
Abstract
Background
One of the most frequent complications in patients affected by traumatic anterior dislocations is bony Bankart lesion. This study evaluates the clinical and functional outcomes of 10 patients with isolated large glenoid fracture and acute glenohumeral dislocation treated with reverse shoulder arthroplasty.
Methods
Patients older than 69 years who underwent reverse shoulder arthroplasty after isolated large glenoid fracture and acute glenohumeral dislocation between 2016 and 2022 at the same institute were selected. Shoulder range of motion and pain level was assessed. The impact on quality of life has been evaluated through four measures: the constant scale, the simple shoulder test (SST), the OXFORD scale, and The University of California—Los Angeles (UCLA) shoulder scale.
Results
The mean Constant score was 77.1 (range 68–84), the mean SST score was 9.4 (range 8–10), the Oxford score was 44.3 (range 35–48), and the UCLA shoulder scale was 27.1 (range 24–30). No reoperation was performed on any patient in this series.
Conclusion
Reverse shoulder arthroplasty for elderly patients with bony Bankart lesion and acute glenohumeral dislocation represents a valuable option in terms of clinical results, patient satisfaction and early- to medium-term complications.
Introduction
Bony Bankart lesions represent one of the most frequent complications in patients affected by traumatic anterior dislocations, 1 with an incidence of 31.6%. 2 In most cases, due to the small size of the lesion, a conservative treatment can be choosen 3 while in other cases, percutaneous osteosynthesis in association with arthroscopic capsuloplasty represents the best option.4,5 Bony Bankart lesions with larger fragments necessitate of a more invasive approach 6 because of their high association with recurrent shoulder instability. 7 Nowadays, open reduction and internal fixation (ORIF) remains the gold standard for treating these types of lesions,8,9 even with its high rate of post-operative complications such as pseudoarthrosis, recurrent instability as well as frequent need of reoperation, in particular for older patients with associated risk factors (osteoporosis and cuff tear deficiency), which can compromise the outcome of the treatment. 10 The aim of the present study was to describe a case series of elderly patients with bony Bankart lesions with larger fragments with an associated pre-existing massive rotator cuff tear treated with reverse shoulder arthroplasty and to evaluate the clinical, radiological and subjective patient satisfaction outcomes.
Materials and Methods
Patients older than 69 years (range 69–82), who underwent reverse shoulder arthroplasty after traumatic anterior dislocation in association with bony Bankart lesion at the Surgical Orthopedic and Traumatological Institute (ICOT) of Latina and the Clinic of Orthopedic and Traumatological Surgery of the ASST Sette Laghi of Varese between 2016 and 2022, have been included in the study. Right after the emergency department access, and the diagnosis made from clinical and x-ray evaluation (Figure 1), all the affected shoulders have been examined through CT-scan (Figure 2), MRI and electromyography in order to delineate the fracture morphology, the status of the rotator cuff and any nervous damages, respectively. Patients with a bony Bankart fracture greater than 20% of the glenoid surface with a pre-existing massive cuff tear and in absence of nervous damages received the surgical indication.

Shoulder anterior dislocation.

Isolated large glenoid fracture.
A total of 10 patients (3 men, 7 women) were included in the study, mean age was 74.8, while the mean follow-up was 12 months with a minimum follow-up of 6 months.
For the outcomes and statistical analysis, we considered the following parameters: age, side, number of rotator cuff tendon ruptured (2 or 3 with supraspinatus always being lesioned), type of prosthesis implanted, use or non-use of metal augment or bone graft, Range of motion while clinical results using the functional scales: the constant scale (CS), the simple shoulder test (SST), the OXFORD Scale, and The University of California—Los Angeles (UCLA) shoulder scale. Patients were evaluated at 1, 3, 6, and 12 months after surgery, also with x-rays of the shoulder (Figure 3).

Post-operative control X-rays.
