
Abstract
Background
This study assesses outcomes in revision shoulder replacements where the glenoid bone loss was managed using a structural allograft (donated femoral head) in combination with a trabecular titanium (TT) implant.
Methods
We contacted patients who had undergone revision shoulder arthroplasty using the Lima Axioma TT metal-backed glenoid with an allologous bone graft as a composite who were over 2 years since surgery. Patients underwent computerd tomography evaluation, clinical review, and scoring preoperatively, at 6 months and the latest follow-up.
Results
Fifteen patients were included with a mean age of 59 (33-76). The average follow-up period was 40.5 months (24-51). 80% showed satisfactory bone graft incorporation and peg integration at the latest follow-up. Three had signs of significant bone graft resorption, although in 2 patients the pegs were still soundly fixed in the host bone. Clinically all patients showed a statistically significant improvement in pain relief, movement, and function. No unusual complications were reported.
Conclusion
Results show femoral head structural allograft in combination with TT metal-backed glenoid baseplate is a viable option for revision total shoulder replacement in the context of massive glenoid bone loss. We do, however, acknowledge that this resorption rate is higher than in other reported series where autograft is used.
Keywords
Introduction
Over the last two decades there has been a dramatic increase in the number of shoulder arthroplasty procedures performed. In the United Kingdom, the National Joint Registry (NJR) estimates an increase in total shoulder arthroplasty (reverse or anatomic) of 4-fold over the most recent 7-year period. 1 As an almost inevitable result of this, the number of revisions has also increased (NJR, 2020). 2 These revision procedures are often technically demanding and as a consequence, a number of surgical techniques have been developed to try and attain a successful outcome.
Obtaining successful glenoid fixation in the presence of glenoid bone loss is one of the most challenging aspects of revision shoulder arthroplasty. Options to deal with this glenoid bone loss include taking autograft from the iliac crest, allograft, metallic augments, or bespoke implants. The morbidity from using the iliac crest donor site has been described previously. 3 At the time of surgery any available metal augments were frequently inadequate in managing the amount of bone loss often seen in revision arthroplasty. Finally, the long-term outcome of bespoke or custom implants remains unknown. The use of donated allograft, therefore, remains a viable option.
Previous studies using allograft have found varying success rates ranging from 92% bony union down to 45% at 12-month follow-up.4–7 Unfortunately, much of this published work does not standardize the implant choice nor the source or use of the allograft. That is, whether it is used as a structural graft or part of an impaction process.
Trabecular titanium (TT) is a highly porous material that mimics the morphology of trabecular bone. It has been used in complex hip arthroplasties with excellent results and was developed for clinical use in the shoulder in 2012 (Figure 1A and B). The SMR Axioma TT is a metal-backed glenoid baseplate that can be used for anatomic or reverse total shoulder arthroplasty (TSA). In vivo, studies have shown osseointegration with a high percentage of bone ingrowth.8–14

(A) Lima SMR Axioma trabecular titanium (TT) Implant. (B) (i) Stereomicroscopy image of metal bone interface. (ii) SEM with AU coating (30 × magnification). Images published with the kind permission of Dr Oana Bretanu, Newcastle University, School of Engineering.
The aim of this prospective study is to determine the clinical and radiographic outcomes of a reverse polarity shoulder arthroplasty (rTSA) using a trabecular metal baseplate in combination with a femoral head structural allograft to reconstruct glenoid bone deficiency in revision shoulder arthroplasty.
Materials and Methods
Patient Group
This is a single center study. We used our prospective arthroplasty database to identify patients who had undergone revision shoulder arthroplasty using a combination of the Lima SMR Axioma TT implant together with an allologous structural bone graft taken from a donated femoral head.
Ethical approval was prospectively attained, Rec number 17/YH/0318 (York and Humber Rec) IRAS 214242. This research is on the NIHR Portfolio.
The inclusion criteria were all patients who had more than a 2-year follow-up from surgery. Patients having undergone clinical and radiological assessment prior to surgery and at subsequent reviews. The latter included not only plain X-ray but also CT scanning. Informed consent was obtained in all cases.
Exclusion criteria included any patient who had supplementary autograft insertion either structural or impaction grafting.
Operative Technique
A standard deltopectoral approach was used in all patients, all of whom were revision cases. Following the dislocation of the prosthesis both the humeral and glenoid components, if present, were removed. Following a soft tissue release around the glenoid an inspection was undertaken to confirm the nature and the degree of glenoid bone loss. The glenoid was then prepared to accept the implant/allograft composite. Essentially, soft tissue and debris were removed using a reamer or burr. Hard cortical bone was removed down to a bleeding surface. Using cannulated/reaming system instruments the glenoid was prepared to accept the peg of the Lima SMR Axioma TT system.
On a side table, a structural allograft was harvested from a donated femoral head. These were fresh frozen and non-irradiated specimens. The donor graft and storage facility is overseen by the NHS Blood and Transplant (NHSBT) special authority. A rigid consenting and donor selection process is applied nationally to ensure safety in the use of these tissues.
Once the femoral head has warmed it is placed in a holding clamp. A guide wire is placed into the center of the femoral head and is advanced ∼5 cm. Initial cannulated reaming is undertaken to achieve conformity with the backside of the base plate. A central hole is then made for the TT peg using a central peg drill. The Lima Graftalogy saw is used to undercut the bone graft at the required level. The chosen peg and base plate are then impacted into the femoral head and a large reamer is used for the final separation of the implant/bone composite from the femoral head. Any further shaping of the graft can be undertaken using rongeurs (Figure 2).

