
Abstract
Elbow arthrodesis is an uncommonly performed operation, but it has a specific and niche place in the management of difficult elbow pathology. Many indications and contraindications have been reported, but one of the more challenging aspects of this procedure remains choosing the appropriate angle of fusion. Varying results have been reported along with speculations as to why the fusion may not have been obtained, such as lack of bony structure in the site. Common complications have also been reported most notably fractures distal to the plate. One area of future research is that of the reversibility of this procedure; going from a total elbow arthroplasty to an elbow arthrodesis has been studied well but not so for converting an arthrodesis to an arthroplasty. Elbow arthrodesis remains a valuable but niche solution for complex elbow pathologies that cannot be addressed with other commoner elbow operations.
Keywords
Introduction
Arthrodesis is a less common surgical procedure that has been used for several different joints of the body to fuse together adjacent bones. The typical indication for an arthrodesis procedure is a painful joint when all other treatment modalities have failed to provide a stable pain-free joint. It is generally performed in cases of chronic infection, failed arthroplasty, or comminuted fractures with severe bone loss, where arthroplasty is not possible or has failed. This procedure has been studied and well documented for various joints; however, relatively little has been reported about elbow arthrodesis (EA). In most cases, it remains simply a salvage procedure when all other methods have failed to alleviate painful loss of motion, instability, or infection of the elbow.1,2 Therefore, there has not been much investigation into certain aspects of EA. The goal of this article is to perform a narrative review of EA. A PubMed search with words elbow and arthrodesis was performed and relevant articles were reviewed in order to combine what is known of this procedure and to address possible future areas of investigation.
Indications
One of the first indications for EA was that of tubercular arthritis, but thanks to medical advancements the number of these cases is far fewer than in the past.1–4 Presently, EA has been reported to have a few common indications, of which the most notable are intractable instability, pain, and deep infection of the elbow (Figure 1).1,2,5 Total elbow arthroplasty (TEA) remains a more common procedure than EA due to the total loss of motion and the difficulties this subsequently produces. EA is suitable for failed TEA or patients who have contraindications for TEA.1,3,6 However, EA has been used as a remedy for other less common pathologies such as open intra-articular fractures due to high-impact trauma; e.g., gunshot, motor vehicle, and industrial accidents have been reported.3,4 In addition, it has been performed on soldiers suffering large bone and soft tissue defects.2,3 EA may be considered as a possible option in certain patients with severe elbow rheumatoid arthritis; however, it is less preferred due to polyarticular nature of the rheumatoid arthritis, and other compensatory joints may be also involved in the disease process. 7 Another less common indication may be for comminuted distal humerus fractures in elderly when bone quality is not suitable for osteosynthesis or replacement. Overall, EA remains mostly a last choice procedure with very limited indications because the loss of motion in general is not tolerated by patients when trying to perform the activities of daily living. However, EA has been proven to be the only predictable option when presented with hard to treat conditions of the elbow. 4

A young patient with minimal articular cartilage and a painful elbow joint. H, humerus; LE, lateral epicondyle; ME, medial epicondyle; OF, olecranon fossa.
