
Abstract
A thorough assessment and understanding of glenoid morphology is critical prior to shoulder arthroplasty for primary glenohumeral osteoarthritis. This is due to the fact that multiple studies have demonstrated the importance of reestablishing the native glenoid anatomy on the long-term survivability of the polyethylene glenoid component. In 1999, Walch et al. created a classification system for primary glenohumeral osteoarthritis based upon glenoid erosion and retroversion, and humeral head posterior subluxation. Since its original publication, the Walch classification has been the most widely used classification system for primary glenohumeral arthritis. However, after its initial publication in 1999, additional modifications have been made to the classification to clarify various definitions as well as further characterize other glenoid morphopathology seen in primary glenohumeral osteoarthritis. This article will discuss the original and modified Walch classification, the key differences between the two and the importance of these differences on the classification of the “B2 glenoid.”
The Original Walch Classification
In their original article, using 2-dimensional (2D) axial computed tomography (CT) scans, Walch et al. describe 3 categories and 5 subcategories for glenoid morphology in primary glenohumeral osteoarthritis in 113 shoulders (Figure 1). 1 Type A glenoids were arthritic glenoids with a well-centered humeral head and subdivided into A1 glenoids (43%), defined as those with “minor erosion,” and A2 glenoids (16%), defined as those with “major erosion.” Type B glenoids were described in the setting of posterior humeral head subluxation. These were also subdivided, with B1 glenoids (17%) demonstrating posterior joint narrowing, subchondral sclerosis, and osteophytes, while B2 glenoids (15%) demonstrated a biconcave glenoid due to significant posterior erosion. Type C glenoids were those with greater than 25° of retroversion, regardless of erosion and of dysplastic origin.

The original Walch classification, demonstrating type A, B, and C glenoids and their associated subtypes.
As stated earlier, the key differentiation of a type B glenoid is the posterior humeral head subluxation. Posterior humeral head subluxation was calculated using the mediatrice method, which measured the percentage of the humeral head that lies posterior to a perpendicular and bisecting line to the glenoid face (Figure 2). 1 , 2 The lines measuring both the humeral head diameter and distance of head subluxation were drawn parallel to the glenoid fossa tangent line. Using this method, they defined normal head subluxation between 45% and 55% and suggested that any subluxation greater than 55% constituted posterior humeral head subluxation. They described an average posterior humeral head subluxation of 59% (range, 56.8%–61.7%) among 36 type B glenoids. In addition, they also stated that B2 glenoids, compared to B1 glenoids, were associated with older patients (71 years vs 63 years, respectively) and higher degrees of retroversion (23.4° vs 14.9°, respectively).

Method used by Walch et al. to calculate posterior humeral head subluxation in the original Walch Classification. A, Line tangent to the anterior and posterior glenoid margins. B, Line bisecting the glenoid. C, Line parallel to Line A that lies on medial third of humeral head. D, Line parallel to Line A representing humeral head posterior to Line B. E, Humeral head diameter parallel to Line C. Index of subluxation defined as Line D/Line E.
