
Abstract
Objective
Recent reports have shown that outpatient shoulder arthroplasty (SA) may be a safe alternative to inpatient management in appropriately selected patients. The purpose was to review the literature reporting on outpatient SA.
Methods
A systematic review of publications on outpatient SA was performed. Included publications discussed patients who were discharged on the same calendar day or within 23 hours from surgery. Articles were categorized by discussions on complications, readmissions, and safety, patient selection, pain management strategies, cost effectiveness, and patient and surgeon satisfaction.
Results
Twenty-six articles were included. Patients undergoing outpatient SA were younger and with a lower BMI than those undergoing inpatient SA. Larger database studies reported more medical complications for patients undergoing inpatient compared to outpatient SA. Articles on pain management strategies discussed both single shot and continuous interscalene blocks with similar outcomes. Both patients and surgeons reported high levels of satisfaction following outpatient SA, and cost analysis studies demonstrated significant cost savings for outpatient SA.
Conclusion
In appropriately selected patients, outpatient SA can be a safe, cost-saving alternative to inpatient care and may lead to high satisfaction of both patients and physicians, though further studies are needed to clarify appropriate utilization of outpatient SA.
Introduction
Shoulder arthroplasty (SA) is a well-established and effective treatment for patients with glenohumeral joint arthritis. As the world’s population ages, both demand for and utilization of shoulder arthroplasty has increased. In 2008, there were approximately 47,000 shoulder arthroplasties performed in the United States. 1 As innovation in SA improves and the indications for treatment expand, there has been an exponential increase in the number of SA performed each year in the United States. Comparing the prevalence of SA between 2000 and 2010, Day et al estimated a 7% to 13% increase per year. 2 By 2017, one study from the National Inpatient Sample found 1,08,300 primary SAs performed. 3 A Poisson model estimated of 3,50,558 SAs by 2025, largely attributable to the rapid increase in reverse total shoulder arthroplasty (RTSA) over the steady increase in anatomic total shoulder arthroplasty (TSA) and decline in hemiarthroplasty (HA).3–5
With technological and surgical advancements, improvements in perioperative care, and increasing efforts to reduce health care costs, there has been a push towards outpatient SA. Recently in 2021, the Center for Medicare & Medicaid Services (CMS) removed Current Procedural Terminology codes reflecting SA from the inpatient-only list, including codes 23472 (Arthroplasty, glenohumeral joint; total shoulder (glenoid and proximal humeral replacement (for example, total shoulder)) and 23474 (Revision of total shoulder arthroplasty, including allograft when performed; humeral and glenoid component). 6 Furthermore, ambulatory surgical centers (ASC) offer treatment at a significant cost savings compared to traditional hospital-based care. 7 A recent systematic review reported a mean cost savings of 17.6% to 57.6% for ambulatory procedures compared with inpatient procedures. 8 Additionally, surgeons and patients have higher levels of satisfaction with procedures in an ambulatory setting. 8 Recently, there has been more emphasis on outpatient total hip arthroplasty (THA) and total knee arthroplasty (TKA), focusing on a variety of topics including safety, 9 , 10 patient satisfaction, 11 and cost. 12 One common theme in the literature examining the transition to outpatient surgery is that physicians must be well-informed and balance the push for outpatient management with its safety. 13 , 14
In 2018, Brolin et al surveyed 484 active American Shoulder and Elbow Surgeon (ASES) members to evaluate experience with and perceived barriers to outpatient SA. 15 For surgeons already performing outpatient SA, the five biggest barriers were patient comorbidities, patient social support, patient age, concern for medical complications and insurance contracts. For surgeons not performing outpatient SA, the five biggest barriers to performing outpatient arthroplasty were patient comorbidities, patient social support, patient age, concern for medical complication, and readmission risk. Both groups agreed on four of their top five concerns, highlighting the importance of a clear understanding of these issues for performing outpatient SA. The purpose of this systematic review is to evaluate the current evidence of the safety, patient selection, perioperative pain control, costs, and patient and physician satisfaction levels associated with outpatient SA.
