
Abstract
Background
Medical professionals remain conflicted about the best rehabilitation protocol a patient should perform after rotator cuff repair surgery. Exercises deemed passive may be activating the shoulder muscles to a moderate level, thus putting the surgical repair construct at risk for re-injury. The purpose of this study was to measure the activation of the rotator cuff and surrounding musculature during exercises used in physical therapy following rotator cuff repair surgery using electromyography (EMG).
Methods
Muscle activation was recorded in fourteen participants performing sixteen exercises. Four fine wire electrodes (supraspinatus, infraspinatus, subscapularis, teres minor) and six surface electrodes (upper and middle division of the trapezius, anterior, medial and posterior head of the deltoid, biceps brachii) were utilized. EMG activity values for each muscle were normalized to the maximum voluntary isometric contraction and activation levels were assessed.
Results
Twelve of the sixteen exercises tested were moderately active in the subscapularis muscle. The results show the subscapularis muscle was activated in all three planes of motion.
Discussion
Most exercises were found to have low activation levels for the supraspinatus, infraspinatus and teres minor muscles. While the exercises examined in this study appear to be safe for the more commonly repaired supraspinatus, caution should be used when administering exercises to individuals with repairs involving the subscapularis.
Keywords
Introduction
Rotator cuff repair (RCR) surgery, while highly successful for relief of painful shoulder pathology, has a high rate of failure with 11–95% re-tearing reported. 1 Early failure generally occurs within the first three to six months post-operatively. 2 It is thought to be due to excessive strain on the surgical repair construct before proper healing has occurred, possibly through over activation of the rotator cuff muscles.3,4 Persistent post-operative stiffness rates range from 1.5–15% and is one of the most common sources of patient dissatisfaction and poor outcomes.1,5,6 A delicate balance of regaining mobility without overstraining the repair site must be maintained in the immediate post-operative time frame. It is critical to engage the shoulder in passive range of motion (ROM) exercises to avoid adhesions, while taking care not to activate the shoulder complex muscles to avoid failure of the surgical repair. In addition, healing of the rotator cuff, specifically the subscapularis, is essential for proper shoulder function after anatomical shoulder arthroplasty. 7
Current RCR rehabilitation protocols are designed with consideration of the patient’s repair and ultimate functional goals for the shoulder joint. 8 Post-operative rehabilitation protocols remain one of the more important factors in determining a successful outcome following RCR surgery. 9 Surgeons and therapists remain conflicted and uncertain about the best rehabilitation protocol a patient should follow after RCR surgery, particularly when to introduce passive and active-assisted exercises during the early post-operative period. 2
Muscle activation levels during passive and active motion can be determined using electromyographic (EMG) analysis. EMG provides information on when, how much and how often a muscle is active throughout an exercise. Surface EMG involves electrodes placed directly on the skin over the muscle belly, while fine wire EMG involves using a needle to insert the electrodes intramuscularly during the testing. Several studies have measured the activation of various shoulder muscles using surface EMG, 10 fine wire EMG,11–15 and a combination of surface and fine wire EMG.16–24 While they provide insight into shoulder muscle activation, these previous studies suffer from lower sample size (n ≤10),10–12,15,17,19 minimal use of fine wire electrodes (≤ 2),13,15–18,22 and analysis of limited rehabilitation exercises23,24 or muscle recruitment patterns instead of rehabilitation specific exercises.20,21 Therefore, the current study focused on determining muscle activation levels of a more comprehensive set of muscles in the rotator cuff and shoulder complex during exercises following the post-operative period of RCR rehabilitation.
The purpose of this study was to measure the activity of the shoulder muscles in volunteers without shoulder pathology during exercises used in physical therapy and normal patient activities following RCR surgery, using fine wire and surface EMG. It was hypothesized that some exercises deemed passive are activating the shoulder muscles to a moderate level of activation, thus putting the surgical repair construct at risk for re-injury.
Methods
Study Participants
The study was approved by the Medical College of Wisconsin Institutional Review Board. All participants signed a written informed consent document. Fourteen participants, eight females (24.9 ± 4.5 years) and six males (27.8 ± 3.1 years) with non-injured shoulders were included in this study. Exclusion criteria were younger than 18 or older than 50 years old, along with any history of shoulder injury, surgery, instability or pain. Participants with extensive knowledge of rehabilitation exercises were excluded to eliminate bias from experience. 23 Participants over the age of 50 were excluded due to the prevalence of asymptomatic rotator cuff tears in adults ages 50 and above.25–27 The dominant hand shoulder was used for all participants.
