
Abstract
Background
In an era of advanced shoulder stabilization procedures, arthroplasty implants and techniques, shoulder arthrodesis is considered an end-stage salvage procedure with negative connotations. However, in correctly selected patients, arthrodesis can alleviate pain, provide acceptable and stable motion, with a resultant functional shoulder.
Methods
The current literature on shoulder arthrodesis was reviewed to determine the indications, surgical technique, post-operative rehabilitation, complications and outcomes.
Results
Indications for shoulder arthrodesis include brachial plexus injuries, paralytic disorders, pseudo paralysis from combined severe/irreparable rotator cuff and deltoid injuries, inflammatory arthritis with severe rotator cuff pathology, persistent refractory instability, and tumor resection. Shoulder arthrodesis generally involves compression screws with or without plate fixation and bone graft. The arthrodesis is positioned to optimize the function of the extremity, primarily for activities of daily living. Postoperatively, most patients are immobilized for 8 to 10 weeks, dependent on the completeness of radiological fusion. Complications include nonunion, shoulder girdle muscle atrophy, painful hardware, periprosthetic fractures, and infection.
Discussion
With the use of recent biological innovations, the nonunion rate has declined, and rehabilitation technologies have allowed maintenance of muscle mass for future conversion to shoulder arthroplasty. Hence, in carefully selected patients, shoulder arthrodesis provides a valuable option for a stable, functional, and pain-free shoulder and should be retained as part of the treatment algorithm for complex shoulder pathology.
Keywords
Introduction
In an era of advanced shoulder arthroplasty implants and techniques, shoulder arthrodesis is considered an end-stage salvage procedure by most physicians and patients. 1 However, it is a valuable option in appropriately selected patients, when all other options in the treatment of shoulder conditions have been exhausted or not possible. The goal of this operation is to provide satisfactory pain relief and stable shoulder. In this article, we will provide an updated review of indications, technique, results, and complications of shoulder arthrodesis, with future directions in the form of reversal to arthroplasty in few selected cases of painful arthrodesis.
Indications
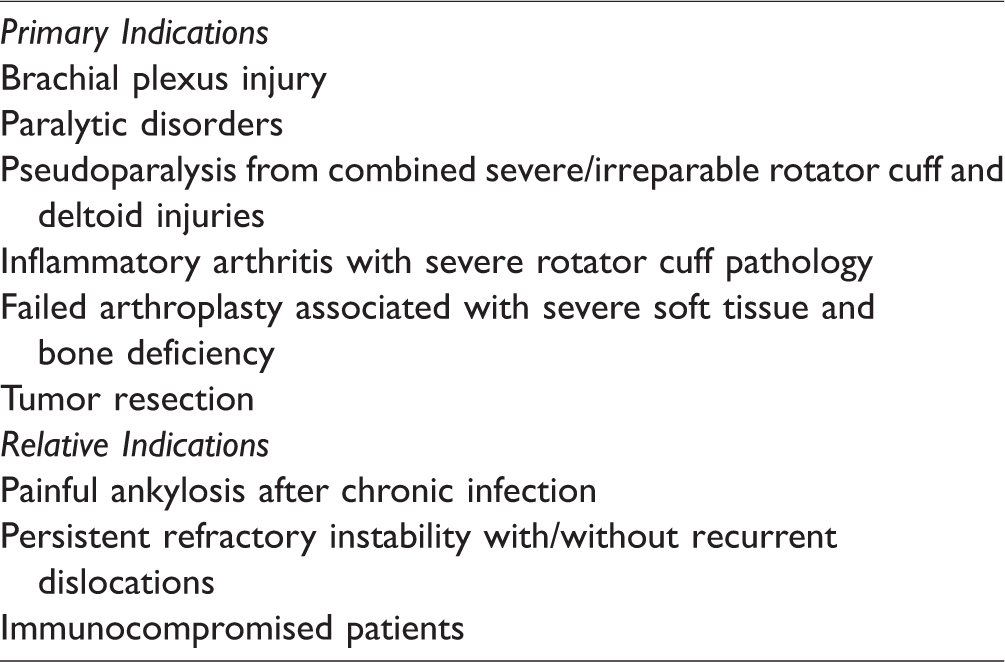
The term shoulder “fusion” or “arthrodesis” has often come with a negative connotation, primarily with respect to a severe limitation of motion and function. However, in a specific patient population, shoulder arthrodesis can optimize function, alleviate pain, and actually provide substantial motion. 2 Primary indications include brachial plexus injury,3–5 paralytic disorders, isolated nerve injuries like deltoid palsy resulting from axillary nerve injuries, pseudo paralysis from combined severe/irreparable rotator cuff and deltoid injuries,6,7 inflammatory arthritis with severe rotator cuff pathology, failed arthroplasty,8,9 persistent refractory instability and/or recurrent dislocations,10,11 and tumor resection.12–14 Relative indications include chronic infection 15 and immunocompromised patients.1,16
To achieve optimal results, it is important to preoperatively assess scapulothoracic mobility and periscapular muscle function. 1 Normal shoulder motion is dependent upon 5 “motion planes”: (1) glenohumeral, (2) scapulothoracic, (3) sternoclavicular, (4) acromioclavicular, and (5) subacromial—coracoacromial arch. The glenohumeral joint (GHJ) as well as the scapulothoracic articulation account for the majority of the motion, in an approximate 2:1 ratio, and hence the scapulothoracic motion has to be well preserved when considering a GHJ fusion. Despite losing motion at the GHJ, the shoulder girdle has an extraordinary ability to compensate and provide significant mobility and function primarily via the scapulothoracic interface (Figure 1). 2

