
Abstract
Background
The Patient Acceptable Symptom State (PASS) is a symptom state that a patient considers acceptable. No prior study has determined the PASS for the American Shoulder and Elbow Surgeons (ASES) score, the Simple Shoulder Test (SST), and the Visual Analog Scale (VAS) pain score after shoulder arthroplasty. The purpose of this study was to determine the PASS for the ASES score, the SST score, and VAS pain for patients treated with a total shoulder arthroplasty.
Methods
A total of 326 patients had a primary anatomic total shoulder arthroplasty (TSA) or primary reverse total shoulder arthroplasty (RSA) by 1 of 5 shoulder and elbow surgeons at 1 of 2 institutions. Each patient completed the SST, ASES score, and a VAS pain preoperatively and at a minimum of 2 years postoperative (average 3.5 years). The PASS value for the ASES score, SST, and VAS pain was calculated.
Results
The PASS for the ASES score, SST, and VAS pain was 76, 8.4, and 1.5, respectively. Neither hand dominance nor age had a significant effect on PASS for SST, VAS, and ASES (P > .05). Gender had significant effect on SST and ASES scores with P-values of < .01 and .034, respectively. Duration of follow-up is correlated with VAS (P = .004) but not with ASES or SST scores.
Conclusions
Patients treated with a shoulder arthroplasty consider ASES score of 76, SST score of 8.4, and a VAS pain level of 1.5 to be acceptable symptomatic states. Females typically consider a slightly higher ASES and SST score to reach an acceptable state.
Introduction
Patient-reported outcome measures have been increasingly emphasized when assessing the value of orthopedic treatment options for common musculoskeletal conditions. 1 Many traditional outcome instruments have been widely utilized to assess outcomes in various domains. One common limitation of these measures is that most outcome scores are expressed as continuous data at a population level. This makes it difficult to interpret the response in a way that is meaningful to an individual patient. 2 Additionally, many traditional outcome scales rely on objective parameters with minimal subjective patient evaluation of their disease. The Patient Acceptable Symptom State (PASS) has been developed as a means to improve the subjective interpretation of outcome scores at the individual patient level. 3 Little existing research exists regarding PASS estimates for commonly used outcomes instruments which assess musculoskeletal conditions of the shoulder.
PASS is defined as a symptomatic state that is considered acceptable by the patient or the minimum score needed for the patient to “feel good.” 2 The PASS concept is helpful in interpreting currently utilized outcomes scores at the individual patient level. By comparing changes in commonly utilized functional scales to subsequent changes in PASS scores, a better understanding of the validity of the traditional scales can be obtained as it relates to a patient’s subjective feeling about their condition. In a changing health-care environment that places greater emphasis on subjective outcomes, patients’ experience, and quality of health-care delivery, there exists a need to understand traditional outcomes scales with patient-derived subjective assessment as is achieved with PASS.
The American Shoulder and Elbow Surgeons (ASES) score is a reliable, valid, and responsive measure of patient self-reported outcome for a variety of shoulder conditions. 4 The Simple Shoulder Test (SST) is a subjective measure of shoulder function that has been determined to be valid, reliable, and responsive when assessing psychometric properties by age and injury type. 5 Visual Analog Scales (VAS) are patient-based outcome scales that assess a variety of symptoms based on questions associated with that scale. VAS are validated, patient-reported scales that have been commonly utilized to evaluate pain.
While PASS scores have been established for various conditions including the arthritic hip and knee, Ankylosing Spondylitis, and rotator cuff disease,2,6,7 PASS has not been determined for ASES, SST, and VAS scales when assessing outcomes after shoulder arthroplasty. Given the rising incidence of shoulder arthroplasty in North America,8,9 there exists a need to determine PASS scores for traditional shoulder scales in order to gain better understanding of the patient’s interpretation of their symptomatic state.
The purposes of this study are (1) to estimate the PASS levels for the ASES score, the SST, and a pain VAS pain in patients treated with shoulder arthroplasty and (2) to determine the effect of various factors on these estimates.
Materials and Methods
A total of 326 patients who had previously undergone a primary anatomic total shoulder arthroplasty (TSA) or primary reverse total shoulder arthroplasty (RSA) or hemiarthroplasty between 2000 and 2012 by 1 of 5 shoulder and elbow surgeons at 1 of 2 institutions agreed to participate in this study. Patients were randomly selected from the clinical practices of the 5 shoulder and elbow surgeons if they were greater than 2 years removed from surgery. Patients were contacted by phone to collect subjective data allowing tabulation of outcomes.
