. Moreover, given the complexity of the case, an intra-operative navigation system (GPS Navigation System, Exactech, Gainesville, FL, USA) was deployed to adhere to pre-operative planning and prevent component malpositioning or incorrect fixation (Figure 5).
Prosthetic components were removed during the first phase of the 2-stage revision procedure (A), and a preformed antibiotic loaded spacer has been implanted (B). Note the version defect filled with bone cement.

The pre-operative 3D CT-based planning highlighted a severe combined glenoid bone loss, shown on the 3 planes of space: (A) sagittal, (B) coronal, and (C) transverse.

Customized baseplate (A) and PSI required to its implant (B). A 3D-model of the patient's scapula was obtained with a 3D-printer to verify the correspondence between patient's anatomy and the customized implant.
After the completion of the antibiotic treatment, and the achievement of normalization of inflammatory markers, the patient underwent surgery. Under general anesthesia, a deltopectoral approach on the previous incision with the patient in a beach-chair position was performed. A thorough debridement was implemented, the antibiotic-loaded spacer was removed, and the definitive components were implanted starting from the glenoid side. The customized glenoid was secured with 3 screws (30, 34, 34 mm) whose length and direction corresponded to the preoperative planning, and a size 42 glenosphere was placed.9,12 As regards the humeral side, a cemented Equinoxe® Reverse Shoulder System stem (Exactech, Gainesville, FL, USA) size 13 mm with 25° retroversion was implanted (Figure 6). The subscapularis was re-attached with multiple non-reabsorbable stitches, and the wound was closed in layers. Again, to control bleeding, tranexamic acid was administered both intravenously and locally. 14 The arm was then placed on 45° abduction/neutral rotation splint to be maintained for 30 days. Afterwards, passive forward elevation and abduction of the shoulder were allowed, at 5 weeks after surgery active forward elevation and abduction were encouraged, and rotations and strengthening exercises were started at 6 weeks from surgery. Radiographs were obtained at 1, 3, 6, and 12 months from surgery. Functional assessment was undertaken at 6 and 12 months, using the Constant-Murley Score (CMS) 16 and the American Shoulder and Elbow Surgeons Score (ASES). 17
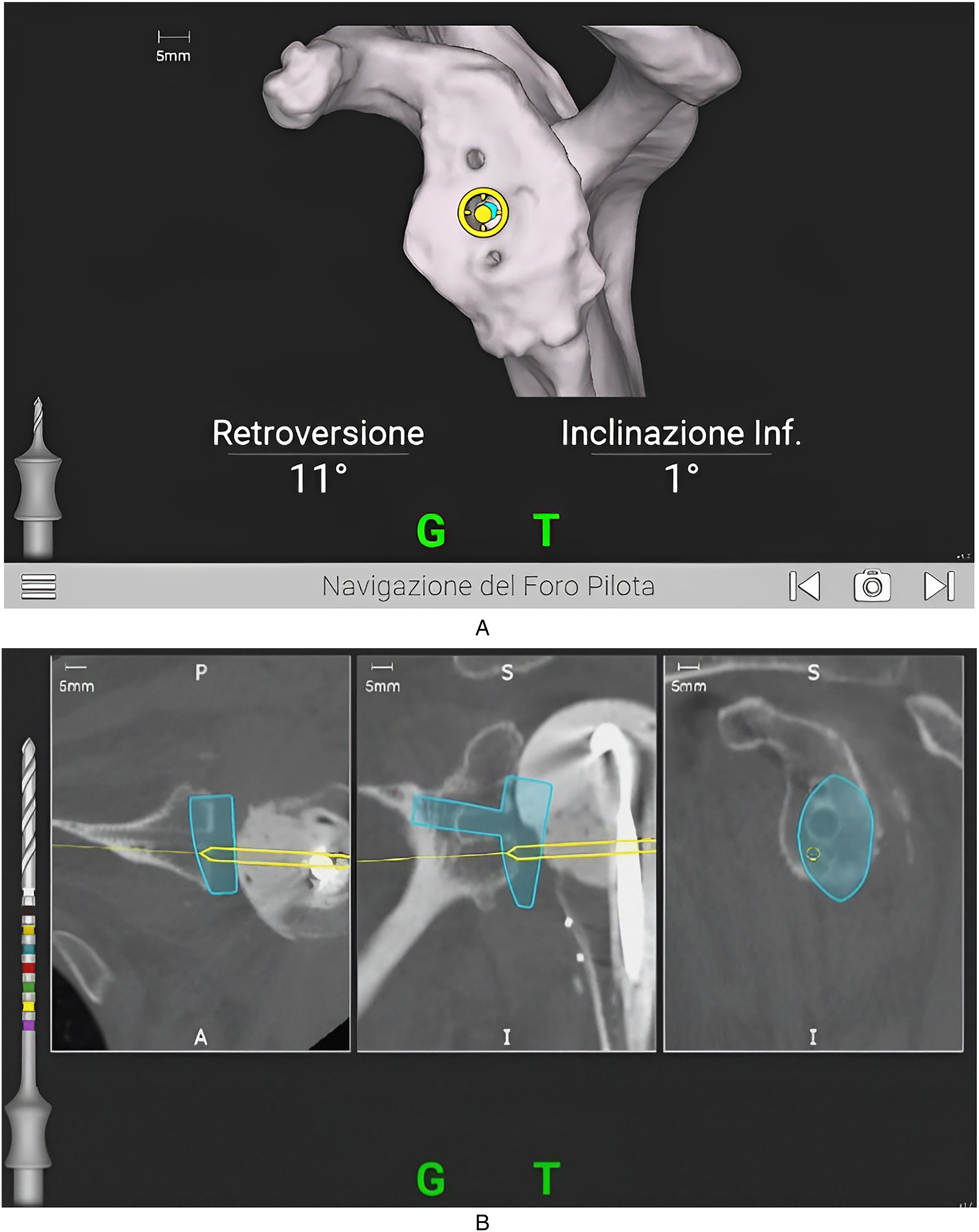
Intra-operative computer-assisted navigation for the central peg's (A) and screws’ (B) holes have the aim to support the surgeon during operation giving real-time feedback on the position of the drill.
