
Abstract
Background
The purpose of this study is to assess the incidence of acromial stress fractures in a population of reverse shoulder arthroplasties (RSA) and determine potential risk factors for fracture.
Patients and Methods
Between August 2004 and December 2013, 1082 primary RSA were performed at a single institution. Twelve (1.11%) patients were diagnosed with a postoperative acromial stress fracture. This group was case-matched to a control group of 48 shoulders. Clinical and radiographic risk factors for fracture were assessed.
Results
Compared to controls, fractures were less satisfied with their outcome despite equivalent American Shoulder and Elbow Surgeons scores, pain scores, and range of motion. Osteoporosis was significantly associated with acromial fractures (P = .027). A smaller lateral offset of the greater tuberosity, greater arm lengthening, and a thinner acromion were more common in the fracture group (P = .026, P = .004, and P = .008, respectively).
Conclusions
In summary, postoperative acromial stress fractures appear to be incidental lesions with little influence on the outcome after RSA. The combination of a thin acromion and superior migration of the humeral head increase the risk of acromial fracture. Lateralized designs that do not excessively verticalize the deltoid line of pull on the acromion may decrease the risk of postoperative acromial fractures.
Introduction
Acromial Fractures Previously Reported in the Literature.
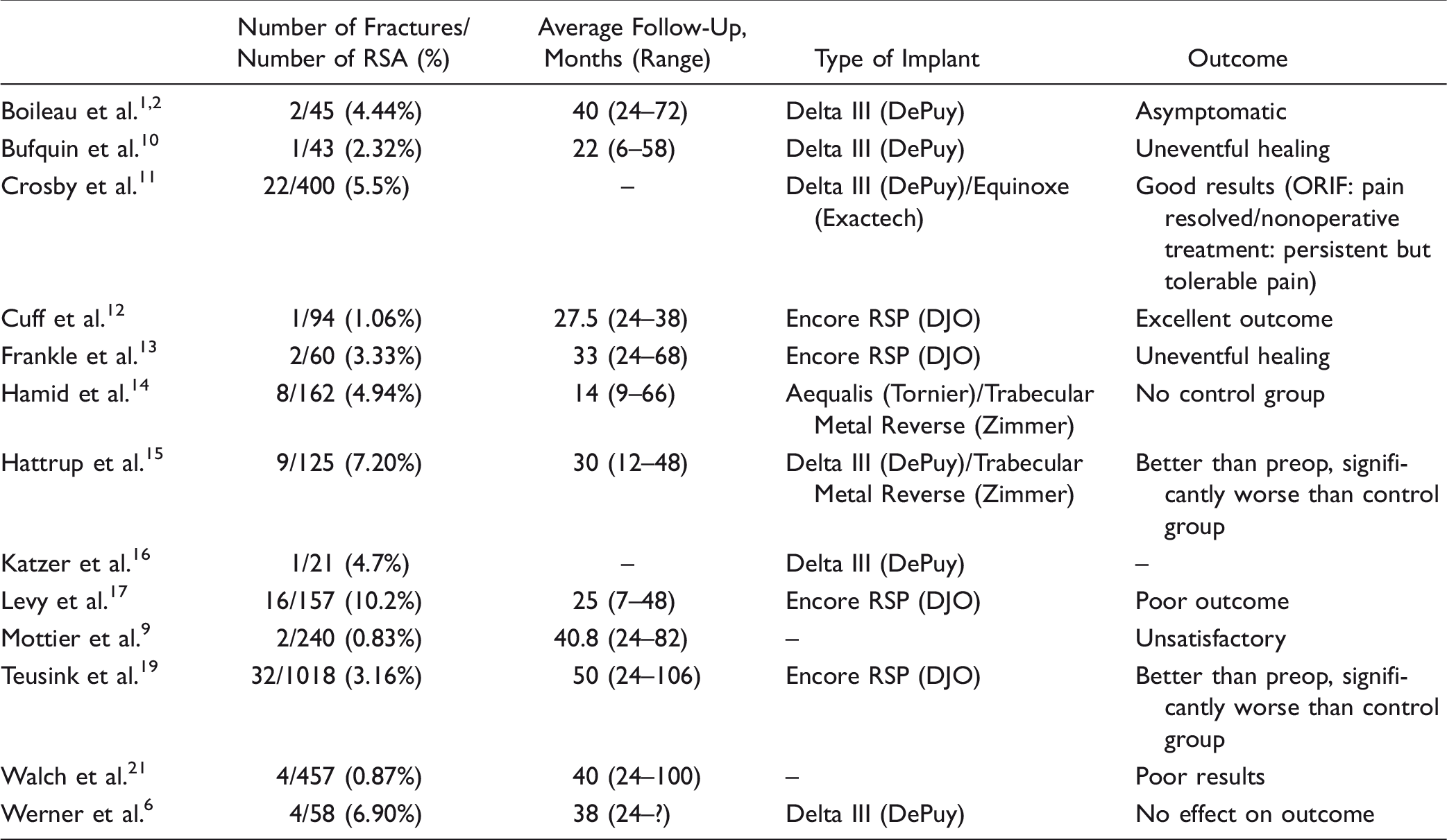
Previous reports27,19 have attempted to determine the risk factors and best therapeutic approach for this complication as well as the associated outcomes. However, the answers to these questions remain unclear. The purpose of this study is to review our institutional incidence of acromial stress fractures following RSA and to further assess potential risk factors for fracture and their associated clinical outcomes.
Materials and Methods
Patients
