
Abstract
Background
Total shoulder arthroplasty (TSA) is the fastest growing sector of arthroplasty in the United States. One of the greatest drivers of costs following joint replacement surgery has been shown to be discharge disposition. This study examines the costs associated in the first 90 days of care following shoulder arthroplasty with a specific focus on the effects of discharge disposition.
Methods
We conducted a retrospective, case–control study of the entire Medicare population from 2011 to 2014 identifying TSA patients based on International Classification of Disease ninth revision codes. Only patients with demographic and discharge information were included. Costs were analyzed based on mean reimbursements. Patients were stratified according to 4 disposition groups: home, skilled nursing facility (SNF), intermediate care facility (ICF), and inpatient rehabilitation (InR). The correlation of the Charlson Comorbidity Index (CCI) to discharge disposition was also examined.
Results
A total of 50 979 patients met the inclusion criteria. The mean 90-day costs for patients discharged home were $12 691 (standard deviation [SD]: $471.9), for those who went to an SNF was $15 093 (SD: $622.4), for ICF $15 473 (SD: $2366) and for those who went to InR $24 731 (SD: $1922; P < .001). Over the 4-year period, trends in discharge to home significantly increased (P = .037), while trends in discharge to InR significantly decreased (P = .015). The CCI correlated significantly with discharge disposition setting (P < .001).
Conclusion
The 90-day reimbursements of TSA are significantly affected by discharge disposition. Although discharge to home continues to increase, patients with a greater comorbidity burden are discharged more often to an inpatient facility.
Introduction
Shoulder arthroplasty is the fastest growing field of arthroplasty in the United States.1,2 This growth in popularity and utilization relates to successful outcomes and an expanding population of patients with end stage arthropathy. Most recently, Day et al. projected that the volume of shoulder arthroplasty would increase between 192% and 322% from 2007 to 2015, 1 demonstrating an economic burden which will continue to increase with time.
Due to the growth of arthroplasty procedures in the recent years and the transformation towards a value driven health-care system, new payment models have been introduced aiming at decreasing costs, improving quality and decreasing complications. The model that has gained most attention is the Comprehensive Care for Joint Reconstruction (CJR) model. Introduced by Medicare in April of 2016, this model is designed to reimburse health-care providers with a fixed payment for care provided from the date of surgery up until 90 days after (specific dates may vary). Currently, shoulder arthroplasty is not included in CJR; however, similar modeling is being performed for other forms of bundled payment efforts. In examination of the 90-day cost of care, it has been shown that more than 40% of the cost occurs after discharge from the initial hospitalization.3,4 A greater understanding of the impact of the discharge disposition is needed as bundle payment plans are developed.
Previous studies have shown that disposition to locations other than home can increase the risk of postoperative complications.5,6 Certain risk factors have been identified as predictors of discharge to postacute care facilities including Medicare patients, older age, females presenting with fractures, and those with multiple medical comorbidities.3,7 Nonetheless, the cost associated with discharge disposition to one of these postacute centers has not been well studied. Improved understanding of these post-date-of-surgery costs may have an enormous impact on Medicare expenditures, the development of a risk-adjusted bundle, and patient care. The purpose of this study was to compare the 90-day costs of total shoulder arthroplasty (TSA) with a focus on discharge disposition. We hypothesized that patients discharged home the day of surgery would incur in the least costs to Medicare.
Materials and Methods
The Standard Analytical Files, which house all of the information from Medicare patients, were reviewed through the PearlDiver supercomputer (Colorado Springs, CO). This publicly available commercial supercomputer allows analysis of all Medicare files through International Classification of Disease (ICD) ninth revision codes. For this analysis the ICD code utilized was 81.80, which is representative of TSA. Patients were stratified by 1 of 4 discharge settings: home, skilled nursing facility (SNF), intermediate care facility (ICF), and inpatient rehabilitation (InR). Total Medicare reimbursements per year were extracted, and a calculation of mean cost per patient was conducted. The mean reimbursements were used for comparison of average patient cost. Length of stay (LOS) was also compared among the 4 cohorts. The Medicare files include data from 2005 to 2014. The dates chosen for analysis in this study included 2011 to 2014, as to evaluate current practice and costs. An analysis of variance was conducted.
