
Abstract
Posttraumatic elbow arthritis presents a difficult problem in young patients. Total elbow arthroplasty may not be suited to the functional demands placed on the prosthesis in younger, more active individuals. Interposition arthroplasty is a useful nonprosthetic alternative in these patients. Various biologic materials have been employed as an interpositional graft, with Achilles tendon allograft being the preferred material. Successful outcomes have been reported in 26% to 94% cases, with the best results in patients with posttraumatic arthritis with stiffness and no underlying instability. Poor prognostic factors associated with this procedure include malalignment and pre- and postoperative instability. Use of a hinged-distraction device to allow immediate postoperative range of motion while protecting the graft may further improve results. In those patients where postoperative instability occurs or where results deteriorate with time, stability and pain relief can be salvaged by conversion to a semiconstrained total elbow arthroplasty.
Keywords
Introduction
Posttraumatic elbow arthritis presents a difficult problem in young patients. Total elbow arthroplasty, while successful in older individuals, may not be suited to the functional demands placed on the prosthesis in younger, more active individuals. Although prosthetic design modifications and the role of hemiarthroplasty present a future treatment alternative in these patients, limited long-term follow-up is available on these techniques to guarantee their results. Interposition arthroplasty is a useful nonprosthetic, biologic solution in these patients.1
Resection arthroplasty was initially described for the treatment of tuberculous arthrosis by Park and Moreau in 1806, and a variety of techniques utilizing interposition materials have since been described. 2 Interposition materials have included silicone, metals, tendon, muscle, fat, skin, and fascia.3,4,5,7, 15 The most popular technique has been cutis or fascial arthroplasty, and results ranging from 26% to 94% success have been reported.3,5–10,11,14--17,19 Modifications of this technique have included the use of a hinged fixator to prevent the postoperative instability that occurs with aggressive soft tissue release.10,13, 15 External fixator placement also allows early motion while protecting the soft tissues, the interposed graft, and the ligament repair or reconstruction. The results of this technique in 13 patients were recently reported, with 62% good or excellent results. 8
One of the theoretical advantages of interposition arthroplasty is that later conversion to total elbow arthroplasty may be performed when the patient has reached a more advanced age. 1 This strategy avoids the potential complications associated with revision of prosthetic total elbow arthroplasty. Interposition arthroplasty preserves bone stock and motion so that total elbow arthroplasty may be performed successfully.
Indications
Interposition arthroplasty may be considered in patients with pain and/or stiffness who are not suitable candidates for prosthetic replacement. Best results have been reported in posttraumatic arthritis with stiffness and no underlying instability, as well as in rheumatoid arthritis.3,5, 6 Patients who cannot tolerate the postoperative lifting restrictions after total elbow arthroplasty (2 pounds repetitive, 10 pounds single event 20 ) are also good candidates for interposition arthroplasty. 8
Contraindications
Patients older than 60 years who are appropriate candidates for prosthetic elbow arthroplasty are a relative contraindication to interposition arthroplasty.1,12,13, 18 Patients with significant deformity (fixed varus or valgus deformity greater than 10°) are also a contraindication to interposition arthroplasty due to increased shear stresses imposed on the graft. 8 Moderate to severe instability is considered a relative contraindication depending on the likelihood of rendering the reconstructed joint stable at the time of the interposition. Active elbow infection is a contraindication to interposition arthroplasty.
Surgical Technique
Preoperative Planning
Careful preoperative evaluation and planning are important to achieve a successful result. Radiographs are essential to determine the osseous morphology. Advanced imaging such as computed tomography with postimaging 3-dimensional reconstruction can be extremely useful in planning for appropriate bone resection and ligament balancing. Specific surgical equipment for this procedure include an interpositional graft (ie, Achilles tendon allograft), a hinged external fixation device (ie, Stryker Hoffman II Dynamic Joint Distractor), and alternative instruments should also be available (eg, total elbow arthroplasty instrumentation and prosthesis).