Methods
Literature Search
A comprehensive systematic review of the literature was performed using PubMed (Medline) and Embase databases in October 2020 according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. The review included the following for search terms: “shoulder replacement” or “shoulder arthroplasty” and “ambulatory” or “outpatient.” Prior to data abstraction, the systematic review was registered in the international prospective register of systematic reviews (PROSPERO, registration number CRD42019119808). During full-text review, the reference lists were examined to ensure a full systematic review of the literature.
Study Selection
The inclusion criteria were determined prior to data collection. Articles were included if they had a study population that underwent SA that was discharged on the same day or after a 23-hour stay. Only articles in English were included. Three independent reviewers (SA, EC, DAL) evaluated all titles for eligibility. After title review, relevant abstracts were examined. After title and abstract assessment, the remaining studies underwent a full-text review. Review articles were excluded but the references were evaluated for inclusion.
Data Abstraction
Categories for data collection for each article included author names, study title, journal name, interventions, and outcome measures. Three reviewers (SA, EC, DAL) extracted outcome data on complications and safety, patient selection, pain management strategies, patient satisfaction, surgeon satisfaction, and cost effectiveness.
Results
The initial search generated a total of 226 potentially relevant articles. 51 full text articles were reviewed. Following full text review, 26 articles were included in the review (Figure 1).16–41 Of the included studies, 18 articles discussed complications, readmissions, and safety,16–19, 21 , 22 ,24–33, 40 , 41 7 articles discussed patient selection, 21 ,27–31, 40 6 articles discussed pain management, 20 , 28 ,34–37 6 articles discussed the cost implications of outpatient surgery, 15 , 22 , 23 , 30 , 38 , 41 2 articles discussed patient satisfaction, 24 , 32 and 1 article discussed surgeon satisfaction. 15 The level of evidence of the included articles ranges from Level II to Level V.
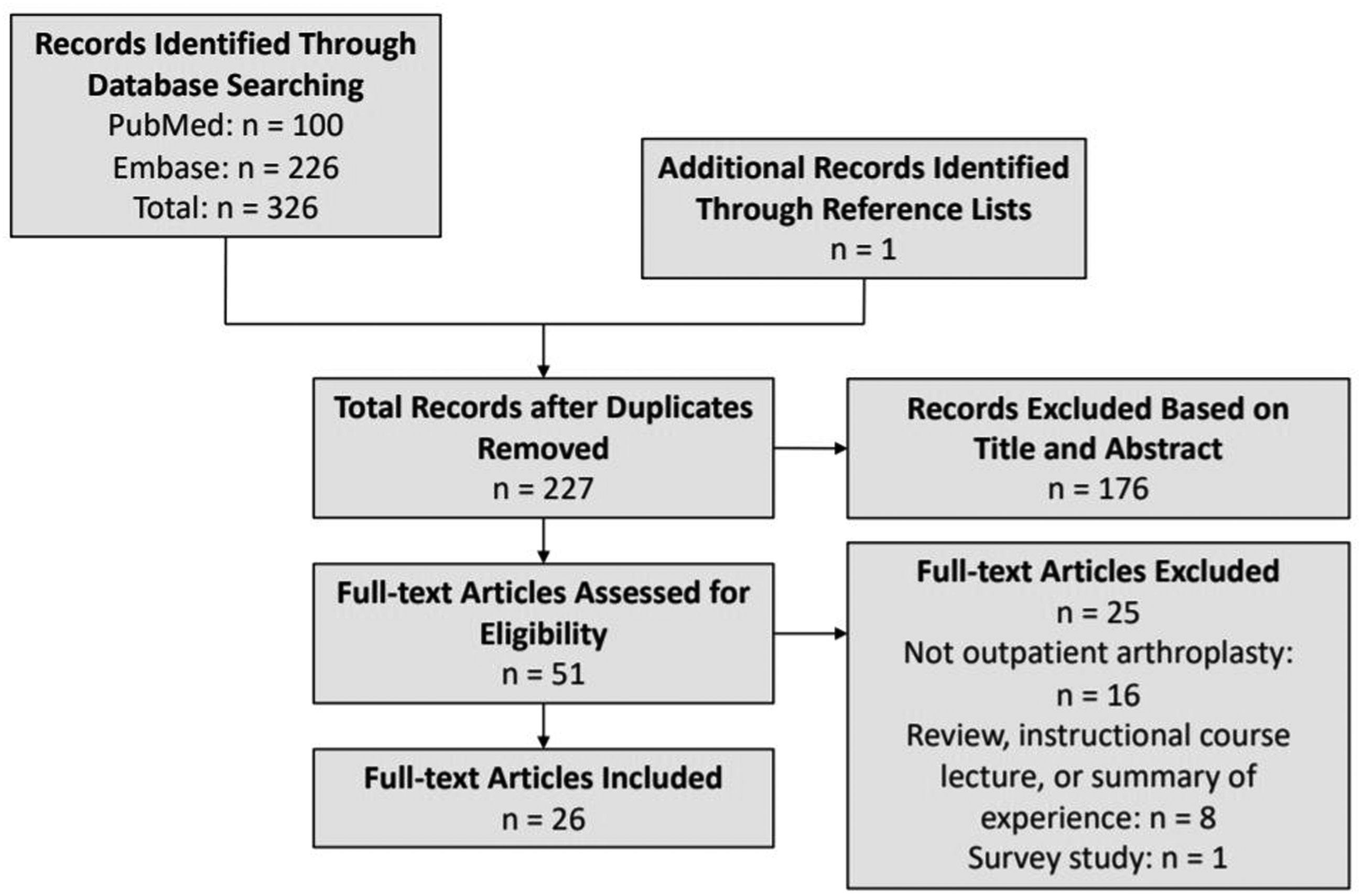
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart for study selection.
Complications, Readmissions, and Safety
The 18 studies examining complications and safety of outpatient SA fall into two categories: retrospective cohorts and series from single centers16–18, 22 , 24 , 28 , 29 , 32 , 33 , 40 and larger database or registry studies (Table 1). 19 , 21 ,25–27, 30 , 31 , 41 Seven studies found higher complications with inpatient SA, 18 , 21 , 27 , 28 , 30 , 31 , 33 one study found higher complications in outpatient SA, 25 four studies found no differences in complications or readmissions, 19 , 22 , 29 , 41 one study had mixed findings, 26 and five studies did not compare inpatient and outpatient SA. 16 , 17 , 24 , 32 , 40 Brolin et al found no statistical difference between inpatient (10%) and outpatient (13%) complication rates when comparing 30 inpatient and outpatient SA performed by a single surgeon, 29 and Arshi et al found higher rates of surgical site infections (SSI) requiring irrigation and debridement at 6 months (OR = 1.49; 95% confidence interval (CI), 1.01–2.19; P = .045) and 1 year (OR = 1.65; 95% CI, 1.15–2.35; P < .001) in an outpatient SA cohort. 26
Articles and Findings Relating to Complications, Readmissions, and Safety of Outpatient Shoulder Arthroplasty.

OR: odds ratio; 95% CI: 95% confidence interval; SA: shoulder arthroplasty; TSA: total shoulder arthroplasty; RTSA: reverse total shoulder arthroplasty; ASA: American Society of Anesthesiologists.