Contraindications
As EA is an uncommon procedure with limited reported indications, there remains even less knowledge about the contraindications, with very few reported in the literature. When a joint is fused, it loses its mobility; therefore, the adjacent joints must accommodate movement. Because of this, EA is contraindicated in patients who have compromised shoulder and wrist motion/function of the affected arm and in patients with spinal column problems.2,3 This would decrease the patient’s ability to adapt and overcome the range limitation of a fused elbow. Also, it may be contraindicated in patients with compromised soft tissues, as they would not be suitable for flap reconstruction. 2
By the time that patients present, and EA has been established as the operation of choice, many challenges are also present. Mainly, these problems are associated with the presence of infection, poor soft tissue coverage, significant bone loss, poor bone quality, and nerve injuries.1,2,4,5,8,9 The 2 nerves that reportedly seem to be the most affected are the radial and ulnar nerves.5,8,9 Another problem associated specifically with high impact trauma cases is that of the compromise of vascular structures. 2
Operative Considerations
Approach for Arthrodesis
As for the procedure itself, both internal and external fixation have been used; however, internal fixation is usually preferred.1,4 Either anterior or posterior plating is performed, depending on the local anatomy and problem addressed, but in general, posterior plating is the preferred method (Figure 2). 9 It appears that most authors choose to resect the radial head when possible. 5 This is believed to help with the limited forearm rotation; however, Koller et al. found no benefit. 1
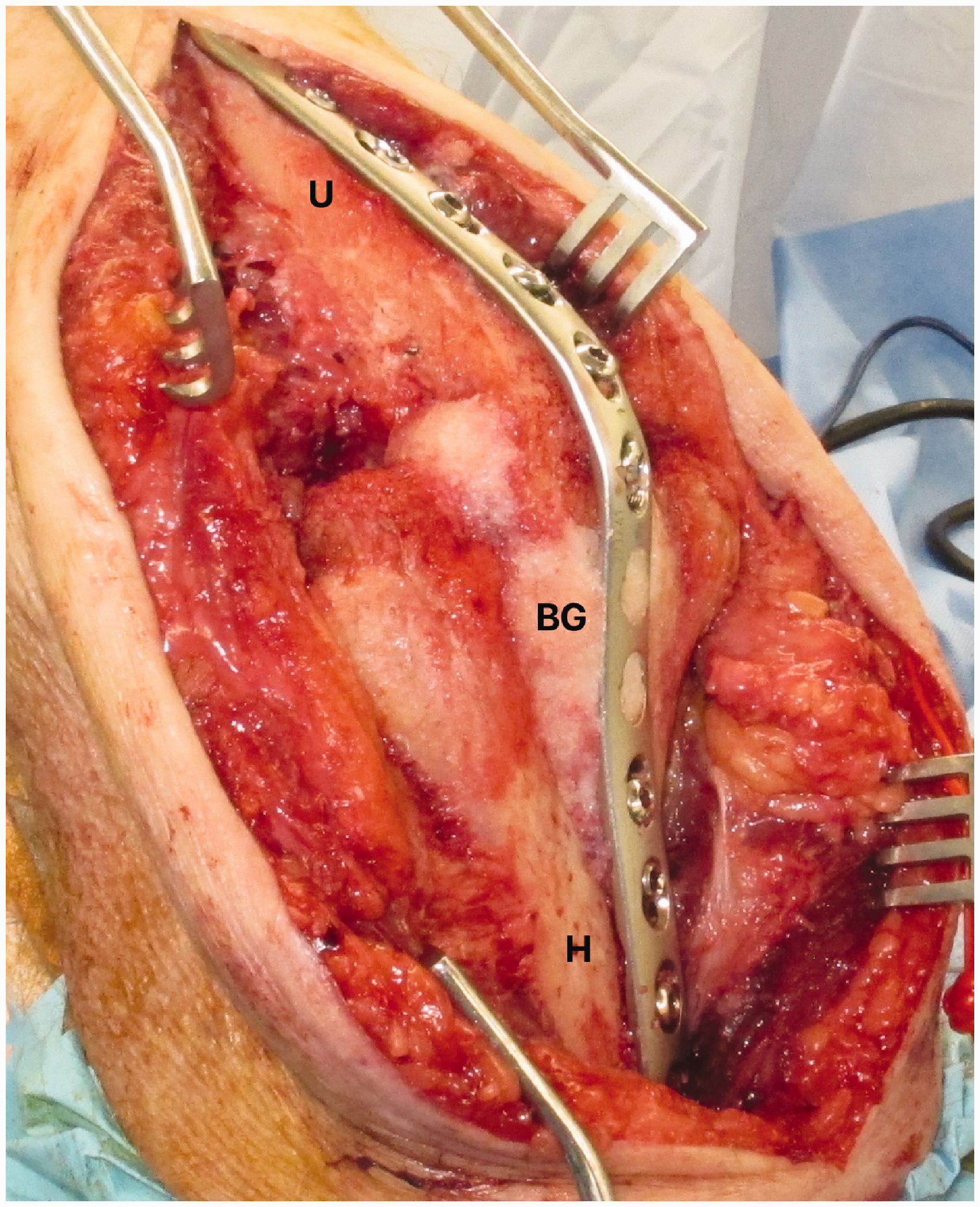
Operative technique of a dorsal locking plate with bone graft impacted into any gaps. BG, bone graft; H, humerus; U, ulna.
