
Abstract
Aims
Patient-specific instrumentation (PSI) in primary shoulder arthroplasty has been studied; results supported the positive impact of the PSI on the glenoid positioning. Nevertheless, no clinical outcomes have been reported. We compare the clinical outcomes of primary reverse total shoulder arthroplasty using PSI versus the standard methods.
Methods
Fifty-three patients with full records and a minimum of 24-months follow-up were reviewed, 35 patients received primary standard RSTA, and 18 patients received primary PSI RSTA. All patients were operated on in a single center. The median follow-up was 46 months (53 months in the standard group vs 39 months in the PSI group).
Results
There was an overall significant post-operative improvement in the whole cohort (P< 0.05). The standard group had more deformed glenoids (B2, B3, C&D) and significantly low preoperative constant score and forward flexion (P=0.02 & 0.034). Compared to the PSI group (all were A1, A2, B1 &one type D), there were no statistically significant differences in any clinical outcome postoperatively. PSI neither prolonged the waiting time to surgery (P=0.693) nor the intraoperative time (P=0.962). Radiologically, PSI secured a higher percentage of optimum baseplate position and screw anchorage; however, no statistical correlation was found.
Conclusion
In this series, both groups achieved comparable good outcomes. PSI did not achieve significantly better clinical outcomes than Standard after primary RSTA. Yet comparison has some limitations. PSI did not negatively impact the waiting time or the surgical time.
Keywords
Introduction
In 1985, Paul Grammont designed a reverse total shoulder arthroplasty (RTSA) based on two biomechanical concepts: medialization and distalization of the center of rotation (COR), 1 and RTSA became established as a treatment for rotator cuff arthropathy (RCA). 2 RTSA replaces the constraint effect of rotator cuff tendons and compensates for its motor function as an abductor. Before Grammont's innovation, several implant designs were abandoned for failing to achieve these biomechanical advantages. 2 Further designs from different manufacturers have emerged, and the indications for RTSA have expanded beyond RCA to include irreparable massive cuff tear without osteoarthritis, rheumatoid arthritis with a cuff tear, acute proximal humerus fractures, fracture sequelae and revision procedures. 3
Patient-specific instrumentation (PSI) evolved to eliminate or minimize the risks of a malpositioned glenoid component, facilitating a more precise glenoid component positioning. Several cadaveric and clinical studies have examined the impact of PSI, particularly from the radiological point of view.4–23 The evidence is accumulating that PSI improves the glenoid component position, decreases the deviation from the preoperative plan, achieve a better version and tilt; however, its impact on clinical outcomes remains unclear.
This study analyzes and compares the clinical outcomes of two groups of primary RSTA procedures. A standard method of central guide application was used in one group, and in the second group, PSI was used. The hypothesis was that the PSI would improve clinical outcomes as it would improve the radiological parameters of the glenoid component position.
Patients and Methods
Design
A retrospective case-control study was conducted on a series of patients who received a primary RTSA in a single center between October 2010 and October 2016. During this period, One hundred thirty-seven patients (147 shoulders) who had been planned to receive a specific type of RSTA, either primary or revision, were available for review. After exclusions, there were 53 patients (shoulders) with a minimum follow-up of 24 months and complete records were analyzed; 35 patients (66%) received a primary standard RSTA, and 18 patients (34%) received PSI (Figure 1).

Flowchart shows the total number of operated patients and the final number of the included patients.
There were 17 men (32%) and 36 women (68%). They all had a full record of preoperative data and were available for yearly review at the arthroplasty follow-up clinic. All patients received the same prosthesis; Comprehensive® Reverse Shoulder System (Zimmer Biomet, Warsaw, IN, USA).
Standard RSTA was the only method used between 2010 and 2013, where 32 patients were operated. PSI (Signature guide) was introduced in 2013; it was offered for every patient afterward; 18 patients were operated on using PSI between 2013 to 2016. Only three patients received standard RSTA after 2013 (one acute trauma, one trauma sequelae, and one Rheumatoid arthritis with RC tear). The overall median age at surgery was 68 years (range, 47 to 89 years), and the median follow-up was 46 months (range 24 to 86 months). The underlying pathological background varied in this patient series (Table 1).