EMG Placement
All electrodes were placed by a physiatrist board-certified in Electrodiagnostic Medicine by the American Association of Neuromuscular and Electrodiagnostic Medicine. Selected muscles were localized using techniques previously described. 28 The rotator cuff muscles (infraspinatus, subscapularus, teres minor, and supraspinatus) were studied using paired fine wire electrodes (fwEMG). These were identified utilizing a 50mm monopolar EMG needle electrode (Natus Medical, Inc., Middleton, WI) and a Neuro-Stim 3 Plus nerve stimulator (Mainline Medical Inc, GA, USA). Prior to electrode insertion, the skin overlying each area was cleaned using 70% isopropyl alcohol. The four muscles were identified using the landmarks described below and then verified using electrical stimulation. Proximity to the motor point was verified by eliciting the appropriate motor response in the selected muscle with a stimulus intensity of ≤0.8 mA. Then, paired fine wire electrodes housed inside a hypodermic needle (12 cm × 0.05 mm, needle length 50 mm; Natus Medical, Inc., Middleton, WI) were inserted adjacent to the EMG electrode to the same depth as the EMG electrode. For all fine wire electrodes placed, the periosteum was identified, and the needle electrode was withdrawn slightly, and the fine wire electrodes were inserted at this depth. 23 During withdrawal, the wires were protected from being pulled out by pressure applied to the wires as they exited the skin insertion site. Proper placement was verified using the Neuro-Stim 3 Plus attached to each of the fine wires, eliciting the corresponding motor response. After needle removal and confirmation of electrode placement, the wires were looped and taped to the skin and then attached to a Trigno Wireless EMG sensor (Delsys, Inc., Natick, Massachusetts).
For the teres minor, the electrode site was identified by first noting the acromion and the inferior angle of the scapula. A line was drawn between these two points. At the midpoint of this line, the electrode was inserted 1 cm lateral to the lateral border of the scapula. 23 To identify the infraspinatus, the electrode was placed at the center of the scapula, using the scapular spine, medial scapular border and lateral scapular border as landmarks. 23 Identification of the supraspinatus was performed by noting the junction of the middle and lateral thirds of the clavicle. From an anterior-posterior approach, the needle electrode was inserted towards the scapular spine. The subscapularis was located using a medial approach.15,24 With the humerus internally rotated, the needle electrode was inserted anterior to the medial border of the scapula at the midpoint between the spine of the scapula and the angle of the scapula.
For the surrounding musculature, wireless surface electrodes (sEMG) were utilized – trapezius, upper division; trapezius, middle division; deltoid, medial head; deltoid, anterior head; deltoid, posterior head; and biceps brachii (Figure 1). Localization was based on techniques described previously. 29 The electrodes have a bipolar Ag/AgCl surface (Delsys Inc., Natick, MA) with a fixed inter-electrode distance of 1 cm and are 10×1 mm. Gel was not required for these electrodes and were applied to participants using double-sided tape.