To analyze and process the data, the following software has been used: IBM SPSS Statistics 24.0. For this study, we used descriptive statistics. We used the Student’s t test with independent and paired samples for normally distributed data in order to assess the effect of cofactors on outcomes and differences between subpopulations and repeated measures over time. Using a multivariate analysis, the presence of any correlations between variables and/or cofactors was assessed. Subsequently, a linear regression analysis was carried out to determine whether these correlations were significant. The threshold of statistical significance was established for a P value < .05.
Surgical Technique
The patient was placed in a beach-chair position. The deltopectoral approach was preferred. Two centimeters of pectoralis major tendon was released, while the subscapularis tendon was tenotomized along with the long head of the biceps tendon. The humeral head was dislocated and cut with a 20° of retroversion. The humeral canal was prepared with specific broches. The glenoid was clearly exposed with a circumferential release while the fracture was individuated (Figure 4). Due to the anterior bone loss the “metal back tornier perform reversed” lateralized baseplate was placed and fixed with four screws (two compression screws and two stable interlocking screws). One of the screws was used to reduce the glenoid fracture. Glenosphere was then inserted. The Humeral canal was prepared for the trial implant. After the stability check, the definitive Aequalis Ascend flex short stem was placed, and in none of the cases was cemented. Tenodesis of the subscapularis tendon along with the long head of the biceps tendon was performed for every surgery. Articular drainage was placed. All the patients were immobilized in a neutral rotation. Post-operative x-rays were performed in all cases (Figure 5).
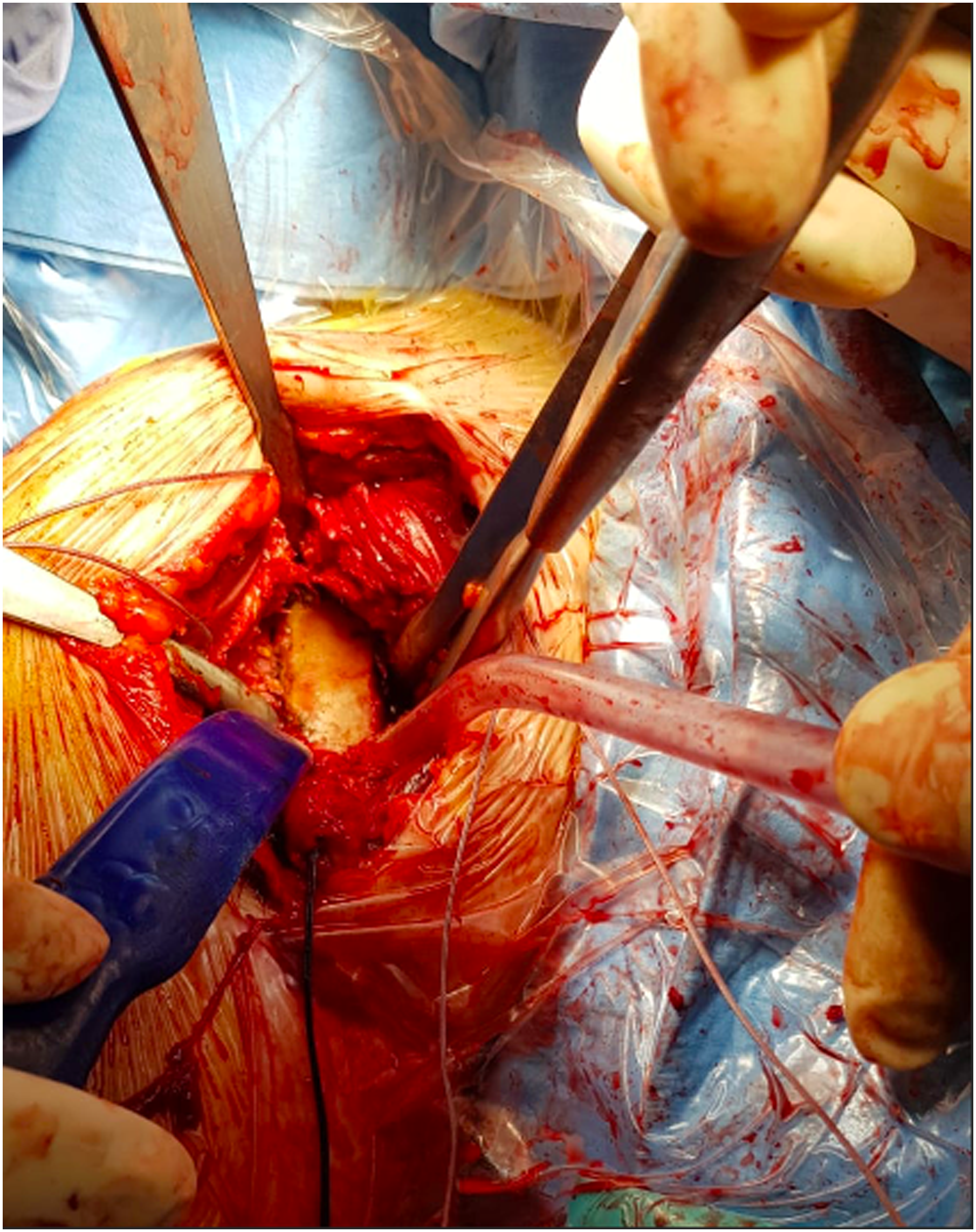
Large glenoid fracture.

Augmented glenoid.
Results
At final follow-up, average active elevation was 164° (range 150–180°), external rotation 21.5° (range 15–30°). The mean constant score was 77.1 (range 68–84), the mean SST score was 9.4 (range 8–10), the Oxford score was 44.3 (range 35–48), and the UCLA shoulder scale was 27.1 (range 24–30) (Table 1). No reoperation was performed on any patient in this series. No significant difference was found in the clinical results, obtained with constant score, Oxford score and SST, and the number of ruptured rotator cuff tendons, the type of implanted prosthesis and the use of bone graft/wedge metal augment or not. The only significance in the analysis was a slightly worse result at UCLA when implanted Tornier Aequalis prosthesis (UCLA only, the other scales no significant difference).
Clinical Outcomes.

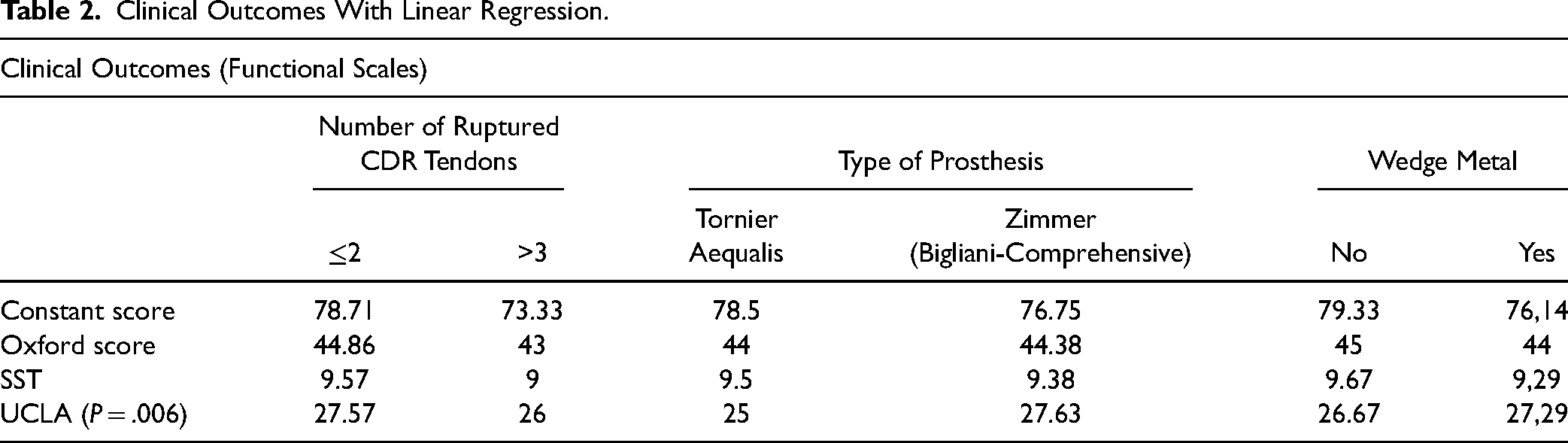
Furthermore, there was a trend towards significance when performing the linear regression between UCLA scale score and age with R-square of 0.35 and P = .072. (Table 2.)