Pathological Background of the Study Population.

Preoperative Assessment
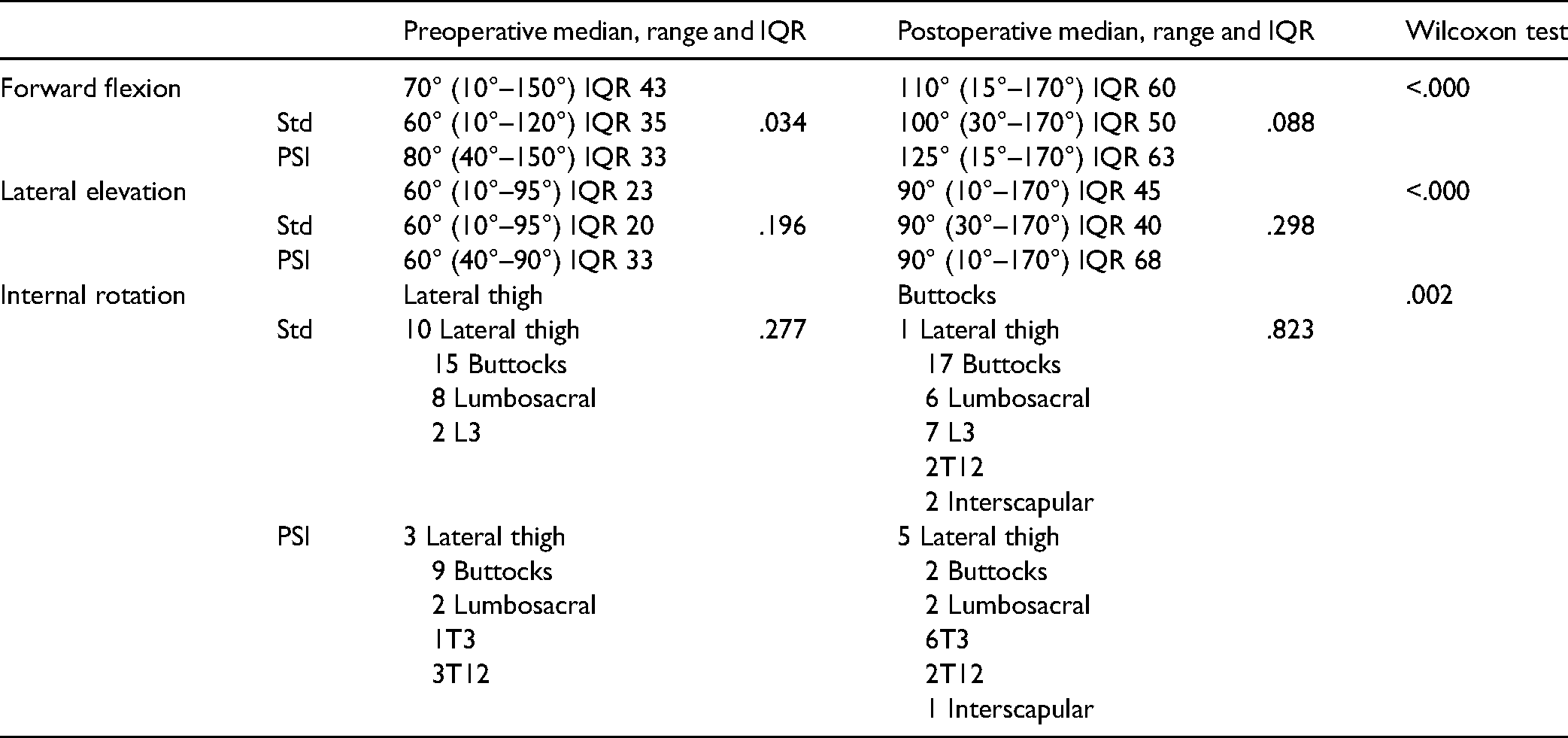
The study was registered with the departmental research committee and was designated as a service evaluation (ref no 21-9672). As such formal research ethics approval was not required. Preoperative pain and shoulder functional limitation were obtained objectively using numeric rating scales.. Patients rated their pain using pain analog scale. Patients rated how much their shoulder function was limited by pain or stiffness between 0 (no limitation) and 10 (severe limitation). The constant score (CS) and the Oxford shoulder score (OSS) were recorded. The patients’ physical and mental health was scored using the validated SF-12v1 health survey. Active shoulder range of motion measurement was collected: forward flexion and lateral elevation in degrees, internal rotation by highest anatomic landmark.