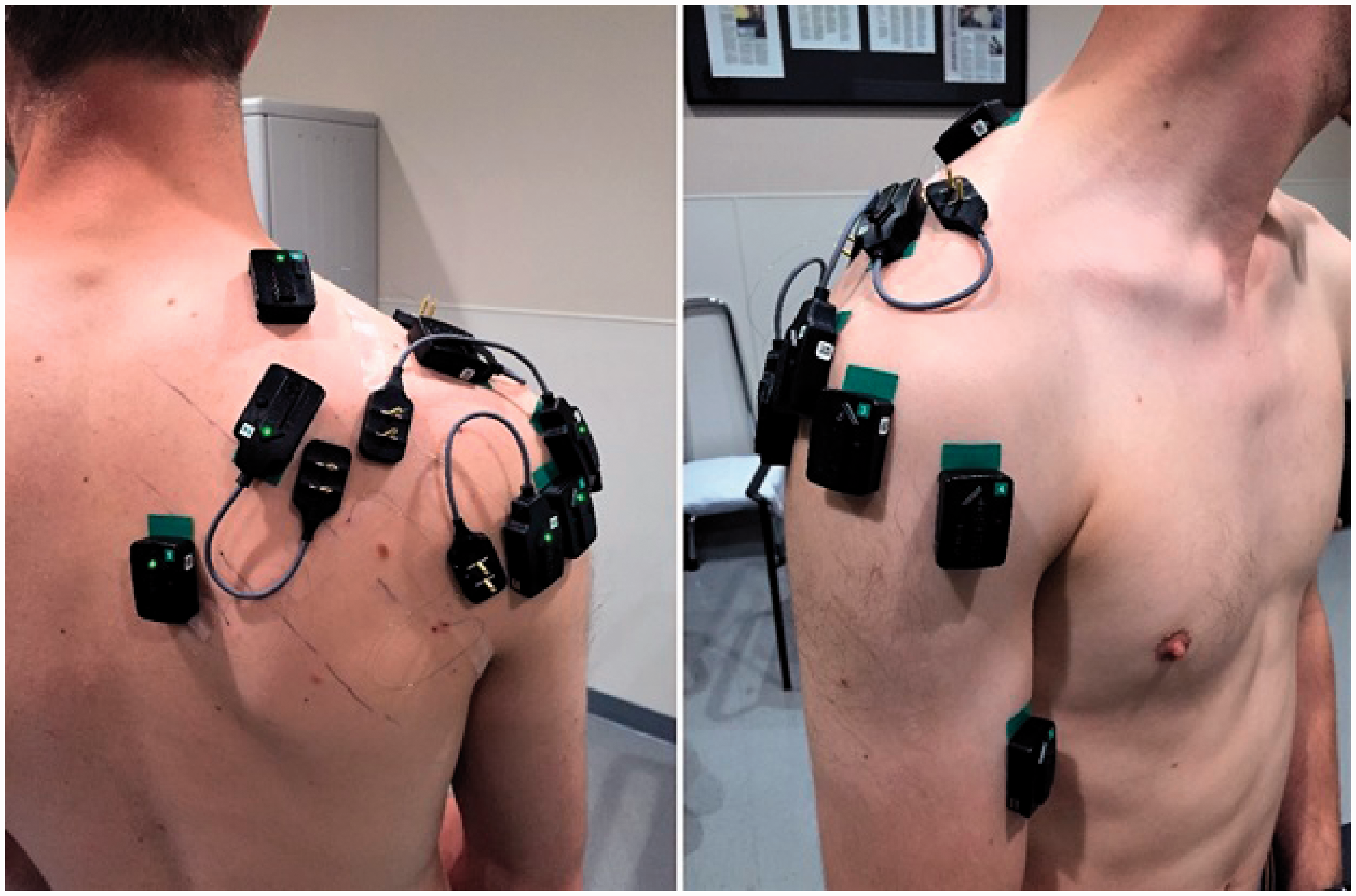
Placement of electrodes on the shoulder with area marked for shoulder brace strap.
Determination of MVIC
After EMG placement, maximum voluntary isometric contractions (MVIC) were recorded for each muscle. Using a Biodex 3 (Biodex Corp., Shirley, NY) dynamometer to position the arm for optimal maximal contraction, the participant was instructed to perform maximal isometric contractions of each muscle three times for three second intervals, with ten seconds of rest between contractions. Arm positions for MVIC testing were based on previous studies (Table 1).18,20,21,30,31
Arm Position and Action for Each Muscle During Maximum Voluntary Isometric Contraction Testing.

Exercises
Participants were instructed by a licensed physical therapist in the proper technique of the tasks. The two physical therapists involved in the study used a script to maintain consistency between participants. Prior to EMG placement, participants were fitted for a shoulder sling with 15° abduction pillow (Arc Shoulder Sling with Pillow, Bledsoe Brace Systems, Grand Prairie, TX) and a shoulder Continuous Passive Motion (CPM) machine (OptiFlex S3, Chattanooga Group, Vista, CA). Participants practiced donning/doffing the brace by themselves as well as with an aide assisting them while instructing them to remain as relaxed and passive as possible while the brace was applied. After being fitted for the CPM machine, the participants were taken through the three preset levels of motion to familiarize them with the machine during testing. For all other exercises, instructions and practice were given after EMG placement and MVIC trials.
