
Abstract
Introduction
Total elbow arthroplasty (TEA) is an increasingly popular surgical option for many debilitating conditions of the elbow. There currently exists a paucity of literature regarding patient and hospital factors that lead to inferior outcomes following TEA. The purpose of this study is to identify independent predictors of increased complication and revision rates following TEA.
Methods
The National Readmissions Database (NRD) was queried from 2011 to 2018 to identify all cases of TEA (n = 8932). Relevant patient demographic factors, comorbidities, and hospital characteristics were identified and run in a univariate binomial logistic regression model. All significant variables were included in a multivariate binomial logistic regression model for data analysis.
Results
Independent predictors of increased complication rates included age, female sex, Medicare and Medicaid payer status, medium bed-sized center, and 18 of 34 medical comorbidities (all P < .05). Independent predictors of increased revision rates included medium bed-sized centers, non-teaching hospital status, chronic pulmonary disease, depression, and pulmonary circulatory disorders (all P < .05).
Conclusion
This study identified several patient and hospital characteristics that are independently associated with both increased complication and revision rates following TEA. This information can aid orthopedic surgeons during shared decision making when considering TEA in patients.
Level of Evidence
Level III, retrospective cohort study.
Introduction
Total elbow arthroplasty (TEA) has been available for several decades as a surgical option for severe debilitating conditions of the elbow. There are currently an estimated 3000 TEA procedures that take place in the United States yearly, though the actual number may be slightly less based on data from recent studies.1–4 One theory for the limited growth of TEA in recent decades is the rapid improvement of disease-modifying antirheumatic drugs which have shifted the use of TEA away from inflammatory arthropathy-related indications, which were traditionally one of the most common indications for TEA. 5 However, TEA is still used to treat debilitating elbow pain and dysfunction most commonly due to osteoarthritis, post-traumatic arthritis, acute fracture, neoplasm, or other mechanical indications. 6
Several studies have documented the outcomes of TEA, showing mixed results. Some of the most common complications of TEA include infection, aseptic loosening, and peri-prosthetic fracture. 5 Zhou et al in 2016 investigated 3146 patients who received TEA and identified an overall 30-day complication rate of 3.1%, readmission rate of 4.4%, and revision rate of 0.5%, results overall comparable to arthroplasties of the hip and knee. 4 Other studies and systematic reviews have looked to identify specific patient characteristics that are associated with poor outcomes following TEA, and include young age, obesity, diabetes, smoking, hypothyroidism, rheumatoid arthritis, and overall high comorbidity burden.7–14
Additionally, several recent studies have identified patient and hospital factors that are associated with inferior outcomes following total hip arthroplasty, total knee arthroplasty, and total shoulder arthroplasty (TSA).15–28 Patient factors like sex, insurance status, income, and race have all been identified as factors that lead to inferior outcomes following total joint arthroplasty.15–20 Increasing hospital volume has also been associated with superior outcomes for both TSA and TEA.21,23 Several patient comorbidities that are potentially predictive of inferior outcomes have also been identified for TSA, including depression, obesity, chronic lung disease, chronic renal disease, heart disease, paraplegia, and history of a previous solid organ transplant.22,24–28
Therefore, the purpose of this study is to determine what patient demographic factors, hospital characteristics, and medical comorbidities affect 90-day complication and revision rates following TEA. Current literature is limited to 30-day complication and revision rates, only accounting for events that occurred within the first 30 days after surgery. Extending the follow-up period to 90 days provides a more robust analysis of outcomes allowing surgeons to identify high risk patients and plan accordingly to limit the adverse events associated with TEAs. Additionally, this kind of information is essential to estimating financial risk in health systems with hospitals and surgeons that are part of a 90-day bundled payment program involving elbow arthroplasty. The hypothesis is that both patient and hospital factors will be independent predictors of increased 90-day complications and revision rates following TEA.