We retrospectively reviewed data from the Mayo Clinic Total Joint Registry that has prospectively enrolled all shoulder arthroplasties performed at our institution since 1969. 22 All patients are asked to return for an examination, interview, and radiographic evaluation at 1, 2, and 5 years’ follow-up and then every 5 years thereafter. Patients who are unable to return for evaluation are sent a standardized, validated questionnaire 28 to evaluate their function and satisfaction, with radiographs performed locally and sent for review. All complications, reoperations, and revisions are recorded in the registry.
One thousand eighty-two shoulders (1003 patients: 418 men and 585 women) who underwent primary RSA between August 2004 and December 2013 were screened for postoperative acromial fractures. The mean age at surgery was 73 years (range, 25–93). Indications for RSA included: CTA (812, 75%), sequela of trauma (132, 12%), osteoarthritis with cuff tearing (49, 5%), acute trauma (42, 4%), inflammatory arthritis (28, 2.5%), neoplasia (14, 1%), and avascular necrosis (5, 0.5%).
Twelve shoulders (12 patients) with acromial fractures were identified and had a minimum follow-up of 2 years, unless they underwent reoperation prior, in which case they were included to the point of reoperation. Patients who presented in follow-up with isolated pain over the acromial spine were further evaluated to confirm the presence of an acromial stress fracture. When radiographs did not show evidence of a fracture, a standard shoulder computed tomography scan was performed to assess for a fracture line or increased calcification representing healing of a stress fracture. A control group was created and matched for age, gender, and time to follow-up at a ratio of 4:1. A total of 48 control cases were included.
Demographic data including gender, arm dominance, age at the time of surgery, body mass index (BMI), prior procedure on the concerned shoulder (including acromioplasty), osteopenia/osteoporosis, and indication for surgery were collected for each patient.
Patients with risk factors for osteoporosis and osteopenia were assessed by dual-energy X-ray absorptiometry scanning and defined as a T score ≤ −2.5 and a T score between −1.0 and −2.5, respectively. Patients without risk factors were considered to have normal bone density.