Clinical Outcomes With Linear Regression.
Discussion
Around 20% of shoulder dislocations occur at an age of 60 or older 11 and they are associated with a 31.6% 2 risk of a concomitant glenoid fracture. Also, the number of future dislocations seem to be related to the size of the bone fragment. 12 In the elderly, the risk of recurrent anterior instability has been estimated around 22% after the first episode. 13 Moreover, in the elderly the risk of an acute cuff tear or the presence of a preexistent tear is higher. 14 Behalf the cohort of patients of the present study, we found positive clinical and radiological results as well as level of subjective satisfaction. Also, the patients seem to regain their full recreative activities around 12 weeks, without mid-term complications being recorded. Interestingly, the only significance, or tendency to significance, obtained is when the data are crossed with the UCLA functional scale; this suggests a certain sensitivity of the scale in the analysis of our data. Our results are in accordance with Maassen et al., 15 who reported a case of a proximal multifragmentary humeral fracture associated with a bony Bankart lesion treated with an RSA and a concomitant fixation of the glenoid. They reported excellent clinical outcomes with no complications and a full return to recreative activities in a one-year follow-up. Thus, the use of RSA permits a rapid functional regain avoiding dangerous complications such as ROM stiffness, cognitive impairment, post-traumatic arthritis and reoperation for fixing screws removal. Itoi et al., 16 in a cadaveric biomechanical study, found that a glenoid deficit superior of 21% is associated with recurrent instability and ROM reduction even after surgical fixation. The role of the cuff tear management appears to be as relevant as the management of the fracture. The gold standard for bony Bankart lesions remains the ORIF. 8 However, literature reports several complications for the procedure.
Dirk Mayer et al. 14 reported a 39% subscapularis insufficiency and a 23% post-traumatic osteoarthritis in the analyzed cases. Schandelmaier et al. 10 reported 2 fixation fails over 22 cases, as well as 2 infections. Also, in a systematic review of 15 studies evaluating the surgical treatment for bony Bankart lesions, Lantry et al. 17 found frequent complications due to the fixing screws, which needed to be removed in more than 7% of cases. Scheibel et al. 8 found a high rate of early complications in patients with articular fractures with a glenoid deficit superior of 25%. Moreover, the long period of immobilization could lead to articular stiffness and cognitive impairment in a fragile and elderly patient. Thus, for these types of patients a reverse shoulder arthroplasty should be considered as a treatment.
This implant has become a valuable option for the cure of eccentric arthritis as well for proximal humeral fracture in the elderly patient. 13 The literature presents a lack of studies analyzing bony Bankart treatment in the elderly. Garofalo et al. 18 studied 26 patients with bony Bankart associated to a proximal humeral fracture treated with RSA and bone grafting finding promising results with no major complication. The use of RSA, in elderly patients, for the treatment of these fractures should be considered after careful study of the tendon component. The main limitations of our study are the small number of patients and the lack of a control group undergoing conservative/ORIF treatment for the same pathology.
Conclusion
Reverse shoulder arthroplasty for elderly patients with bony Bankart lesion and rotator cuff deficiency after traumatic anterior dislocation represents a valuable option in terms of clinical results and patient satisfaction and short- to medium-term complications.
For all these reasons we believe that it is necessary in all patients over 65 with a dislocated fracture of the shoulder to have a study of the integrity of the rotator cuff, the fracture pattern of the glenoid and the degree of arthrosis present.
This type of treatment could avoid early to mid-term complications of ORIF, providing to the patient early mobilization and better clinical outcomes. Better comparative and well-designed studies are needed to define the specific treatment advantages as well as the long-term outcomes.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.