Clinical example of range of motion in patient 3 years status post glenohumeral arthrodesis of right shoulder. A, Forward flexion. B, External rotation. C, Abduction.
Arthrodesis of the GHJ is considered to be relatively contraindicated in patients lacking functional scapulothoracic motion, periscapular musculature (trapezius, levator scapulae, rhomboids, or serratus anterior) paralysis, ipsilateral elbow arthrodesis, contralateral shoulder arthrodesis, Charcot arthropathy, elderly patients, and patients with progressive neurologic disease.16,17 However, while not absolute contraindications, these factors need careful personalized consideration in individual patients when considering GHJ fusion.
Standard Surgical Technique
There are a number of documented surgical techniques for GHJ arthrodesis, with variations primarily involving the configuration of the fixation method, the use of bone grafts, and the postoperative regime prior to the allowance of activities.
Fixation Options
Various fixation options have been used historically from spica casting, compression screws, and compression screws with plates. In the early days of shoulder arthrodesis, postoperative management involved 3 to 4 months of spica casting (without internal fixation). 16 Later, external bone compression was used by Charnley and Houston. 18 Further evolution of glenohumeral arthrodesis involved compression screws described by Beltran et al. 19 and reduced postoperative immobilization to only 1 month. For years, glenohumeral compression screws were the standard fixation method.20–22
In the1980s, Richards et al. 4 described the use of a 4.5 mm dynamic compression plate (DCP) contoured over the spine of the scapula, acromion, and lateral humeral shaft. In his series of 14 patients, 100% obtained solid fusion with postoperative spica casting for 8 weeks. Richards et al. 23 followed this with the use of a single more malleable 4.5 mm pelvic reconstruction plate on a series of 11 patients. The authors concluded that the reconstruction plate provided sufficient stability, a high union rate (14/14 patients), and had minimal complications. In 1997, Groh et al. 24 also recommended the use of a pelvic reconstruction plate. Clare et al. 17 preferred the use of the 4.5 mm pelvic reconstruction plate for most patients but recommend the 4.5 mm DCP plate for heavier patients (>100 kg). In 2009, Chun and Byeon 25 reviewed 8 shoulders and concluded that the use of the pelvic reconstruction plate was useful and achieved eventual fusion in all patients (Table 1).
To be complete, although very infrequently utilized, various articles have described the use of external fixation (with or without compression screws) for arthrodesis.18,26–28 Charnley and Houston 18 described a technique of compression arthrodesis of shoulder using an external fixator. Johnson et al. 27 reported on 4 patients who underwent shoulder fusion with the use of Hoffman external fixator. He observed osseous fusion within 6 to 10 weeks and the fixator were removed between 8 and 15 weeks. Before removal, the fixator was loosened when radiographic evidence of healing was observed and was removed completely after clinical evaluation of healing.
There have also been few reports of arthroscopic guided glenohumeral arthrodesis which will spare deltoid muscle.29–31 In this technique, arthroscope is placed into the joint through standard portals. A burr is used to denude the joint of the cartilage. The placement of the screws can be facilitated either with the help of an anterior cruciate ligament zig or with the help of the O-arm navigation. 31 However, in the later study, only intraarticular fusion was carried out.
