
Abstract
Background
Few studies report rate of improvement following reverse total shoulder arthroplasty (RTSA) in a single cohort. The purpose of this study was to compare functional scores following RTSA across postoperative time points in patients who have follow-up scores available at all selected time points.
Methods
A prospective database was retrospectively queried for patients with functional outcome data from preoperatively and after RTSA at 3 to 6 months, 1 year, and 2 years, excluding any patients with data missing at these points. All patients included had measures from every time point. Collected outcomes included American Shoulder and Elbow Surgeons (ASES), visual analog scale pain, subjective shoulder value (SSV), and range of motion.
Results
Outcomes from 173 shoulders were analyzed. Average age was 68 ± 9 years, 68% were females, and 15% were revision cases. The average preoperative ASES score (33 ± 17) improved to 73 ± 18 at 3 to 6 months, 80 ± 19 at 1 year, and 81 ± 19 at 2 years after RTSA. Only outcomes at 1 and 2 years were not significantly different (P = 1.0). SSV scores and forward elevation followed this pattern, with large improvements in the first 3 to 6 months, then reaching a plateau at 1 year. External and internal rotations did not improve by 3 to 6 months, but did significantly improve by 1 year, and remained stable through 2 years. Pain scores improved from 6.8 points before surgery to roughly 1.3 points at all subsequent time points.
Conclusions
Patients undergoing RTSA can expect significant reductions in pain and the majority of their functional gains to occur in the first 6 months after surgery. At 12 months after RTSA, the average patient will achieve maximal improvement.
Keywords
Introduction
Reverse total shoulder arthroplasty (RTSA) results in consistent improvements in shoulder function and pain for patients,1–7 and rates of RTSA have been increasing exponentially over the past decade.8,9 To date, few studies are published examining the rate of improvement after RTSA.10–12 Follow-up studies often present on patient data at final follow-up, or at a minimum of 2-year follow-up, but the follow-up period can span a large range.10,13–17 This makes it difficult to discern the degree of improvement expected at specific time points following surgery and to determine when patients will reach maximal improvement. Recently, Puzzitiello et al. in a systematic review found that maximal medical improvement for anatomic total shoulder arthroplasty occurs at 1 year after surgery. 18 Simovitch et al. examined rate of improvement after RTSA from 3-month follow-up out to 8 years and also found that maximal improvement occurred around 1 year postoperatively. 12 However, this study is limited in that the patient population is different at each time point, which may introduce bias into the data. Accurate data on the rate of patient functional improvement after surgery are important for patient counseling and postoperative guidance. Additionally, these type of data are becoming increasingly important for value-based reimbursement.
The goal of this study was to determine the rate of functional recovery after RTSA from the early postoperative period into the late follow-up period. We followed a set cohort of patients undergoing RTSA and retrospectively compared their preoperative, 3- to 6-month postoperative, 1-year, and 2-year functional scores and range of motion with no patient dropout. We hypothesized that after 1 year no significant functional changes would occur.
Methods
At the authors’ institution, all patients who give informed consent are enrolled into an institutional review board (IRB) approved prospective database that monitors patient outcomes before surgery, at 2 weeks, 3 to 6 months, 1 year, and then yearly after RTSA performed by a single surgeon. A trained, independent clinical research nurse examines patients before surgery and at all postoperative visits. Outcomes collected include the American Shoulder and Elbow Surgeons (ASES) score, 19 visual analog scale (VAS) score for pain (range 0 [no pain] to 10 [max pain]), patient satisfaction, and subjective shoulder value (SSV), where the patient rates their shoulder on a scale of 0 to 100 (completely normal). 20 A standard goniometer was used to measure active forward elevation (FE) and active external rotation (ER) range of motion with the shoulder in 0° of abduction. Active internal rotation (IR) range of motion was assessed as the highest spinal level that the patient’s thumb was able to reach and was coded as follows (based on the scoring system used in the Constant–Murley score): 1 point for end of thumb to lateral thigh, 2 points to the buttock, 3 points to lumbosacral junction, 4 points at L3, 5 points to T12, and 6 points to T7. 21 Medical records are also searched for general patient demographics.