Inclusion criteria included patients who had undergone a primary total shoulder arthroplasty, primary reverse total shoulder arthroplasty, or hemiarthroplasty with at least 2 years of postoperative follow-up who agreed to participate in the study. Arthroplasty was performed to surgically treat glenohumeral osteoarthritis, rotator cuff tear arthropathy, avascular necrosis, or proximal humerus fracture. Prior surgery to the involved shoulder was not considered a criteria for exclusion so long as it did not include a prior arthroplasty procedure. Exclusion criteria included any patients undergoing revision shoulder arthroplasty or those patients who declined to participate in the study.
Prior to shoulder arthroplasty, patients were evaluated with a history, physical examination, and radiographs of the shoulder. Some patients who had a concern for rotator cuff deficiency also underwent an MRI or ultrasound. Preoperative CT scan was performed in cases where advanced imaging of the glenohumeral osseous structure was deemed necessary. Patients were indicated for surgery after failing a period of nonoperative management. Nonoperative treatment was not standardized but was tailored to the individual needs and wishes of the patient. Each patient completed the SST, ASES score, and a VAS pain preoperatively.
Patients were evaluated at a minimum of 2 years following surgery. At final follow-up, each patient completed a questionnaire that included the ASES, SST, and VAS pain score. In addition, patients responded to a question regarding their final satisfaction with their symptom state. The question was a “yes/no” question as follows: “Taking into account all the activities you have during your daily life, your level of pain, and also your functional impairment, do you consider that your current state is satisfactory?” This question was derived from the anchor questions designed by Tubach 3 estimating the PASS.
Statistical Analysis
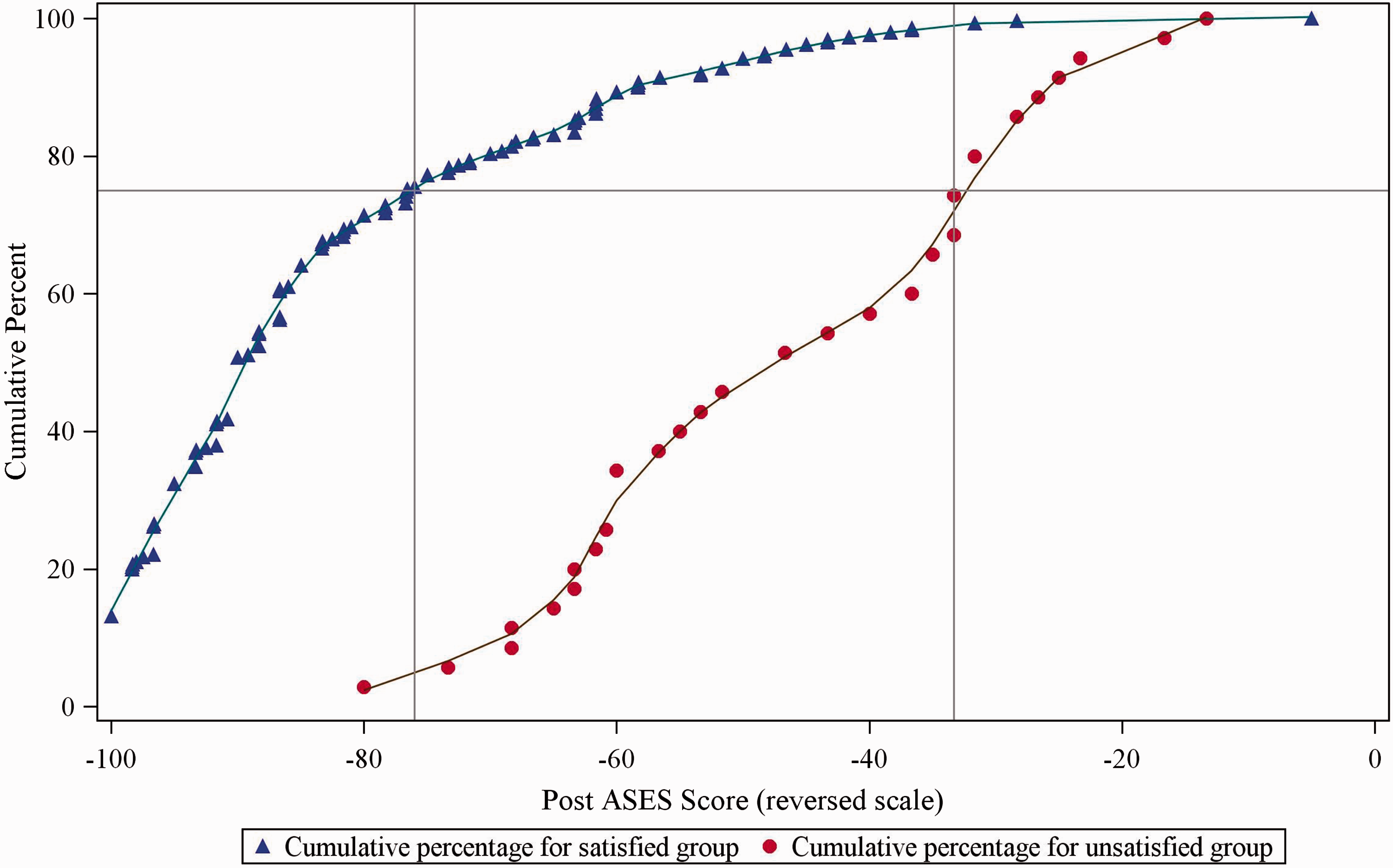
The change in ASES, SST, and VAS pain scores from initial evaluation to final follow-up for each patient was calculated. The patient acceptable symptomatic state (PASS) was estimated by constructing a curve of cumulative percentages of patients as a function of the score of interest at the final visit among patients who considered their state satisfactory based upon the 2-item question described in the previous section. The 75th percentile of the cumulative percentage curve was defined as the PASS by Tubach 3 (SAS Institute, Inc, Cary, NC). In the PASS calculation, VAS pain score was used as the original scale, but SST and ASES scores were reversed to match the direction of the pain scales.