At 1-year follow-up, the patient presented with no signs of local infection nor pain, a stable prosthesis (Figure 7) and a good shoulder ROM (80° abduction, 70° anterior elevation, 15° external rotation, and hand to the buttock in internal rotation). Functional score showed an ASES of 62 and CMS of 36. No further dislocations occurred. Patient rated the overall satisfaction as good.
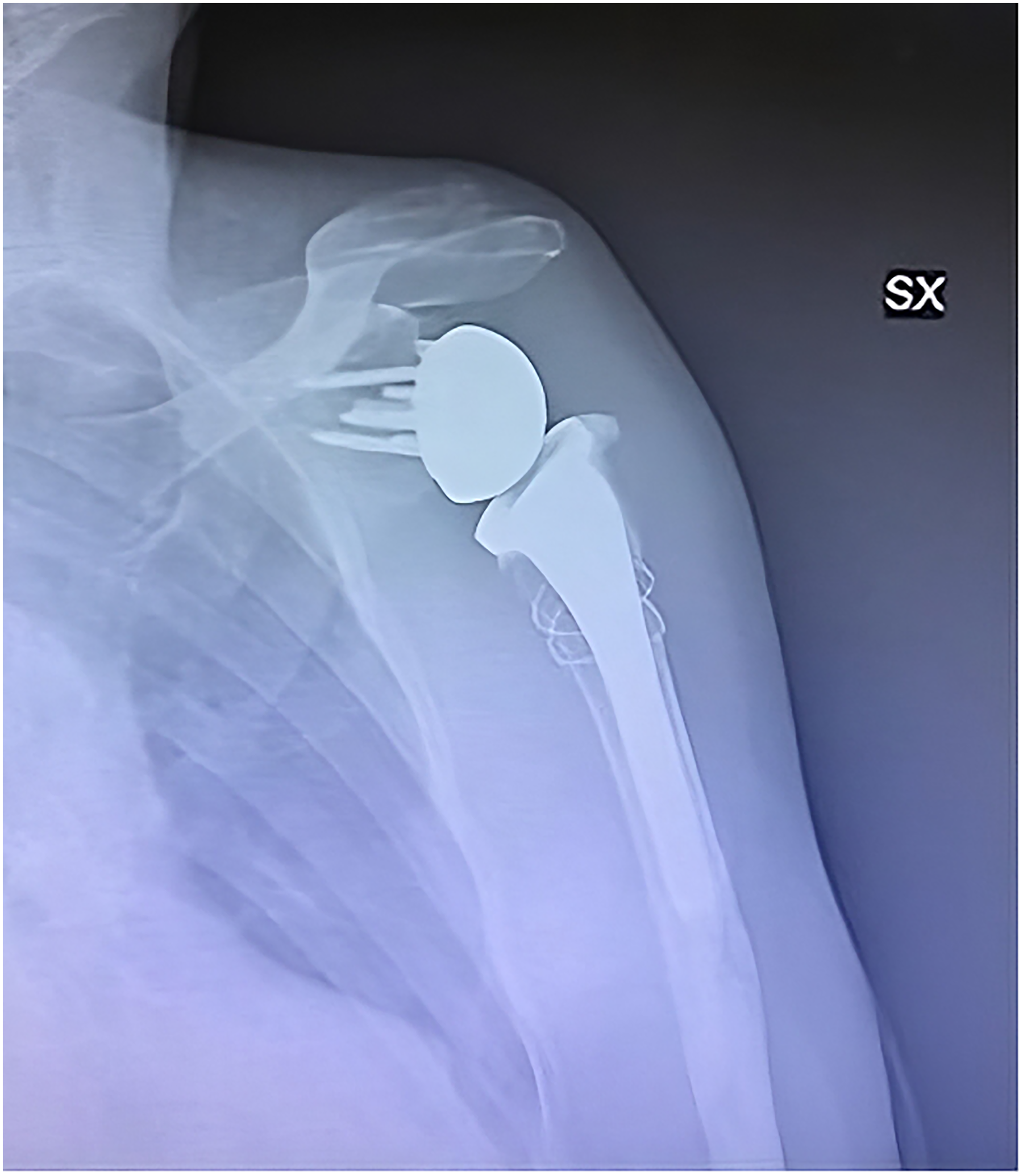
Antero-posterior radiographs obtained at 1-year follow-up showing a stable prosthesis.