Materials and Methods
The Nationwide Readmissions Database (NRD) was queried from 2010 to 2018 for this study. The NRD is a large, de-identified, publicly available national registry of inpatient hospital admissions in the United States maintained by the federal Healthcare Cost and Utilization Project (HCUP). It contains data on hospital admissions from 27 states and represents a sample of approximately 58% of the US population. The database contains a patient linker variable that allows for the analysis of all same-state patient admissions at participating centers over the course of a year, allowing for the collection of outcome data on complications and revisions following operative hospital stays. A follow-up period of 90 days was established for this study by excluding patients admitted during the last 3 months of the year in order to ensure that all patients have at least 90 days of follow-up available in the database, in accordance with the methods of previous similar studies.21,29 This is necessary as patient linker variables change at the beginning of each year, making it impossible to track patients through multiple years. The database also provides a discharge weight coefficient variable that allows for the extrapolation of data to represent the entire US population. This coefficient was applied for this study and was then multiplied by a factor of 4/3 to account for the patients admitted during the last quarter of the year that were excluded to establish the minimum 90-day follow-up. Patients who had surgery in the fourth quarter of the year were eliminated because they did not meet the minimum follow-up requirement. Using this methodology accounted for the excluded patients and ensured all patients with any 90-day readmissions or complications were captured for the analysis.
Cases of TEA were identified using ICD-9 and ICD-10 codes for primary TEA (ICD-9 code 8184; ICD-10 codes 0RRL0JZ, 0RRM0JZ). Cases of revision TEA were identified similarly using ICD codes for revision and removal of hardware (ICD-9 codes 8197, 8002; ICD-10 codes 0RPL0JZ, 0RWP0JZ, 0RPL0JZ, 0RPM0JZ). To ensure that the revision was performed on the TEA of interest, all patients with previous upper-extremity arthroplasties were excluded from the analysis. A total weighted sample of 8932 primary TEA were included in the study. The primary diagnosis code for this sample included elbow fracture (61.7%), osteoarthritis (13.1%), rheumatoid arthritis (11.0%), post-traumatic arthritis (8.14%), and other (6.00%).