Sixteen exercises were investigated: 1) seated active assisted external rotation with a cane, 2) standing active assisted towel slide on a door into flexion, 3) Codman’s pendulums, 4) active assisted swiss ball rolls on a tabletop into flexion, 5) seated active assisted towel slides on a table into flexion, 6) standing active assisted forward bows into flexion, 7) seated active assisted pulleys into flexion, 8) seated active assisted pulleys into scaption, 9) seated active assisted pulleys into abduction, 10) CPM machine level 1: 30 to 50° abduction (ABD), 0 to 10° external rotation (ER), 11) CPM machine level 2: 30 to 95° ABD, 0 to 25° ER, 12) CPM machine level 3: 30 to 140° ABD, 0 to 40° ER, 13) donning sling with abduction pillow, 14) doffing sling with abduction pillow, 15) donning sling with abduction pillow with assistance, and 16) doffing sling with abduction pillow with assistance. The participants practiced each task to the satisfaction of the therapists, and then the therapist instructed the participant to begin the task. At that time, the EMG operator started data collection manually and stopped data collection when the task was completed.
Data Analysis and Processing
EMG activity was recorded for all ten muscles during three repetitions of each task. A baseline EMG measurement was also recorded, with the participant sitting quietly at rest for at least five seconds. The average baseline muscle activation level at rest was determined and subtracted from all other values. Raw EMG signals were collected using a Trigno Wireless EMG system (Delsys, Inc., Natick, MA; CMRR > 80 dB at 60 Hz; gain of 1000; band pass filtered at 20–450 Hz for sEMG and 20–900 Hz for fwEMG) and sampled at 2000 Hz. Analysis of EMG data was carried out using Delsys EMGWorks 4.3.1 Analysis software. The EMG signals were rectified and root mean square (RMS) smoothed using a 62.5-millisecond moving average window. The peak amplitude during the three MVIC trials was operationally defined as 100%. The mean EMG activity values were calculated for each muscle for the entire duration of each task. The means for each muscle were normalized to the corresponding MVIC and expressed as a percentage of MVIC (%MVIC).16,17,23
Previous studies have categorized muscle activation into levels (low, 0–20% MVIC; moderate, 21–40% MVIC, high, 41–60% MVIC, and very high, greater than 60% MVIC).10,11,19,20,32 Long et al. used biomechanical calculations to determine that MVIC values below 15% are safe to perform in early rehabilitation. 16 Based on this, we defined activation levels as: low, 0% to 15% MVIC; low to moderate, 16% to 20%; moderate, 21% to 40%; and greater than 41% as high, similar to those previously defined. 2
A power analysis to detect a difference of 12% MVIC was performed, as pilot data from three subjects showed a range of differences of the rotator cuff muscle activation levels between 6.7 and 11.8%MVIC for all exercises. It was determined that 12 subjects would be sufficient to provide 80% power, when controlling for type 1 error at 0.05 using a 2-sided test.
One hundred and sixty measures (sixteen exercises, ten EMG measurements) were analyzed using SAS version 9.4 (Cary, NC) and R 3.4 (www.r-project.org) statistical analysis software. For every measure, the normal distribution assumption was evaluated using the Kolmogorov-Smirnov normality test and QQ plot. Since the normality assumption was violated for half of the outcomes, the two-sided Wilcoxon signed rank tests was applied to compare the sample median with 15% MVIC activation. Medians were used instead of means because the normality assumption was violated. The sample median estimate and its 99% nonparametric bootstrap confidence intervals were reported for each comparison. Similarly, confidence intervals were calculated for medians.
Results
Twelve of the sixteen exercises showed a median peak %MVIC to be statistically moderately active in the subscapularis muscle. The remaining four exercises also had medians over 20% MVIC but were not statistically significant. The majority of the exercises were found to have statistically low activation levels for the supraspinatus, infraspinatus and teres minor muscles. The supraspinatus exhibited significantly low activation for all but one exercise (exercise 4), active assisted swiss ball rolls on a tabletop into flexion, which only had a median peak %MVIC of 6.7%. Median peak %MVIC and confidence intervals for all exercises for the rotator cuff muscles are reported in Table 2. The surrounding shoulder musculature showed nearly all the exercises to be significantly low muscle activation, except for the middle trapezius, which was not statistically significant. Median peak %MVIC and confidence intervals for all exercises for the surrounding muscles are reported in Table 3.
