
Abstract
Using a subscapularis- and deltoid-preserving anterior approach is an option for patients undergoing reverse shoulder arthroplasty. Outcomes are better at short term than compared with the standard deltopectoral approach. Maintaining the integrity of the subscapularis tendon and preserving the deltoid muscle minimizes the need for postoperative immobilization and rehabilitation, allowing the patient to achieve active shoulder range of motion more rapidly, without increasing the incidence of shoulder dislocation. Overall length of hospital stay and duration of postoperative physical therapy are minimized, leading to significant economic gain. Future studies with longer follow-up are required to document the potential long-term benefits of this surgical technique.
Keywords
Introduction
Reverse shoulder arthroplasty (RSA) can be performed through several approaches, the deltopectoral and superolateral being the most common, each with their advantages and disadvantages. The deltopectoral approach that tenotomizes the subscapularis or osteotomizes the lesser tuberosity allows for increased visibility and accessibility of the humerus, better positioning of the glenoid component, reduced implant loosening, and scapular notching. 1 However, this approach is associated with a higher risk of instabilty, therefore, to decrease this risk surgeons may place in reverse in tight, over-tensioning the deltoid, 2 and potentially increasing the risk of a neurological injury. 3 Furthermore, although the subscapularis tendon is often repaired after the tenotomy, the healing, integrity, and hence function of this structure may be compromised.4–8 Subsequent subscapularis insufficiency may be a cause for poor outcomes5,9,10 and failure of shoulder arthroplasty. 11 This has led surgeons to consider surgical options to avoid detaching the subscapularis during the procedure or improve its healing postoperatively. An alternative technique is the superolateral approach that has the main advantage of better postoperative stability, because the anterior structures, including ligament complexes, are preserved. 12 Although this technique has shown good results, it involves splitting of the deltoid muscle with the risk of weakening of the anterior deltoid (mechanical or neurologic by damage to the distal branches of axillary nerve) 2 and improper postoperative function. 13
Subscapular-sparing approaches for anatomic total shoulder arthroplasties (TSAs) have been performed.14,15 Potential advantages of performing a TSA through the rotator interval include improved subscapularis function and accelerated postoperative rehabilitation. Early results show that patients who do not undergo subscapularis tenotomy have favorable clinical outcomes. 16
The aim of this article is to present the surgical technique and to review the advantages, disadvantages, and short-term results of the subscapularis-on approach with preservation of the deltoid for RSA.
Methods
Surgical Technique
Indication for subscapularis-on approach was all types of primary RSA with an intact subscapularis. The patient lies in the beach chair position with a 60° tilt of the chest, at the lateral side of the table, leaving the anterior and posterior sides of the shoulder free from obstruction. The elbow must be free of any support to enable the operating assistant to apply a proximally directed force at the elbow to allow proximal subluxation of the humeral head. The forearm rests on an armrest and is draped free. The skin incision extends from the tip of the coracoid process and runs along the axis of the arm. A deltopectoral approach is performed. 17 After further excision of the bursa, the surgeon explores the cuff. If an intact subscapularis is confirmed (Figure 1), deep dissection is carried out either through the supraspinatus tear or after detaching it. With the arm held in extension and adduction, 2 long blunt-tipped Hohmann retractors are placed around the humeral head, allowing clear exposure of the proximal humerus (Figure 2). The humerus is prepared to accommodate a short curved anatomical 132.5° stem with 20° of retroversion (Figure 3).18–20 A retroversion guide is placed, the level of the osteotomy is marked on the humeral head with an electrocoagulation device, and a free-hand osteotomy is performed. The humeral head osteotomy should be generous to allow optimal exposure of the glenoid. The humeral shaft is then prepared with compactors only (Figure 4). If the initial osteotomy is too shallow or the inclination is suboptimal, it is then revised to maximize the anatomic fit between the prosthesis and the bone. After preparing the humerus, a trial humeral prosthesis is inserted to protect the humeral epiphysis during the time of glenoid preparation. Cartilage removal, labrum resection, and peripheral capsular release are then completed. Tight inferior glenohumeral ligaments, which may prevent adequate exposure of the glenoid or postoperative shoulder mobility, are released with an electrocautery while maintaining contact with the bony rim. A forked retractor is inserted inferiorly to maintain visualization and accessibility to the glenoid (Figure 5). This presses the humeral epiphysis inferiorly, which is protected by its trial prosthesis. The glenoid is prepared according to the recommended surgical technique to obtain neutral inclination and version. Preoperative planning software is used to determine the amount of inferior tilt and whether an augmented baseplate is required. The baseplate is secured onto the glenoid with nonlocking and locking peripheral screws. A 2-mm eccentric 36-mm glenosphere is used to limit impingement in adduction, extension, and external rotation. 21 The authors do not recommend implanting a larger glenosphere as the excess lateralization may hinder access to the humerus. The glenosphere is impacted into the baseplate via a Morse taper and secured with a locking screw. Once the glenoid implant is in place, the surgeon subluxates the humerus superiorly and anteriorly. A stem with an inclination of 132.5° is combined with a 12.5° angled polyethylene (PE) insert to achieve a final 145° construct. This modular stem can be combined with either a concentric or eccentric (1.5 mm or 3.5 mm) humeral tray. The eccentric inferomedial position of the tray is always used to limit arm lengthening and to maximize lateralization. 22 The shoulder is reduced via gentle traction on the arm and range of motion (ROM) tested in all planes to ensure stability and that the prosthesis moves easily without impingement. The prothesis is then dislocated and a definitive PE is impacted. Osteophytes are removed and lateral tuberoplasty performed to maximize flexibility and avoid bony impingement. After skin closure, the surgical incision measures about 7 to 10 cm (Figure 6).