Graft Options
As with all operations, preoperative planning is critical especially in determining the need and type of bone graft. For extensive bone loss (possibly due to injury, infection, osteolysis following failed arthroplasty, or tumor resection), structural allografts, tricortical iliac crest graft, or vascularized fibular grafts may be required.9,16 Smaller cancellous defects may be managed with local graft (ie, resected proximal humerus) or with iliac cancellous graft. More recently, many authors are utilizing autologous iliac crest bone marrow aspirate mixed with allograft which provides a larger volume and less morbidity than traditional iliac crest cancellous autograft. 9 We have been utilizing autologous iliac crest stem cell aspirate mixed with allograft demineralized bone matrix and cancellous allograft bone chips which has also provided a very consistent fusion.
Ideal Fusion Position
The ideal position for fusion has been debated for decades, but all agree that shoulder positioning should allow for activities of daily living and hygiene (ie, eating, washing face, dressing/buttoning shirt, reaching back pocket, and even possibly bathroom hygiene). In 1942, the American Orthopedic Association made recommendations for positioning for arthrodesis of 50° abduction, 15° to 25° flexion, and 25° of internal rotation. 32 In the 1970s, Rowe argued that the above degree of abduction lead to periscapular pain due to persistent loading and winging at rest. 21 He suggested 20° to 25° of abduction, 30° of flexion, and 45° to 50° of internal rotation, with remaining functional motion achieved by elbow motion.21,33 Around that time, Cofield and Briggs reviewed 70 patients and did not find a correlation in position with periscapular pain, satisfaction, and activities of daily living. 22 In 2009, Scalise and Iannotti described the optimal position to be 10° to 20° abduction, 10° to 20° flexion, and 35° to 40° internal rotation. 9 Regardless of precisely measured positions, intraoperatively the shoulder should be positioned to optimize patient function and facilitate reaching the mouth, waist, back pocket, and contralateral shoulder (Figure 2).2,9,15,17,23,25,34 Although the literature defines the angles stated earlier, it is practically important for an individual patient, with a specific individual body habitus, to be able to achieve the expected activities of daily living, and the angles of fusion appropriately titrated.
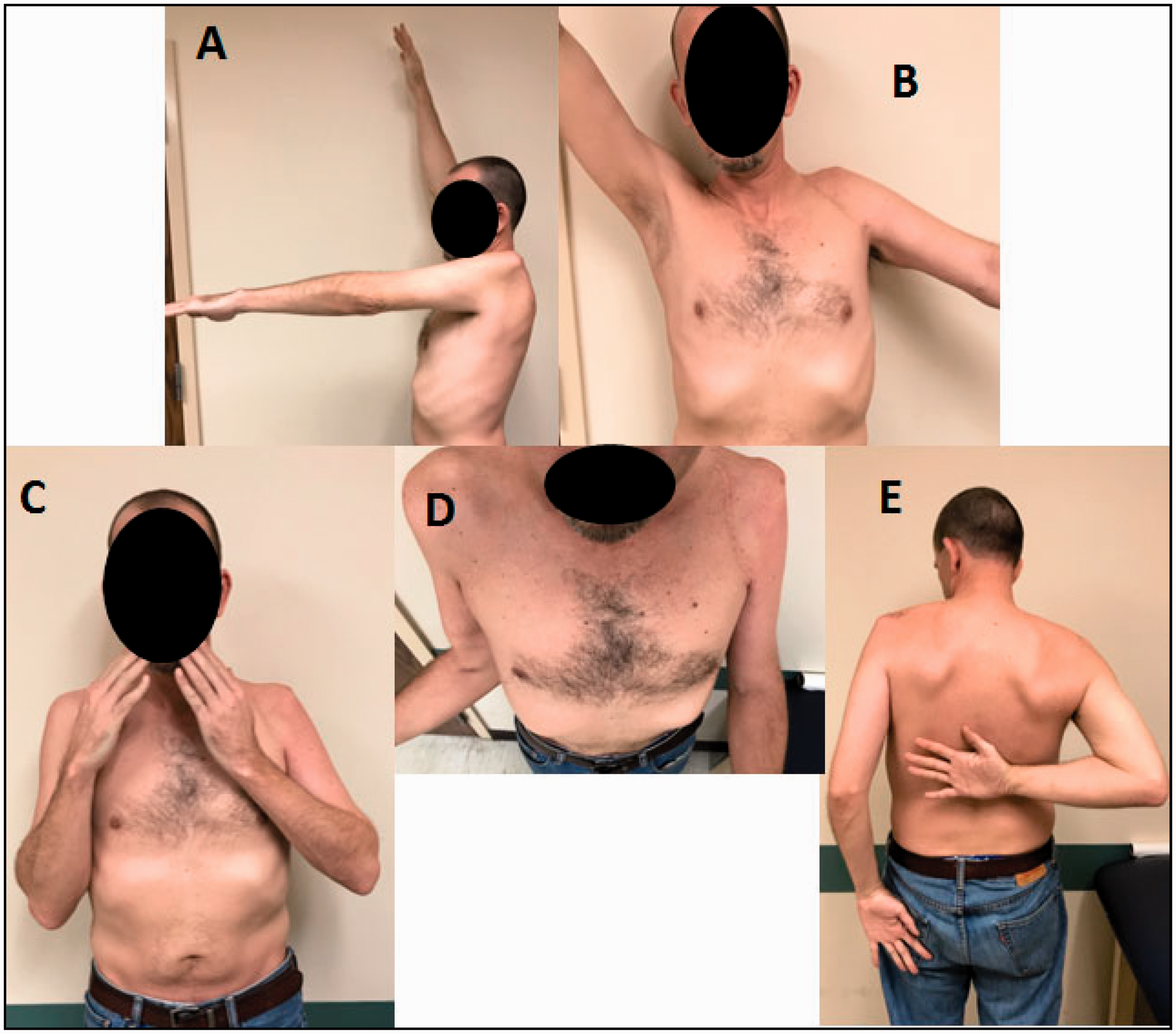
Clinical photos after left shoulder glenohumeral arthrodesis. A, Forward flexion. B, Abduction. C, Hand-to-mouth position allowing eating and hygiene. D, External rotation to neutral. E, Internal rotation to back pocket allowing activities of daily living and hygiene.
Surgical Technique
The optimal patient positioning for a glenohumeral fusion is a semisitting posture of 45° to 60° in a beach chair positioner, with freedom to move the upper extremity into full extension as well as abduction/adduction. Access to the posterior shoulder and the scapular spine is important. Some may prefer a sterile arm holder which facilitates easier positioning of the arm, while others may allow the arm to hang free and be held by an assistant. The deltopectoral approach, first described by Henry in 1957, is the workhorse to the shoulder that allows for extensile exposure. 