Plain radiographs, anteroposterior and axial, were obtained and used to assess the glenoid bone stock. Modified Walch Classification was used. 24 Preoperative 2D shoulder CT was requested for the candidates for PSI only; it was obtained according to a protocol (Signature, Biomet, Warsaw, IN, USA). The manufacturer makes a 3D scapula model to simulate the best glenoid component position, and together with the surgeon's input, they refine it for the best option for every individual case. The pin trajectory is adjusted to 10 degrees of inferior tilt and neutral version.8,25
The waiting time for surgery was calculated from the date of the first clinic visit till the date of the surgery. Not every patient was planned to have the surgery from the first visit, some investigations were done, or physiotherapy/injection was tried as non-operative management. Some patients opted to delay the surgery for various reasons. Thus, this waiting time does not reflect a lag in the process, but it has included many variables.
Operative Technique
All patients were operated on the beach chair position. The deltopectoral approach was utilized in all cases. When intact, the subscapularis tendon was tenotomized near its insertion. The humeral cut was done using an intramedullary resection guide in retroversion (20 degrees). The glenoid was prepared by removing the remaining labral remnants and soft tissues around the edges of the glenoid, specifically the anterior glenoid border where the Signature Guide is placed. The central guidewire was applied either by the customary freehand orientation of the standard jig or utilizing PSI (Zimmer Biomet Signature Glenoid Shoulder System) (Figure 2). Baseplates, 25 mm or 28 mm, were used according to glenoid size. Baseplates were placed flush on the glenoid surface, in the neutral version, as inferior as possible with inferior tilt 10 degrees, fixed by a central compression screw and 3 or 4 peripheral locking screws. The 36 mm glenosphere was used in all cases. Lateralized offset was used to adjust the deltoid tension in few cases.

The 3D print of the glenoid and the guide. The guide is made with a neutral tilt for anatomic TSA, and with 10 degrees inferior tilt for the RTSA.
Glenosphere was adjusted at the inferior offset choice (D) in all patients. The mini stem (83 mm) was used whenever suitable, in the cementless fashion in 46 shoulders (87%). Subscapularis tendons were repaired whenever possible, otherwise left unrepaired. Soft tissue biceps tenodesis was done when applicable.
Postoperative Follow-up
Immobilization in a sling was maintained for 2 to 3 weeks, and a particular protocol of physiotherapy was followed (ULTRA protocol). 26 Patients were invited for regular follow-up visits (clinical and radiological) at defined postoperative periods of two weeks, six weeks, three months, six months, and yearly. Clinical assessment was completed using the same preoperative proforma.
The radiographic assessment included anteroposterior and axillary views; adverse reactions were documented. Postoperative CT could not be requested as a routine for every patient. Notching was assessed and classified according to Nerot-Sirveaux classification. 27 All radiographs were reviewed and assessed by a fellowship-trained surgeon. Data from the operative summary, ward records, and clinic letters were also examined for further insights into complications or adverse events.