Lateral view of a left shoulder. A long broad-tipped Hohmann retractor is placed on the coracoid process superiorly. Brown-Deltoid and Langenbeck retractors, placed posteriorly and medially, respectively, retracts the deltoid and the conjoint tendon. This allows confirmation of an intact subscapularis. Reproduced with permission from Lädermann A, Lo EY, Schwitzguebel AJ, Yates E. Subscapularis and deltoid preserving anterior approach for reverse shoulder arthroplasty. Orthop Traumatol Surg Res. 2016;102(7):905–908.

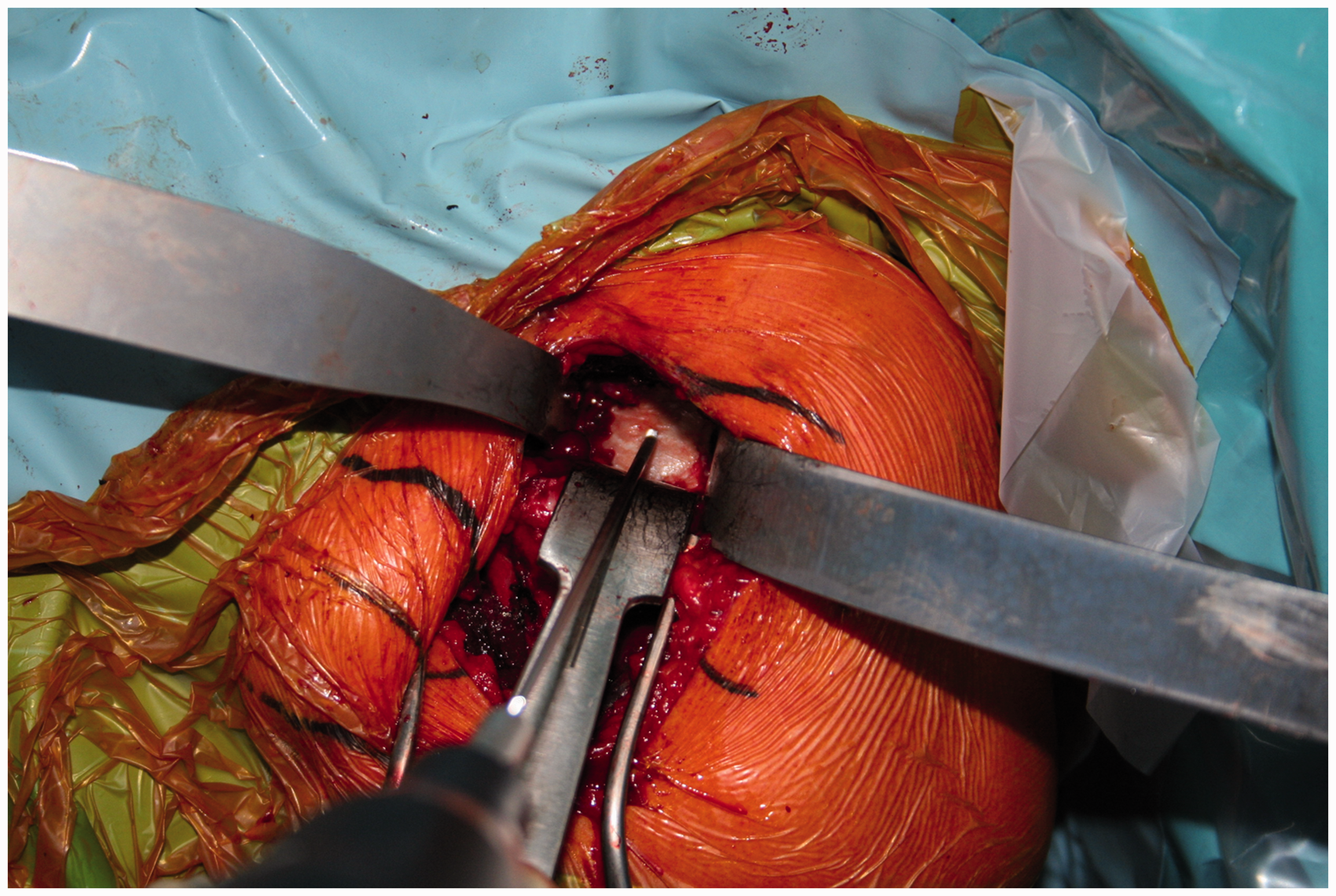
With the arm held in extension and adduction, 2 long broad-tipped Hohmann retractors are placed around the humeral head, retracting the subscapularis and the remnant posterior rotator cuff, allowing clear exposure of the humeral head. Reproduced with permission from Lädermann A, Lo EY, Schwitzguebel AJ, Yates E. Subscapularis and deltoid preserving anterior approach for reverse shoulder arthroplasty. Orthop Traumatol Surg Res. 2016;102(7):905–908.