Information of patient demographics, hospital characteristics, and medical comorbidities was provided by the NRD and was utilized in this study. Patient demographic information included in the database includes age, sex, mean ZIP-code income quartile, and primary payer (Table 1). Primary payer data included Medicare (federal health insurance for individuals 65 and older), Medicaid (federal health insurance for individuals with low income), and private insurance. Data on patient race or ethnicity is not available in the NRD. Hospital characteristics include location (metropolitan vs non-metropolitan), hospital ownership (government owned non-federal, private non-profit, private investor-owned), bed size, and teaching status (Table 2). Hospital bed size definitions vary based on the region of hospital location as well as teaching status. Small hospital beds across the United States in urban, nonteaching hospitals have a bedsize range between 1 and 124, medium sized hospitals range between 125 and 199 and large hospital bedsize is 200 and up. In urban teaching hospitals the bed size definition changes. Small hospitals have a bed size range between 1 and 249, medium hospitals range from 250 to 450 and large hospitals are 325 or more depending on the location. 30 Patient comorbidity information was provided by Elixhauser Comorbidity Software from HCUP as well as independent identification of ICD-9 and ICD-10 codes for relevant medical comorbidities (Table 3). Comorbidity information was also used to calculate the Charlson-Deyo comorbidity index.
Univariate Logistic Regression Analysis of Patient Factors on 90-Day TEA Complication and Revision Rates.

*Statistical significance.
Univariate Logistic Regression Analysis of Hospital Factors on 90-Day TEA Complication and Revision Rates.
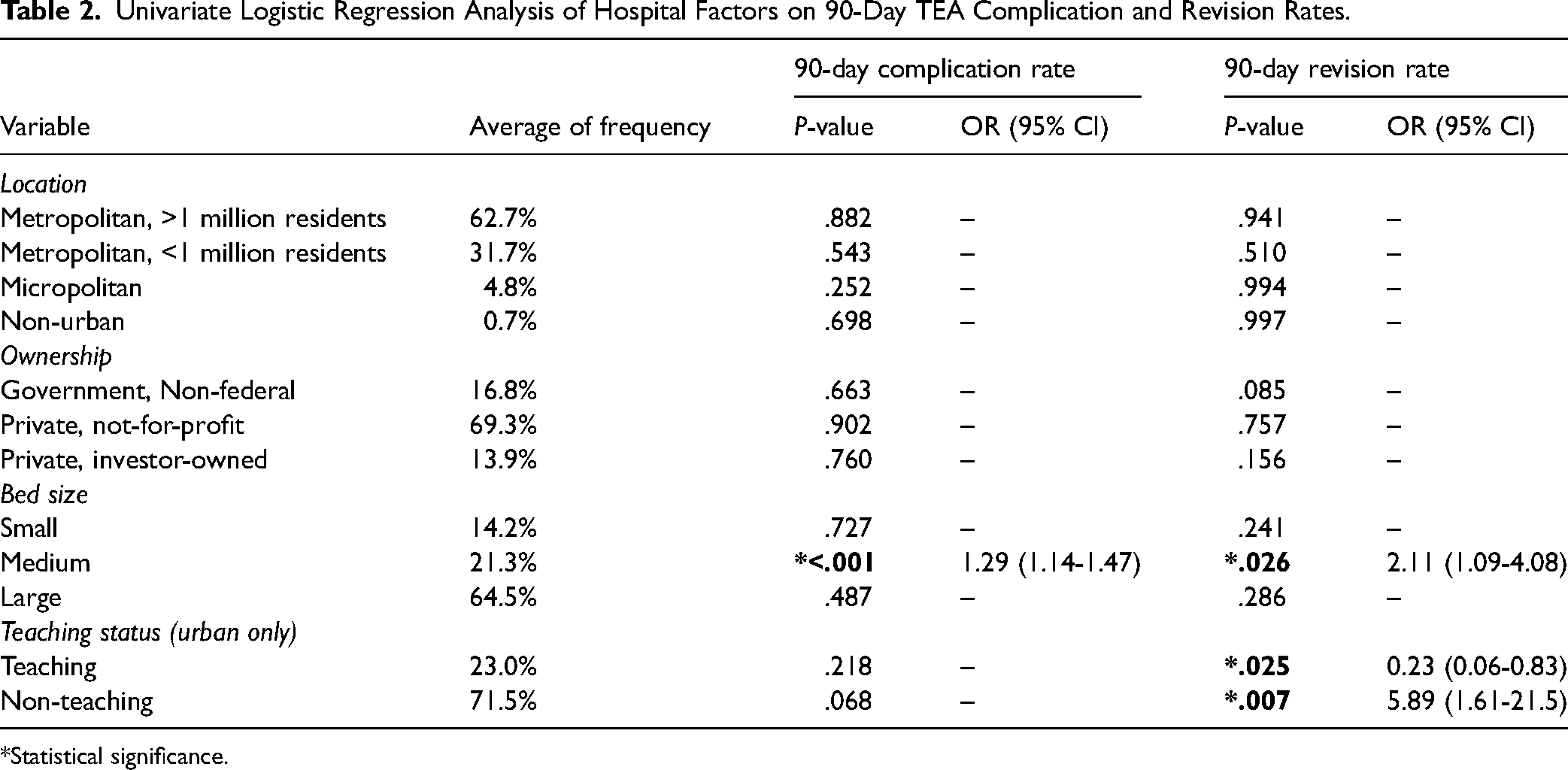
*Statistical significance.
Univariate Logistic Regression Analysis of Common Pre-operative Medical Comorbidities on 90-Day TEA Complication and Revision Rates.
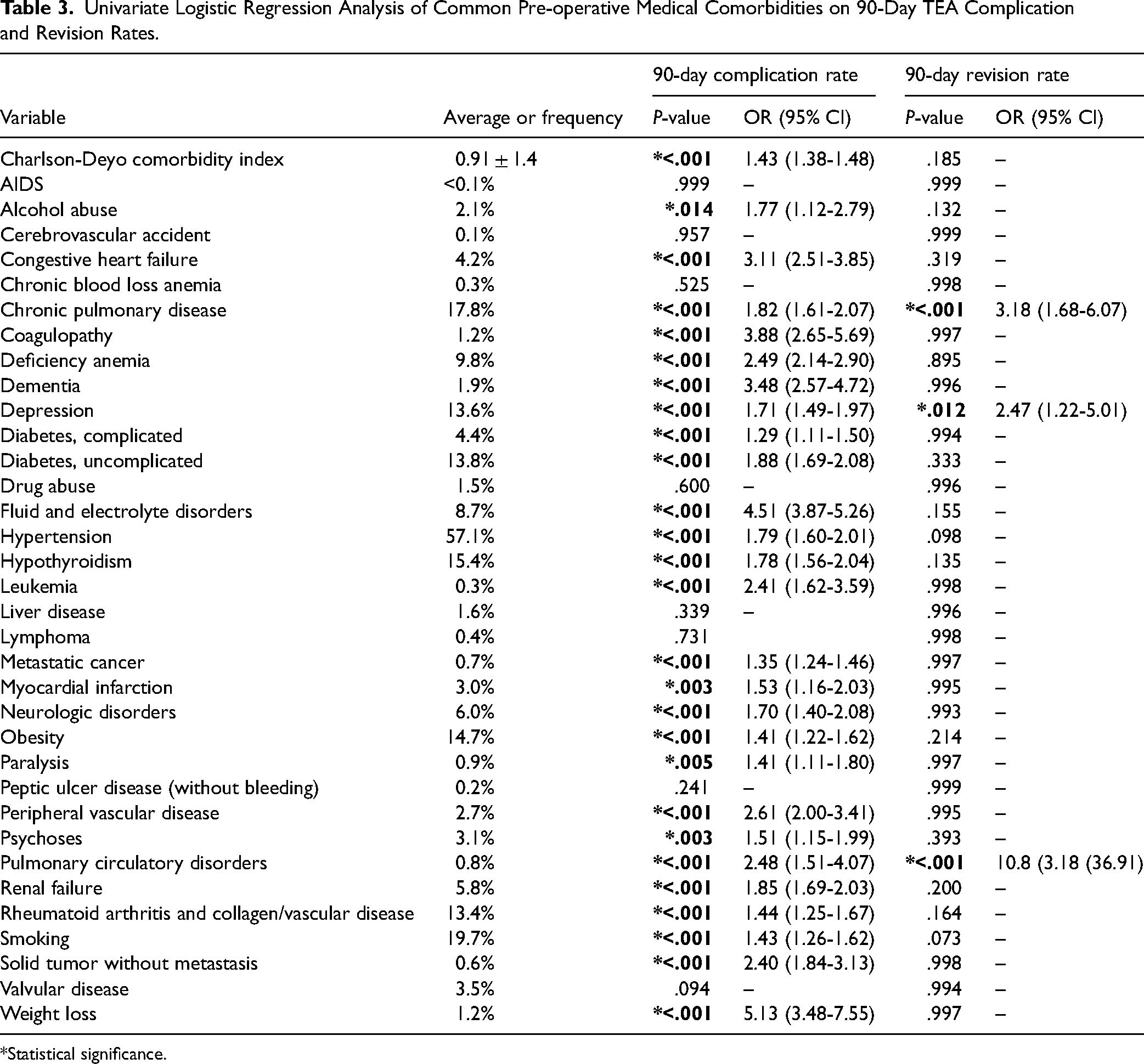
*Statistical significance.
Outcomes included in this study were 90-day complication and revision rates. Complication rates were calculated using ICD-9 and ICD-10 codes for post-operative complications identified in previous similar orthopedic studies using HCUP data.28,31 Complications included in the 90-day post-operative period included both mechanical complications (including hardware failure, dislocation, loosening, periprosthetic osteolysis, and periprosthetic fracture) and medical complications (including bleeding, cardiac-related, central nervous