Median and Confidence Intervals of Fine Wire EMG of the Rotator Cuff Muscles as %MVIC for All Exercises.

Statistical significance levels (p-value < 0.05): low activation = *, median < 15% MVIC; moderate activation = †, median > 20% MVIC.
Median and Confidence Intervals of Surface EMG for Surrounding Shoulder Musculature as %MVIC for All Exercises.
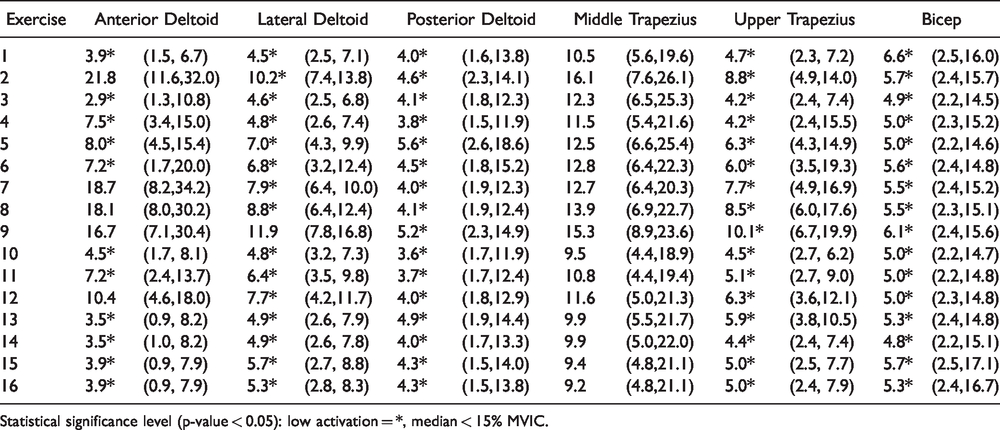
Statistical significance level (p-value < 0.05): low activation = *, median < 15% MVIC.
The subscapularis had the highest activation median of 35.2% MVIC for exercise 6, standing active assisted forward bows into flexion. Standing active assisted towel slide on a door into flexion (exercise 2), active assisted swiss ball rolls on a tabletop into flexion (exercise 4), seated active assisted towel slides on a table into flexion (exercise 5), seated active assisted pulleys into scaption (exercise 8), and seated active assisted pulleys into abduction (exercise 9) were also moderately activated over 30% MVIC. Donning and doffing a sling with and without assistance (exercises 13-16) and the CPM machine level 3 were moderately activated over 30% MVIC. These results show the subscapularis moderately activated in all three planes of motion.
Discussion
The shoulder has the greatest range of motion of any joint in the body, which also makes it an inherently unstable joint. 33 The shallow concavity of the glenoid fossa requires active and passive tension from tendons, muscles and ligaments to maintain joint stability throughout its ROM. Successful use of the shoulder requires coordinated motion and strength from multiple muscle groups concurrently. This makes successful surgical RCR as well as appropriate rehabilitation of the shoulder an exceedingly complex and delicate task. While patient satisfaction along with post-operative ROM and strength rely on a progressive passive early ROM protocol, this must be weighed against the risk of an early strain of the repaired construct by a theoretical over activation of the rotator cuff musculature.
Many studies have investigated the activation of these muscles using EMG in regards to simple shoulder motions, with various electrode arrays, unsupervised or therapist guided rehabilitation exercises, and daily activities on healthy and post-operative patients.10–24 Various recruitment patterns and EMG data analysis methods20,21 have been used to attempt to classify safe and unsafe motions of the immediate post-operative shoulder. The current study investigated tasks involved in the early stages of a rehabilitation protocol as supervised and directed by a physical therapist using a combination of fine wire and surface EMG electrodes to assess activation of the shoulder complex muscles. Results showed, when exercises are properly directed by a physical therapist under controlled conditions in healthy shoulders, there is low muscle activation of most of the shoulder muscles, except the subscapularis.