Positioning and Approach
The patient is positioned supine with a well-padded nonsterile tourniquet applied as high as possible on the arm. An extensile posterior skin incision is typically used, although the prior incision may be used if it does not interfere with the deep approach. The ulnar nerve is dissected and tagged with a vessel loop, and in most cases is transposed in a subcutaneous location at the end of the procedure (Figure 1(A)). Some form of triceps attachment sparing exposure should be employed. Most commonly, Kocher’s interval is developed between the anconeus and extensor carpi ulnaris. The lateral collateral ligament complex and the common extensor origin are next released from the lateral condyle of the humerus and tagged for later repair (Figure 1(B)). An anterior and posterior capsulectomy and bony debridement (coronoid and or olecranon tip) are then performed as required to restore elbow motion. The triceps muscle is elevated from the lateral distal humerus and the anconeus mobilized from its ulnar attachment. The lateral one-half of the triceps attachment is released from the olecranon and the extensor mechanism insertion. The ulnohumeral joint is then exposed with varus stress and supination. If greater than 50% of the trochlea and capitellum are covered by articular cartilage, interposition is not necessary, and debridement and capsular release without interposition is recommended. If the cartilage is severely involved (>50%), interposition arthroplasty is performed.
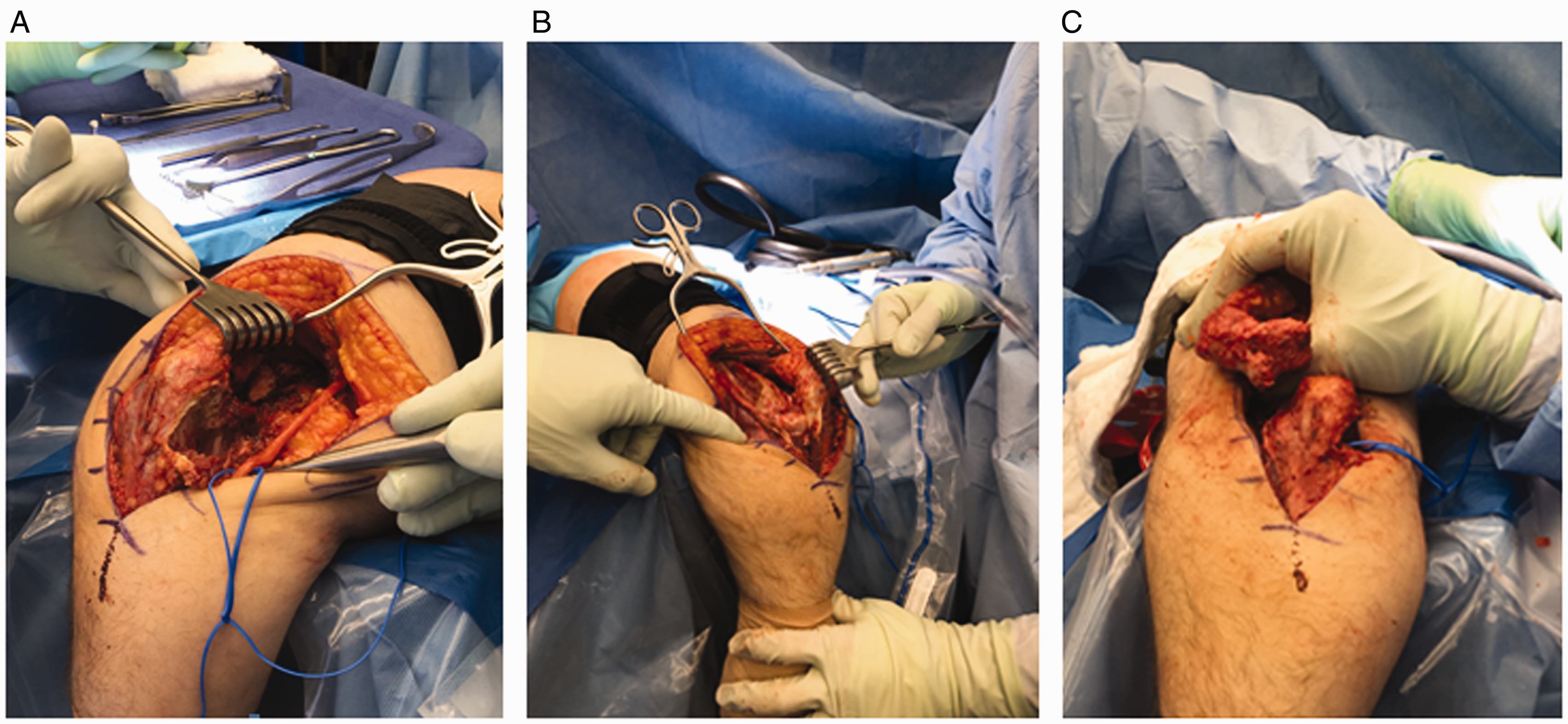
A, Medial approach to the ulnohumeral joint demonstrating the ulnar nerve tagged with a vessel loop. B, The lateral collateral ligament complex and the common extensor origin are released from the lateral condyle of the humerus and the joint is hinged open on the intact medial structures. C, Surface preparation of the ulnohumeral joint. The ulnar and humeral surfaces are prepared with a burr or microsagittal saw to obtain a congruent articulation.