In their original article, Walch et al. demonstrated good inter- and intraobserver reliability, reporting kappa indices of 0.70 and 0.65, respectively. 1 These values were calculated among 2 observers and only classified glenoids based upon the 3 main types: A, B, and C. However, independent follow-up studies were unable to demonstrate similar inter- and intraobserver reliability to the original study. For example, Scalise et al. found only fair inter- and intraobserver reliability among 4 observers when using all 5 subtypes of the Walch classification (κ = 0.37 and κ = 0.34, respectively). 3 When simplifying the classification into the main 3 types as was done with the original Walch et al. article, the interobserver reliability improved slightly to moderate agreement (κ = 0.44). In regard to B2 glenoids specifically, the interobserver reliability was also fair (κ = 0.32). Although other subsequent studies have found higher observer agreements than Scalise et al., they have not been able to reproduce the agreements found in the original Walch et al.’s study. For example, Nowak et al. demonstrated a moderate interobserver reliability among 8 observers for all 5 subtypes (κ = 0.508), which only slightly improved when comparing only the 3 main types (κ = 0.572). 4 Interestingly, they found the highest agreement for B2 glenoids (κ = 0.714), which they attribute to the often obvious biconcavity that defines the B2 subtype. 4
The Modified Walch Classification
Due to the lower reported inter- and intraobserver reliabilities reported in the literature following the original publication of the Walch classification, Bercik et al. published a modification to the Walch classification in 2016. 5 The main modifications include the addition of B3 and D glenoids in addition to a clarification of the definition of an A2 glenoid. A B3 glenoid was defined as one with uniconcavity due to posterior erosion and with at least 15° of retroversion or 70% posterior humeral head subluxation, or both (Figure 3). A D glenoid was defined as an anteverted glenoid or with anterior humeral head subluxation measuring 40% or less. Lastly, the modified definition of an A2 glenoid is one in which a tangent line to the native glenoid transects the humeral head. Among 3 observers utilizing the original Walch classification, the average inter- and intraobserver reliabilities were 0.391 (fair agreement) and 0.604 (moderate agreement), respectively. Utilizing the modified classification, the inter- and intraobserver reliabilities improved to 0.703 (substantial agreement) and 0.882 (almost perfect agreement). 5

Example of a B3 glenoid described by Bercik et al. and included in the modified Walch classification.
However, there are many differences between the original classification and the modified classification. In the original classification, Walch et al. utilized 2D CT scans, 1 whereas the modified classification utilized 3-dimensional (3D) CT scans. 5 However, 2D CT scans cannot account for patient position and scapular orientation during the study. Therefore, glenoid malalignment can occur and lead to errors in glenoid version. In fact, Boker et al. demonstrated that scapular malalignment of 15° can result in miscalculation of glenoid version by 10 or more degrees. 6 Three-dimensional CT scans allow for orientation of the axial images in the plane of the scapula, thus resulting in a more accurate representation of the glenoid version and are not affected by certain variables, such as patient position.