Post hoc analysis of the analysis of variance (ANOVA) was conducted through the Bonferroni test. An alpha value of less than 0.05 was deemed as significant. Two comparisons were conducted through these methods: one for the reimbursements on the day of surgery and the second for the 90 days after. The 90-day period was selected, as this is typically the period covered by the CJR model. Trends in discharge disposition were analyzed based on data from the same study period and through linear regressions. The Charlson Comorbidity Index (CCI) was also calculated for the 4 groups in order to compare their baseline comorbidity burden. A Pearson correlation was used to determine the association of discharge disposition and the CCI. SPSS version 20 (IBM, Armonk, NY) was utilized for statistical analysis.
Results
Demographics of the Included Patients.
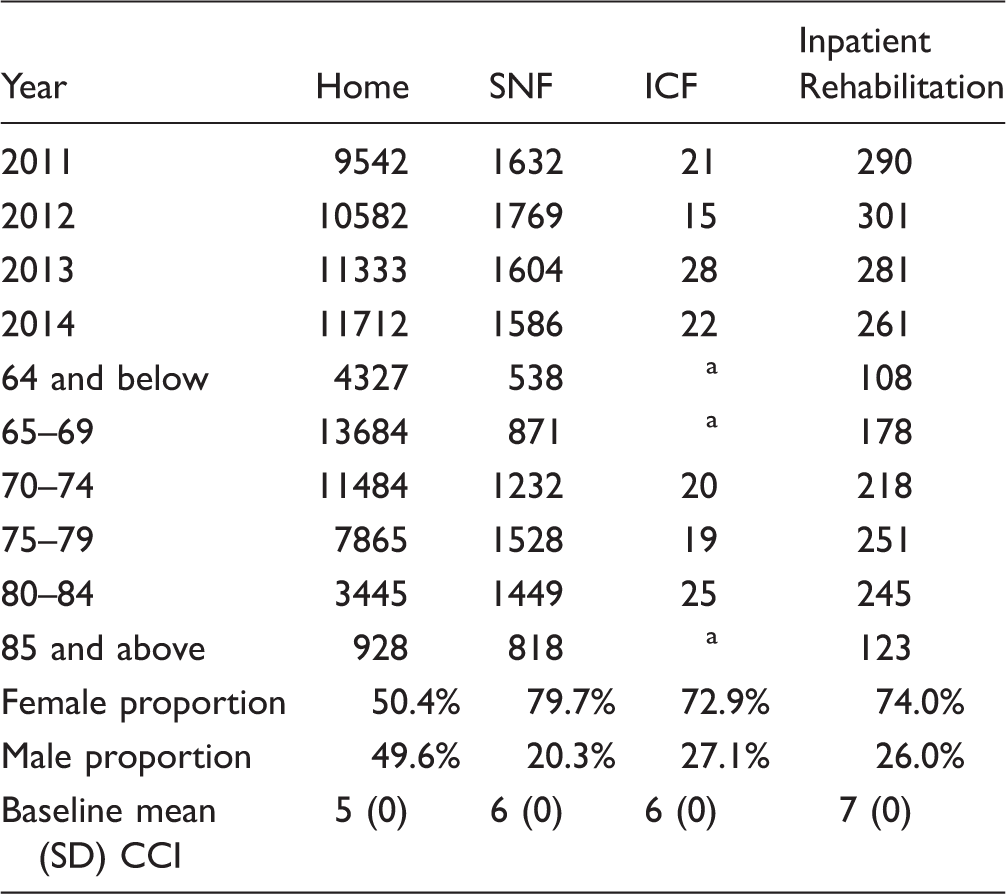
CCI, Charlson Comorbidity Index; ICF, intermediate care facility; SD, standard deviation; SNF, skilled nursing facility.
aGroup with less than 11 patients.