Surface Preparation
The preparation of the bony surfaces is a critical step in the technical execution of this procedure. Care is taken to avoid overaggressive resection of the subchondral bone, which may lead to bone resorption and postoperative instability. The ulnar and humeral surfaces are prepared with a burr or microsagittal saw to obtain a congruent articulation which may be critiqued by direct visualization assessing passive motion following temporary joint reduction. Sufficient bone is resected from the ulnar and humeral articular surfaces to accommodate at least 2 to 3 mm of joint laxity after insertion of the tendon (Figure 1(C)). The medial and lateral trochlear ridges may be removed if necessary to obtain a smooth articulation. The subchondral bone should be preserved if possible.
Graft Application
Fresh-frozen Achilles tendon allografts are the current graft material of choice in the practice of the authors (Figure 2(A)). The graft is thawed at the start of the procedure in sterile saline, ringers, or antibiotic solution. Drill holes are made across the distal humerus with a 2 to 2.5 mm drill to allow for the passage of #2 braided nonabsorbable sutures (Figure 2(B)). The graft is laid across the distal humerus, and excess anterior edges are trimmed from the sides. Additional strips of the graft are preserved in the event that lateral or medial collateral ligament reconstruction if required (Figure 2(C)). Using a horizontal mattress stitch, the graft is sutured to the distal humerus through the drill holes (Figure 2(D)).

A, Achilles tendon allograft is the preferred interposition material. B, Drill holes are made across the distal humerus with a 2–2.5 mm drill to allow for the passage of #2 braided nonabsorbable sutures. The graft is laid across the distal humerus, and sutures are used to secure the graft. C, Additional strips of allograft are preserved to augment reconstruction of the medial and lateral collateral ligaments. D, Horizontal mattress stitch is used to secure the graft to the distal humerus through drill holes.
Ligament Reconstruction
After the ulnohumeral joint is reduced, the integrity of the medial and lateral collateral ligaments is assessed. The congruency of the articulation and elbow range of motion are determined. In most cases, the medial collateral ligament is satisfactory and reconstruction of the lateral collateral ligament alone is necessary. If adequate tissue is present, the lateral collateral ligament is repaired primarily. If inadequate, a lateral strip of the tendon graft is secured to the anatomic origin at the lateral epicondyle and distally secured at the crista supinatoris through a drill hole (Figure 3(A)). Subsequently, medial collateral ligament may be reconstructed if necessary for stability (Figure 3(B)). These reconstructions may also be augmented with suture anchors placed at the point of origin of both the medial and lateral collateral ligaments (Figure 3(C)).

A, Lateral collateral ligament reconstruction. B, Medial collateral ligament reconstruction (Frasier tip suction used as pointing device). C, Suture anchors used to augment reconstruction of collateral ligaments.
In cases where both lateral and medial collateral ligaments are found to be deficient, another option is a transosseous drill tunnel through the distal humerus, replicating the axis of rotation. A second tunnel connects the sublime tubercle and the tubercle of the crista supinatoris. The distal strands of the allograft are threaded through the humeral tunnels ulnar tunnels to create a “sling” to reconstruct both medial and lateral collateral ligaments in anatomic location. The sling is tensioned to maintain joint stability and to allow for a congruent flexion-extension arc. Following the reconstruction, the elbow is again taken through a range of motion and tested for stability.
External Fixator Application
When ligament reconstruction is performed and/or when the stability of the joint is not adequate, a hinged external fixator (DJD I or II Dynamic Elbow Joint Distractor, Stryker, Kalamazoo, MI) may be applied (Figure 4). This fixator may also be used to apply distraction, reducing forces on the interposition graft.

When ligament reconstruction is performed and/or when the stability of the joint is not satisfactory, a hinged external fixator (DJD I or II Dynamic Elbow Joint Distractor, Stryker, Kalamazoo, MI) may be applied.