system-related, gastro-intestinal-related, acute renal failure, urinary tract infection, post-operative infection, peripheral vascular-related, shock, respiratory-related, wound-related, cellulitis, pulmonary embolism, pneumonia, acute respiratory distress syndrome, sepsis, thrombosis, transfusion necessary, and debridement necessary). All patients who received an additional procedure within the 90-day window were excluded to ensure that the complication was related to the TEA. Revision rates were identified using ICD-9 and ICD-10 codes for revision TEA as previously outlined. Indications for revision cases included in the study include periprosthetic fracture (42%), prosthesis infection (33%), and other hardware complications (25%).
Since all data used were de-identified and publicly available, no IRB approval was necessary based on institutional guidelines. All data analysis and statistics for the study were performed using SPSS version 27 (IBM, Armonk, NY, USA). Univariate, binary logistic regression models were initially run on all variables independently to identify which variables were individually predictive of increased or decreased complication or revision rates following TSA. Next, all significant variables were run simultaneously in a multi-variate binary logistic regression analysis model to determine which variables were independently associated with increased complication or revision rates. One model was run for complication rates and a separate model was run for revision rates.
Results
A weighted total of 8932 patients who underwent TEA were included in this study. Most cases were elective (61.7%), with the remaining cases being non-elective. Among these patients, the overall 90-day complication rate was 24.2% and the overall 90-day revision rate was 1.1%.
The results of the patient demographics analysis are shown in Table 1. Most patients analyzed in this study were females (72.2%), came from a diverse range of zip codes in terms of income quartiles, and had Medicare as their primary payer (54.5%). Patient factors that were significantly predictive of higher 90-day complication rates included increased age (P < .001), female sex (P < .001), and having Medicare as the primary payer (P < .001). Conversely, patients having private insurance as the primary payer was significantly predictive of lower 90-day complication rates (P < .001). With the univariate logistic regression analysis, no patient factors were significantly associated with worse 90-day revision rates, however Medicare as the primary payer approached significance (P = .055).