Trends in Discharge Disposition
Discharge to home was the most common disposition (84.7%), followed by SNF (12.9%), InR (2.2%), and ICF (0.2%; Figure 1). Trends over time analysis demonstrated that between the 4 groups, only 2 observed significant trend changes over time (Figure 2): discharge to home increased significantly from 83.1% to 86.2% (P = .037) and discharge to InR decreased from 2.5% to 1.9% (P = .015). No significant change occurred in the analysis over time of discharge to SNF (P = .054) and ICF (P = .741).
Distribution of discharge dispositions during the study period. ICF, intermediate care facility; SNF, skilled nursing facility. Discharge trends over time. ICF, intermediate care facility; SNF, skilled nursing facility.

Discharge Disposition Costs
Day of surgery
Mean Day of Surgery Reimbursements per Discharge Disposition.
ICF, intermediate care facility; SD, standard deviation; SNF, skilled nursing facility.
Global 90-day postoperative period
The total amount reimbursed by Medicare for the 50 959 patients was $678 038 480 US dollars. There was a significant difference (P < .001) in 90-day reimbursements based on the location of discharge disposition. The highest reimbursements were for those who were discharged to InR ($24 741; SD: $1922) and to ICF ($15 473; SD: $2366). Discharge to SNF ($15 093; SD: $622) and home ($12 691; SD: $471) was less costly.
Post hoc analysis demonstrated significant differences when comparing InR to all other disposition settings (P < .001). The post hoc test analysis demonstrated that there were no significant differences when comparing home to SNF (P = .311), home to ICF (P = .167), or ICF to SNF (P = 1.00). Figure 3 demonstrates these differences. The 90-day reimbursements of each group are presented in Table 3 and the 90-days charges in Table 4.
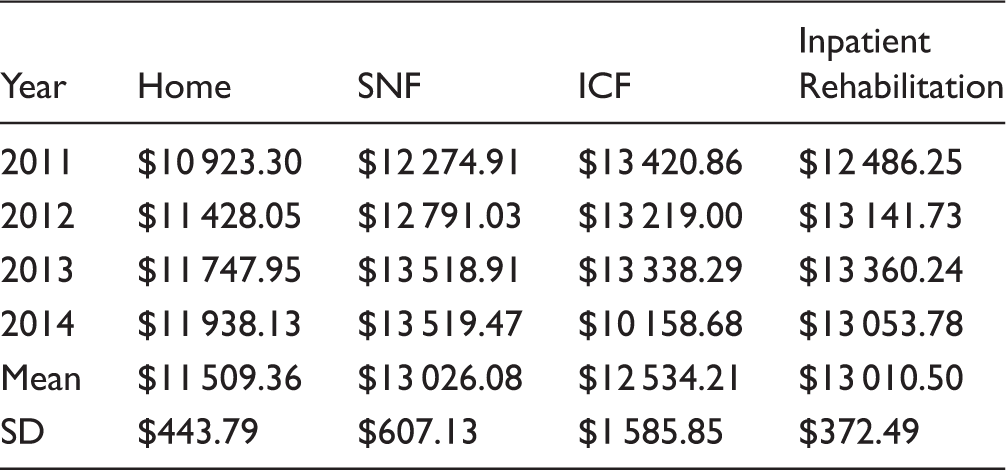
Mean 90-day reimbursement comparison. Mean 90 Days After Surgery Reimbursements per Discharge Disposition. ICF, intermediate care facility; SD, standard deviation; SNF, skilled nursing facility. Ninety-day Charges per Discharge Disposition. SNF, skilled nursing facility.


Percent of Reimbursement Differences Compared to Patients Discharged Home.

ICF, intermediate care facility; SNF, skilled nursing facility.