Another clarification was the definition of a C glenoid. In the original classification, the article describes a C glenoid as one with greater than 25° of retroversion regardless of erosion. 1 The clarified definition describes a C glenoid now as one with 25° of retroversion “not caused by erosion.” 5 This clarification is important because based upon the original definition, many B2 glenoids were incorrectly defined as C glenoids. For example, if a patient had a biconcave glenoid with greater than 25°, the glenoid was incorrectly labeled as a C glenoid.
Another difference between the original and modified classification system was the method by which posterior humeral head subluxation was calculated. As mentioned earlier, the original classification utilized the mediatrice method. However, the modified system utilized the scapular axis method, which calculates subluxation as the amount of the humeral head relative to its diameter that lies posterior to a line drawn from the medial border of the scapula through the center of the glenoid (Figure 4). 5 Depending upon the method used, the calculated subluxation can vary significantly. When evaluating 115 patients with both methods, Kidder et al. demonstrated an average humeral head subluxation of 73.5% when using the scapular axis method versus 59.7% when using the mediatrice method. 2 An example for how such a difference in calculated subluxation can occur is demonstrated in Figure 5. 2 Furthermore, when evaluating B2 glenoids versus original classification non-B2 glenoids utilizing both methods, both demonstrated a statistically significant difference in humeral head subluxation (mediatrice method: 62% for B2 glenoids, 57% for non-B2 glenoids; scapular axis method: 81% for B2 glenoids, 66% for non-B2 glenoids). 2 Despite the scapular axis method calculating a significantly higher degree of subluxation compared to the mediatrice method utilized in the original classification, there was no alteration in the modified classification of the “centered head” 1 definition of 45% to 55% described in the original classification. However, a recent study by Jacxsens et al. suggests that the cut-off value for posterior humeral head subluxation should be 62% or greater when using the scapular axis method on 3D CT scans. 7
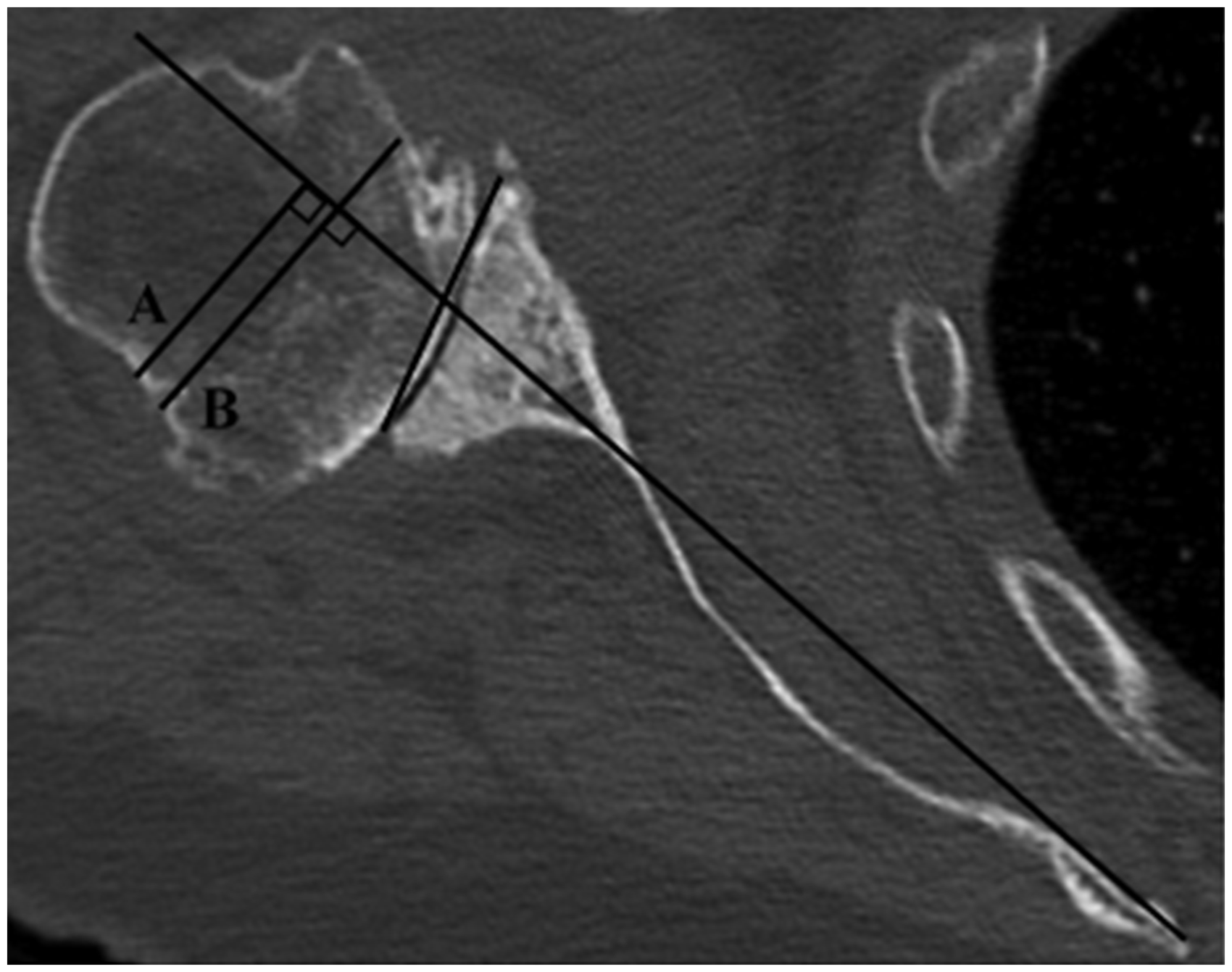
Scapular axis method for determining humeral head subluxation. A line is drawn from the medial border of the scapula through the center of the glenoid. Line A is the amount of humeral head that lies posterior to the scapular axis line. Line B is the humeral head diameter. Subluxation is defined as A/B.

Comparison of humeral head subluxation utilizing the mediatrice method (A) and the scapular axis method (B).