A 20° retroversion guide is placed and the level of the osteotomy is marked on the humeral head with an electrocoagulation device. Reproduced with permission from Lädermann A, Lo EY, Schwitzguebel AJ, Yates E. Subscapularis and deltoid preserving anterior approach for reverse shoulder arthroplasty. Orthop Traumatol Surg Res. 2016;102(7):905–908.

Following humeral head removal, preparation of the humeral shaft is completed using only compactors. Reproduced with permission from Lädermann A, Lo EY, Schwitzguebel AJ, Yates E. Subscapularis and deltoid preserving anterior approach for reverse shoulder arthroplasty. Orthop Traumatol Surg Res. 2016;102(7):905–908.
A forked retractor is placed inferior to the glenoid to maintain visualization and accessibility. The glenoid is prepared according to the recommended surgical technique to obtain neutral inclination and version. Reproduced with permission from Lädermann A, Lo EY, Schwitzguebel AJ, Yates E. Subscapularis and deltoid preserving anterior approach for reverse shoulder arthroplasty. Orthop Traumatol Surg Res. 2016;102(7):905–908.

Length of the surgical incision (8 cm in this particular case). Reproduced with permission from Lädermann A, Lo EY, Schwitzguebel AJ, Yates E. Subscapularis and deltoid preserving anterior approach for reverse shoulder arthroplasty. Orthop Traumatol Surg Res. 2016;102(7):905–908.
Postoperative Rehabilitation
By using this subscapularis-sparing technique, patients do not require any immobilization with a sling following the operation. We allow immediate active motion in all planes postoperatively.
Results
One surgeon (AL) performed 65 subscapularis-on RSA from August 2013 to June 2017. The cohort consisted of 17 men and 48 women with a mean age of 76 ± 8 years. The constant score improved from 45.6 ± 14.5 points at baseline to 74.7 ± 14.8 points at 1-year follow-up.
Complications
There were 3 tuberosity avulsions that require suture cerclage. All of them healed without malunion (Figure 7), but 1 case developed a stem subsidence that did not require revision. One patient suffered from axillary nerve palsy that maybe due to insufficient removal of the inferior humeral osteophytes (Figure 8). 23 The nerve palsy completely resolved after 1 year. This complication could also be due to arm lengthening, which is contributed by implant design and the necessity of retensioning the deltoid in order to obtain better postoperative function 24 and stability. 25 Maintaining the integrity of the subscapularis improves stability, prevents excessive lengthening of the arm, and protects the axillary nerve from traction injuries during the procedure, which may be why only 1 neurological lesion and no dislocations have been observed. Four stress fractures of the scapular spine have also been recorded, although no direct relationship with the approach could be established. Finally, we did not observe any infections. Preservation of the rotator cuff, which limits the subacromial dead space, may explain the absence of infection in this series of patients.