The results of the hospital characteristics analysis are shown in Table 2. Most TEAs in this study took place in populated metropolitan areas (62.7%), in large bed size (64.5%), private not-for-profit (69.3%), non-teaching hospitals (71.5%). Regarding both location and ownership of the hospitals, no factors were significantly predictive of worse complication rates or revision rates from the univariate logistic regression analysis. Medium bed size was significantly predictive of both increased complication rates (P < .001) and increased revision rates (P = .026). Regarding teaching status, teaching hospitals were significantly predictive of lower 90-day revision rates (P = .025) while non-teaching hospitals were significantly predictive of higher 90-day revision rates (P = .007).
The results of the pre-operative medical comorbidity analysis are shown in Table 3. An overall higher comorbidity burden, indicated by a higher average Charlson-Deyo comorbidity index, was predictive of increased complication rates (P < .001) but not revision rates. Of the 34 chosen medical pre-operative comorbidities, 26 were significantly predictive of higher 90-day complication rates in patients undergoing TEA. The 5 comorbidities with the highest odds ratios that were significantly predictive of higher 90-day complication rates were weight loss (P < .001, OR = 5.13), fluid and electrolyte disorders (P < .001, OR = 4.51), dementia (P < .001, OR = 3.48), coagulopathy (P < .001, OR = 3.88), and congestive heart failure (P < .001, OR 3.11). Chronic pulmonary disease (P < .001), depression (P = .012), and pulmonary circulatory disorders (P < .001) were the only comorbidities that were significantly predictive of higher 90-day revision rate in patients undergoing TEA. Additionally, smoking was predictive of higher complication rates (P < .001) but not revision rates (P = .078).
Shown in Table 4 is the result of the multivariate logistic regression analysis of the independent predictability of variables on 90-day complication rates following TEA. The following patient factor variables were significantly independently predictive of higher complication rates: age, Medicare, and Medicaid as the primary payer (all P < .001). The only hospital factor variable that was independently predictive of increased complication rates was if the procedure was performed at a medium bed size hospital (P < .001). Of the 26 preoperative comorbidities that were found to be significantly predictive of higher complication rates, 18 were found to be independently predictive of higher complication rates. The independently predictive comorbidities with the highest odds ratio of increased complication rates were fluid and electrolyte disorders (P < .001, OR = 3.22), leukemia (P < .001, OR = 2.89), coagulopathy (P < .001, OR = 2.74), weight loss (P < .001, OR = 2.17), and solid tumor without metastasis (P < .001, OR = 2.10). The only variable that was independently predictive of lower complication rates was private insurance as the primary payer (P < .004).
Multivariate Logistic Regression Analysis of All Variables Independently Predictive of Increased Complication Rates Following TEA.

*Statistical significance.
Table 5 shows the multivariate logistic regression analysis of variables independently predictive of increased revision rates following TEA. No patient factor variables were significantly independently predictive of increased or decreased 90-day revision rates. Hospital factors that were independently predictive of increased revision rates include medium bed size (P = .013) and non-teaching status (P = .011). Comorbidities that were independently predictive of increased revision rates included COPD (P = .001), depression (P = .025), and pulmonary circulatory disorders (P < .001).
Multivariate Logistic Regression Analysis of All Variables Independently Predictive of Increased Revision Rates Following TEA.

*Statistical significance.
Discussion
The results of this study identified several patient and hospital characteristics that are predictive of increased complication and revision rates following TEA. This is the first study to our knowledge to perform a comprehensive investigation of patient and hospital factors that affect complication and revision rates combining both a large database and a 3-month follow-up period.