35 The incision typically incorporates prior deltopectoral incisions and often extends proximally/superiorly over the acromion and the spine of the scapula to allow full exposure (Figure 3). Care should be exercised when exposing the acromion with a goal of gaining exposure while minimizing damage to the deltoid. We elevate the deltoid with an osteotome and a thin sliver of acromion, thereby relying on bone-to-bone healing when reattaching the deltoid. Preserving the deltoid will leave the option of a future conversion to a reverse arthroplasty viable in appropriate cases.

Superficial landmarks for shoulder arthrodesis incision. A, acromion; C, coracoid; Cl, clavicle.
After exposure of the joint, the glenoid is prepared by removing the labrum and articular cartilage (possibly removal of arthroplasty components) and creating a bleeding surface to optimize union, while retaining a bleeding subchondral bone surface when possible. The subacromial surface is prepared by removing all soft tissues and creating a bleeding bony surface without losing of cortical supporting bone. The humerus is placed in the prepared glenoid at the shoulder position preoperatively and intraoperatively assessed to optimize hand positioning as described previously. Two 3 mm Steinmann pins are used to provisionally stabilize the proximal humerus/glenoid in this optimal position.9,16 The proximal humerus is then finally resected to match the prepared glenoid and subacromial contour; depending on bone loss, the resected proximal humerus may provide enough cancellous graft for fusion minimizing comorbidity associated with remote graft harvest. A 4.5-mm pelvic reconstruction plate is contoured over the spine of the scapula, acromion, and lateral humeral shaft. Two partially threaded 6.5 mm cancellous compression screws are placed through the proximal humerus and into the glenoid, attempting to achieve fixation across a minimum of 3 cortices. Likewise, 1 or 2 compression screws can be placed through the acromion into the proximal humerus. The pelvic reconstruction neutralization plate is applied, and typically at minimum, one of the compression screws is placed through the plate. Additional screws to secure the plate, through the acromion and humerus, are placed using AO (Arbeitsgemeinschaft für Osteosynthesefragen) technique followed by bone graft placement to augment the fusion between the proximal humerus, acromion, and glenoid (Figures 4 to 6). The choice of bone graft is according to surgeon’s preference. This author’s preferred method is to use autologous iliac crest bone marrow aspirate mixed with demineralized bone matrix. However, in cases of severe bony deficiency, different options like autologous vascularized fibula, autologous iliac crest bone graft, allograft fibula, or allograft femoral head should be kept available. Fluoroscopy is utilized to confirm the position of humerus relative to the glenoid and acromion and the length of the screws. However, this is simply used to confirm what is visible during the open procedure which is certainly a better depiction of the area of contact between the humerus and the scapula. The deltoid should be reattached over the plate, with nonabsorbable sutures, to provide secure fixation and minimize skin irritation.