The subscapularis was consistently excessively stimulated for participants in this study, as evidenced by twelve of the sixteen exercises with a moderate activation level. Fritz et al. had similar findings of high subscapularis activation in healthy shoulders during passive exercises (internal rotation, external rotation, rows), with activation levels ranging from 17.7 to 20.1%MVIC. 14 Smith et al. reported MVICs of 40-63% in their limited series of the upper subscapularis fwEMG during selected exercises, hypothetically due to incorrect execution of the prescribed motions. 19 Elevated subscapularis muscle activity while donning/doffing a sling and donning/doffing a button up shirt was also found by Gurney et al., with an average median EMG of 31.2 and 23.2%MVIC, respectively. 23 Contradictory to the current study, they found lower activation of the subscapularis during sagittal plane pulleys (7.4%MVIC), pendulums (9.3%MVIC), and scapular plane pulleys (10.4%MVIC). 23
Subscapularis tears are less common than supraspinatus, especially in isolation, but repair is crucial as it is the primary internal rotator and a key in maintaining the paired force couple of the shoulder.34,35 Given the elevated muscle activity seen in the subscapularis during the rehabilitation exercises, a more conservative approach may be beneficial in rehabilitation of subscapularis repairs, where a longer period of rest and immobility is prescribed before active or assisted exercises are implemented. This is consistent with recommendations of a more restricted rehabilitation protocol following anatomic shoulder arthroplasty to reduce the risk of failure of the repaired subscapularis.36,37 The results of this study support the role of the subscapularis as a shoulder stabilizer, as it was activated during exercises of flexion, external rotation and abduction.38,39
The supraspinatus, infraspinatus, and teres minor were all below 10% MVIC activation all sixteen exercises. These results indicate that the exercises tested were generally passive in nature for these muscles. This low activation finding was consistent with other studies during similar rehabilitation exercises and activities of daily living.10,17,23,40 The low activation of the surrounding shoulder musculature showed the subjects were keeping their shoulder relaxed during the exercises.
The main limitation of the current study was the use of younger participants devoid of shoulder pathology. The activity of shoulder muscles in healthy participants may not be representative of the activity of individuals post-surgical repaired rotator cuff. Most rotator cuff tears occur in older patients (mean age: 58 years), 41 where our study population mean age was 26.4 years old. Older patients or patients in pain may be more guarded and consequently have a different ability to allow for or follow true passive range of motion. Therefore, caution should be used in applying our results to the general population of rotator cuff repair patients. Future studies assessing older patients with shoulder tendonitis without tear may provide more applicable results to rotator cuff repair patients.
Due to the placement of the fwEMG electrode bases and the spring contact connection of the fire wire electrodes, common passive supine ROM exercises could not be analyzed as the participants would be laying on the wires. Supine external rotation with a cane was modified to a seated position. It is not clear if the more commonly used supine position for patients would have yielded higher muscle activation. Lastly, this study used %MVIC activation to assess risk of exercises. While this is a widely used and accepted method, %MVIC is not a direct correlation to force generated by muscles and there may not be a linear relationship between muscle recruitment and power.11,16 The low activation levels in this study are conservative estimates of safety cutoffs in regard to rotator cuff repair loading limits and should be applied cautiously knowing these limitations.
Conclusions
This study on passive shoulder rehabilitation exercises showed that while none of the exercises were absolutely passive, the bulk of the exercises examined generated low muscle activation levels in the shoulder musculature, with the exception of the subscapularis and the middle trapezius muscles. The moderate activation levels in the subscapularis through all planes of motion should warrant a more cautious approach when administering exercises to individuals with surgical repairs involving the subscapularis, including anatomic shoulder arthroplasty. By knowing muscle activation levels during routine postoperative activities and prescribed rehabilitation tasks of rotator cuff repaired patients, clinicians and therapist are better informed as to the appropriate and safe post-operative activities and exercises for these patients. The results of this study provide evidence that supraspinatus and infraspinatus muscle activation is relatively low for most passive physical therapy exercises, patient CPM machine usage and patient initiated donning and doffing of slings.
Footnotes
Acknowledgements
The authors thank Sergey Tarima and the Medical College of Wisconsin Department of Biostatistics for their assistance with the statistical analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded through a Medical College of Wisconsin Department of Orthpaedic Surgery intramural grant.