Statistical Analysis
Data were recorded into Excel (Microsoft, Redmond, WA, USA) and analyzed using the Statistical Program for Social Science the IBM SPSS ver. 24.0 (IBM Co., Armonk, NY, USA). Quantitative data were expressed as a median, range (Min-Max), and interquartile range. Qualitative data were expressed as frequency and percentage. Correlations were investigated using Fisher's Exact Test. Wilcoxon's test was used to detect differences between paired data sets. Mann-Whitney test was used to identify differences in preoperative, postoperative findings between two groups. Kruskall-Wallis test was used to investigate differences between multiple groups. The level of significance was set at P = .05.
Results
Clinical Outcomes
The postoperative outcomes for the whole patient cohort showed highly significant improvement (P < .001) in comparison to the preoperative values, except for the SF-12 mental component (MC), which was not changed significantly (P = .833). There were no statistically significant differences in any postoperative outcome between the standard and PSI groups (P > .05).
Regarding the pain, although all patients have improved, the amount of change was remarkably small in the PSI group, in whom the median pain decreased from 7 to 5, while in the standard group, the median pain decreased from 8 to 1. However, both shared nearly the same range and interquartile ranges, with no statistical difference between them either preoperatively (P = .459) or postoperatively (P = .091). This discrepancy might be related to the PSI group's short follow-up period or the glenoid wear pattern.
Age, gender, and dominant side involvement were not statistically different between the two groups. The waiting time for surgery was slightly longer in the PSI group but was not statistically significant (P = .693). The operative time was nearly identical in both groups (P = .647). Follow up period was significantly shorter in the PSI group (P = .004), which was expected, as PSI was introduced recently in our center (Table 2).
Age, Gender Dominant side Involvement, Waiting Time, Surgical Time and Follow-up within the Study Cohorts.

The glenoid wear and deformity were evident in the standard group (Table 3), which has more deformed glenoid (B2, B3, C, and D) than the PSI group (all are A1, A2, B1, and one patient type D). The preoperative CS and the preoperative forward flexion in the standard group were poor compared to the PSI group (P = .02 and .034). Other preoperative scores showed no significant difference between the two groups. However, postoperatively, there were no statistically significant differences in the scores between the two groups (Tables 4 and 5). The median postoperative satisfaction of the whole cohort was 10 (range 0-10), IQR 2. The median satisfaction in the standard group was 10 (range, 0-10), IQR 1, and in the PSI group 9.5 (range, 4-10), IQR 3. There was no statistical difference between the groups (P = .192)
Modified Walch Classification of the Glenoid in Both Groups.

Preoperative and Postoperative Clinical Scores of the Study Cohorts.

Mann Whitney test (two independent groups).
Wilcoxon signed-rank test (two related groups).
Preoperative and Postoperative Range of Motion in the Study Cohorts.
Radiological Outcomes
Radiologically, there was no statistical difference between the two groups regarding notching, baseplate position, screws, loosening, or heterotrophic ossification.
Baseplate position
Examination of the plain x-ray anteroposterior and axial shoulder views, the position of the baseplate was optimum (inferior position, inferior offset, neutral version, and 10 degrees inferior tilt) in 37 shoulders (69.8%). There was a higher probability of achieving the proper baseplate position in the PSI group (72.2%) than in the standard group (63.2%). The screw position and the purchase was found properly (engaged the far cortex, penetrating the far cortex less than 10 mm) in 45 shoulders (84.9%), also there was a higher percentage of achieving the best purchase in the PSI group (94.4%), than in standard group (80%), though no statistical correlation was found in either situation.
Loosening
On the humeral side, there was no loosening of the humeral component. On the glenoid side, only one shoulder (1.9%) in the standard group had loosening around the baseplate screw after a fall; this was revised later. No other glenoid baseplate loosening was identified.
Notching
The overall incidence of notching was 5.66
Follow-up
Complications
Three patients of 53 patients (5.7%) had major complications that required further surgery during the treatment course. One patient developed a postoperative extensive hematoma collection in the second week. It needed a surgical evacuation and (polyethylene) PE insert change and continued follow-up.
