
Abstract
Purpose
To describe the reverse shoulder arthroplasty angle (RSA angle) in magnetic resonance imaging (MRI) and compare the angle formed using bony landmarks (Bony RSA angle or B-RSA angle) with another angle formed using the cartilage margin as reference (Cartilage RSA angle or C-RSA angle).
Methods
Adult patients with a shoulder MRI obtained in our hospital between July 2020 and July 2021 were included. The C-RSA angle and B-RSA angle were measured. All images were independently assessed by 4 evaluators. Intraclass correlation coefficient (ICC) was determined for the B-RSA and C-RSA to evaluate interobserver agreement.
Results
A total of 61 patients were included with a median age of 59 years (17-77). C-RSA angle was significantly higher than B-RSA (25.4° ± 0.7 vs 19.5° ± 0.7, respectively) with a P-value <.001. The overall agreement was considered “good” for C-RSA (ICC = 0.74 [95% CI 0.61-0.83]) and “excellent” for B-RSA angle (ICC = 0.76 [95% CI 0.65-0.85]).
Conclusions
C-RSA angle is significantly higher than B-RSA angle. In cases without significant glenoid wear neglecting to account for the remaining articular cartilage at the inferior glenoid margin may result in superior inclination of standard surgical guides.
Keywords
Introduction
Pre-operative planning is key to achieve good results and avoid complications in reverse shoulder arthroplasty (RSA) surgery.1–3 Superior inclination of the glenoid component has been associated with elevated risk of aseptic loosening and poor functional outcomes.4,5 An inferior tilt between 0 and 10° is recommended to achieve good results and avoid the “rocking horse effect”.5–7
Computed tomography (CT) is widely used for 2D and 3D preoperative planning based on bony landmarks. Boileau et al 8 described the reverse shoulder angle (RSA angle) to better estimate the inferior glenoid inclination as opposed to the β-angle,9,10 or also called the total shoulder arthroplasty angle (TSA angle), that accounts for the vertical inclination of the complete glenoid (Figure 1). RSA angle is widely used among shoulder surgeons for 2D and 3D preoperative planning of the glenoid baseplate. Though evidence suggests that magnetic resonance imaging (MRI) can accurately determine version and inclination in most cases,11,12 available pre-operative planning software use only CT.2,13

TSA and RSA angles as described by Boileau et al. 8 Supraspinatus fossa line is depicted in blue. RSA angle better describes the inclination of the inferior glenoid, while TSA angle measures the inclination of the complete glenoid.
The articular cartilage of the glenoid is thicker at the periphery 14 and may be present in common RSA indications such as cuff tear arthropathy and fracture. To estimate glenoid inclination intraoperatively, surgical instrumentation is set at the inferior glenoid rim. If the presence of articular cartilage at the inferior glenoid rim has a significant impact on the estimation of glenoid inclination remains unknown. The purpose of this study is to describe the RSA angle in MRI and compare the angle formed using bony landmarks (Bony RSA angle or B-RSA angle) with another angle formed using the cartilage margin as reference (Cartilage RSA angle or C-RSA angle). We hypothesize that C-RSA angle will be significantly higher than B-RSA angle.
Material and Methods
Population
An observational retrospective study was designed. Adult patients (17 years old and older) with a shoulder MRI obtained in our hospital between July 2020 and July 2021 were included. Basic demographic data such as age, sex, and studied side was obtained. Exclusions entailed patients with tumoral lesions, congenital deformities, and glenoid fractures. The study was conducted in concordance with the Declaration of Helsinki and was approved by our Institutional Review Board.
MRI Acquisition and Measurements
The MRI acquisitions were made in a Philips™ Ingenia 1.5T MRI scanner (The Netherlands) using a dedicated shoulder RF coil (8 channels). A standardized protocol was carried out using as reference the scapular coronal axis and sequentially including sagittal and axial planes acquisitions. The field of view was 140 × 140 mm. The C-RSA angle and B-RSA angle were measured in the coronal proton density fat suppressed images (Figure 2). Glenoid articular cartilage thickness at the intersection with the suprascapular fossa line and at the inferior rim was measured. To better characterize the sample, glenoid version, subluxation index, state of the rotator cuff, tendon retraction (according to Patte 15 ), Goutallier classification 16 (fatty infiltration), and glenoid chondral lesions (if present) were noted in every case. For chondral lesions severity was recorded according to the International Cartilage Repair Society (ICRS) classification. 17 Finally, TSA angle was also recorded in the same fashion as RSA angle using bony (B-TSA) and cartilaginous (C-TSA) landmarks.