Allograft bone preparation from donated femoral head.
The implant/allograft composite is then inserted into the prepared glenoid and impacted into place. The composite is then fixed by two, 4 mm, or 6.5 mm screws at 6 and 12 o’clock. In 13 cases, the revision was to a reverse total shoulder arthroplasty and in 2 to an anatomic total shoulder arthroplasty. In the latter group, the rotator cuff was noted to be functioning preoperatively and was found to be intact at the surgery. The humerus was then prepared for the appropriate component.
In 3 cases this was undertaken as a two-stage procedure, specifically the glenoid component/structural allograft was inserted as the first stage and somewhat later at a second operation the glenosphere and humeral component were inserted. The reason for this being at the first stage it was felt that the fixation of the composite was not secure enough to allow completion of the procedure. In these cases, prior to the second stage, a CT scan was undertaken to assess peg fixation and bone graft integration. The second procedure is being undertaken at a minimum of 4 months after the first. In the remaining 12 cases, the operation was completed in one stage.
Clinical Follow-Up
All patients included in the study had a minimum follow-up of 2 years. Outcome measures were the Oxford Shoulder Score (OSS) and American Shoulder and Elbow Score (ASES), as well as a range of motion including elevation and abduction. A complete set of post-operative assessment scores were available for all patients (n = 15).
Radiological Assessment
Preoperative radiographs and CT scans were reviewed to assess the glenoid bone defect. The CT scans were also used to template the implant size, peg length, correction required, and graft thickness. All the patients enrolled in the study had standard anteroposterior and axillary view radiographs and a CT scan (Siemens SOMATOM Definition AS + 128-slice; in 1-mm slices and metal artifact–reducing protocol using iMAR software).
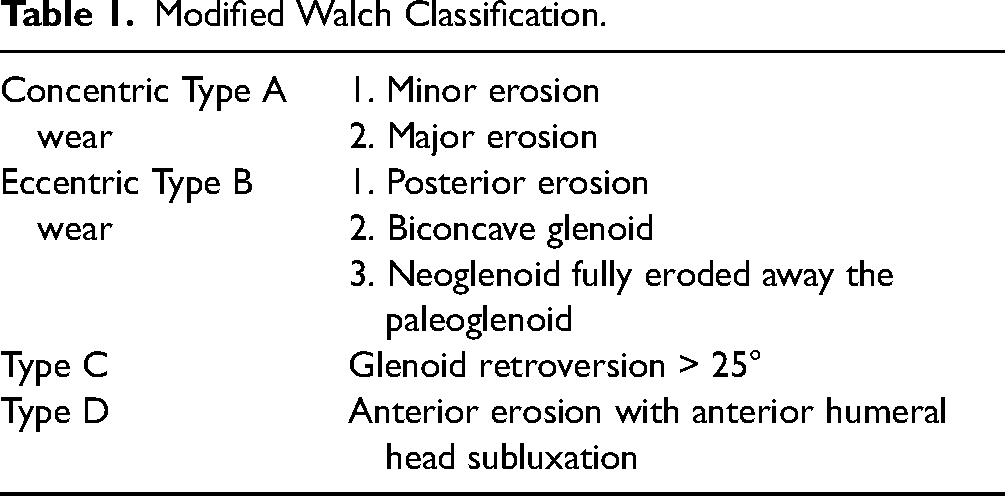
The modified Walch classification (Table 1) was used to assess glenoid wear in cases of shoulder arthroplasty where a glenoid component has not been implanted previously.
Modified Walch Classification.
In revisions involving a glenoid component, the volume, and depth of the vault are the 2 important factors to consider. Bony deficits were graded as per the modified Antuna classification as shown in Table 2.
Modified Antuna Classification With Severe Glenoid Loss.