Surgical Technique
The implants used included 710 (66%) Comprehensive Reverse (Biomet, Warsaw, IN), 250 (23%) Delta Xtend (DePuy, Warsaw, IN), 48 (4%) Aequalis (Tornier, Bloomington, MN), 46 (4%) Encore RSP (DJO, Vista, CA), and 28 (3%) Delta III (DePuy). Operative reports were reviewed to determine surgical approach (deltopectoral or superior), management of the subscapularis (tenotomy, peel, and osteotomy of the lesser tuberosity or torn), retroversion of the humeral component, fixation of the humeral component (cement or uncemented), and use of a bone graft on the glenoid.
Clinical Evaluation
Pain was graded according to scales previously published by Cofield 26 and Neer et al., 25 where 1 indicates no pain; 2, slight pain; 3, pain after unusual activity; 4, moderate pain; and 5, severe pain. Active elevation in the scapular plane and external rotation were recorded in degrees. Internal rotation was measured as the most cephalad vertebral segment reached by the thumb. Subjective satisfaction was assessed by asking the patients at follow-up how they felt compared with before surgery and was graded using a 4-point scale: 1, much better; 2, better; 3, same; and 4, worse. Global outcome was assessed using the American Shoulder and Elbow Surgeons (ASES) Standardized Shoulder Assessment form. 24
Radiological Evaluation
A standardized 40° posterior oblique view of the shoulder in external rotation in addition to an axillary view was used for radiographic analysis. Preoperative radiographs for patients who underwent RSA were reviewed to determine the presence of superior glenohumeral subluxation and acetabulization of the acromion. 8
Radiographs at the time of fracture were also reviewed. Radiographic measurements were all performed by 1 orthopedic surgeon. Fracture displacement was assessed, and fracture type was determined using the Levy classification. 17
Acromial thickness was measured at the middle and anteromedial portions of the acromion in the 2D scapular Y-view image of plain radiographs.
Four additional types of measurements were made. Immediate postoperative radiographs were reviewed to measure the distance between the acromion and the greater tuberosity (AT) and the distance from the glenoid–baseplate interface to the greater tuberosity (GT). The method earlier described by Otto et al.
27
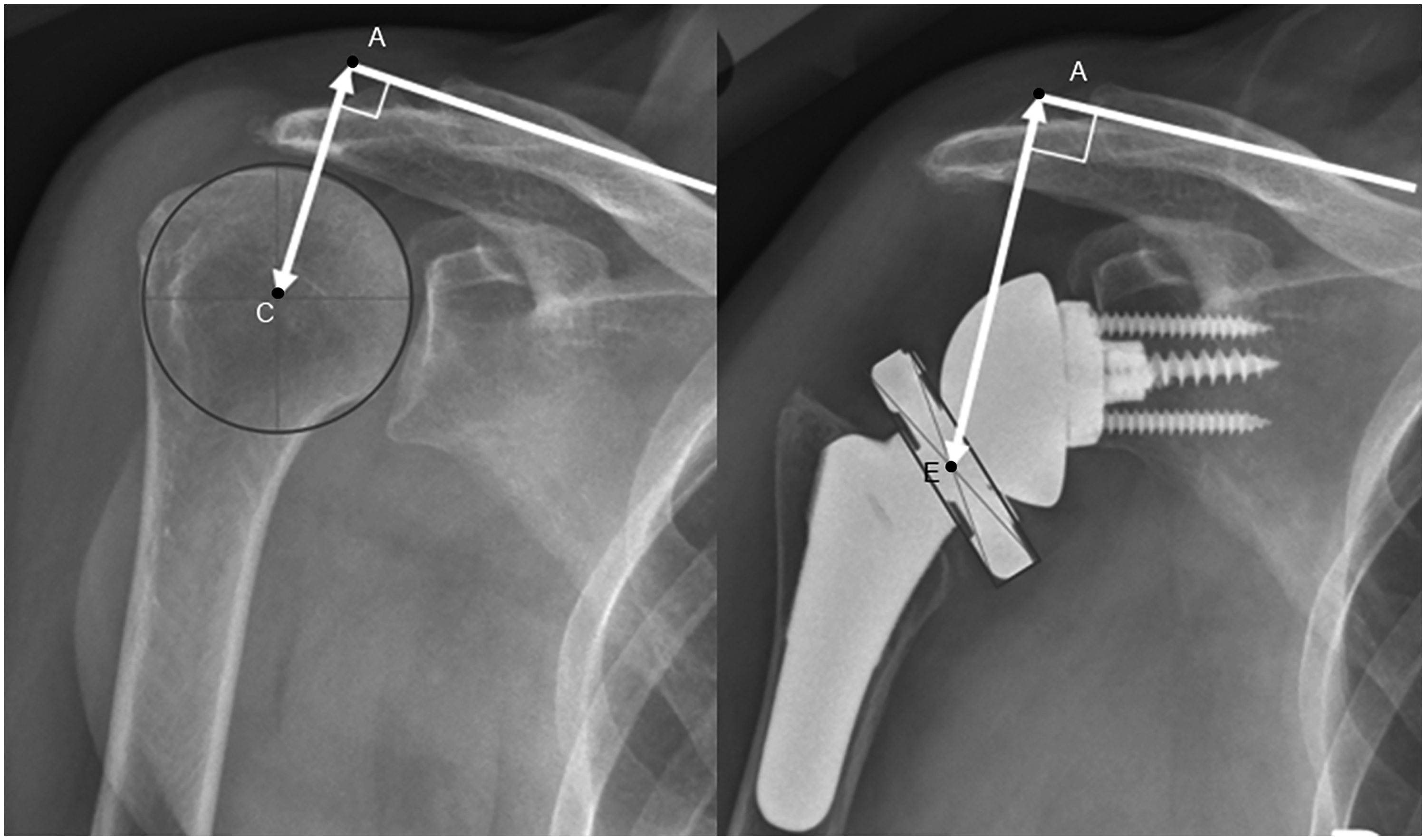
