
Abstract
Introduction
Interscalene regional anesthesia is effective for pain management but is not without complications. To determine whether postoperative neurologic findings were related to the surgery versus the regional catheter, we developed the dry catheter technique where patients could be examined after the surgery prior to dosing the catheter. The purpose of the study was to assess the utility of the dry catheter block in recognizing neurological deficits associated with regional anesthesia.
Methods
An interscalene catheter was placed but not started. After the surgery, a neurovascular examination was performed. If the examination was normal, the regional anesthesia was started. Throughout the patient’s hospitalization, pain levels were collected.
Results
A total of 125 shoulders were studied. There were 9 postoperative nerve-related complications. The patients experienced the most pain relief in the first 12 hours.
Conclusion
The dry catheter technique allows differentiation between complications associated with regional anesthesia versus those associated with the surgery. Although interscalene anesthesia provided effective pain control, we stopped using it because we felt its complication rate was too high.
Introduction
Adequate pain control after total shoulder arthroplasty (TSA) is important because it allows for improved early range of motion, faster recovery, decreased morbidity, and improved patient satisfaction.1–4 The effect of a prolonged delay in pain management for patients can result in multiple postoperative complications, including activating the physiological stress response, immobility, deep vein thrombosis, delay of discharge, and decreased patient satisfaction.2,4 Furthermore, these complications may be amplified in the patient with a history of chronic pain and narcotic dependence.5,6
Brachial plexus block using an interscalene approach with a peripheral nerve catheter for acute perioperative pain management has been a standard protocol at our institution. However, interscalene regional anesthesia is not without complications and is associated with a complication rate of up to 11.2%.7,8 A dry catheter regional anesthesia technique was developed because the clinicians had observed neurologic sequelae following TSA under general endotracheal anesthesia combined with interscalene regional anesthesia. It was difficult to determine whether these neurologic findings were related to the surgical procedure or were related to the regional catheter anesthetic procedure or a combination of both. To delineate whether the neurological deficits were caused by the regional anesthesia or the surgical procedure, we developed the dry catheter technique so that patients could be examined just after the surgical procedure in the recovery room prior to dosing the regional catheter. Our hypothesis was that a dry catheter anesthesia technique would help us understand the cause of the postoperative neurologic complications, and that it would also provide adequate postoperative pain control despite not being dosed until after neurological examination in the recovery room. Therefore, the purpose of this study was to assess the utility of a preoperative dry catheter block in recognizing early neurological deficits associated independently with interscalene blocks and/or surgical procedures as well as to characterize the postoperative pain control the patient received when using an interscalene regional anesthesia technique.
Material and Methods
Study Design
The study was approved by our institution’s institutional review board committee. This is a retrospective case review of a new dry catheter technique to assess postoperative neurologic complications and patient pain control. Study participants included 125 consecutive patients who received interscalene regional anesthesia after undergoing a shoulder arthroplasty between September 2011 and January 2014. Exclusion criteria consisted of patients under the age of 18, non-English speakers, and patients with cognitive impairment.
Study Cohort
In the preoperative holding area, all patients were placed in a semirecumbent position with standard American Society of Anesthesiologists (ASA) monitors and supplemental oxygen prior to peripheral block placement. Patients were sedated with intravenous fentanyl (0.5–2 mcg/kg) and intravenous midazolam (1–50 mcg/kg) and titrated to a Ramsay Sedation Scale Score of 2 to 3. The brachial plexus was initially identified with a high-frequency linear array ultrasound transducer (SonoSite M8 Turbo, Bothell, WA) in the supraclavicular fossa, where the subclavian artery can be viewed in short axis. The transducer was moved in a cephalad fashion until the upper trunk could be identified in a stacked trifascicular pattern, and a 17-gauge Tuohy needle was then inserted and advanced through the middle scalene muscle until it was within the subepimyseal compartment. The position of the needle was confirmed using 4 to 5 mL of normal saline during the process for hydrodisection. A 19-gauge wire-reinforced catheter (FlexTip Plus, Teleflex; Arrow International, Morrisville, NC) was then advanced 1 to 2 cm past the needle tip under ultrasound guidance. No initial bolus of local anesthetic was delivered during continuous catheter placement. All patients were examined after catheter replacement prior to the surgery to confirm that all peripheral nerves were intact with no neurologic sequelae after placement of the catheter.