Iannotti et al. recently published an additional modification to the Walch classification, in which they utilized the vault model theory to further define the B3 glenoid, as well as introduce a new subtype, the C2 glenoid. 8 Using 3D CT, they determined that B3 glenoids had no paleoglenoid (or one that is so small that it is unable to be measured), normal premorbid glenoid version, and high pathologic retroversion. Interestingly, a B3 glenoid had significantly more joint-line medialization, but a more centered humeral head compared to B2 glenoids. Although both B3 and C glenoids had similar pathologic retroversion (−22.6°± 6.1° and −23.4°± 3.0°, respectively), C glenoids had a significantly higher premorbid retroversion compared to B3 glenoids (−19.0°± 8.0° and −7.0°± 3.2°, respectively). Using an algorithm based on the premorbid and pathologic retroversion, and joint-line medialization, 73% (19 of 26) of glenoids initially classified as C glenoids were subsequently changed to B3 glenoids. In regard to the newly defined C2 glenoid, it is similar to the B2 glenoid in that it has a biconcave surface. However, both the premorbid and pathologic retroversion of the C2 glenoid (−19.4°± 3.3° and −22.8°± 4.4°, respectively) were significantly greater than in B2 glenoids (−8.3°± 2.8° and −20.2°± 6.6°, respectively). 8 Therefore, the authors believe their findings support the hypothesis that the B2 glenoid is the precursor to the B3 glenoid (Figure 6), ultimately forming when further posterior erosion eliminates the biconcavity and that the native morphology of a C2 glenoid is dysplastic and developed from further erosion of a C1 glenoid. 8

Progression of a B2 glenoid. A, B2 glenoid with posterior humeral head subluxation and a biconcave glenoid. Note the size of the paleoglenoid. B, Two years later, the glenoid remains a B2 but with increased posterior glenoid erosion and smaller remaining paleoglenoid.
Erosion in B2 Glenoids
The key feature of B2 glenoids is biconcavity that occurs secondary to asymmetric posterior glenoid erosion in the setting of a posteriorly subluxated humeral head. 1 When comparing 2 CT scans performed on average 74 months apart in patients with primary glenohumeral osteoarthritis, Walker et al. demonstrated a significantly higher rate of progression of B1 glenoids to B2 or B3 glenoids compared to the rate of progression of A1 glenoids to A2 glenoids. 9 Of the original B1 glenoids, 79% progressed into B2 glenoids and 11% progressed into B3 glenoids, while 81% of the original A1 glenoids remain unchanged. They suggest their results support the hypothesis that initial posterior humeral head subluxation is the precursor to further posterior erosion that is the hallmark of B2 and B3 glenoids. 9 They also demonstrated that B-type glenoids were 8.1 times more likely to undergo joint line medialization compared to A-type glenoids and that this medialization in B-type glenoids significantly increased over time (0.70 mm/year; P = .036), unlike A-type glenoids which did not (0.013 mm/year; P = .95). 9
Chan et al. also further evaluated the B3 glenoid, in which they also proposed the B3 glenoid to be the result of further erosion of the B2 glenoid. 10 Using 3D CT reconstructions, they found a mean retroversion, inclination, and medialization of 24° ± 7°, 8° ± 6°, and 14 ± 4 mm, respectively, as well as a mean posterior humeral head subluxation of 80% ± 8% and 54% ± 6% when measured using the scapular axis and mediatric methods, respectively. Interestingly, they demonstrated that with every 1° increase in retroversion, there was also a 1% increase in posterior humeral head subluxation when measured using the scapular axis method. 10 However, it should be noted that of the 3 glenoids identified initially by Walker et al. as B2 glenoids, none progressed to a B3. 9
As mentioned earlier, by definition, a B1 glenoid is one in which there is posterior humeral head subluxation and posterior joint space narrowing without glenoid bony erosion. This definition was challenged in a recent study by Beuckelaers et al. in which 24 B1 glenoids and 48 B2 glenoids were examined utilizing 3D CT scans with particular focus on glenoid erosion. 11 They determined that regardless of the classification, there was always erosion of the posterior glenoid, with the minimum amount of erosion of 1.7 mm and an average amount of erosion of 4.2 mm. Therefore, despite the original definition of a B1 glenoid stating otherwise, there is always detectable posterior glenoid erosion in B1 glenoids. One possible explanation for this is that, historically, the glenoid wear in 2D CT scans has been measured on the first axial cut just distal to the coracoid. Beuckelaers et al. demonstrated that the posterior erosion in a B1 glenoid was significantly more inferior compared to the erosion seen in B2 glenoids. As a result, the posterior glenoid erosion patterns seen in B1 glenoids are often neglected. 11 The results of their study suggest that while biconcavity remains the hallmark of a B2 glenoid, defining a B1 glenoid as one without posterior glenoid erosion may not be entirely accurate.