to measure GT was modified. Instead of measuring a straight line from the glenoid–baseplate interface to the greater tuberosity, the distance from the bone–implant interface to the center of rotation of the joint was added to the distance between the center of rotation to the greater tuberosity in order to get a measure independent from different arm positions (Figure 1). In this measure, the center of rotation of the joint was defined as the center of the best-fit circle around the glenosphere. Arm lengthening was measured perpendicular from the superior cortex of the base of the acromion to the center of rotation of the humeral head in preoperative images and to the center of the prosthetic epiphysis of the humeral component in postoperative images as described by Renaud et al.
29
(Figure 2).
Measurement of the distance from the glenoid–baseplate interface (I) to the greater tuberosity (GT). The method earlier described by Otto et al.
27
to measure GT was modified. Instead of measuring a straight line from the glenoid–baseplate interface to the greater tuberosity, the distance from the bone–implant interface to the center of rotation of the joint (C) was added to the distance between the center of rotation to the greater tuberosity in order to get a measure independent from different arm positions. Postoperative AP radiographs of the shoulder of 2 different patients. Arm lengthening was calculated as the difference of lengths measured perpendicular from the superior cortex of the base of the acromion (A) to the center of rotation of the humeral head (C) in preoperative images (left) and to the center of the prosthetic epiphysis of the humeral component (E) in postoperative images (right) as described by Renaud et al.
29

Statistical Analysis
Descriptive statistics are described as mean (range) for continuous measures and number (percentage) for discrete variables. For the clinical outcome, pre- versus postoperative changes in pain and range of motion (ROM) were assessed using a paired t test. Comparison of the clinical outcome in control versus fracture group was likewise done using a Wilcoxon rank-sum test. Significant differences among the characteristics of the study population were estimated using a Cox-regression analysis. The alpha level for all tests was set at .05 for statistical significance.