Postoperative Care
Patients are typically treated with continuous passive motion (CPM) in the hospital with an axillary block for regional pain control. Postoperative indomethacin or single-dose radiation may be given preoperatively to minimize risk of heterotopic ossification following surgery; however, this is not a common complication and is not routinely used. In patients where there is significant swelling and the wound is threatened, an initial period of splinting in full extension for 48 to 72 hours is appropriate, after which the use of CPM is reevaluated. Patients are dismissed home when the wound is not threatened and range of motion goals are reached. CPM is continued at home where appropriate. In those with external fixator application, removal of the external fixator is performed under anesthesia 3 to 4 weeks following the initial procedure. The elbow should be gently moved through the full range of motion at this time, though no forceful maneuvers should be employed. Static adjustable flexion and extension splints may be used 23 hours per day for an additional 3 weeks to maintain the range of motion obtained at the examination under anesthesia. Maintenance bracing may be continued for 8 to 12 weeks as necessary.
Outcomes Analysis
There are multiple case series which have investigated the results of interposition arthroplasty for elbow arthritis, though indications, techniques, and graft choices varied widely. Two series reporting the results of tendon distraction interposition arthroplasty using current techniques are available.3, 8
Cheng and Morrey reported the results of interposition arthroplasty in 13 patients with elbow arthritis and average age of 33 years. 3 Fascial interposition was performed and a hinged distraction device was applied for 4 weeks postoperatively. At an average follow-up of 5.2 years, 62% satisfactory results were reported according to the Mayo Elbow Performance Score. Pain relief was achieved in 69% of patients; however, inferior results were associated with preoperative instability.
A recent retrospective study evaluated the results of the current technique (Achilles tendon allograft interposition arthroplasty) for the treatment of inflammatory (45) or posttraumatic (34) elbow arthritis. 8 A hinged external fixator was used postoperatively in the majority (31) cases. At a mean 6-year follow-up (range, 2.9–10.5 years), the flexion-extension arc improved from a preoperative mean of 51° to 97° postoperatively. Seven patients subsequently underwent revision surgery: 2 infection cases, 2 instability cases, 1 elbow arthrodesis for instability, and 2 elective total elbow arthroplasties. In the patients with surviving allografts (38), Mayo Elbow Performance Scores improved from 42 to 65 postoperatively. Twenty-nine percent of patients obtained a good or excellent result, 31% a fair result, 24% a poor result, and 16% were revised. Subjectively, 27% of these patients rated the elbow as somewhat better, 42% rated the elbow as much better following the interposition procedure, and 80% indicated in retrospect, they would still have the procedure performed.
Laubscher et al. preformed a retrospective review of 18 consecutive cases of interposition arthroplasty in young patients with mean age of 41 years with the primary diagnosis of posttraumatic osteoarthritis in 12 cases and inflammatory arthritis in 5 cases. At a mean 54-month follow-up, 1 case was excluded due to incomplete follow-up and 7 cases were revised. In the 10 patients with the interposition currently in situ, mean visual analog scale score for pain improved from 7.4 to 2.4 and mean Mayo Elbow Performance Score improved from 42 to 76 points. 21
Failure of Interposition Arthroplasty
In young patients where interposition arthroplasty is performed as a temporizing procedure, semiconstrained total elbow arthroplasty can be performed successfully at a later date. The results of 13 consecutive semiconstrained total elbow arthroplasties in 13 patients with prior interposition arthroplasties for degenerative elbow arthritis were evaluated at an average follow-up of 8.8 years. 1 The average age at the time of operation was 50 years (range, 29–80), and the average interval from interposition arthroplasty to total elbow arthroplasty was 12 years. At follow-up, postoperative pain was rated as mild or none in 11 patients, and satisfactory results were achieved in 11 of the 13 patients (85%) The average Mayo Elbow Performance Score (MEPS) improved from 34 preoperatively to 84 postoperatively. There were 3 excellent, 6 good, 2 fair, and 2 poor results. All of the elbows were stable following arthroplasty, and all patients were subjectively satisfied with the procedure.
There have also been reports of revision interposition arthroplasty with reasonable outcomes. The results of 9 patients with average age of 47 with severe posttraumatic arthritis who underwent revision of a failed interposition arthroplasty with a further interposition procedure using Achilles allograft were evaluated with an average follow-up of 4.7 years. 22 The mean MEPS improved from 49 preoperatively to 73 postoperatively. One was lost to follow-up, but of the remaining patients, 1 had an excellent, 2 had good, 3 had fair, and 1 had a poor result. Subjectively, 5 of the 9 patients were satisfied. Four continued manual labor.