Medical complications were more common in inpatient cohorts relative to outpatient SA patients, with complications ranging from 0%–17.7% for inpatients and 0%–15.9% for outpatients. 16 , 18 , 21 , 22 , 24 , 25 , 28 , 30 , 31 Common complications identified in the inpatient vs outpatient cohorts were blood transfusion (range, 4.48–4.7% vs 0.49–3.5%), urinary tract infection (range 0.9–8.7% vs 0.58–6.8%) and acute kidney injury (range, 0.4–4.3% vs 0–4.5%). 27 , 30 , 31
Inpatient SA had a higher readmission rate compared to outpatient SA in several studies 21 , 27 , 30 , 33 (OR = 1.8, P = .016 for 30-day readmission and OR = 1.8, P < .001 for 90-day readmission). 27 Cancienne et al identified obesity, morbid obesity, diabetes mellitus, peripheral vascular disease, congestive heart failure, chronic lung disease, depression and chronic anemia as risk factors for readmission within 90 days after ambulatory SA. 30 The database study by Ode et al. similarly identified obesity as a significant risk factor for readmission (P < .0001). 41 Smaller single-center studies have identified no difference in 90-day morbidity or mortality rates between inpatient and outpatient SA. 22 , 24 , 33
In contrast, Kramer et al. found no differences between same-day discharge and in-hospital stay groups in terms of 90-day readmission (OR = 0.71, 95% CI: 0.42-1.20), 90-day ED visits (OR = 1.08, 95% CI: 0.80–1.47), and 1-year mortality (OR = 1.61, 95% CI: 0.63–4.15), ultimately concluding that same-day discharge was not inferior to in-hospital stay SA in terms of 90-day readmission. 19 Harris et al. found higher all-cause 30-day readmission rates in the outpatient cohort (3.4% vs. 1.7%, P < .01), but no difference in 30-day readmissions specific to surgical complications (1.9% vs. 1.4%, P = .32). 25
Some studies evaluated different outpatient settings. Charles et al. examined both ambulatory surgical centers and hospital-associated surgical centers and found no differences in complications between the two sites. 17 Ode et al. in noted a trend towards a higher, though not statistically significant, readmission rate for SA cases at an ambulatory center (8%) relative to hospital-based outpatient departments (6%) or inpatient settings (6%) (P = .0844). 41
Overall, more studies reported higher readmission and complication rates for patients having inpatient SA, with diabetes, obesity and cardiac and pulmonary comorbidities as risk factors for readmission.
Patient Selection
Seven studies discussed patient selection for outpatient SA. 21 ,27–31, 40 (Table 2). There were differing reports on the BMI of patients undergoing outpatient SA, with three studies reporting a lower BMI relative to a matched inpatient group, 21 , 29 , 31 one study reporting more obese patients in the outpatient SA group, 27 one study reporting no difference between BMI for inpatient and outpatient SA, 30 and one study evaluating only an outpatient cohort. 40 Patients undergoing outpatient SA had consistently fewer medical comorbidities such as pulmonary disease, hypertension, chronic kidney disease, diabetes, congestive heart failure and coronary artery disease. 21 , 27 ,29–31, 40 Patients undergoing outpatient SA were more likely to be younger, male, and with a lower ASA score relative to those treated with inpatient SA. 21 , 28 , 31 The machine learning predictive model developed by Biron et al. found that male sex (P < .001), white race (P < .001), and surgery performed in a recent year (P = .001) were all predictive of short length of stay. 21
Articles and Findings Relating to Patient Selection in Outpatient Shoulder Arthroplasty.