Radiographic Assessment of Bone Graft Incorporation and Volumetric Change
Three of the authors assessed the postoperative CT scans to evaluate osseointegration of the glenoid peg with the native glenoid and graft integration and incorporation into the native glenoid.
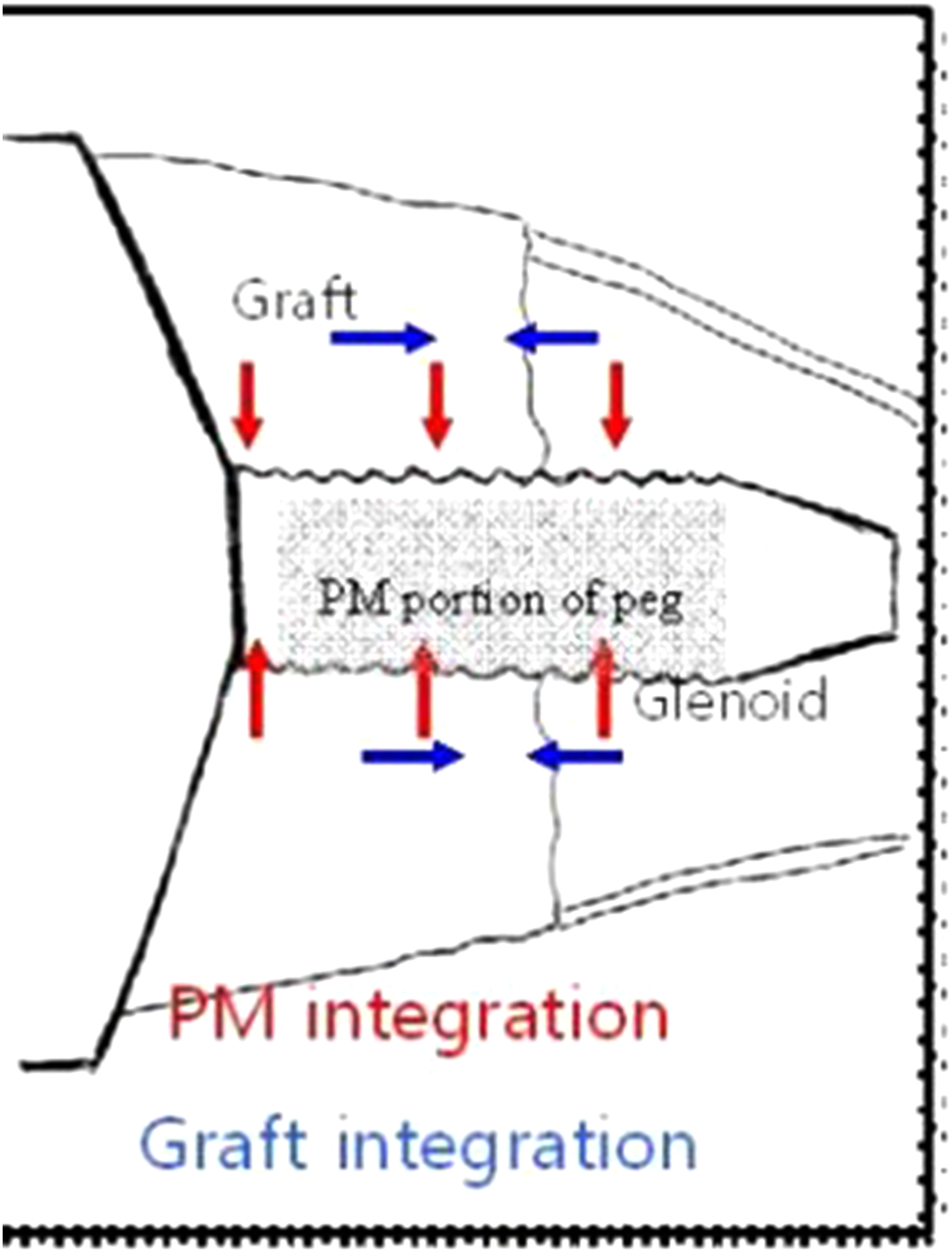
Crossing trabecular bone and no visible gap between the peg and native glenoid were the markers for integration. Images in axial and coronal planes were reviewed in bony windows. To standardize the methodology, we scrolled across the baseplate to look for the porous titanium portion of the peg, the bone graft, and the native glenoid to grade peg integration and bone graft incorporation. Serial postoperative CT scans (6 months and latest) were reviewed to assess evidence of incorporation or integration of peg and notching. Figure 3 shows the assessment of peg integration with the graft and native glenoid as demonstrated by red arrows and graded as no or < 50% integration (1 or 2) and > 50% or complete integration (3 or 4). Table 3 using the Granville-Chapman classification 15 shows the assessment of glenoid graft incorporation and is graded from A to D with A complete lysis of the graft and D complete incorporation.
Granville-Chapman classification system for osseointegration of glenoid peg and incorporation of bone graft.
Assessment Quantification of Bone Graft Integration Into Implant Peg and Host Bone.