Example of 4.5 mm pelvic recon plate used for arthrodesis.

A, Thirty-seven-year-old female laborer with history of prior trauma to right shoulder with recurrent instability associated with poor glenoid bone stock that persisted despite multiple instability procedures. B, Fifty-three-year-old female with osteosarcoma status post resection and shoulder arthrodesis 20 years ago.
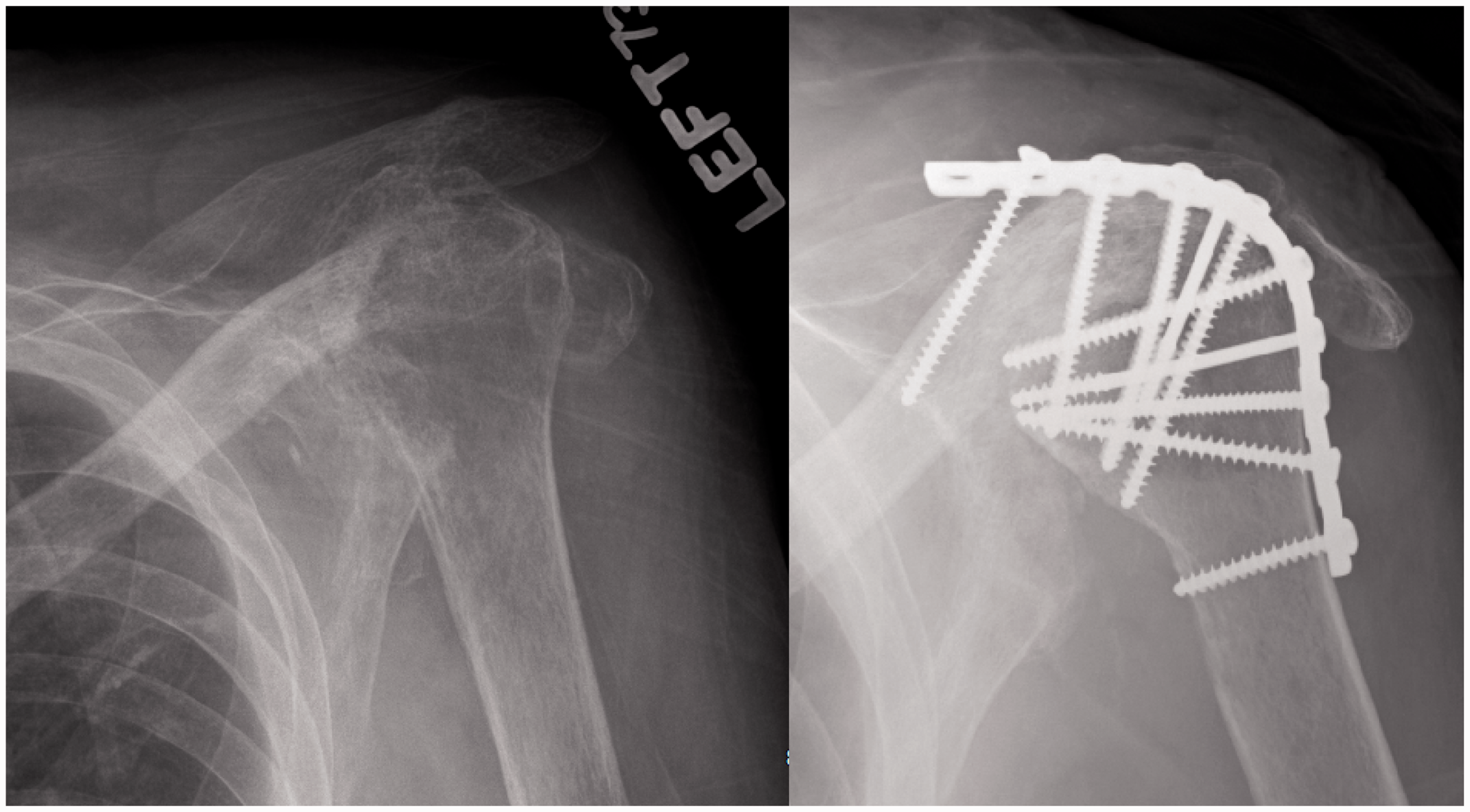
Preoperative and postoperative radiographs of a 75-year-old male with end-stage rotator cuff arthropathy associated with significant glenoid bone loss.