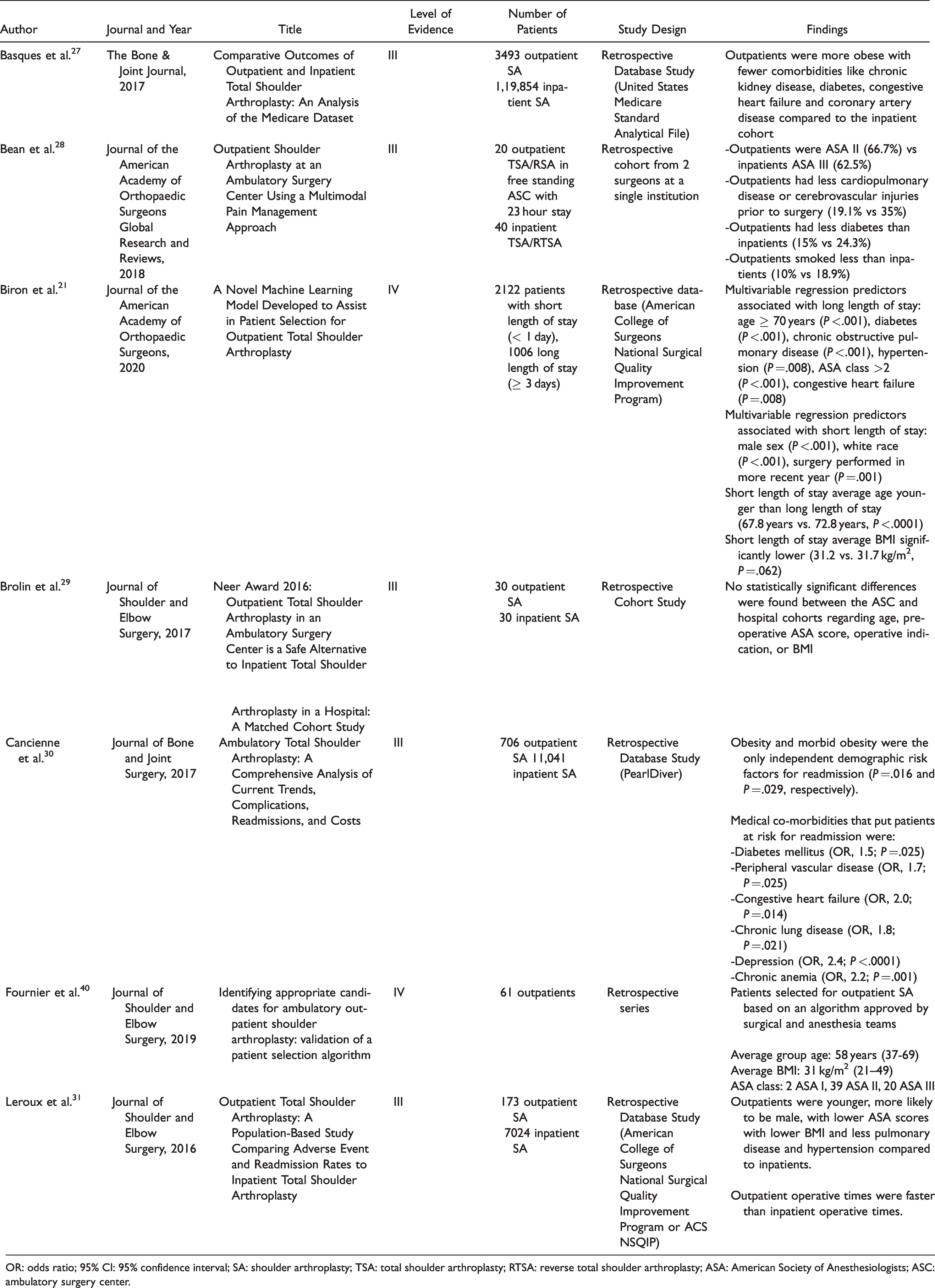
OR: odds ratio; 95% CI: 95% confidence interval; SA: shoulder arthroplasty; TSA: total shoulder arthroplasty; RTSA: reverse total shoulder arthroplasty; ASA: American Society of Anesthesiologists; ASC: ambulatory surgery center.