Patient Demographics
As EA provides an individual with a stable and pain-free joint, it is usually reserved for younger patients in need of strength; the average age reported being in the mid-40 s.3,8,10–12 There also appears to be gender predilection, more men are reported to have undergone EA than women.3,8,10–12 Bilic et al. reported EA in 9 patients after war injuries, out of which 8 were men. Koch and Lipscomb reported 8 male patients out of total 11 patients with EA. However, Koller et al. reported 14 patients with equal gender distribution with 7 men and 7 women. 1 It has not been investigated to find if this is due to men simply being affected more with certain elbow pathologies or if their desire to have a stable joint, that allows for heavier loading activities, is higher than women. It is possible that men are relatively more likely to present as physical laborers with high occupational demands in such a salvage setting that may require arthrodesis.
Fusion Angle
One of the main considerations when planning to fuse an elbow is choosing the angle. Many investigations have been performed to determine what the most appropriate angle is for EA.1,2,13,14 Historically, 90 degrees has been the standard angle for fusion; it is believed to provide the most strength for an individual.3,4 However, after reviewing different studies, no angle remains clearly superior. Several different factors must be taken into consideration: age, occupation, compensatory ability of other joints, dominant versus nondominant side affected, unilateral or bilateral, and most important is the patient’s choice.1,3,13 It has been reported that an angle of greater than 90° is better for personal hygiene, while an angle of less than 90° is better for daily activities.1,2,13,14 When choosing the angle of the arm in a bilateral arthrodesis, an angle greater than 90° (110°–120°) is preferred for dominant arms, while an angle of less than 90° (40°–65°) is preferred for the other (Figure 3).1,2,14 In this way, the best functional outcome can be obtained. Ozer et al. reported a good functional outcome at 90° due to the patient’s occupation as a teacher and his use of computers in a routine setting, something to consider in today’s technologically advancing society. 8 There also appeared to be a sexual preference when deciding the angle; males seem to choose from a range of 70° to 90°, while females pick from a range of 40° to 70°. 2 Like the sexual discrepancy in having the operation performed, it is not known if there is a reason for this difference. The resection of the radial head allows better forearm rotation. However, the best position for the forearm in cases in which rotation is not possible is a neutral position. Slight pronation position is useful for individuals who desire for better writing abilities and better ability to use a computer. Slight supination is for better object holding ability. 3

Six-month postoperative lateral radiograph demonstrating good osteointegration and a solid fusion.
Although no consensus agreement remains regarding the ideal fusion angle, the surgeon should allow the patient to decide the angle in order to mitigate the functional outcome after discussing advantages and disadvantages of different fusion angles. Locking the patient’s arm in a brace at a varying angle preoperatively may help the patient to make the best choice, given the fact that every patient’s demand and activities are different.
Postoperative Rehabilitation
Something that has not been addressed sufficiently in the literature is the need and benefit of physical therapy for fused elbows. Koller et al. 1 mention that patients develop tricks in order to help overcome the limitations of a fixed elbow and the value of physical therapy in training patients. It is not mentioned that patients received regular physical therapy; therefore, the benefit of such has not been reported. If occupational therapy can be introduced post-surgery and if patients were taught how to accommodate for the lack of mobility of the elbow instead of learning on their own, the recovery process and complications, such as fractures, may be lower. The overall extent and value of a sustained program such as this for patients after EA could prove to be very beneficial.
The role of preoperative rehabilitation has not been discussed in the literature. However, it may be helpful if the patient can be set up for a couple of preoperative sessions of physical therapy with a fixed brace/casting angle, so that patients can get a sense of functional outcomes and realistic expectations after the surgery.