This database was retrospectively queried over a 7-year span for patients who had completed follow-up data available preoperatively, at 3 to 6 months, 1 year, and 2 years after RTSA. Across that 7-year span, there were 888 RTSA cases in the database, of which 20% of procedures were revisions, and 62% of cases were on female patients. Indications for surgery included persistent pain, decreased range of motion, and inability to perform activities of daily living due to any combination of these symptoms secondary to rotator cuff tear arthropathy or irreparable rotator cuff injury. This included patients who presented with rheumatoid arthritis, failed previous arthroplasty, or nonunion/malunion from previous fracture. Inclusion criteria included primary and revision RTSA that had complete data from preoperative, 3- to 6-month, 1-year, and 2-year clinical nurse visits. Revision procedures were considered any revision of a previous arthroplasty (anatomic or reverse shoulder arthroplasty as well as humeral head replacement); previous rotator cuff repairs were not included in revision cases. Exclusion criteria included any cases with missing data points regarding outcomes from any of the follow-up time points. Patients were also excluded if the reason for any of the follow-up visits was due to a major complication that could impact their results at that given time point (ie, not a routine standard-of-care follow-up visit). This included 1 patient who had an infection 2 years postoperatively prompting revision, 1 patient with a periprosthetic fracture due to a fall 2 years postoperatively, 1 patient with a scapular spine fracture due to a fall 1 year postoperatively, 1 patient with a dislocation 1 year postoperatively prompting revision, and 1 patient with abundant heterotopic ossification at 2 years postoperatively.
Operative Technique
All procedures were performed with the patient in the beach chair position with a standard deltopectoral approach. A subscapularis tenotomy was performed with subsequent repair at the end of the procedure, unless the subscapularis tendon was deficient preoperatively. All components were implanted based on manufacturer recommendations. A Trabecular Metal Reverse Shoulder Implant (Zimmer, Warsaw, IN) was used in 160 of the cases and in 13 cases, a Zimmer Trabecular Metal Reverse Shoulder Implant was used but with a DJO Encore baseplate (Austin, TX). Postoperatively, the arm was kept in a sling for 3 weeks with passive range of motion only. All patients start physical therapy starting at 3 weeks postoperatively. Strengthening begins at 6 weeks postoperatively and physical therapy lasts 8 to 12 weeks.
Statistical Analysis
A repeated measures analysis of variance (ANOVA) was used to determine whether there was significant change across all time points (preoperative, 3–6 months, 1 year, and 2 years postoperatively). The significance was adjusted with a Bonferroni correction for pairwise comparisons. Additionally, gender and revision arthroplasty or previous rotator cuff repair were used as between-subject factors in a mixed ANOVA model to determine whether they impacted improvement over time. Revision arthroplasty and previous rotator cuff repair were encompassed in 1 variable where cases were classified as no prior procedure, prior rotator cuff repair, or revision from previous arthroplasty. All statistical analyses were performed using SPSS (v22; IBM, Armonk, NY). The values of P below 0.05 were considered significant. Values are presented as mean ± standard deviation.
Results
Outcomes from 173 shoulders were available at all time points and included in the analysis. Shoulders were from 163 patients, with 10 patients having bilateral shoulders included. The average age was 68 ± 9 years and 68% were females, with additional demographics presented in Table 1.
Patient Demographics.

Abbreviations: HHR, humeral head replacement; RCR, rotator cuff repair; RTSA, reverse total shoulder replacement; TSA, total shoulder replacement.
The average preoperative ASES score was 33 ± 18, and improved to 73 ± 18 at 3 to 6 months (P < .001), and increased again at the 1-year examination to 80 ± 19 (P < .001), with no additional gains observed at 2-year follow-up (ASES 81 ± 19; P = 1.0) after RTSA (Table 2 and Figure 1).
Post Hoc Analysis for Functional Outcomes and Range of Motion Comparing Each Follow-up Time Period, With the Change in Mean and Significance.