Pain Management Strategies
Six articles described strategies for perioperative pain management, including reports on indwelling pre-operative continuous nerve catheters, single shot (SS) interscalene nerve blockade (ISB) using ropivacaine or bupivacaine, and pericapsular local anesthetic injection at the time of surgery (Table 3). 20 , 28 ,34–37 Studies with indwelling continuous nerve catheters reported no re-admissions for anesthetic related complications,35–37 though one study 35 in the ambulatory group reported 3/8 emergency room visits, 2 of which (25% of the ambulatory group) were related to pain or the catheter. Shah et al evaluated patients with primarily continuous nerve catheters (73/82, 89%) and a small subset of SS interscalene nerve blockade (9/82, 11%). 37 Of the total 82 patients, the initial block was considered inadequate in 7.3% (repeat nerve block was required for 6.1% and 1.2% received additional local anesthetic by the surgeon) and 8.5% of patients required general anesthesia intraoperatively. 37 One study reported on outpatient SA with SS interscalene nerve blockade. 34 One patient (5.1%) presented for a repeat block on post-operative day #1, and no other patients required ED presentation or re-admission for pain control. Bean et al reported on outcomes with patients treated primarily with a periarticular local anesthetic injection. 28 Only 9.5% of patients in their cohort received a regional nerve block. Overall, 4.8% of outpatients presented to an ED or Urgent Care within 90 days of surgery, as compared to 5.0% of inpatients. 28 A database study by Chan et al. examining utilization of peripheral nerve blocks found that 19.1% of inpatient SAs and 20.8% of outpatient SAs utilized peripheral nerve blocks, with an increasing trend of use for inpatients in more recent years. 20 The benefits of the nerve block included lower oral morphine equivalents utilized on the day of surgery in each of inpatient and outpatient groups. 20
Articles and Findings Relating to Pain Management Strategies in Outpatient Shoulder Arthroplasty.

SA: shoulder arthroplasty; TSA: total shoulder arthroplasty; RTSA: reverse total shoulder arthroplasty; ASC: ambulatory surgery center.
Cost Implications
Six articles discussed the individual patient and overall societal cost implications of outpatient SA (Table 4). 22 , 23 , 30 , 38 , 39 , 41 All studies consistently reported that outpatient SA can significantly decrease costs associated with SA with average or median USD cost estimations for inpatient surgery ranging from $18,336 to $76,109 compared to $14,722 to $44,530 for outpatient surgery. 23 , 30 , 38 , 39 , 41 Centers performing a higher volume of SA were less expensive than lower volume centers. 38 Steinhaus et al estimated cost savings between $747 and $15,507 per patient. 39 The authors extrapolated these data to an overall cost savings in 2016 ranged from $4.1 M to $349 M, and 10-year cost savings from 2016 to 2025 varied from $51 M to $5.4B. Ode et al. found the median charge for inpatient cases ($62,905) to be significantly higher than for outpatient cases ($37,395, P < .001). 41 These authors also noted median hospital outpatient department costs ($55,990) were significantly higher than ambulatory surgery centers ($31,790, P < .0001). 41 When itemized in one study, ambulatory SA had significantly lower PACU costs (P < .0001), laboratory costs (P < .0001), physical and occupational therapy costs (P < .0001), and narcotic prescription costs (P < .0001), but significantly higher costs for anticoagulant prescription (P = .014) and antiemetic prescription costs (P = .001). 30 Another economic analysis by Walters et al. evaluated differences in bundled vs. unbundled payments for outpatient SA, noting that the bundled group had significantly lower charges for implants, total surgical day charges, and staff charges, and similar charges for surgery, anesthesia, and postoperative charges; ultimately, the total charges for the bundled group were significantly lower ($42,410.27 ± $10,051.50 vs. $44,529.80 ± $5367.24, P = .024). 23
Articles and Findings Relating to Cost Implications of Outpatient Shoulder Arthroplasty.

SA: shoulder arthroplasty; TSA: total shoulder arthroplasty; RTSA: reverse total shoulder arthroplasty.