The patient then underwent a TSA procedure. General anesthesia was administered for the procedure with endotracheal tube, muscle relaxants, and inhalational agents. Narcotic pain medications were used as determined by the anesthesiologists taking care of the patients. Patients were extubated after the surgery and transported to the recovery room. A neurovascular examination was performed immediately in the recovery room when patients were awake and cooperative, prior to bolusing the existing peripheral nerve catheter. If it was determined that the neurovascular examination was normal, the existing peripheral nerve catheter was bolused with 10 mL of ropivacaine 0.5% in the postoperative recovery unit. Then an infusion of ropivacaine 0.2% 5 to 6 mL/h was started through the catheter, and once the patient had adequate pain control, they were discharged from the postoperative recovery unit. If the neurological examination findings after the surgery were found to be abnormal, the regional catheter was removed and the pain was managed by prescribing a patient-controlled analgesic regimen of hydromorphone as required by the individual patient. The regional anesthesia catheter was discontinued with no taper on postoperative day 1, and the patient’s pain was subsequently controlled by a combination of oral and intravenous (IV) medications. It was felt by our acute pain specialists that a continuous infusion of the ropivicaine was more effective than a single-shot block in the setting of postoperative pain control and reduced the risk of rebound. Changes to the pain regimen were conducted in conjunction with the anesthesia acute pain service in the event that the patient’s pain was not controlled. In some cases, if the patient complained of pain even with the infusion of ropivacaine, the infusion rate of ropivacaine was increased by 2 or 3 mL/h depending on the physical status of the patient up to a total infusion rate of 8 to 9 mL/h.
Data Collection
Throughout the patient’s hospitalization, the patient’s pain levels were measured on a 0 to 10 scale at regular time intervals. Pain scores were recorded every 4 hours and as needed. The average of the maximum pain scores at time intervals of 0–4, 4–8, 8–12, 12–24, 24–48, and >48 hours postoperatively was calculated in the study population. We focused on maximum pain level during these intervals because there was a large variability in the number of times the pain score was reported per patient per time interval. Calculating the mean of these pain scores would have introduced bias due to the fact that in many cases multiple pain scores were recorded minutes apart. Furthermore, it was felt that observing maximum pain score provided more insight into the patient’s overall pain experience. Complications related to the regional anesthesia were also recorded.
Results
Overall, 125 consecutive shoulders of 120 patients were included in the study. There were 46 males and 74 females with an average age of 66.29 (±10.99), body mass index of 32.85 (±6.68), and ASA score of 2.55 (±0.56). Of those, there were 69 total shoulder arthroplasties, 10 revision total shoulder arthroplasties, 28 reverse total shoulder arthroplasties, 6 revision reverse shoulder arthroplasties, 10 hemiarthroplasties, and 2 revision hemiarthroplasties (Table 1). There were 9 postoperative nerve-related complications, the most severe of which were 2 radial nerve palsies which required prolonged monitoring and therapy (Table 2). All postsurgical nerve examinations were normal in the recovery room prior to bolusing the regional catheter except for 1 patient. One patient had an immediate radial nerve palsy found in the recovery room right after the surgery, and the catheter was not bolused and immediately removed. The patient regained full motor strength of the radial nerve within 1 hour of removal of the catheter, and it was thought that this was the reason for the palsy as the patient recovered very quickly.
Case Counts.

Complication Characteristics.

Abbreviation: TSA, total shoulder arthroplasty.
The average maximum pain score of the group after the surgery and neurological examination but prior to the bolus was 6.50 (± 3.55), 0 to 4 hours postoperatively was 6.93 (± 3.2), 4 to 8 hours was 3.88 (± 3.26), 8 to 12 hours was 3.79 (± 3.27), 12 to 24 hours was 5.86 (± 2.72), 24 to 36 hours was 6.34 (± 2.46), 36 to 48 hours was 5.32 (± 2.72), and over 48 hours was 5.15 (± 2.94) (Figure 1 and Table 3).