Imaging Modalities for Determining Glenoid Classification
As mentioned earlier, the original Walch study 1 as well as subsequent studies3–5 determining inter- and intraobserver reliabilities utilized CT scans in their analyses. However, in the clinical setting, CT scans are often expensive, expose the patient to significant radiation, and are not as easily accessible to patients as plain radiographs. As a result, multiple recent studies have evaluated the accuracy of plain radiographs in determining the proper Walch classification in patients with primary glenohumeral osteoarthritis. Kopka et al. compared preoperative axillary x-rays and magnetic resonance imaging (MRI) images of 50 patients and found moderate agreement (κ = 0.42 and κ = 0.47, respectively) for the original 5-category Walch classification and moderate agreement (κ = 0.54 and κ = 0.59, respectively) for the original 3-category Walch classification. However, when x-rays were compared to consensus MRI images, the agreement was only fair to moderate (κ = 0.21–0.51), suggesting that plain axillary radiographs were inferior to other advanced imaging modalities. 12
Aronowitz et al. performed a similar study comparing plain axillary radiographs to CT scans to determine glenoid morphology according to the original Walch classification. They found substantial intraobserver agreement (average κ = 0.66) for plain radiographs and moderate intraobserver agreement (average κ = 0.60) for CT scans. When 2 observers were compared to each other, there was higher agreement on radiographs than CT scans (κ = 0.48 vs 0.39). Therefore, they supported the use of plain radiographs in determining the appropriate glenoid classification. 13 More recently, Shukla et al. performed a study comparing plain radiographs and CT scans to determine glenoid morphology according the modified Walch classification. 14 They demonstrated substantial intraobserver agreement for both CT scans (κ = 0.72) and radiographs (κ = 0.73). Interobserver agreement was found to be lower, with fair agreement for both CT scans (κ = 0.52) and radiographs (κ = 0.75). In addition, when observing for bone loss and eccentric wear/subluxation, the observers agreed 85% and 70%, respectively. 14
Lowe et al. compared MRI to CT scan in patients with glenohumeral osteoarthritis. 15 Although they demonstrated good interobserver agreement for version measurements for both CT and MRI (κ = 0.73 and 0.62, respectively), they demonstrated only fair interobserver agreement for Walch glenoid classification for both CT and MRI (κ = 0.30 and 0.25, respectively). In regards to interobserver agreement for Walch glenoid classification, the authors found moderate agreement for CT (κ = 0.55), while good agreement for MRI (κ = 0.66). They also found nearly identical identification of A1, A2, and B1 glenoids between CT and MRI; however, there was significant disagreement among B2 (P = .001) and C glenoids (P = .03). Therefore, the authors suggest that while MRI is comparable to CT in determining glenoid version and most Walch glenoid classifications, MRI is less accurate in identifying B2 and C glenoids. 15
Conclusion
A thorough and accurate assessment of glenoid morphopathology is critical prior to any shoulder reconstruction due to the importance of restoring anatomy on the longevity of the implant.16–19 Although the Walch classification has become the most widely used classification system for glenoid erosion in primary glenohumeral osteoarthritis, 1 there have been significant clarifying modifications to the classification to improve its reliability as well as additions to include more recently identified glenoid morphologies. In addition, there are equally important differences between the original and modified classifications that must be appreciated when assessing glenoid morphology, in particular posterior humeral head subluxation and, by definition, type B glenoids. Recent studies have demonstrated that it is this subluxation that ultimately results in posterior glenoid bone loss and the formation of the biconcavity that defines a B2 glenoid. It has also been shown that the B2 glenoid is likely an intermediary between the early B1 glenoid and later B3 glenoid. As a result, the Walch classification plays a critically important role in the preoperative assessment of any patient with primary glenohumeral arthritis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Andrew Jawa is a paid speaker and consultant for DJO Global and Ignite Orthopaedics, receives royalties from Depuy Synthesis, and has equity in Boston Outpatient Surgical Suites. The rest of the authors have no potential conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.