Results
Study Population Characteristics
Among the 1082 shoulders which underwent RSA between August 2004 and December 2013, 12 (1.11%) sustained a postoperative acromial fracture. The mean duration of follow-up was 2.2 years (range, 0–7 years). All 12 patients who sustained a postoperative acromial fracture had undergone RSA for CTA. Only 1 of the 12 fractures had a history of direct trauma, while the 11 others were considered stress fractures. The mean time from surgery to fracture diagnosis was 9 months (range, 2–38 months). Five (42%) occurred less than 3 months after surgery, 3 (25%) from 3 to 6 months after surgery, 1 (8%) from 6 to 12 months, 1 (8%) between 1 and 2 years, and 2 (17%) occurred greater than 2 years postoperatively. According to the Levy classification, 17 9 (75%) fractures were type I, and 3 (25%) were type II. Four (33%) of the fractures were displaced. All the fractures were initially treated nonoperatively with sling immobilization. Average follow-up after the fracture was 35 months (range, 13–67 months).
Risk Factors
As patients had been matched for age and gender, these were not analyzed as risk factors. However, the mean age of the fracture group (71.5 years, range: 53–83) was comparable (P = .7) to the mean age of the RSA cohort (72.7 years, range: 25–93) while there were more women in the fracture group (75%) than in the RSA cohort (60%) (P = .3).
In the univariate analysis, variations in BMI and arm dominance were not significantly associated with postoperative scapular fractures (P = .1 and .6). Osteoporosis was significantly associated with a higher risk of acromial fracture (46% vs 12%, P = .027; HR of 3.78 [1.17, 12.19]).
Surgical Parameters
Repartition of the Different Implants in the Whole Cohort and in the Fracture Group.

Demographic and Operative Data.
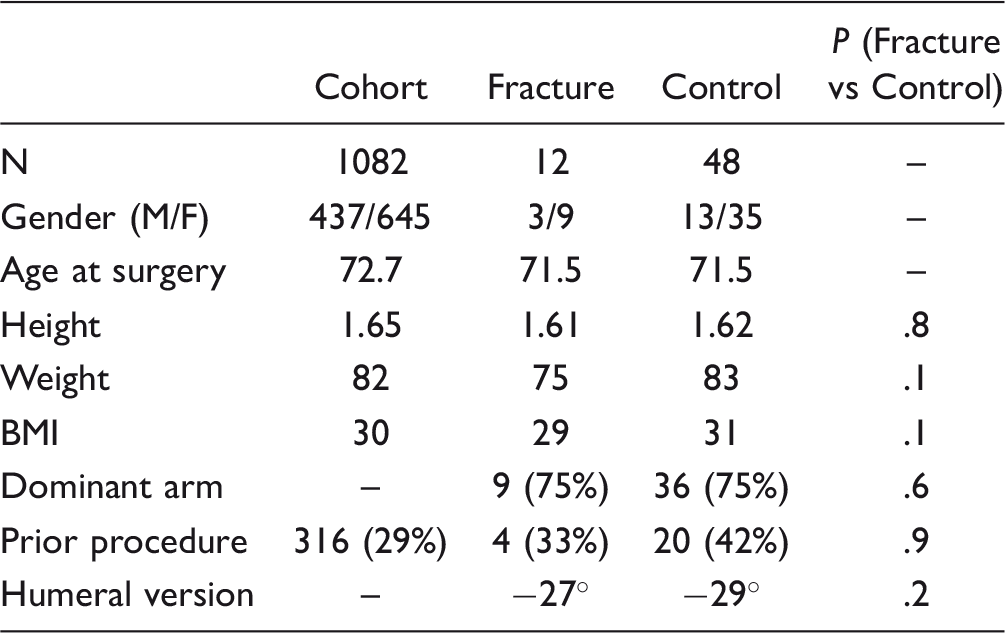
Abbreviation: BMI, body mass index.