Patient Satisfaction
Two studies specifically addressed patient satisfaction following outpatient SA. 24 , 32 35 of 41 patients (85.4%) completed a post-surgical telephone questionnaire in the study by Leroux et al. 32 94.3% of patients felt ready for outpatient discharge, and all but 2 patients (who needed an overnight stay in the ASC with 23-hour stay capabilities) stated they would have outpatient SA again. 97% of patients reported a good to excellent outpatient experience (poor, fair, average, good, excellent scale). The 2 patients that stated they needed an overnight stay were taking narcotics pre- and post-operatively for chronic non-shoulder related reasons. 16/21 patients in the series by Tansey et al. responded to a satisfaction survey at 12 months post-operatively, with 11 (69%) reporting they were “very satisfied” and 3 (19%) reporting they were “satisfied.” 24 81% of these patients reported they would undergo the surgery again as an outpatient. 24
Surgeon Satisfaction
One study examined surgeon satisfaction with outpatient SA. 15 An online survey was sent to 484 active ASES members, which was completed by 37% (179 participants) of members. Only 20.7% (37/179) surgeons performed outpatient SA. Of those surgeons performing outpatient SA, 78.4% (29/37) reported an excellent experience overall.
Discussion
The aims of this study were to summarize the literature on the safety and feasibility of outpatient SA. Though there is a lack of high-quality randomized control trials examining outpatient SA, our review summarizes the available evidence that suggests that outpatient SA can be a safe procedure with potentially lower overall associated costs and high patient satisfaction scores in carefully selected patient populations. In the near future, higher volume studies are expected given the increasing nature of outpatient SA. Outpatient SA rates have increased over time, and this trend is exemplified by the fact that 12/26 (46.2%) articles included in the review were published in 2019 or 2020.16–25, 40 , 41
With the push towards outpatient management of SA, it is important for institutions and individual physicians to independently determine if they are prepared to transition from the inpatient to outpatient setting using these evidence-based criteria for patient selection. All but two studies 25 , 26 examining complications and readmissions included in this review show either no difference or increased complication rates with inpatient SA compared to ambulatory SA, especially patients with diabetes or pulmonary or cardiac co-morbidities. 27 ,29–31, 33 Our review found overall higher complication rates for inpatient SA compared to outpatient SA when looking at larger database studies, but these results should be interpreted with caution. There is selection bias as these studies were performed retrospectively, and patients with more comorbidities were selected for the inpatient setting. It was found that patients undergoing ambulatory surgery were more likely to be younger males with a lower relative BMI and a low ASA score compared to their matched inpatient cohorts, and had a lower readmission rate. 28 , 29 , 31 This concept was further emphasized by Fournier et al who recommended inpatient SA for patients with advanced age, increased BMI and pulmonary or cardiac comorbidities. 40
To help physicians better select patients for outpatient surgery, Fournier et al outlined a decision tree used at their institution. In order to qualify for outpatient SA, patients had to be under 70 years old with a pre-op hematocrit >30. Two or more pulmonary comorbidities (sleep apnea, morbid obesity, and chronic obstructive pulmonary disease) were a contraindication for outpatient surgery, and cardiac comorbidities (coronary artery disease, hypertension, and congestive heart failure) were risk stratified based on timing of intervention and cardiology clearance. 35
It is important to consider the definition of outpatient SA when interpreting published results. Of the included articles in this review, only 2 studies published from the same group evaluated same day discharge from a free-standing outpatient surgery center without 23-hour stay. 29 , 40 While some studies discussed same calendar day discharge, many of the database studies and retrospective reviews do not specify the setting of same-day surgery. Performing outpatient same-day surgery in a free-standing ASC without a 23-hour stay capability and discharge on the same calendar day of surgery has different safety and cost implications compared to performing outpatient SA in an ASC physically connected to a hospital or with 23-hour stay capabilities. In the study by Ifeld et al. valuating post-operative pain control, there was one patient admitted in the outpatient group due to the case ending late. 36 The protocol of transitioning a patient from an outpatient to an inpatient stay can be logistically and financially complex, especially in a true free-standing ASC without 23-hour stay abilities. These scenarios should be considered, and an action plan formulated for potential patients requiring ongoing care when developing an outpatient SA program.
The concept of outpatient arthroplasty is not new, especially in the realms of hip and knee arthroplasty. In hip and knee literature, patient social support is a key theme for successful outpatient joint arthroplasty. 42 , 43 For patient selection, Leroux et al mentioned that a reliable caregiver at home was a requirement for outpatient SA. 32 Ensuring appropriate social support for early recovery should be considered when selecting patients for outpatient SA.