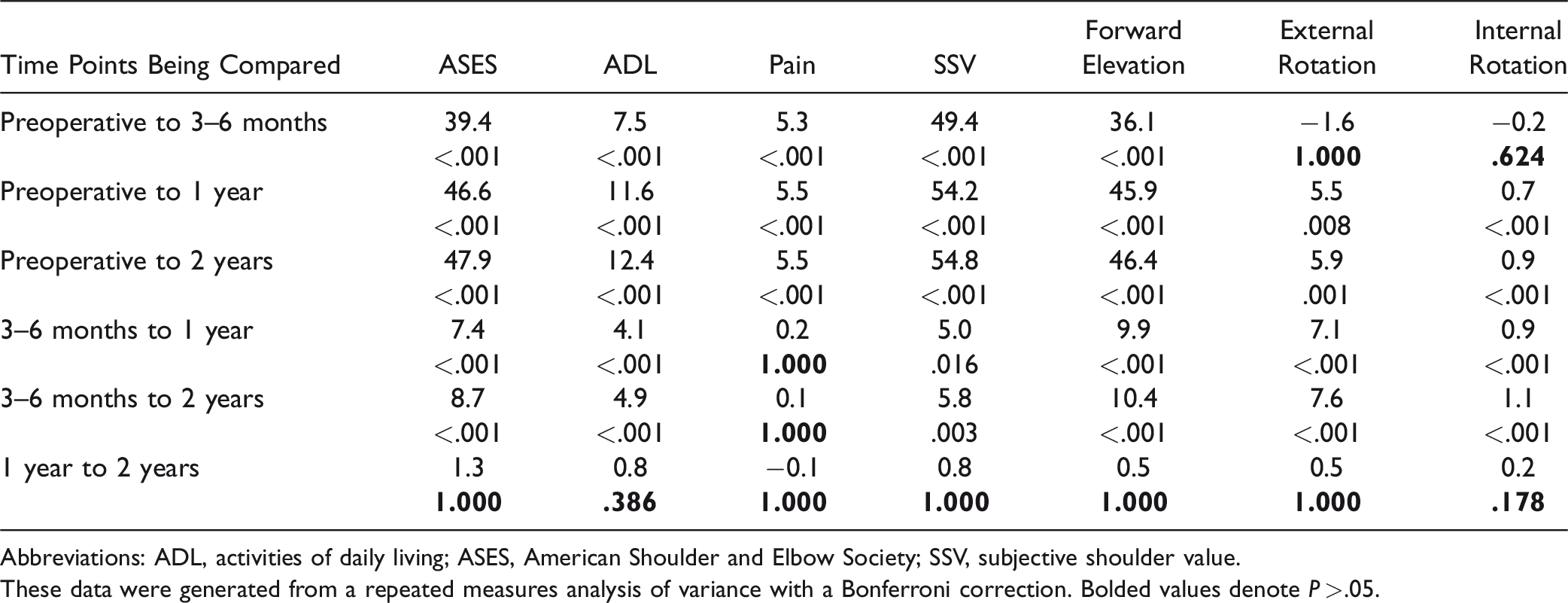
Abbreviations: ADL, activities of daily living; ASES, American Shoulder and Elbow Society; SSV, subjective shoulder value.
These data were generated from a repeated measures analysis of variance with a Bonferroni correction. Bolded values denote P > .05.

Mean scores preoperatively and at each follow-up visit. Error bars represent 95% confidence interval of the mean. Post hoc analysis showed no significant differences for any variable between 1-year and 2-year follow-up. ASES, American Shoulder and Elbow Surgeons.
Patient VAS pain scores averaged 6.8 ± 2.4 points before surgery, and improved to 1.4 ± 2.0 at 3 to 6 months (P < .001), and then remained stable at the 1-year (VAS pain 1.2 ± 1.9; P = 1.0) and 2-year (VAS pain 1.3 ± 2.1; P = 1.0) examinations (Table 2 and Figure 1).
Patient SSV scores before RTSA averaged 27 ± 24, and improved to 76 ± 20 at 3 to 6 months (P < .001), increased again at the 1-year examination to 81 ± 19 (P = .016), with no additional gains at the 2-year follow-up examination (SSV 81 ± 18; P = 1.0) after RTSA (Table 2 and Figure 1).
Patient FE averaged 79° ± 36° before surgery, and improved to 116° ± 24° at 3 to 6 months (P < .001), and increased again at the 1-year examination to 125° ± 21° (P < .001), with no additional gains observed at 2-year follow-up (FE 126° ± 22°; P = 1.0) after RTSA (Table 2 and Figure 1).
Patient ER averaged 21° ± 21° before surgery and remained unchanged with an average of 20° ± 19° at 3 to 6 months (P = 1.0), but increased significantly by the 1-year examination to 27° ± 18° (P < .001), with no additional gains observed at 2-year follow-up (ER 27° ± 17°; P = 1.0) after RTSA (Table 2 and Figure 1).
Patient IR averaged 3.1 ± 1.4 points before surgery and remained unchanged at 3 to 6 months (2.9 ± 1.3, P = .624), but increased significantly by the 1-year examination (3.8 ± 1.4, P < .001), with no additional gains observed at 2-year follow-up (4.0 ± 1.5, P = .178) after RTSA (Table 2 and Figure 1).
In a postanalysis factoring for gender and revision, the interaction between time and revision or previous rotator cuff repair was not found to be significant for any of the examined variables. The interaction between time and gender was significant for FE (P = .001). For males, there was no significant improvement between 3 to 6 months and 1 year (P = .192). Males also had a significantly higher FE than females preoperatively (P < .001) and at 3 to 6 months (P = .001).
Discussion
In this study, we reviewed a set cohort of patients at multiple time points after surgery through 2-year follow-up, with no missing patients at different follow-up points. Based on our data, patients undergoing RTSA will experience the majority of their functional gains, as measured by the ASES, within the first 3 to 6 months after surgery, and typically plateau in terms of functional gains by 1 year. The VAS pain, SSV, and FE measures also followed a similar pattern. The only exception was ER and IR, which did not improve during the first 3 to 6 months, but did significantly improve by 12 months after surgery, and then remained stable through 2 years.