Treatment
Treatment of the acromial fracture was decided by the surgeon and was not standardized. Four patients were treated with an abduction pillow sling for 6 weeks, 6 received a simple sling (4 for 1 month, 1 for 2 weeks, and 1 for 1 week), and 2 were treated with activity modification. Patients were recommended to avoid active shoulder ROM. They were not routinely placed on calcitonin or bone stimulators. Eleven of 12 fractures healed with sling wear. One displaced type II fracture that had been treated with a simple sling for 1 month ultimately underwent open reduction and internal fixation using compression screws 9 months after fracture. This was documented to heal uneventfully.
Outcome
At follow-up, pain relief was achieved in both groups. Pain scores decreased from a mean 5 (range, 4–5) preoperatively to 2 (range, 1–4) postoperatively in the fracture group (P < .0001) and from a mean 5 (range, 1–5) preoperatively to 2 (range, 1–4) postoperatively in the control group (P < .0001). There was no significant difference in ROM between the 2 groups preoperatively and postoperatively. ROM was improved in both groups. However, for the fracture group, improvements in external and internal rotation were not significantly different (P = .314 and P = .320, respectively). Clinical comparison of the 2 groups is detailed in Table 3. Nine of the 12 (75%) patients in the fracture group felt they were better or much better than preoperatively, compared with 44 (92%) of the 48 patients in the control group; however, this did not reach statistical significance (P = .602).
Clinical Data.
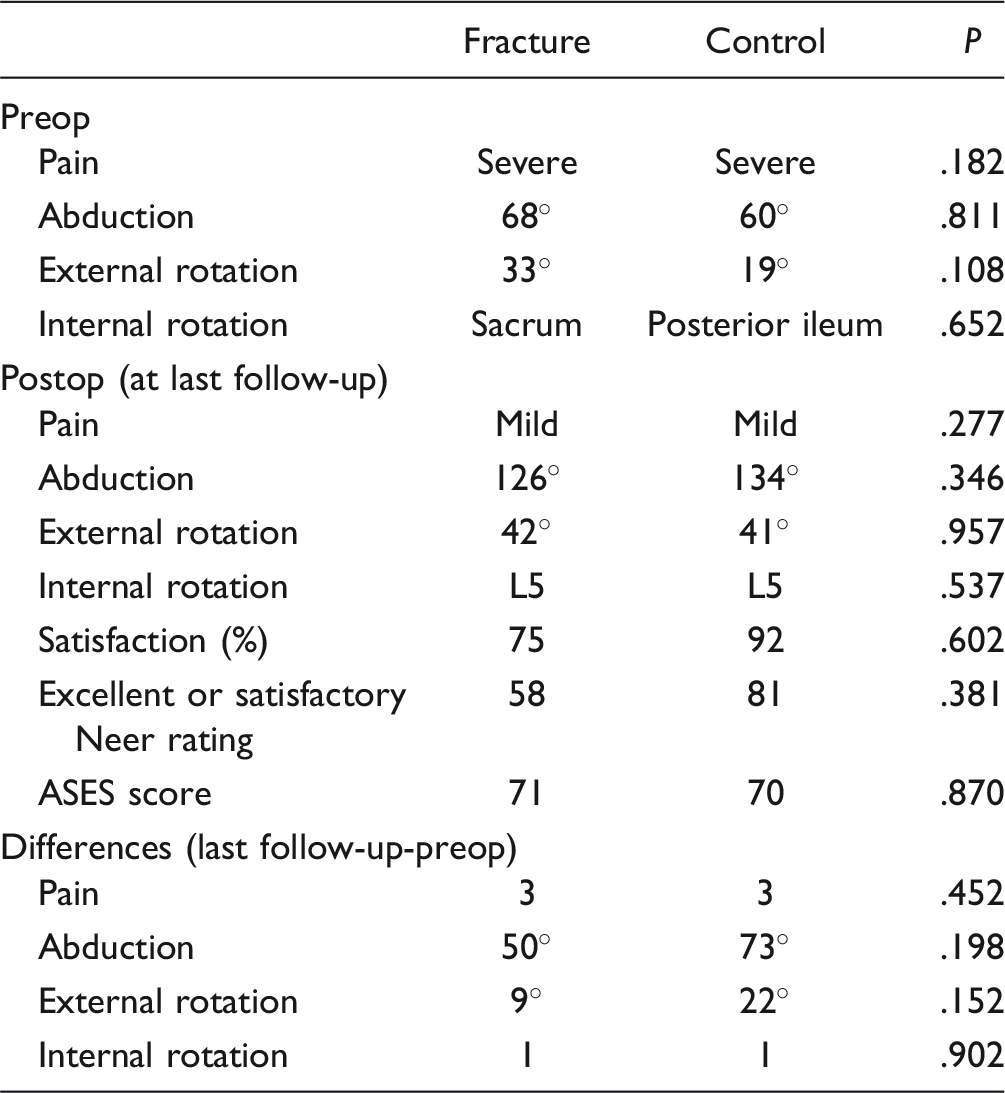
Abbreviation: ASES, American Shoulder and Elbow Surgeons.