A, Example of tuberosity avulsions (black arrows) requiring 3 suture cerclages. B, Observe tuberosity healing at 2-year postoperative.

Postoperative X-ray of a patient suffering from right axillary nerve palsy after RSA. Note mistakes at the beginning of experience: (1) superior tilt of the glenosphere and (2) neglected inferior humeral osteophyte. Consequent humeral lowering associated with nerve impingement by the osteophyte during its course around the humerus may explain the neuropathy.
Discussion
Standard techniques for RSA typically involves dividing muscles or tendons in order to maximize visualization or accessibility to the glenohumeral joint.12,17 There is growing interest for a subscapularis-sparing approach for TSA and RSA. This article summarizes the experience of 1 surgeon for this less invasive technique for RSA in patients with an intact subscapularis tendon that does not require violating the deltoid muscle. This technique has changed our daily practice, as there are obvious short-term benefits. Lädermann et al. found that utilization of the subscapularis-on approach compared to a current standard deltopectoral approach for RSA results in decreased length of hospitalization and improved short-term pain scores and function and treatment costs. 26
The economic savings determined by Lädermann et al. 26 are directly related to the length of stay. Nevertheless, this may vary with different geographical locations and health-care systems. As we encourage our patients to move freely and actively after nerve block levee, they rapidly regain independence in their daily activities. Post-acute care or transfer to a rehabilitation center is unnecessary, and physical therapy may be minimized or avoided entirely. By decreasing length of stay, this surgical approach may also help to lower hospital-acquired infection rates, 27 decrease risk factors for readmission, 28 and improve patient satisfaction. 29
With a subscapularis-on approach, immobilization may be avoided since there is no need to wait for healing of the subscapularis repair. This early mobilization likely accounts for our superior clinical results at the short term. 26 One could argue that the limited surgical exposure may prevent adequate capsular release and reduce postoperative ROM. Nevertheless, this concern was not observed in our series. Other studies analyzing results of TSA performed with a subscapularis-sparing approach also confirm our impression. The superior function at 3 months is, however, not evident at 1 year. 26 As with recent reports of subscapularis-sparing approaches for TSA, 16 long-term clinical and radiological follow-ups are required.
Another relevant finding is the low rate of short-term complications, which is about 20% in traditional deltopectoral approaches.30–32 In the present series, the rate of short-term complications is 12%.
Advantages of Subscapularis-On Approach
There are several reasons why the integrity of the subscapularis tendon during the surgery should be maintained when performing a RSA. First, acute muscle lengthening related to the nonanatomic design of the prosthesis plays a role. The muscle lengthening occurs mainly in the supraspinatus (19 mm with a bony increased offset implant), followed by the upper part of the subscapularis. 22 Muscle lengthening could theoretically make reinsertion of the subscapularis more challenging, particularly with lateral offset designs. Second, the inferior part of the subscapularis has no tendon macroscopically; the muscle attaches directly to the bone, making reinsertion difficult. Third, the subscapularis is described as being the largest muscle in the rotator cuff and stronger (53% of global strength of the rotator cuff) than the supraspinatus, infraspinatus, and teres minor combined. 33 If a muscle has to be divided, it seems logical to sacrifice the supraspinatus that accounts for only 14% of the global strength. 33 Fourth, the subscapularis plays a crucial role in anterior elevation. Collin et al. previously demonstrated that the subscapularis is the most important rotator cuff muscle for elevation in native shoulders. 34 Although the RSA design partially changes the role of the subscapularis, an intact inferior subscapularis assures the joint protection necessary for ROM 35 and the superior subscapularis provides a positive vector force and functions as an abductor. 36 Fifth, although this is still debated in the literature, 37 subscapularis muscle is important for postoperative stability,38–41 at least in Medial Glenoid/Medial Humerus designs. Sixth, preservation of the subscapularis improves internal rotation. 42 A deficit in internal rotation is common after RSA, and lack of healing of the subscapularis may partially account for this deficit.37,42 Seventh and lastly, subscapularis preservation allows for immediate ROM. Immobilization has been associated with increased shoulder stiffness. 43 Postoperative immobilization following shoulder arthroplasty is designed to balance the optimization of healing and prevention of stiffness. A 6-week period of immobilization is typically used to allow the healing to progress through the normal phases of inflammation, proliferation, and remodeling. 44 After subscapularis repair in anatomic total shoulder arthroplasty, 4 weeks of immobilization compared with immediate motion leads to higher healing rates. 5 With a subscapularis-sparing approach, immobilization is avoided, as there is no need to obtain subscapularis healing. This early mobilization likely explains our superior short-term clinical results. 26
Disdvantages of Subscapularis-On Approach
The main disadvantage of the subscapularis-on technique is limited surgical exposure. Even if specialized instruments were not required for the above mentioned technique, the development of specifically designed instrumentation for this procedure seems necessary. Moreover, limited exposure prevents the use of patient-specific surgical guides. Development of less invasive guides or navigation systems may become inevitable in the future. Even if good exposure of the humeral head is achieved, the free-hand humeral osteotomy can be problematic. In a study, Lädermann et al. compared the deltopectoral to deltoid-splitting approaches. The latter was associated with a deeper osteotomy (10 mm, P < .001) to obtain glenoid exposure. 2 Bony resection has to achieve a neck shaft angle of 145° or 135° and to allow for adequate removal of inferior humeral osteophytes. We recognize that subscapularis-on approach is technically challenging in certain cases (eg, stiff shoulders, small patients) and may not be practical or possible in all circumstances. This is not a major problem as subscapularis tenotomy or lesser tuberosity osteotomy can be performed at any time. Furthermore, the design of the prosthesis used is crucial. We implanted a small curved stem that lateralizes the humerus. 22 Intraoperatively, this prevents us from lateralizing too much the glenoid, as you would then be unable to expose the humerus sufficiently to implant the stem. Nevertheless, using 42-mm glenosphere, bony or metallic increased-offset RSA, and aiming inferior tilt with this technique is possible even of more problematic (Figure 9 and Movie 1). This also indicates that the surgeon must make a free-hand osteotomy of the humeral head, which may necessitate a second cut. This surgical technique does not allow significant glenoid lateralization seen in Lateral Glenoid/Medial Humerus design implants. 45 The baseplate used by the authors already incorporates 2 mm of lateralization; any more could prevent adequate humeral exposure and predispose to iatrogenic tuberosity fractures due to excessive traction on the anterior and posterior rotator cuff muscles. Nevertheless, the prevalence of such fractures is comparable to the rate of “controlled fractures” of the lesser tuberosity in deltopectoral approaches during posterior dislocation of the humeral head. Finally, damage to the anterior deltoid muscle could be a problem. In case of doubt, a slight abduction of the arm is applied to relieve tension, while the deltoid is protected by a sponge and larger retractors such as Brown retractors are used.