To determine the volume of the bone graft (Figure 4), we scrolled around the coronal and axial planes and used the back of the baseplate and distance from the central peg as fixed points to determine the volume of the bone graft. We used the mathematical formula of the volume of a cylinder, π R12h (R1 being the radius of the bone graft and h, the height). From this, we subtracted the volume of the Peg using the same formula π R22h (where R2 is the radius of the peg) (Figure 4). To simplify the calculations, we used the following formula:

Schematic descriptions of the volume of cylinder concept applied to the implant bone graft composite.
We used an average of 3 readings of both R1 and R2 in the coronal sagittal, and axial slices of the CT scans.
Statistical Analysis
Descriptive statistics are reported as mean, median, and range for continuous measures and percentage for discrete measures. A paired t-test was used to compare the preoperative versus postoperative changes in the range of movement, Oxford Shoulder Scores, Constant shoulder scores, and ASES.
Results
Patient Group
Fifteen patients were identified from the arthroplasty database for inclusion in the study. The mean age of patients was 59 years (range 33-76 years). There were 11 women and 4 men. The average follow-up period was 40.5 months (range 24-51).
Revision arthroplasty was performed in all 15 cases, with revision to a reverse shoulder replacement in 13 and to anatomic total shoulder replacement in 2. Of these 4 were undertaken for infection with the reverse/allograft composite being used as a second stage after biopsies had shown that the infection had been eliminated. Of the 15, 11 were for revision from a hemiarthroplasty (2 surface replacements and 9 stemmed implants) and 4 were revisions from an anatomic total shoulder replacement. The indications for surgery in the hemiarthroplasty group were cuff failure and instability in 4 and glenoid erosion in 7. For the anatomical total shoulder replacement, all were for loose glenoid components.
Preoperative imaging was available in all 15 cases and the appearances of the glenoid are given in Table 4. As can be seen, all cases had significant glenoid bone loss.
Preoperative Classification of Glenoid Erosion (n = 15).

Radiographic Outcomes (Table 5)
All patients had preoperative and postoperative X-rays and CT scans available for review. Post-operative CT scans were undertaken at 45 months (± 11.6) from surgery.
Bone Graft Incorporation and Volume Change Over a Minimum of 2-Year Interval (n = 15).

Satisfactory bone graft incorporation was seen in 12 cases (80%). In 3 cases, however, there was complete lysis of the bone graft. An interesting observation was that in 2 of these 3 cases, the revision had been undertaken for infection. Of these 3, 2 pegs were well integrated into the host bone and 1 was loose (Figure 5A and B).

(A) CT scan at latest follow-up showing complete integration of bone graft and peg. (B) CT scan at the latest follow-up showing lysis of bone graft and loosening of the peg.
Finally of the 15 cases, notching was seen in 6. Using the Nerot classification 16 2 were grade 2, 3 grade 3, and 1 grade 4.
Volumetric Assessment (Table 5)
Using the above-measured formula, the mean volume of the graft in the immediate postoperative CT scans was noted to be 7499 mm3 (±2612 mm3). The volume of the bone graft in the final CT scans was 6125 mm3 ± 2.18 mm. While this showed some diminution in the size of the allograft this reduction was not statistically significant (P = .09) (Table 5).
As can be seen in Table 6, all patients in this series reported a significant improvement in function and movements, specifically abduction. While there was also an increase in elevation after surgery this was not statistically significant.
Clinical Outcomes.