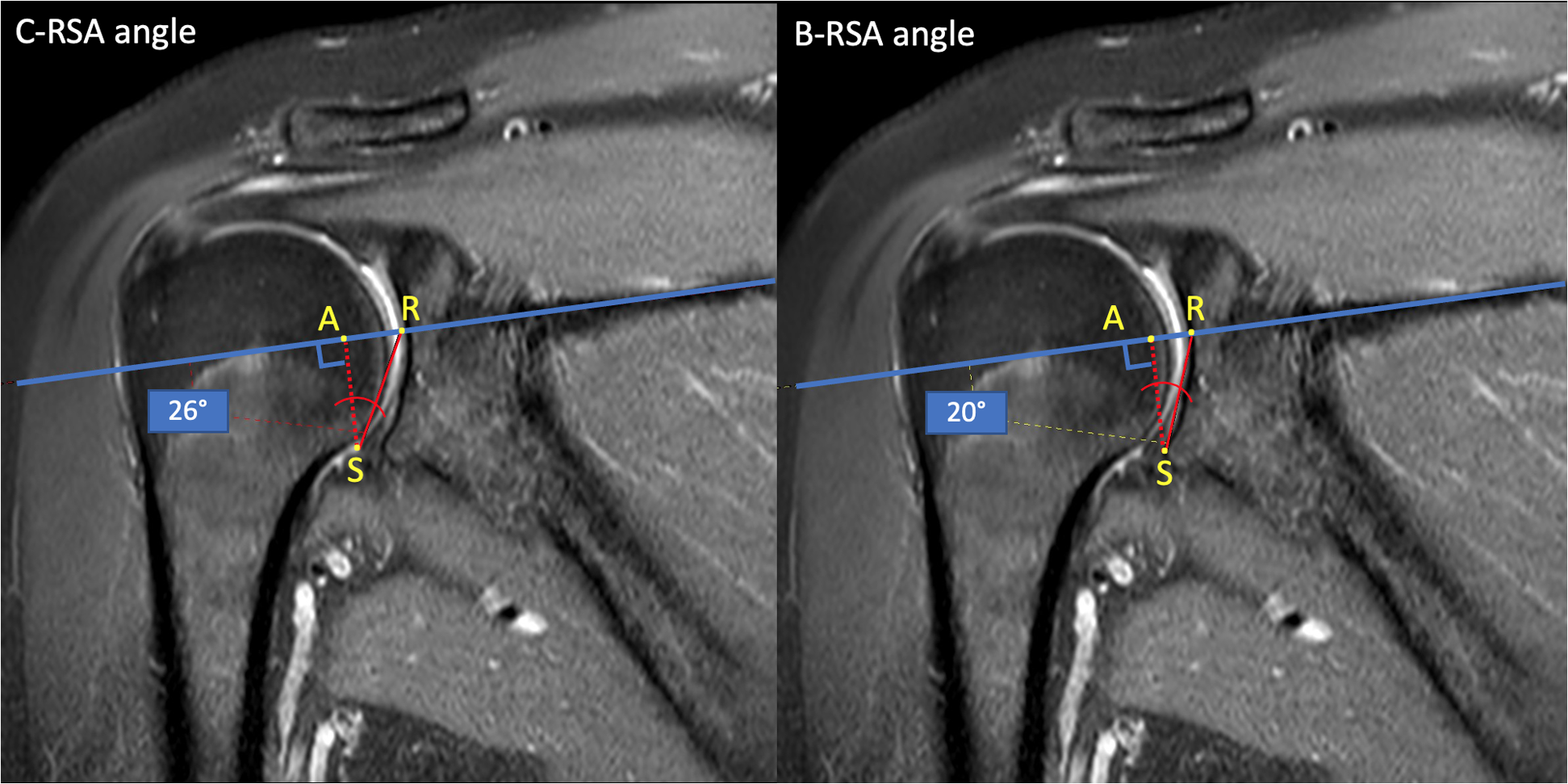
C-RSA angle and B-RSA angle. Supraspinatus fossa line is depicted in blue. Note that RSA angle changes significantly depending on whether is measured using the articular cartilage or the bone as reference.