One patient had a long baseplate superior screw after a standard RSTA. The screw caused a pain that did not settle until it was revised and changed to a shorter one. One patient had the glenosphere dissembled from the baseplate during a simple abduction movement, six months after a standard RTSA. This was revised, and the patient was then stable and continued with usual follow-up.
All these patients, at the final follow-up, showed comparable outcomes to the rest of the series; there was no statistically significant difference in any postoperative parameter (P > .05).
Discussion
The main aim of PSI is to decrease excessive component malposition, a known factor for arthroplasty failure. This retrospective investigation specifically looks at the clinical outcomes of RSTA, comparing the standard base plate application method with the use of PSI. The data demonstrated that PSI neither prolonged waiting time before surgery nor procedure time. Both patient groups benefited from the surgery with no statistical difference in any postoperative clinical or radiological outcome.
Patient-specific instrumentation in shoulder arthroplasty has been investigated for more than ten years, using cadavers, models, or in-vitro simulation.5,9,10,18,25,28–31 Others were smaller clinical studies.4,12–14,16,19–21,23 Of these, three studies compared the standard method to the PSI.4,16,21 A systematic review by Villatte et al. found that deviation from the preoperative plan was significantly lower in the PSI group, specifically for inclination, version, and entry point measures in which PSI was found to have fewer outliers than standard methods. 11
Cabarcas et al. undertook a metanalysis on PSI, including anatomic and reverse arthroplasties, cadaveric and clinical. Glenoid component inclination and version were the most constant outcome measures in 90% of the reviewed studies; the mean postoperative error in inclination or version was 5 degrees or less than the preoperative plan. However, the pooled analysis failed to find direct statistical significance for this improved accuracy. 8 They further highlighted the lack of records on manufacturing time, surgical time, and the impact of PSI on the clinical outcomes.
Heylen et al. was the only study that included RSTA (12 TSA and 24 RSTA), whereby half of each group were PSI. They found no significant improvement in component positioning but identified less likelihood for deviation in the highly deformed glenoid. 16
Data is available from several non-comparative studies that examined the PSI in RSTA, measuring the deviation in version, tilt, or rotation from the planned position. Five studies had very small numbers of patients (four patients in two studies,13,23 seven patients in one study, 19 and ten patients in two studies20,22), and Only one study had a bigger number of patients (32). 12 Based on their results, these studies favored the benefit of using PSI.12,19,20,22,23 Lau and Keith, in a small series of 11 patients (seven TSA and 4 RSTA), was the only study to find no benefit from PSI. 13
In this study, no clinical or technical, or radiological (x-rays) supremacy of PSI was concluded. One possible confounding factor was that the lead surgeon who operated 51 of the 53 shoulders was also a high-volume surgeon, who had operated many primary and revision shoulder arthroplasty cases per year over many years (146 primary and revision surgeries during the study period). Thus, the familiarity and long experience in using the standard methods achieved the technical accuracy of the PSI. However, PSI might be helpful to early-career shoulder surgeons. PSI is also endorsed specifically because it eases the application of the guide in severely deformed glenoid. Glenoid morphology was not assessed in this study; thus, it was not feasible to confirm that all cases were alike, a further limitation of this analysis. This same limitation is present in half of the published data, restricting the analysis of the clinical value and impact of PSI. 8
The waiting time for surgery was slightly longer in the PSI group, but overall, the difference was not statistically significant. Unfortunately, this has been under-explored in the literature. In the most recent systematic review, only a manufacturing time for the guide was reported by two of the studies as two weeks and five weeks as a minimum. 8 Adding the time of the scans to be done and uploaded, also, the shipping time to overseas centers could further increase delays. Moreover, some of the study patients had a long waiting time because of other clinical or personal factors.