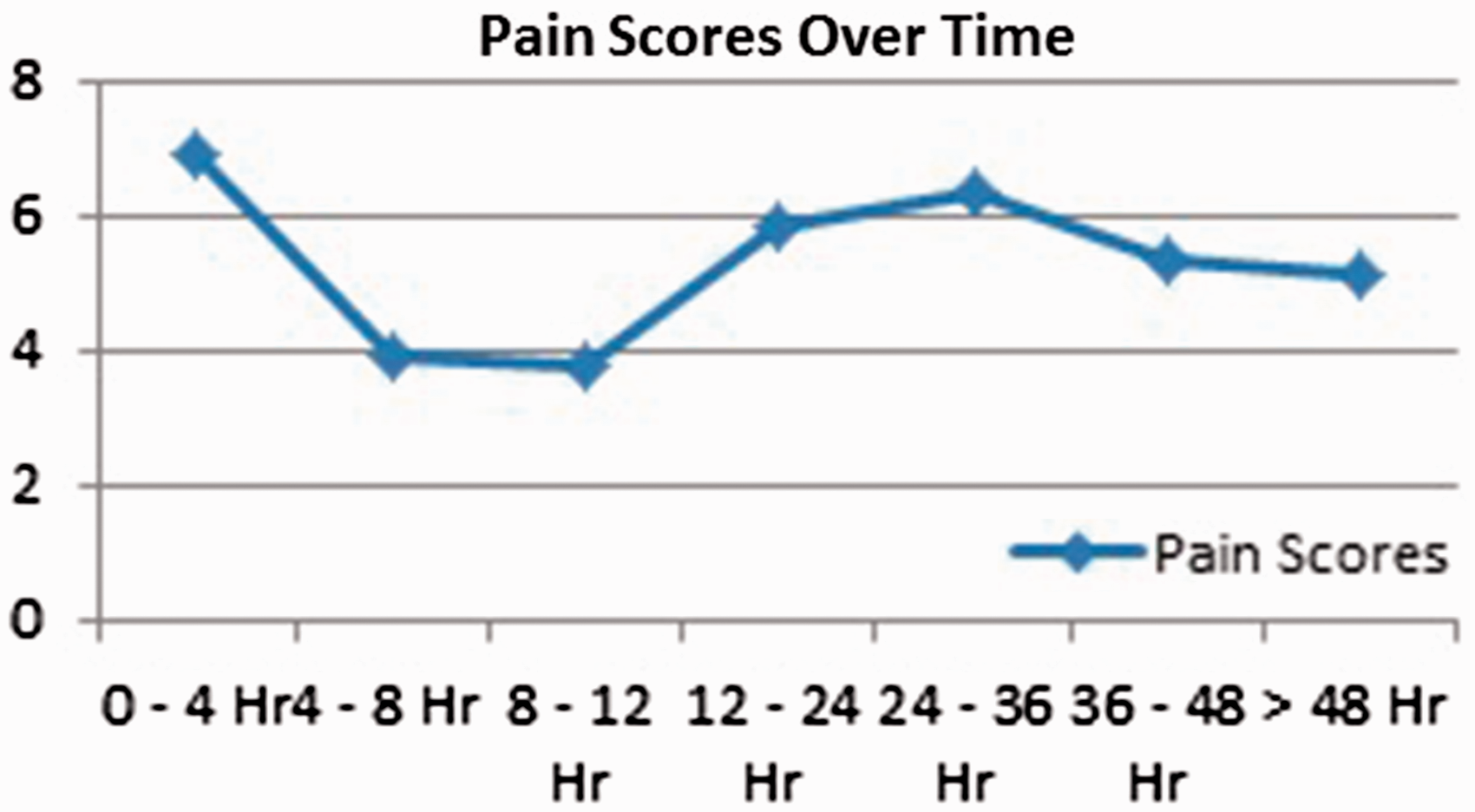
Pain Scores Over Time.
Average Maximum Pain Scores at Regular Time Intervals.