ASES, American Shoulder and Elbow Score.
Of the 3 patients where bone graft lysis was seen at the latest follow-up, the 2 with satisfactory peg integration into the host bone were coping well with little pain and satisfactory shoulder movement and function. The patient with both bone graft lysis and the loose peg is currently unfit for surgery.
Complications and Reoperations
In this series, there were 4 significant complications. One patient developed an hematoma postoperatively which required a second surgical procedure.
A second patient developed a loosening of the humeral component. Currently, this patient remains under review pending further revision. A third patient sustained a peri-prosthetic humeral fracture as a consequence of a fall and this required revision surgery.
Finally, one patient developed significant stiffness post-operatively which has continued. No further surgery has been undertaken.
Of the 4 infected cases, there have been no clinical recurrences.
Discussion
Bone grafting for glenoid deficiencies was utilized by Neer over 3 decades ago, with his series of 20 cases showing that incorporation is enough to allow glenoid implantation. This series, however, is unlikely to have had massive uncontained glenoid defects as those cases that were deemed unreconstructable received a hemiarthroplasty.
Newer implants with metal-backed porous titanium pegged prostheses (like the Lima SMR Axioma TT) have extended the scope of glenoid reconstruction arthroplasty with the capacity for single-stage implantation. Evaluating structural bone graft incorporation and porous metal integration, however, remains a challenge with plain radiographs only able to offer a limited assessment.17,18 Radiostereographic analysis has been used to assess migration but again does not allow for any quantitative assessment of any incorporated bone graft. 19
Whereas autograft glenoid reconstruction has been proven to be a reliable technique with over 90% bone graft survival and peg incorporation, 3 humeral head autograft is not normally available in the revision setting. While autogenous bone grafts can be taken from other sites including the iliac crest, this can lead to increased morbidity. 3 As such a donated allograft has always been considered as a viable alternative as it is readily available and would not result in increased patient morbidity.
Articles investigating the use of allograft in complex shoulder arthroplasty are however relatively few. Femoral head allograft used in a revision setting has shown wide variability in graft incorporation ranging from 70% through to 82%.7,16,20,21 However, many of these studies use only plain X-rays to assess integration and the allograft was used in various modalities either structural or as part of an impaction process. The only article to use CT scanning was by Lopiz et al, 5 who assessed 13 cases using allograft from either the femur or predominantly the tibial plateau used as a structural graft. Unfortunately, this was a mixture of allograft and autograft. However, the authors were able to show at a mean follow-up of 26 months that the bone graft was fully incorporated in 95% of cases. They did, however, report a 20% postoperative complication rate with 1 case of glenoid component loosening, 1 surgical wound hematoma, 1 acromial fracture, and 1 grade 3 symptomatic scapular notching.
In this study a structural femoral head allograft was used in preference to allograft from other sites due in part to its availability through the National Bone Bank but also it’s strength and structural superiority. Another advantage is that we were able to produce an implant/bone graft composite which in the majority of cases allows immediate fixation both by peg insertion into the host bone and also screw fixation.
Using detailed CT evaluation, we were able to show that at a mean of 45 months after surgery, 80% of the allograft had integrated into both the host bone and implant peg. In addition, while we were able to show a reduction in bone graft volume at the latest follow up this was not statistically significant. We do, however, acknowledge that these results are not as good as when autograft is used. However, following a detailed analysis of our failures we have not been able to shed further light on this difference. One observation, however, was that in 2 of the 3 cases where resorption was noted, these were in patients who had undergone revision for previous infection.
Clinically we were able to report significant improvement in pain relief, movement, and function in all patients. This was statistically significant and mirrors other similar studies. In addition given the extensive nature of this surgery complications would not be unusual. We do not, however, believe that any of the ones noted in this series would be unexpected. Lastly, the rate of notching at 40% is consistent with the literature.17,22,23
The strengths of this study lie in its prospective design, which to our knowledge is the first on this topic. It is also from a single-center study utilizing only 1 implant with patient recruitment over a relatively short time period. In addition, all patients received the same type of structural allograft and had a CT follow-up to assess graft resorption and implant incorporation. There was no loss to follow-up. The National Joint Registry in the UK allows the operating surgeon to check whether any patient had a further procedure outside of their institution; this did not occur in this series.
The limitations of this study are the small number of cases included. We do not, however, believe this is unusual given the subject matter and our number is comparable to similar studies. We also acknowledge that follow-up is relatively short with a mean of almost three and a half years. It is our opinion, however, that it is unlikely that there will be any further bone graft resorption after this time period.
Conclusion
The short-term results of this single-center series show that femoral head structural allograft in combination with TT metal-backed glenoid base plate is a viable option for revision total shoulder arthroplasty in the context of massive glenoid bone loss. However, it should be noted that in 20% of cases, the allograft had resorbed at the latest follow-up. The reason for this remains unclear.
Footnotes
Acknowledgments
The authors thank the Upper Limb Research Unit for their help and support with this project. They also thank Diane Allmark for typing the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Committee Approval
Reference number—17/YH/0318, NHS Health Research Authority, Yorkshire & The Humber—Sheffield Research Ethics Committee.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.