All images were independently assessed by 4 authors representing distinct levels of training: 2 fellowship-trained shoulder surgeons, 1 fellowship-trained musculoskeletal radiologist, and 1 senior orthopedic surgery resident. Each one evaluated the images using the institutional imaging system RIS-PACS (Centricity 6.05, General Electric Healthcare™, Barrington, Illinois USA). All evaluators were blind to demographic and clinical data, as well as reports or any other images from the patient.
Statistical Analysis
We calculated a sample size of 61 shoulders as sufficient with a margin of error of 1.5°, 80% power, and 95% confidence, based on previously reported RSA angle standard deviation of 6° in 2D CT. 8 Normality was assessed using the Shapiro-Wilk test. All data and measurements were expressed as frequencies and mean ± standard deviation. We studied the univariate association of comparative variables using chi-square or Fisher's exact test in categorical variables, and paired t-test for continuous outcomes. The reliability of the measurements between the evaluators was estimated using the intraclass correlation coefficient (ICC). Correlations were interpreted as poor (0-0.39), fair (0.4-0.59), good (0.6-0.74), or excellent (≥0.75). Statistical analysis was carried out using R (The R Project for Statistical Computing, Vienna, Austria), Stata™ 13 (StataCorp. 2013. Stata Statistical Software: Release 13. College Station, TX: StataCorp LP), and Microsoft Excel™ considering a significance of 5%.
Results
Sample Characteristics
Sixty-one patients were included, with a median age of 59 years (ranging between 17 and 77 years old), 52.4% (32) female, 69% (42) right shoulders. Table 1 summarizes the rotator cuff pathology found according to its severity. Of note, most patients had a rotator cuff tear without significant retraction or fatty infiltration. Glenoid chondral lesions were present in 29.5% (18). From that set of patients, 83.3% (15) had grade (G) 1 lesions and 16.7% (3) G2 lesions, with no patients having G3 or G4 lesions. All chondral defects were at or superior to the glenoid equator. Glenoid characteristics are further detailed in Table 2.
Rotator Cuff Pathology.

G, Goutallier stage; RCT, rotator cuff tear; n, number of observations.
Glenoid Characteristics.

IGR, inferior glenoid rim; SFL, supraspinatus fossa line; PSI, posterior subluxation index; G, Grade; sd, standard deviation; n, number of observations.
Measurements
C-RSA angle was significantly higher than B-RSA angle (25.4° ± 0.7° vs 19.5° ± 0.7°, respectively) with a P-value <.001. Table 3 compares the TSA and RSA angles according to the landmarks used for their measurement. Articular cartilage at the inferior glenoid rim was in average 1.3 mm thicker than at the level of the supraspinatus fossa (P < .01). A subgroup of patients with functionally irreparable rotator cuff tears 18 were identified as “arthroplasty candidates” to further analyze the difference between B-RSA angle and C-RSA angle. In this subset of subjects in which RSA may be indicated, C-RSA angle was also significantly higher than B-RSA angle with mean values comparable to the rest of the studied population (Figure 3).

Mean and standard deviation of B-RSA angle and RSA-angle for the total sample and the “arthroplasty candidate” group.
Comparison Between RSA Angle and TSA Angle Using Bone or Cartilage as Reference.

Mean and standard deviation are shown for each variable.
Agreement
The overall agreement between the 4 evaluators was considered “good” for C-RSA (ICC = 0.74 [95% CI 0.61-0.83]) and “excellent” for B-RSA angle (ICC = 0.76 [95% CI 0.65-0.85]).