Radiographic Evaluation
No significant difference in glenoid erosion or preoperative subluxation was identified between groups. Three (25%) patients in the fracture group had a preoperative changes of the acromion including acetabulization of the acromion, history of acromioplasty, or the presence of an os acromiale versus 5 (10%) in the control group. This difference did not reach statistical significance (P = .846).
Radiological Parameters, Dimensions in Millimeters or Degrees (± Standard Deviation).

Abbreviations: AT, distance acromion-greater tuberosity; GT, distance glenoid-greater tuberosity; LPA, line-of-pull angle. Bold face values represents the statistically significant values.
Discussion
The biomechanical design of the RSA relies on the deltoid as the primary force to move the shoulder.2,23 Any disruption of deltoid function can potentially lead to impairment of the treated shoulder. Although this complication is reported to be rare, it has reached 10.2% in certain series.6,15,17 The impact on patient outcomes remains unclear, with some authors reporting unchanged results1,2,6,10–13 and others showing a decrease in ROM and satisfaction scores after fracture.9,15,19,21 No risk factors have been clearly identified except for osteoporosis. 27 The indications for surgical fixation remain ill defined. We report a large single center consecutive series of RSA. The rate of acromial fracture in our series was 1.11%, which is at the lower end of the range previously reported. Walch et al. 21 and Mottier et al. 9 who reported the lowest rates of postoperative acromial fractures (0.87% and 0.83%, respectively), included only patients without preoperative acromial changes (fragmentation, old fracture, and os acromiale). In our series, 3 (25%) patients in the fracture group (and 5, 10%, in the control group) had preoperative acromial changes.
Risk factors in this series included: osteoporosis, acromial thickness, glenoid-to-greater tuberosity (GT) distance, and arm lengthening. Walch et al. 21 showed that preoperative acromial pathology (old fracture, nonunion, fragmentation, and os acromiale) was not a risk factor for postoperative fracture. Our results support this conclusion. Otto et al. 27 who specifically studied risk factors did not find any significant relationship between acromial thickness and postoperative fracture. This could be due to the lack of reproducibility of measurements. This was only found to be significant in the 2D Y-views in our series. The only risk factor found by Otto et al. 27 was osteoporosis, which our results support (P = .027).
Compared to controls, fractures tended to be less satisfied with their outcome (75% felt they were better or much better in the fracture group vs 92% in the control group). However, shoulders did have equivalent ASES scores, pain scores, and ROM. One patient in this series required operative fixation of a type II acromial fracture. This is in contrast to previous reports which have more commonly reported on surgical fixation for type III fractures of the acromial base.17,20
The torque force leading to arm abduction is the product of the moment arm of the deltoid times the force from the deltoid. After implantation of an RSA, the torque required to move the arm remains identical. As the center of rotation of the shoulder is medialized and lowered, the moment arm of the deltoid is increased. This decreases the deltoid force required to obtain similar movement
2
and leads to lower tension stresses on the acromion. However, excessive medialization and lowering of the humerus can have deleterious effects. Excessive lowering can lead to arm lengthening and thus increased passive tension of the deltoid on the tip of the acromion. In case of excessive medialization, a lower deltoid wrapping angle is created, leading to a more vertical pull of the deltoid on the acromion.