Case Example
A 23-year-old right hand-dominant female presented 1 year following a motor vehicle collision. Her injuries from the collision consisted of a left elbow fracture-dislocation, multiple lower extremity fractures, and a traumatic brain injury that left cognitive deficits with mildly impaired cognition. Her elbow injury had initially been treated medically by her previous health-care provider with attempted reduction, nonoperative management, and physical therapy. Upon presentation, elbow radiographs demonstrated a chronic posterior dislocation with posttraumatic arthrosis and heterotopic ossification diffusely about the elbow joint (Figure 5). Her physical examination revealed severely limited, painful elbow range of motion restricted to a 10° motion arc from 70° to 80° flexion. She had less than 5° supination-pronation and full pain-free range of motion of both shoulder and wrist with an intact neurovascular examination. Given the patient’s age, activity level and chronicity of the injury, elbow interposition arthroplasty with Achilles tendon allograft was recommended.

Preoperative radiograph of chronic elbow fracture-dislocation.
A standard posterior, midline incision was used for the approach. The ulnar nerve was dissected and tagged for transposition. Medial and lateral windows were made about the distal triceps to visualize the ulnotrochlear joint, which was found to be posteriorly dislocated. The common flexors and extensors were then released from the distal humerus to allow access of the collateral ligaments which were severely deficient. There was severe arthrosis involving both the proximal ulna and distal humerus with complete denuding of the cartilage and a small area of almost complete ankylosis between the medial proximal ulna and trochlea.
The ulnotrochlear joint was now prepared with the use of osteotomes and a microsaggital saw making sure to leave enough subchondral bone to prevent bone resorption but removing enough bone to allow a congruous fit with the proximal ulna. Three tunnels were now drilled in the distal humerus from anterior to posterior to secure the Achilles tendon allograft that was now prepared and sized to fit over the distal humerus. The allograft was then secured to the distal humerus with the use of #2 FiberWire (Arthrex, Naples, FL) passed through the drill holes and tied in a horizontal mattress fashion. Two 5-mm wide tails were cut off the medial and lateral ends of the allograft to fashion as medial and lateral collateral ligament reconstruction.
The ulnotrochlear joint was then reduced with graft in place. Four 4.75 mm SwiveLock anchors (Arthrex) were now inserted into the isometric point for each medial and lateral collateral ligaments proximally and distally at the sublime tubercle and crista supinatoris, respectively. The 2 medial and lateral tails of the graft were used as augments to the reconstruction of the remaining native medial and lateral collateral ligaments. Once fixation was complete, excellent stability was restored. The medial and lateral paratricipital windows were then closed and the ulnar nerve was transposed anterior to the medial epicondyle. The common flexor and extensor origins were repaired back to the distal humerus.
An external fixator (dynamic hinged external fixator (DJD II, Stryker, Kalamazoo, MI) was now applied in standard fashion to protect the ligament reconstruction, with some distraction applied at the joint. We placed an additional bar-to-bar pin to lock our fixator at 90° to allow the soft tissues to heal without tension. Intraoperative fluoroscopy was used to assess for adequate, stable reduction, which was achieved.
The postoperative course consisted of removing the bar-to-bar pin at 4 weeks to allow for gentle range of motion in a stable arc of 30° to 90° of flexion. At 6 weeks, the external fixator was removed in the operating room followed by fluoroscopic examination under anesthesia to assess mobility and stability (Figure 6). During the examination under anesthesia, we were able to passively flex and extend the elbow from 30° to 100° in a stable arc (Figure 7). Physical therapy was initiated at this point to help improve overall flexion. At the 12-week follow-up, the patient had a stable arc of motion from 30° to 130° with minimal pain.