Discussion/Conclusion
Achieving adequate pain control can be a challenge in the postoperative shoulder arthroplasty patient. In our case series of patients who underwent a shoulder replacement procedure utilizing a dry catheter regional anesthesia technique, we found good postoperative pain control and the ability to determine causes of neurologic injury. Using the dry catheter proved to be a good technique for differentiating complications from the regional anesthesia versus the procedure itself. In all but one of the cases where we identified a nerve complication, we were able to document an intact nerve examination in the recovery room immediately after the surgery. In the 1 case that we identified a radial nerve palsy immediately after the surgery, prior to the bolus, the deficit quickly resolved after the regional catheter was removed. We believe that we likely prevented further injury to the radial nerve by removing the regional catheter immediately in the recovery room. Our suspicion was that the catheter shifted during the surgery and was causing irritation to the brachial plexus since the patient’s neurological examination was normal just after the catheter was placed prior to the surgery. In addition, the fact that the radial nerve palsy quickly resolved after the catheter was removed suggests that the catheter was likely the cause and less likely related to the surgery because we would not expect such a quick recovery if it was related to a neuropaxia caused by the surgery.
The patients experienced the most pain relief in the first 12 hours after the surgery while the regional anesthesia was still in place. On postoperative day 1, they began having increased pain levels, as the catheter was discontinued. The pain started decreasing 36 hours after the procedure. This is consistent with the literature that shows that interscalene regional anesthesia can provide better pain control than IV and oral pain medications alone in the postoperative period. 9 This is also demonstrated in the study by Chen et al. where they compared postoperative analgesic volume requirement in patients with and without an interscalene nerve block, and they found that the patients with the interscalene nerve block required less volume of analgesics than patient-controlled analgesia alone group in 24 hours and 48 hours. 10 Furthermore, in a study by Wu et al., they showed that patients who received regional anesthesia had a shorter recovery room stay and required less intraoperative fentanyl and morphine in the recovery room and that a higher percentage of patients who received regional anesthesia had a lower pain rating at 4 hours. 11 The rate of complications associated with interscalene regional anesthesia is not conclusive in the literature. Reported complications include peripheral nerve injuries, puncture of large vessels, and damage to the laryngeal and phrenic nerves causing stridor and hemidiaphragmic paralysis which could necessitate mechanical ventilation.12–15 However, some studies report no increase in complications after an interscalene regional anesthesia. 16 In a study by Stundner et al., they evaluated 17 157 patients, using a national database, who underwent TSA with and without the addition of regional anesthesia and did not find a significant difference in complications or intensive care unit admissions between the 2 groups. Due to the retrospective nature and the use of the national database, they were unable to compare the incidence of peripheral nerve injuries between the 2 populations. 17 In an article by Sviggum et al., they performed a retrospective cohort study at a single institution comparing the incidence of peripheral nerve injuries in patients undergoing total shoulder arthroplasties with and without interscalene regional anesthesia. In their study, they found a 2.2% incidence of peripheral nerve injuries, and there was no significant difference between the 2 groups. 18 However, in some studies, complication rates have been reported as being up to 11.2%.7,8,19 In our study, there were 9 peripheral nerve complications, consisting of 7.2% of our patients. The dry catheter technique identified that the nerve complications were related to the regional catheter as opposed to an intraoperative surgical complication. It is not clear by which mechanism the regional anesthesia caused the nerve sequelae. It is possible that the surgery itself causes the nerves to be irritated to a lower threshold so that any additional nerve insult such as small hematoma from the block technique, space occupancy of the catheter, or placement of the actual local anesthetic caused a second nerve insult to the neurologic structures and resulted in injury. Regardless of the exact mechanism of injury caused by the regional anesthesia, it was felt that the rate of complications was too high and preventable. Therefore, we have since stopped using interscalene regional anesthesia in our shoulder arthroplasty patients.
This study has a number of limitations. First, the retrospective nature of the study predisposes us to confounding variables such as inaccuracies in documentation or the fact that the patients received pain medications intraoperatively, which could have influenced their immediate postoperative pain level. Furthermore, it is possible that some of the deficits noted were secondary to late complications from the surgery (ie, postoperative hematoma). Another limitation is the fact that the procedures included were heterogeneous and included primary and revision total shoulder arthoplasties, reverse shoulder arthroplasties, and hemiarthroplasties. Last, there was no control group against which the dry catheter patients were compared, which makes it difficult to draw firm conclusions, especially regarding the efficacy of postoperative pain control with the dry catheter technique.
In conclusion, the authors feel that the dry catheter regional anesthesia technique was an effective method for differentiating complications associated with the regional anesthesia versus the surgery. Although interscalene regional anesthesia provided effective pain control in the early postoperative period, we have since stopped using this technique due to the additional risk of neurologic complications.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.