In this study, increasing age was shown to be independently predictive of increased complication rates, indicative of the increased comorbidity burden in older patients. Payment with either Medicare or Medicaid were also independently predictive of higher complication rates, while private insurance was the only variable found to be independently predictive of lower complication rates. This may be due to the fact that private insurance could be indicative of both younger age and higher socio-economic status, as insurance status has repeatedly been shown to have a strong effect on TSA outcomes in a similar pattern to the current study.16,17,20
This study also sought to investigate the effect of hospital characteristics other than volume on TEA outcomes. 23 Surgery at medium bed size centers was independently predictive of higher complication and revision rates. This interesting pattern was also seen in a previous study by Poff et al that investigated the volume-outcome relationship of TEA. Low-volume centers performed 1-15 arthroplasties a year, medium-volume centers performed 16-47 a year, and high-volume centers performed 48 or more a year. They found that while the highest volume centers generally had the best outcomes, it was medium volume centers that consistently had the worst outcomes, specifically in both complication and revision rates. 23 They hypothesized that while high volume centers have the advantage of extensive surgeon experience and interdisciplinary networks to maximize outcomes, low volume centers may generally elect to perform TEA on less medically complex patients which leads to overall low complication and revision rates. 23 Both the results seen by Poff et al and the results of the presents study suggest that medium-sized hospitals may be in a particularly disadvantageous position when it comes to short-term TEA outcomes; medium-sized institutions have higher volume demands than low-volume centers and therefore must perform operations on more medically complex patients, but at the same time do not have the surgeon experience or interdisciplinary networks to accommodate these patients as well as high-volume centers can, resulting in worse overall outcomes.
The majority of medical comorbidities included in this study (18 out of 34) were found to be independently predictive of increased complication rates, including alcohol abuse, congestive heart failure, chronic pulmonary disease, coagulopathy, deficiency anemia, dementia, depression, diabetes (complicated), fluid and electrolyte disorders, hypothyroidism, leukemia, metastatic cancer, peripheral vascular disorders, renal failure, rheumatoid arthritis and collagen/vascular disorders, smoking, solid tumor without metastasis, and weight loss. Additionally, an overall higher comorbidity burden as indicated by the Charlson-Deyo comorbidity index was also independently predictive of increased complication rates. There were only 3 comorbidities that were predictive of increased revision rates: chronic pulmonary disease, depression, and pulmonary vascular disorders. This is overall consistent with the results of previous studies investigating both TEA and TSA. Previous studies investigating TEA have to date identified 7 comorbidities associated with inferior outcomes following TEA: young age, obesity, diabetes, smoking, hypothyroidism, rheumatoid arthritis, and overall high comorbidity burden.7–14 These studies consistently show that sicker patients are pre-disposed to developing post-operative complications following TEA due to factors such as compromised immune systems, impaired blood flow, and altered bone metabolism.7–14 The current study both confirms these findings and identifies an additional 18 medical comorbidities that lead to inferior outcomes following TEA. These various comorbidities can lead to states of impaired immune systems, blood flow, bone metabolism, physical mobility, and overall poor health that predispose individuals to complications and revisions following TEA.7–14 While a discussion on the exact physiological mechanisms by which each comorbidity leads to increased complication and revision rates would not be practical for the purposes of this study, the comorbidities identified and the odds ratios associated with each will provide valuable data points for orthopedic surgeons for the purposes of informed shared decision-making and pre-operative counseling. While this study did have a higher overall complication rate (24.2%) than previous studies investigating TEA, this study included both major and minor medical comorbidities in the post-operative period, while previous similar studies such as by Zhou et al included fewer complications, and additionally only included complications in the immediate peri-operative period. 4
There are several potential limitations to this study which stem from the use of a large national database. The database relies on accurate clinical coding, which has been shown to be prone to error. 32 Another limitation is that this study does not capture any complications or revision procedures that occur after 90 post-operative days. While this is a limited timeframe, it does provide post-discharge follow-up time compared to other large publicly available databases like the National Surgical Quality Improvement Project (NSQIP) database and the Nationwide Inpatient Sample (NIS) database. Additionally, as with many large databases there is limited information on functional outcomes, implant type, operative time, and surgical technique. Finally, the database does not capture complications or revision procedure that occurred in a different state, at a non-participating hospital, or during a different calendar year than the original procedure.
Despite these limitations, this study is the first of its kind to use a large database to identify independent predictors of increased complication and revision rates at 3 months follow-up and provides valuable information to physicians and patients regarding preoperative patient risk stratification in preparation for TEA. Future studies should look to investigate similar study populations with a longer follow-up period, with emphasis on functional outcomes and procedure-specific readmission rates, which were not available in the current database.
Conclusion
This study identified several demographic factors, hospital characteristics, and patient medical comorbidities that are independently associated with increased complication and revision rates following TEA. Surgeons should use this information for the purposes of pre-operative risk stratification so that opportunities for optimization can be identified in high-risk patients undergoing TEA. This information will help facilitate shared decision-making and provide more accurate patient-specific counseling regarding the projected outcomes of TEA in different patient populations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.