Discussion
The management of complications related to RSA, and in particular instability, is always a demanding challenge for the orthopedic surgeon. The issues highlighted in this case report include the correct identification of the cause of prosthetic instability and severe bone loss requiring novel techniques for reconstruction on the glenoid side. The correct identification of the cause of prosthetic instability is fundamental for the success of the surgery. Restoring an adequate deltoid tensioning by correcting humeral version and medialization 3 was not sufficient to solve the instability. Indeed, a misdiagnosed PJI was identified as a contributing factor to the main biomechanical issue for recurrent dislocations. Infection has been reported to occur in 44% of the cases of RTSA instability, 18 and therefore it is always advisable to exclude a possible infection before performing a revision surgery in order to treat it promptly and avoid future new complications. Furthermore, each new revision further worsens the state of the soft tissues, increasing the risk of new dislocations. Despite numerous studies on PJI, there is currently no gold standard treatment. A recent review of the literature 19 showed that better outcomes are obtained with 1-stage revision surgery. Nevertheless, this procedure is reserved for cases in which the microorganism responsible for the infection is known, while a 2-stage revision procedure becomes a valid option in all those cases of unknown pathogen and/or suspected PJI and/or combined issues that may anticipate an unpredictable amount of bone loss.
A careful evaluation of the glenoid bone loss is essential for a correct preoperative planning. The patient presented with a significant bony defect on the glenoid side made even more extensive by the presence of peg and screw holes of the previous implant. This situation led to 2 issues that needed to be solved. First, an adequate management of the defect was required since traditional methods of surgical techniques are not able to provide consistent means to correct moderate to severe glenoid deformity. 20 Few studies are available in the literature describing the management of poor bone stock in complex cases of revision surgery. Authors resorted to the use of different technical solution including customized baseplate with special tantalum augments, 21 customized glenoid implants and the use of PSI, 22 custom-made titanium glenoid implant with porous coated back-side, 23 and allograft-prosthesis composite. 24 In some cases, although limited, salvage procedures such as glenohumeral arthrodesis or resection arthroplasty represent the only viable alternatives to maintain an adequate autonomy in activities of daily living. 25 Secondly, the severe bone loss caused a significant difficulty in choosing the most suitable positioning, orientation, and fixation of the new metaglene, and determined also the need to preserve the remaining bone stock. The most critical issues of shoulder reconstruction PSI-aided techniques are still represented by a proper exposure, preparation, and positioning of the implant. 22 In this context, intra-operative navigation could be of enormous help as it allows the surgeon to receive continuous real-time feedback both in terms of precision of baseplate positioning and screws’ direction and length. As a matter of fact, screws’ actual length and direction have been shown to correspond to the one provided by pre-operative planning. This technology, in expert hands, allows to minimize errors, and ensure stable fixation as already demonstrated in the literature with regards to primary RSA.11,13
Correct management of the infection, with well-defined diagnostic protocols and adequate revision techniques, combined with the possibility of customizing the implants to better adapt to the patient's altered anatomy, can further reduce the need for multiple revision procedures, ensuring good functionality and consequently patient satisfaction.
Conclusions
To the best of our knowledge, this is the first description of the use of intra-operative navigation in a complex case of revision surgery to implant a customized glenoid component of a RSA. When addressing to shoulder revision surgery, an accurate planning plays a role of primary importance. If due to instability, infection or any other existing technical errors affecting the previous implant must be detected and corrected, and the altered anatomy needs to be studied in depth. 3D-CT planning allows for a thorough knowledge of the extent of the bone defect, and an accurate assessment of its best management. PSI and custom-made implants can be deployed to treat even the most extensive bone losses, and their limits in terms of precision of fixation can be overcome by computer-assisted intra-operative navigation to preserve the residual bone stock. The combination of these techniques has proven to be highly effective in the management of an extremely complex RSA revision case.
Footnotes
Author Contributions
ET, GP, GBC, and NM wrote and reviewed the paper, cured editing. ET and IC cured data acquisition, collection and analysis, interpreted the data and drafted the work. NM and SG conceptualized the study, wrote, and reviewed the paper. All authors approved the submitted version and agreed to be accountable for all aspects of the work.
Consent for Publication
The patient gave his informed consent to data collection and their anonymous use for scientific and teaching purposes.
Availability of Data and Material
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Thanks to the University of Siena for the contribution made to the publication of this article.