Fusion Rate
As EA is usually a last resort operation, much of the local bone may be compromised at the time of the procedure. If there is not enough bony structure present at the site, the fusion may not be stable or may progress to a nonunion. 1 For this reason, many authors have reported using autologous bone grafts, mostly from the iliac crest.3,4,9,11,15 In a study by Otto et al., local radial head or condyle bone was used; this was to decrease the added morbidity of using iliac crest graft in case of spreading deep infection. 6
Although it can be difficult to achieve high primary fusion rates after EA, due to varying factors, Koller et al. 1 had a successful union in 11 of 14 patients and Bilic et al. 3 did so too with 89% of patients. The average for primary fusions can vary between 50% and 100%. 2 In a study by Otto et al., 6 at the final follow-up, no patient had achieved fusion. The goal of EA is to alleviate the symptoms of the particular elbow pathology and create a stable and pain-free fusion following the first operation. However, this does not always occur due to persistent nerve problems, hardware failure (such as screw loosening or plate breakage), soft tissue complications (such as skin breakdown), persistent infections, or bone graft fractures.1,3,6 Although not commonly reported, in a study by Koller et al., 1 it was found that the average number of revision surgeries needed was 1.4. It is possible that such low rates of primary fusions and resultant need for revision surgeries is due to the overestimation of the quality of soft tissue and bone present, insufficient bony resection, or from not using bony autologous grafts. 1
Outcomes After EA
As there are normally multiple comorbidities in EA patients, function after the procedure can be hard to assess. 4 This is why many authors report overall satisfaction with the procedure as a main indication for success after fusion. Patients who had successful fusions in multiple studies responded that they would have the procedure again and that it has helped.1,4,9,11,15 As the purpose of EA is to achieve a stable, pain-free joint, the ability to perform daily activities and overall use of the arm is also an important inquiry. In a report by Bilic et al., 3 all 9 patients rated their functional daily activities as either good or satisfactory, while Vaishya’s 5 patient was able to fully use his wheelchair and perform daily activities (such as get into/out of his bed and wheelchair) with little or no assistance. The procedure has even allowed patients to return to work; Ozer et al. 8 reported the patient returned to work as a teacher, and 4 of Koller et al.’s patients 1 were able to return to work as well. We did not find studies with the use of preoperative bracing and its relation to positive outcomes.
As pain relief is a major indication for EA, the alleviation of pain is another aspect to be noticed. It is one of the major goals and reason when the patient and surgeon decide to compromise elbow motion. When asked about pain levels associated with the elbow, all of Koller et al.’s 1 patients reported to either being pain-free or with pain not requiring the use of analgesics. In another study, 4 only 1 patient reported pain, but that was due to neuromas of the major nerves.
In the study by A Moghaddam-Alvandi published in German literature, the pain intensity was judged to be low in 13 cases and moderate in 3 cases; no patient reported severe pain. 4 Nine patients complained about occasional pain, 6 patients complained about regular pain, and 1 patient complained of constant pain. The overall results were rated as very good by 3 patients, as good by 11, and with satisfactory results by 2 patients; no patient was dissatisfied with the result. In this study, patients achieved an average of 80 points (65–93) out of a maximum 100 points.
Another important factor to be analyzed is the range of motion (ROM) for the arm (Figure 4). The greatest reported restricted ROM is that of forearm supination and pronation, while the least restricted is both wrist flexion/extension and shoulder abduction/adduction. 1 Although forearm rotation was found to be the most limited, patients were found to compensate by way of shoulder and spinal movements. 1 It seems that for patients who achieve a solid fusion, the main indicators for increased functional abilities and daily activities are both the presence of acquired compensatory abilities and the absence of comorbidities. 1

One-year postoperation of the range of motion.