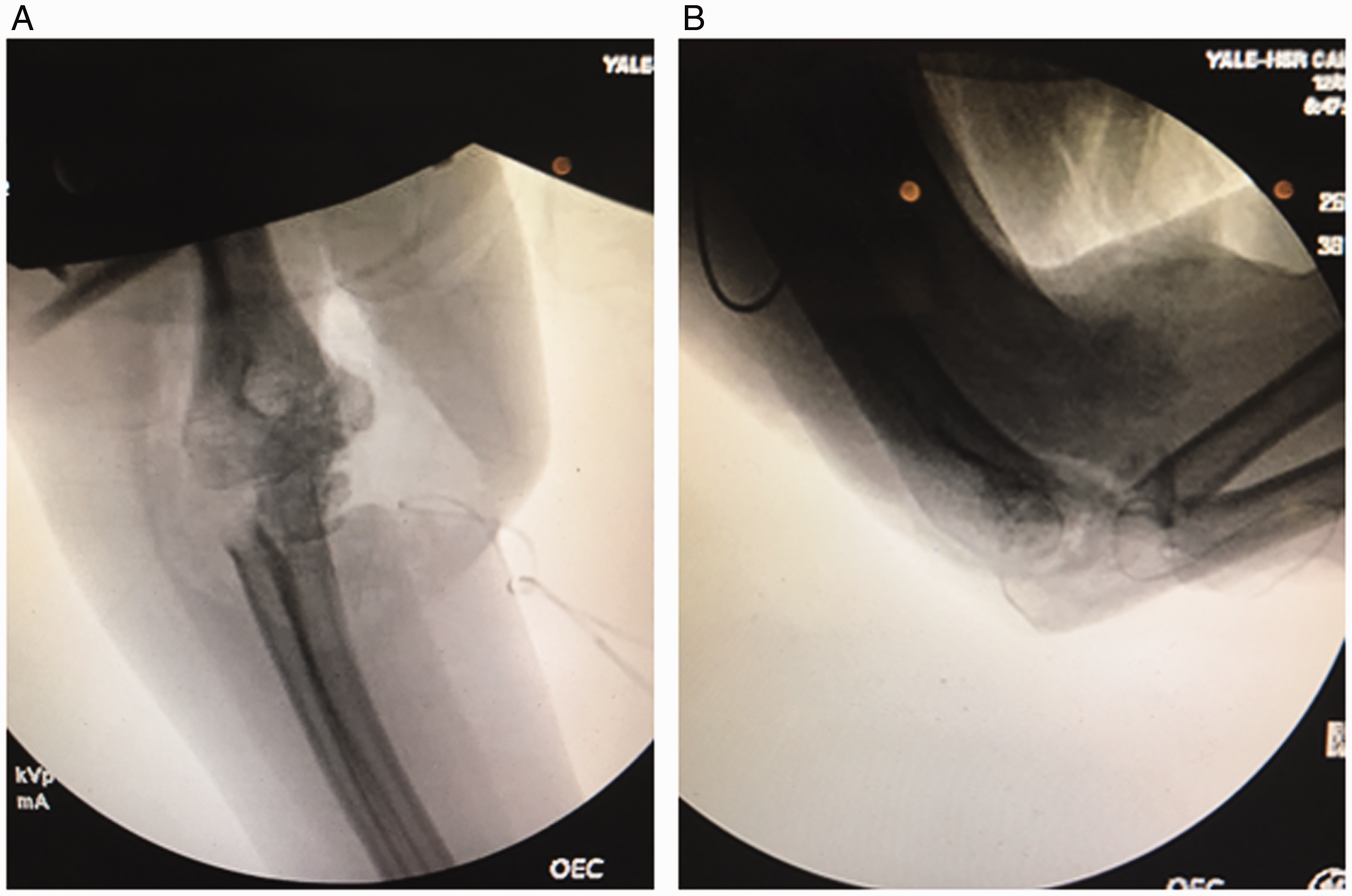
Fluoroscopic imaging in operating room showing adequate reduction at 6 weeks postoperatively in both (A) lateral and (B) AP views.

Showing stable arc of motion in operating room at (A) 30° and (B) 100°.
Summary
Interposition arthroplasty was initially described as early as 1804 for the treatment of tuberculous arthritis. 2 Since that time, its indications have included rheumatoid arthritis, posttraumatic arthritis, infection, ankylosis, and stiffness. Initially described as a resection arthroplasty, the procedure evolved to a limited resection with interposition of graft material. The interposition materials have included tin, zinc, silicone rubber, bovine graft, gelfoam, fascia lata graft, cutis, and most recently, Achilles tendon allograft.
Although it is difficult to compare results from different series due to varying evaluation criteria, successful results ranging from 26% to 94% have been reported, with the best results in patients with posttraumatic arthritis with stiffness and rheumatoid arthritis. Poor prognostic factors associated with this procedure include pre- and postoperative instability. Use of a hinged-distraction device to allow immediate postoperative range of motion while protecting the graft may further improve results. In those patients where postoperative instability occurs or where results deteriorate with time, stability and pain relief can be salvaged by conversion to semiconstrained total elbow arthroplasty.
Interposition arthroplasty is a reasonable treatment alternative in young, active patients who do not meet the criteria for total elbow arthroplasty. Semiconstrained total elbow arthroplasty should be performed in older, less active patients, or in patients in whom prior interposition arthroplasty no longer provides satisfactory pain relief or stability.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.