Postoperative Care/Restrictions/Rehabilitation
Postoperative immobilization recommendations in the literature vary. Early recommendations were spica casting for 3 to 4 months, 16 while others have achieved good results with no postoperative immobilization other than an abduction pillow. 36 Most recommend immobilization in a sling incorporating an abduction pillow for 8 to 10 weeks. For more complex cases with severe bone loss or poor bone quality, immobilization for several months with spica casting may be required. We prefer brace incorporating abduction wedge and a circumferential body strap to minimize motion in compliant patients for 8 to 10 weeks. We prefer Spica for noncompliant patients. Elbow, wrist, and hand range of motion is allowed immediately postoperatively to prevent stiffness and loss of function. After radiographic evidence of fusion, periscapular motion and strengthening exercises commence to help optimize function.
Results
Shoulder arthrodesis remains controversial with the availability of modern arthroplasty, but in select patients it is a valuable procedure by optimizing function, alleviating pain, and providing acceptable motion when the arthroplasty option is not possible. Ruhmann et al. 2 reviewed 43 patients at a mean of 6.7 years postoperative and found patients to have ∼56° of active shoulder abduction and ∼60° forward flexion. They saw increases in the Constant-Murley Score (CMS) from 27 to 57 with 91% of patients rating the outcome of surgery as excellent, good, or satisfactory. Unfortunately, they also found a 28% complication rate including pseudarthrosis, infection, and fracture.
Thangarajah et al. 11 reviewed 6 patients with epilepsy who underwent glenohumeral arthrodesis for persistent instability and found improved functional outcomes with no recurrent instability. All patients achieved union at a mean of 2.8 months. Mean subjective shoulder value improved from 37 to 42 and Oxford shoulder instability score improved from 13 to 24.
Scalise and Iannotti 8 reviewed 7 patients who underwent fusion after failed arthroplasty. Mean Penn Shoulder Scores increased from 17 preoperatively to 58 postoperatively with the most common complication being delayed union/nonunion requiring additional secondary bone grafting. However, the authors noted that these cases are extremely challenging due to extensive glenohumeral bone loss and soft tissue deficiency. Often, the autologous iliac crest bone graft is not enough for such deficiencies and other option like vascularized autogenous fibular graft, fibular allograft, or femoral head allograft should be available. The authors further noted that expectations should be realistic and repeated radiographic evaluations are necessary to diagnose nonunions early and additional surgical procedures may be necessary to obtain fusion.
Atlan et al. 37 reviewed 54 patients with a brachial plexus palsy who underwent fusion. Mean shoulder abduction was 59° and mean external rotation was >45°. Fusion rates after 1 attempt were 76% and 94% after reoperation with secondary grafting.