It is clear that patients undergoing RTSA have significant improvements in function at final follow-up.1–6,22 Long-term implant survival rates have also been reported at 91% after 10 years,23,24 and roughly 81% at 20 years for total shoulder arthroplasty in general. 24 These studies largely focus on final follow-up or have extrapolated survival curves due to progressive loss of patients to follow-up with time. To date, only a few previous studies have investigated the actual rate of recovery in the ASES score after RTSA at multiple time points in the acute postoperative period.11,12,25 These authors also found that the majority of gains were achieved in the first 6 months, with most patients reaching a plateau between 12 and 24 months after surgery.12,25
Data by Simovitch et al. compare favorably to our work.12,25 Our data also demonstrated that the majority of functional gains are achieved in the first 3 to 6 months after RTSA, and patient outcomes had, on average, reached their maximum by 12 months, with no change between the mean 12-month and the mean 24-month measures for any outcome in our study (ASES, SSV, VAS pain, FE, and ER). The main difference in our study is that all our patients had follow-up at the same postoperative times out through 2 years. In the study by Simovitch et al., roughly 50% or less of the patients are accounted for at each postoperative time point. 25 This is an unavoidable weakness with studies that have multiple follow-up time points. For this reason, we carefully selected this group of patients who had measurements at all follow-up time points to see whether this altered the data.
It is unclear why rotation improved on a delayed basis compared to all other measures in this study. Unlike the ASES, VAS pain, SSV, and FE, all of which were drastically improved at 3 to 6 months, patient’s IR and ER were not significantly improved until 12 months after RTSA. The center of rotation with RTSA is medialized, and this can have a negative impact on the working of the posterior rotator cuff muscles, making them less effective.26,27 It may take patients a longer period of time to adapt and compensate for the decreased mechanical advantage of these muscles. Additionally, this may also explain why the gains in ER were so small, with the average increasing just 6° from before surgery through 2 years postoperation. It is also unclear why FE increased more slowly in females than males. It is possible that it is due to higher muscle quality in males or because males had a higher mean FE preoperatively.
These data are important in terms of patient management. Knowing the rate in which average patients make functional gains helps to set expectations with regard to patient inquiries on their speed of recovery. When patients ask whether they should expect additional gains at a particular postoperative time point, studies like this offer actual data to base a response. Additionally, if patients are not making functional improvements as expected, knowing where a patient should be may help guide the surgeon as to when additional work up is indicated.
Data of this nature are also important for research. Many journals request or mandate 2-year follow-up for clinical data. However, this comes at the cost of not only prolonging the follow-up period for patients but also prolongs the need for research staff to be contacting patients, storing files, on top of additional IRB reviews to keep the study open. Perhaps some of these requirements might be adjusted if there are enough data to demonstrate patient outcomes plateau by 1 year, at least for certain procedures. These kind of data can also help with research study planning, especially in terms of when to see patients back after a procedure, depending on the goals of the study.
This study is weakened by its retrospective design, which may induce bias into the outcomes. The patients selected for the cohort were picked based on follow-up time points and were not consecutive patients, which may have also introduced bias. This cohort is also relatively small compared to many outcomes-based studies, with only 173 shoulders in 163 patients analyzed. Furthermore, it is a heterogenous cohort with varying pathologies, which may influence the rate of recovery. Future studies with more patients should stratify by specific diagnoses. Additionally, it may have been beneficial to split up the 3- and 6-month visits; however, there were too many patients who fell in between these time points. As with any study with a large number of statistical tests, and many P values, the odds that some of the P values are significant by chance also increases. We attempted to control for this with our statistics by using an adjusted P value. Additionally, the authors feel that these weaknesses are counterbalanced by our cohort having preoperative, 3- to 6-month, 12-month, and 24-month outcome data on 100% of patients at all time points.
Patients undergoing RTSA can expect significant reductions in pain and the majority of their functional gains to occur in the first 6 months after surgery. At 12 months after RTSA, the average patient will have achieved maximal improvement.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: No authors have any direct conflicts related to this study. J. Michael Wiater reports research support from Biomet and DJ Orthopaedics, IP Royalties from Smith and Nephew, consulting fees from Catalyst OrthoScience and Zimmer, and stock or stock options from Catalyst OrthoScience, Coracoid Solutions, and Hoolux Medical.
Ethical Approval
This study was approved by our institutional review board (Beaumont Health IRB# 2006-088). All participants provided verbal informed consent.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.