Charlson Comorbidity Index analysis
The ANOVA for the CCI demonstrated a significant difference in comorbidity burden (P < .001). The mean CCI of each group correlated with the setting of discharge disposition (P < .001), with lower CCI associated with an increased likelihood of a home discharge.
Length of stay analysis
Mean LOS for Each Patient Cohort.

ICF, intermediate care facility; LOS, length of stay; SD, standard deviation; SNF, skilled nursing facility.
Discussion
The purpose of this study was to compare the reimbursement costs based upon the location of discharge following TSA using an analysis of the Medicare database. Our results demonstrate that there is a difference in cost based upon the location of discharge. Although discharge to home continues to increase, discharge to an InR center (which was the most costly of all) increases 90-day reimbursements by 194% when compared to a home discharge. Additionally, patients with a higher comorbidity index were less likely to be discharged home.
Previous literature has focused mainly on the risk factors for discharge to a nonroutine facility. These recent articles have identified factors such as fracture indication, age, and gender that play a significant role in disposition to long-term treatment facilities. However, none of these studies have focused on the costs associated with placement in these facilities.6,8–11 Using the National Inpatient Sample and a sample of over 58 500 TSA procedures, Sivasundaram et al. 7 reported that number of comorbidities, older age, reverse shoulder arthroplasty, and female gender increased the odds of discharge to a postacute care facility. As systems begin to develop bundled payment initiatives for shoulder arthroplasty, recognition of the risk factors associated with discharge to a more costly inpatient facility can help impact patient selection for specific bundled payments. Furthermore, identification of such risk factors can facilitate preoperative risk stratification to select preventative care initiatives that may help these at-risk patients avoid costly discharge locations.
The finding that CCI score varied significantly by discharge disposition is similar to findings reported in previous arthroplasty literature.12–14 Voskuijl et al. 15 analyzed a centralized registry from the Massachusetts General Hospital and reported that a single point increase in the CCI score increased the risk of readmissions 0.45% for arthroplasty patients. Additionally, the authors found that during the 30-day postoperative readmission period, an increase in CCI meant increased mortality risk (0.25%, P < .001). Our observations that patients with increased CCI were more likely to be discharged to higher care facilities are consistent with this literature. Furthermore, our results suggest that the CCI may serve as a predictor of cost, with more expensive discharge dispositions being expected with higher CCI.
Our study also helps to reemphasize that the subsequent cost of care following the day of surgery significantly impacts the 90-day cost of care. Despite significant comorbidity (CCI) differences for each of the discharge disposition groups, the day-of-surgery reimbursement costs were identical, yet 90-day costs differed significantly. This is consistent with previous reports that have described how medical comorbidities significantly impact the cost of care for shoulder arthroplasty.16,17 A substantial portion of the increased costs seen after discharge for patients with comorbidities may relate to the location of discharge.
This study is not without limitations. The retrospective nature of this study introduces retrospective bias. Additionally, the PearlDiver database is reliant on accurate ICD-9 and Current Procedural Terminology (CPT) coding practices among physicians, which creates the potential for reporting bias. Furthermore, by restricting the analysis to Medicare claims, the actual cost of care may not be appreciated, as Medicare has more uniform reimbursement levels that may not reflect reimbursement costs seen with managed care contracts. Nonetheless, the major strength of this study is the completeness of data and large population size. Multiple variables may also determine discharge disposition trends such as hospital type, surgeon volume and/or region where the surgery was performed, thus further studies should aim at identifying the effects of these variables on discharge disposition, outcomes, and costs.
Conclusion
In the Medicare patient population, recent trends in discharge disposition demonstrate an increased trend toward discharging patients home, with a decreased use of InR services. Disposition of patients to InR increases the 90-day reimbursement costs by 195%, while those discharged to ICF have 123% greater costs than those discharged home. Patients with higher CCI index are more often discharged to facilities with higher overall cost.
Footnotes
Declaration of Conflicting Interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Author JCL is a paid consultant for DJO Orthopedics and Globus Medical. He receives royalties from DJO Orthopedics and Innomed.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.