Postoperative X-rays after left RSA with subscapularis- and deltoid-preserving anterior approach. Inferior tilt (A) and left glenoid reconstruction (B) with a 15° full wedge baseplate (Aequalis™ PerFORM+ Reversed, Wright Medical Wright Medical, Bloomington, MN, USA) for superior glenoid erosion.

Illustration of a right subscapularis-on RSA with superior glenoid erosion.
We acknowledge that there are many limitations to this technique. Despite being more technically challenging, we now use this approach for all our patients who have an intact subscapularis intraoperatively. Few specific complications have been noted, and there are numerous theoretical benefits of this approach.
Conclusion
Using a subscapularis- and deltoid-preserving anterior approach is an option for patients undergoing RSA. At short-term follow-up, outcomes seem better than that after the standard deltopectoral approach. Leaving the subscapularis tendon intact and preserving the deltoid muscle minimizes the need for immediate postoperative immobilization and rehabilitation, allowing the patient to achieve active shoulder ROM more rapidly, without increasing the incidence of shoulder dislocation. Postoperative physical therapy is reduced, leading to significant long-term economic gain. Future studies with longer follow-up are required to document the potential long-term benefits of this surgical technique. Less invasive systems such as augmented reality devices or navigation may be useful.
Supplemental Material
sj-vid-1-sea-10.1177 2471549218808818 - Supplemental material for Subscapularis-On Approach in Reverse Shoulder Arthroplasty
Supplemental material, sj-vid-1-sea-10.1177 2471549218808818 for Subscapularis-On Approach in Reverse Shoulder Arthroplasty by Alexandre Lädermann, Eileen Tay and Markus Scheibel in Journal of Shoulder and Elbow Arthroplasty
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AL is a paid consultant from Wright, Arthrex, and Medacta. ET: This author, their immediate family, and any research foundation with which they are affiliated did not receive any financial payments or other benefits from any commercial entity related to the subject of this article. MS is a paid consultant from Wright, Arthrex, Exactech, Storz, and Medacta.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material is available for this article online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.