Another possible drawback of PSI is surgical time. The intraoperative navigation system was evolved to increase the accuracy of component placement. However, it has been tagged with increased surgical time. Kircher et al. reported an increased accuracy with navigation, but at the expense of time. They identified a significantly longer operation in the navigation group 169 min compared to138 in the standard group. 32
On the contrary, Wang et al. reported no difference between navigation and standard, with 77 min in the navigated RTSA group and 78 min in the non-navigated group. They highlighted the learning curve, the need to be familiar with the system. 7 We were unable to explain the big difference in procedure duration between the two studies. Unfortunately, there was no clear definition of surgical time in either report.
PSI has been endorsed as an alternative to navigation, spared from the lengthy operation and the reported intraoperative hardware malfunction; operative time has been under-addressed in similar studies, 8 which raises the further question of cost-effectiveness and clinical impact. We present such data for the first time to our knowledge, demonstrating that surgical time was not statistically affected by PSI application compared with standard protocols.
Despite the growing body of evidence favoring PSI, based on meticulous measurements of inclination, version, and angulation, no clinical outcomes were reported in these studies. It was imperative to review and compare the clinical outcomes of PSI, specifically whether this technical success would be reflected in the patients’ range of motion, the longevity of the prosthesis, loosening, or notching. According to our results, there was no clinical advantage in the PSI group over the standard group.
Notching in this series was low 5.66%; the design of this implant has recruited many strategies to decrease notching (inferior offset, 10° to 15° inferior tilt and neck-shaft angle of 147°); however, the follow-up period (53 months in the standard group vs. 39 months in the PSI group) would affect this observation. Evidence showed that notching evolves over time, and the longer the follow-up, the more chance of developing a notch. Simovitch et al. reported the average time to notch development at 51.4 months in their big series of 324 patients with a minimum five-year follow-up. 33 Mollon et al. analyzed 476 shoulders with a minimum two-year follow-up; they concluded that notching is more likely to develop with longer follow-up (46.1 vs. 37.0 months; P = .0001). 34
Limitations
There are some limitations in this study, the retrospective non-randomized nature of the study, diverse pathological backgrounds, lack of preoperative CT for all cases, neither postoperative CT. Additionally, variable glenoid wear pattern was evident between groups (based on x-ray analysis by a single assessor); the standard group has more deformed glenoid (B2, B3, C, and D) than the PSI group (all are A1, A2, B1, and one patient type D), lastly, the variable follow-up periods (shorter in the PSI group).
Conclusions
PSI was proved to increase the accuracy of the glenoid component positioning in the literature; its impact on the clinical outcomes is not yet proved. We present the results of two groups of patients who were operated on in one center, a group of standard RTSA and another group of PSI RTSA. There were no significant differences in any clinical or radiological outcomes. Additionally, PSI did not prolong the waiting time nor operative time. This design of RSTA had a very low incidence of notching.
Footnotes
None.
Author Contributions
AAE conceived the original idea, designed the analysis, collected the data, performed the analysis, writing—original draft preparation. MSG collected the data, edited and reviewed the paper. MAM collected the data, edited and reviewed the paper. MMR designed the analysis, writing—original draft preparation. AW collected the data, edited and reviewed the paper. QY designed the analysis, edited and reviewed the paper. SPF conceived and designed the analysis, supervise the project.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Prof Simon P. Frostick: received royalties and consultant payments from Biomet for work related to the subject of this article. All other authors: NONE.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical Approval
The study was registered with the departmental research committee and was designated as a service evaluation (ref no 21-9672). As such formal research ethics approval was deemed NOT to be required. Liverpool Orthopaedic and Trauma Service (LOTS) Research Group. Liverpool University Hospitals NHS Foundation Trust. Prescot St, Liverpool L7 8XP, United Kingdom, Tel:0151 706 3697, Email: lotsresearchgroup@luhft.nhs.uk
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.
All Authors Witness That
There is no prior or duplicate submission or publication elsewhere of any part of this work including details of any presentation of the study as an abstract at a professional meeting. This manuscript has been read and approved by all authors. Each author believes that this manuscript represents honest work. We hereby witness that the senior author