30
The addition of increased passive tension and a vertical line of pull from the deltoid leads to an increased bending moment applied to the acromion and potentially places the acromion at risk for fracture (Figure 3(A) to (F)).
Pre- and postoperative AP radiographs of the shoulder with 3 different types of implants, (A) and (B): Comprehensive Reverse, Biomet; (C) and (D): Encore RSP, DJO; (E) and (F): Delta Xtend, DePuy, showing differences in arm lengthening and pulling due to different designs. The center of rotation, the origin and insertion of the deltoid, and the moment arm of the deltoid are noted. Implantation of an RSA medializes the center of rotation, distalizes the humerus, and elongates the deltoid. Depending on the importance of the medialization, the greater tuberosity may be completely aligned with the tip of the acromion. In which case, the greater tuberosity cannot act anymore as a pulley of reflection of the deltoid, and its line of pull becomes almost vertical.
Excessive passive tension may explain why 11 of the 12 fractures observed in this series occurred after a minimal effort event, such as reaching a high shelf. In addition, the distribution of implants observed within the whole cohort was different from the distribution in our fracture group. Implants which had a Grammont-style design which lead to a shorter GT distance were more likely to lead to acromial fracture. A significant difference in GT distance had not been previously identified by Otto et al. 27 This may be due to the use of the Encore RSP implants in their series. This implant has a 23-mm to 27-mm lateral offset 31 and leads to high GT values in both groups (54 mm in the fracture group vs 55 mm in the control group). As many different types of implants were used in our series, greater variations in lateral offset and GT values were found among the 2 groups (48 mm in the fracture group vs 51.7 mm in the control group).
Arm lengthening was also significantly associated with acromial fractures. However, there was no significant difference in postoperative arm length. Preoperative length was significantly shorter in patients from the fracture group because they had more severe proximal migration of the humeral head. The implantation of an RSA and the subsequent correction of this superior subluxation lead to an increase in passive tension of the deltoid on the acromion which could be responsible for weakening the bone.
The main limitation of our study is the small sample size due to the rarity of this complication. The study also remains limited by its retrospective nature, despite data being captured prospectively through our institutional registry. In addition, multiple surgeons and implants were utilized. However, the utilization of multiple implants did allow us to compare designs and their association with fracture, which have not previously been examined. Some patients may have developed acromial stress fractures and did not follow up in clinic. However, patients who do not follow up in person are routinely followed through our joint registry to track their progress. Any patient with unexplained ongoing pain or worsening function was asked to come back for in person evaluation. However, it remains possible that some patients with acromial stress fractures may have been missed using this study design. The strength of this study is our use of a large cohort of patients treated by fellowship-trained shoulder surgeons. In addition, the use of a large registry also allowed us to case match patients for assessment of risk factors.
In summary, postoperative acromial fractures are rare and may lead to subjective dissatisfaction; however, this complication does not appear to affect ROM or ASES scores. The combination of a thin acromion and an excessive superior migration of the humeral head increase the risk of acromial fracture after lowering and medializing the center of rotation of the joint. Lateralized designs that do not excessively verticalize the deltoid line of pull on the acromion may decrease the risk of postoperative acromial fractures.
Footnotes
Authors’ Note
Each author certifies that his or her institution approved the human protocol for this investigation and that all investigations were conducted in conformity with ethical principles of research (IRB #4-003206).
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Robert H Cofield receives royalties for shoulder prosthesis design from Smith-Nephew. John W Sperling receives royalties from Biomet. The other authors, their immediate families, and any research foundations with which they are affiliated did not receive any financial payments or other benefits from any commercial entity related to the subject of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.