Discussion
In this study, we proposed a new MRI measurement, the C-RSA angle, based on the previously reported RSA angle in CT. In our study, C-RSA angle was approximately 6° greater than B-RSA (25.4° ± 0.7° vs 19.5° ± 0.7°) confirming our hypothesis that C-RSA angle would be significantly higher than B-RSA angle.
Interestingly, the average B-RSA angle in our study (19.5° ± 0.7°) was very similar to the value that was reported for RSA angle in 2D CT (20° ± 6°) by Boileau et al. 8 This is consistent with previous reports comparing CT and MRI to measure glenoid version and inclination that found comparable results between these 2 modalities. 19 Of note, a proper validation of RSA angle in MRI would have required to directly compare MRI and CT images from the same pool of patients, but that was out of the scope of our study.
The development of 3-dimensional imaging techniques and computerized planning for shoulder arthroplasty has aided surgeons with preoperative planning; however, the software planned arthroplasty era advances, and correct translation to patient is crucial. 20 There are various technologies that help surgeons to translate planning to surgery. Patient-specific instrumentation (PSI), navigation, robotic assistance, and mixed or augmented reality have been proposed.20–22 PSI uses CT 3D reconstructions to build custom-made jigs to guide pin placement based on the bony anatomy of the patient. Typical guide landmarks include the center of the glenoid, the glenoid rim, and the base of the coracoid. 20 Berhouet et al 23 and Gauci et al 19 using 4-point contact PSI (coracoid base and superior, anterior, and inferior glenoid margins) reported low deviation from preoperative planning, but with considerable variability (−0.4° ± 4.9° and 1.8° ± 5.3°, respectively). When comparing PSI guides that reference the inferior glenoid rim with those that mainly set on the center of the glenoid and the coracoid base, both achieve excellent accuracy but less variability is reported for the latter.24–28 Whether this observation is clinically relevant is yet to be elucidated. Standard instrumentation is more frequently used than PSI in clinical practice and has a lower direct cost. Deviation from preoperative plan for standard instrumentation is reported to be 5-6° in average with significantly more outliers than PSI.29,30 In cases without significant glenoid wear neglecting to account for the remaining articular cartilage at the inferior glenoid margin may result in superior inclination of standard surgical guides (Figure 4).

Images show the aspect of a glenoid instrumentation guide sitting at the glenoid rim in a cadaveric specimen with (A) and without (B) articular cartilage. Images C and D show the aspect under fluoroscopy of the images A and B, respectively.
In our study, the glenoid inclination (RSA angle) and version were reliably measured using MRI. Future studies may further investigate the role of MRI in the preoperative planning of shoulder arthroplasty. Moreover, MRI-based PSI guides have been studied for total knee arthroplasty providing favorable alignment outcomes while sparing the radiation dose of a CT. 31
This study has many limitations. We did not select arthroplasty patients, although some arthroplasty patients do not necessarily have any glenoid wearing, it would have been ideal to select a cohort of arthroplasty candidate patients. Another limitation is the fact that we did not compare B-RSA angle and C-RSA angle directly with RSA angle in CT (the “gold standard”).
Strengths of this study include a sufficient sample size (established a priori), with measures performed by various observers with different levels of training and with good levels of correlation. To our knowledge, this is the first study to evaluate the impact of the articular cartilage in the estimated inclination of the inferior glenoid.
Conclusion
RSA angle can be reliably measured using MRI. C-RSA angle is significantly higher than B-RSA angle. In cases without significant glenoid wear neglecting to account for the remaining articular cartilage at the inferior glenoid margin may result in superior inclination of standard surgical guides. Future studies may elucidate the clinical relevance of these findings.
Footnotes
Acknowledgments
The authors acknowledge their families for their unconditional support.
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by Julio Contreras, Cristobal Palma, Manuela Angulo, Catalina Vidal, Claudio Calvo, and Rodrigo de Marinis. The first draft of the manuscript was written by Rodrigo de Marinis and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee “Comité Ético Científico Hospital Dr Sótero del Río” (IRB N° 1116) June 2021.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.