Complications
A successful uncomplicated procedure is always desired; however, complications do arise and have been reported. EA causes a more substantial decrease in the ability to use the hand than any other arm fusion.2,4,11,14 Once the elbow is fused, it creates a long lever arm and due to this, fractures through the humerus or forearm bones have been reported.1,4,9,10 Along with the creation of a long lever arm, the lack of pro-supination and stiffness of the elbow may contribute to high fracture tendencies. 9 Most fractures tend to occur distal to the end plate (Figure 5).1,4,9,10 In patients with previous surgeries with an external fixator, it is proposed that extending the internal fixation plate past previous pin sites can prevent this complication.1,4

Four-year postoperation, after a fall onto the arm, a fracture at the distal end of the plate was treated conservatively in a cast until the fracture healed, at which point the plate was removed.
Koch and Lipscomb reported 4 out of 17 patients with reinjury and fracture through the elbow. 10 Two patients had fractures through a solid fusion and 2 patients had fractures through a fibrous ankylosis. 10 Koller et al. reported postoperative complications in 6 cases out of 14 cases (43%). 1 These complications included plate fracture in 1 case, humeral fracture in 2 cases, wound complications in 2 cases, and infection in 1 case. McAuliffe et al. reported delayed healing in 4 out of 14 patients which were treated with repeat bone grafting. 4 Eight patients had wound complications, and these wounds were allowed to heal by secondary intention. One patient required transhumeral amputation due to gangrene. Two patients sustained fractures of the forearm bones. More research should be conducted specifically aimed at preventing, or at least reducing, such high rates of fractures.
Reversibility
An area of specific interest that has not been investigated thoroughly is the concept of reversibility of EA to TEA. Successful reversal of other joints is reported, but rarely for the elbow. This could be a beneficial area of research due to the fact that patients’ lives change over time and so does the demand on the elbow. When one is younger, a stable and strong joint is required to lead an active, load-bearing lifestyle, even with the tradeoff of limited ROM. Later in life, it might be more beneficial to have a functional ROM with the tradeoff being significantly reduced load bearing. 6 There are a couple of case reports of conversion of EA to TEA.15,16 One such procedure was performed by Rog et al. 15 with a very good outcome; the patient was satisfied with the results, experienced minimal pain, and was also able to return to work with a lockable brace for his elbow. Rog et al. 15 reported that active elbow extension and flexion was achieved by the patient from 0° to 110°, and almost full forearm rotation was also reobtained. As addressed in his study, there are certain considerations to be taken into account when planning a reversal: the duration of fusion and any alterations to the local anatomy due to previous surgeries. 15 A major concern would be that of neurological function if the elbow has been fused for a long period of time, certain muscles have been inactive and the ability for activation may have been compromised. 15 This was addressed by implanting a specialized device that accurately tensioned the elbow. 15 Burkhart et al. reported a case of 44-year-old patient with left EA who requested a conversion to TEA due to significant restriction of function 7 years after the arthrodesis. 16 It was converted to a TEA and at 3-month follow-up, the patient had no pain and was able to perform most activities.
Recent Advances
Although the procedure for EA has remained relatively standard, either internal or external fixation, with internal fixation being favored, there have been some recent advances. Kovack et al. 2 reported using a stepwise cut of the bone in order to achieve better surface contact and more predictable fusion. Lerner et al. 11 used a hinged external fixation frame that was locked at full elbow extension and then slowly increased in flexion, approximately 5 degrees per day until 90 degrees was obtained. Sala et al. 9 used the Ilizarov frame claiming that it provided an advantage of lowered infection risk, the ability to reconstruct, if there was bone loss, and the possible ability to change the angle of fusion during treatment. Also, Ozer et al. 8 used a rib-latissimus dorsi flap in order to overcome bone and soft tissue deficits. All of these are intriguing approaches and achieved good results showing that the future of the EA procedure may be changing and increasing in efficiency.
Conclusion
In summary, elbow arthrodesis can be a useful procedure in a very few selected indications. Detailed discussion with the patient before the surgery can help identify the patient’s needs and the selection of a proper fusion angle. Complication rates are high and further research is needed to improve the outcomes after elbow arthrodesis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
IRB Approval and Consent
This study was a review of published literature and thus no IRB approval was required. Patients appearing in the photographs consented to having their photographs taken for educational purposes only; not commercial use. These consents were obtained in the clinic verbally, in the presence of the author and the clinic nurse.