Complications
Complications related to the shoulder arthrodesis have historically been frequent with nonunion being as high as 20% in some series. In Ruhmann’s 2002 article, 38 9% of patients had nonunion. He followed this article in 2005 and showed that union rate was higher in plate arthrodesis versus screw only arthrodesis. 2 In 2007, Dimmen and Madsen 39 also demonstrated good results in fusions using plate fixation. They retrospectively assessed 18 patients over 20 years and found 16/18 with complete fusion and the remaining 2 with asymptomatic partial fusion (glenohumeral or acromiohumeral) radiographically. Despite historically high nonunion rates, several authors have demonstrated nearly 100% union with reoperation and secondary bone grafting.16,25,37
With the use of perioperative antibiotics, Dimmen and Madsen 39 (series of 18) and Chun and Byeon 25 (series of 8) had no infections, while other studies previously have demonstrated 0% to 14% infection rates.2,22,23,25,39–41
In terms of postoperative fracture, up to 11% of patient’s undergoing arthrodesis have had humeral shaft fractures below the plate.2,22,24,34,39 It is felt that a combination of an immobile GHJ, osteopenia, and a stress riser created by the plate lead to periprosthetic fracture. Cofield and Briggs 22 had 8 fractures in their series of 71 patients, while no fractures were reported by Richards et al.4,23 or Stark et al. 36
Another complication is hardware prominence and irritation (Figure 7). Several studies have demonstrated the need for hardware removal after union for symptomatic plates and/or screws.22,23,36 Typically, the most irritation occurs over the scapular spine and acromion due to less soft tissue coverage.

Clinical and intraoperative photos of hardware prominence. A, Hardware prominence resulting in skin irritation. B, Intraoperative photo of prominent plate. C, Plate can be cut in situ or may be removed entirely once fusion obtained.
Reversal to Shoulder Arthroplasty
Shoulder arthrodesis is typically thought of as an end-stage salvage procedure. However, prior literature has shown that fusion may not always be the end of the road. Alta and Willems 42 recently reported on 4 patients aged between 46 and 66 years with persistent pain and dissatisfaction with range of motion after years of arthrodesis (5–11 years). Mean fusion position was 60° to 80° abduction, 20° to 40° flexion, and 40° to 50° of internal rotation. A functioning deltoid was assessed with an electromyogram prior to considering conversion to reverse shoulder. At follow up 22 to 60 months after conversion to reverse arthroplasty, CMS improved from 15–21 to 30–60 and pain (VAS) improved from 8–10 to 0–4 with conversion. Range of motion increased from 40° to 60° forward flexion preoperatively to 40° to 110° postoperatively, active external rotation increased from 0° to 10°–20° postoperatively, and active internal rotation increased from the greater trochanter to L5 and sacrum.
Indications for shoulder arthrodesis.
Older studies have reported on smaller series of patients with conversion from fusion to total shoulder arthroplasty with suboptimal results. Nho et al. 43 reported on a single case of conversion from fusion to total shoulder arthroplasty for persistent pain, specifically scapulothoracic pain. Three months after surgery, the patient noted significantly decreased periscapular pain from that preoperatively; however, he still required narcotics at 9 months. Prior to Nho’s case review, Sperling and Cofield reported on a series of 3 patients with conversion to total shoulder arthroplasty with minimal relief of symptoms. 44 The worse results from these older studies may be attributed to greater atrophic changes to the deltoid. We have performed 11 shoulder arthrodesis in the past 8 years with a protocol that uses stem cell aspirate mixed with demineralized bone matrix which has achieved a 100% first time fusion rate. Postoperatively, patients are maintained on an electrical muscle stimulation unit for 15 minutes per day, to maintain deltoid function and bulk, for the future need for conversion to a reverse arthroplasty. Preservation of deltoid muscle mass and strength may be helpful for future options.
There have been some reports in favor of neuromuscular electric stimulation as modality with or without exercise program to improve muscle strength and endurance.45,46 It is a possibility to use electric stimulation after arthrodesis to preserve muscle strength. However, this need to be further validated in terms of muscles around the fused joints. Some studies have demonstrated beneficial effect of muscle anabolic beta-2 adrenergic agonists like salbutamol and clenbuterol in reducing muscle losses in experimental catabolic states in animal models. 47 These medicines increased muscle weight and carcass protein content in this study. It remains exciting possibility in preserving muscles mass, but their safety and efficacy in humans needs to be further evaluated. However, these studies are limited in numbers and specific recommendations are not available.
We believe that though fusion still remains as an end-stage salvage procedure and probably the last procedure the patient is going to need, but, reversal to arthroplasty may become a possible option, in presence of painful arthrodesis in functionally significantly impaired patient. However, bigger studies with longer follow-up are required.
Summary
With modern shoulder arthroplasty implants and techniques, shoulder arthrodesis is rarely needed. However, in select patients, arthrodesis may provide a valuable alternative to help provide a stable shoulder, alleviate pain, and optimize function and has the possibility to be reconverted to a reverse shoulder arthroplasty.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.