As interest in cost reductions for joint arthroplasty grows, especially given the initiation of bundled payments, there has been more research investigating the true cost of outpatient arthroplasty. Outpatient TKA and THA have been shown to be more cost effective than inpatient surgery, with savings driven primarily by the costs of the inpatient stay. 44 , 45 The findings from all studies included in this review evaluating outpatient compared to inpatient costs demonstrate similar cost reductions when SA was performed in the outpatient setting. 22 , 30 , 38 , 39 , 41 It is important to consider potential disincentives towards efficient and affordable care delivered in the outpatient setting. Hospital systems may lose facility fees, and lose revenue related to inpatient admissions, while surgeons with ownership in surgery centers may be financially motivated to perform these surgeries in an outpatient setting. As SA was just recently approved as an outpatient procedure with Medicare with the 2021 CMS updates, previous limitations in utilization may improve over time. 6 , 28 Regulatory support is necessary to ensure access to outpatient procedures for appropriately-indicated patients, regardless of their payor status. Current data demonstrate approximately $2119.53 in cost savings in patients undergoing outpatient SA with bundled payment plans. 23
Appropriate pain control is also a key component of successfully performing SA in the outpatient setting. The included studies suggest a possibly higher rate of re-presentation after discharge with indwelling nerve catheters rather than SS interscalene nerve blocks or even local periarticular anesthetic injection, though the included studies have small sample sizes. Swenson et al reported outcomes of 620 patients treated with indwelling catheters for post-operative pain, including 190 patients with interscalene catheters. 46 There was an overall 4.2% rate of patients requiring re-intervention by the anesthesiologists, with the highest rate (6.8%) seen in patients with interscalene catheters. Additionally, five patients with an interscalene catheter had dislodgement of the catheter during the early post-operative period with three patients requiring repeat SS nerve block. 46 Ilfeld et al. reported that a continuous infusion of ropivacaine via catheter decreased the time to discharge following shoulder arthroplasty relative to patients treated with placebo nerve catheter infusion. 47 These studies demonstrates low rates of complications of continuous nerve catheters but emphasizes the importance of having post-operative systems in place to manage these instances when they arise to minimize potential need for re-admission or treatment through an ED. Additionally, future clarification of the role of continuous nerve catheters relative to perineural injection or single-shot injection would be beneficial in determining the optimal regional anesthetic for outpatient SA.
Both patient and surgeon satisfaction are important considerations when transitioning to outpatient management of SA. With the possibility of reimbursements being linked to patient satisfaction and a push towards value-based care, both of these metrics are being more closely examined. Patients report high satisfaction scores following outpatient SA, 24 , 32 and Brolin et al showed that 78.4% of surgeons performing outpatient SA reported an excellent experience. 15 If both patient and surgeon satisfaction scores are higher in the outpatient setting and SA can be safely performed in the outpatient setting, the proportion of outpatient SA is likely to continue to increase.
Our current review is not without limitations, primarily related to the limitations of the included studies. There are limited studies on outpatient SA and most of these studies represent lower-quality evidence with small sample sizes. The studies that compare complication rates between inpatient and outpatient SA have selection bias, though still do demonstrate that this procedure may be performed safely with appropriate and careful patient selection. Given the heterogeneity of the outcome measures reported, we are also not possible to perform a meta-analysis to provide more quantitative synthesis of the data. Furthermore, given the heterogeneity in reporting and small numbers, we are unable to break down outcomes reliably by SA type such as TSA, RTSA, and HA.
Conclusion
This systematic review demonstrates that outpatient SA, when performed in appropriately selected patients, can be a safe, cost-effective alternative to inpatient SA that leads to high levels of patient and surgeon satisfaction. Given the lack of high-level evidence, however, future research is needed to establish appropriate patient selection and utilization of outpatient SA.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.