Secondary analysis was performed to determine the effect of patient-related and treatment factors on the PASS. Spearman correlations were utilized to compare the PASS with age, gender, hand dominance, and duration of follow-up. The effect of baseline SST, VAS pain, and ASES scores on the PASS was determined by defining first a cutoff point for high and low baseline scores, which were the median baseline values for the corresponding scores. The association between high/low baseline scores and the overall PASS was evaluated using odds ratios. P values less than .05 were considered significant.
Results
Patient Characteristics.
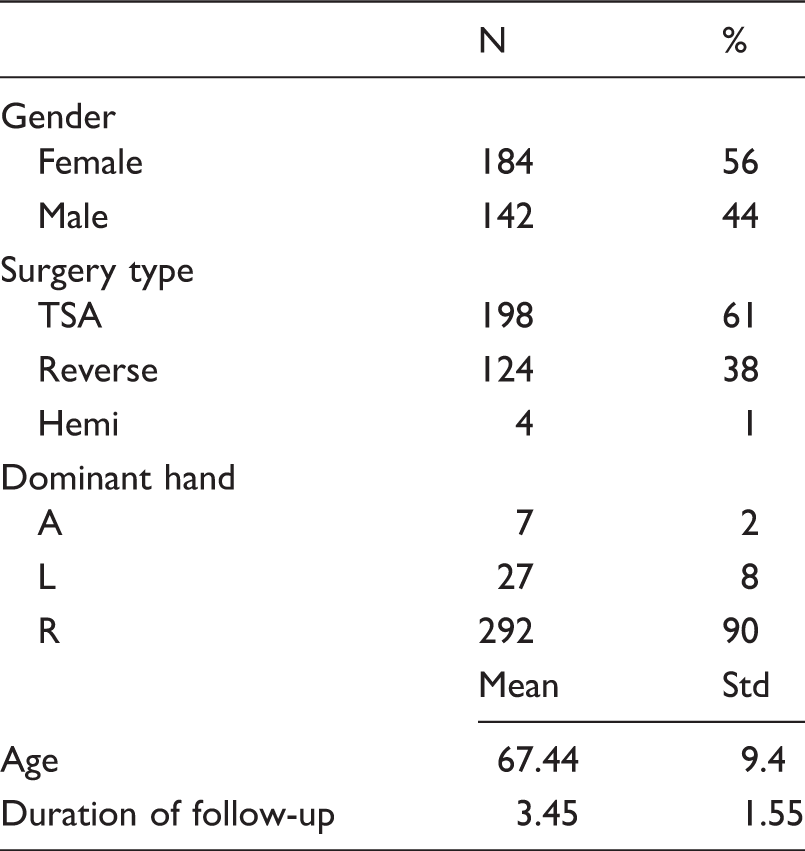
TSA, Total Shoulder Arthroplasty.
The PASS was estimated as the 75th percentile of the score for patients who considered their state satisfactory. The PASS for the ASES score, SST, and VAS pain was 76, 8.4, and 1.5, respectively (Figures 1 to 3). Median score for SST is 2, for VAS is 7, and for ASES is 30.
Cumulative Distribution Function Used to Determine the PASS for SST. Cumulative Distribution Function Used to Determine the PASS for VAS. Cumulative Distribution Function Used to Determine the PASS for ASES.

Spearman Correlations Evaluating Associations Between Age and Duration of Follow-up Time With SST, VAS, and ASES in Satisfied Group.
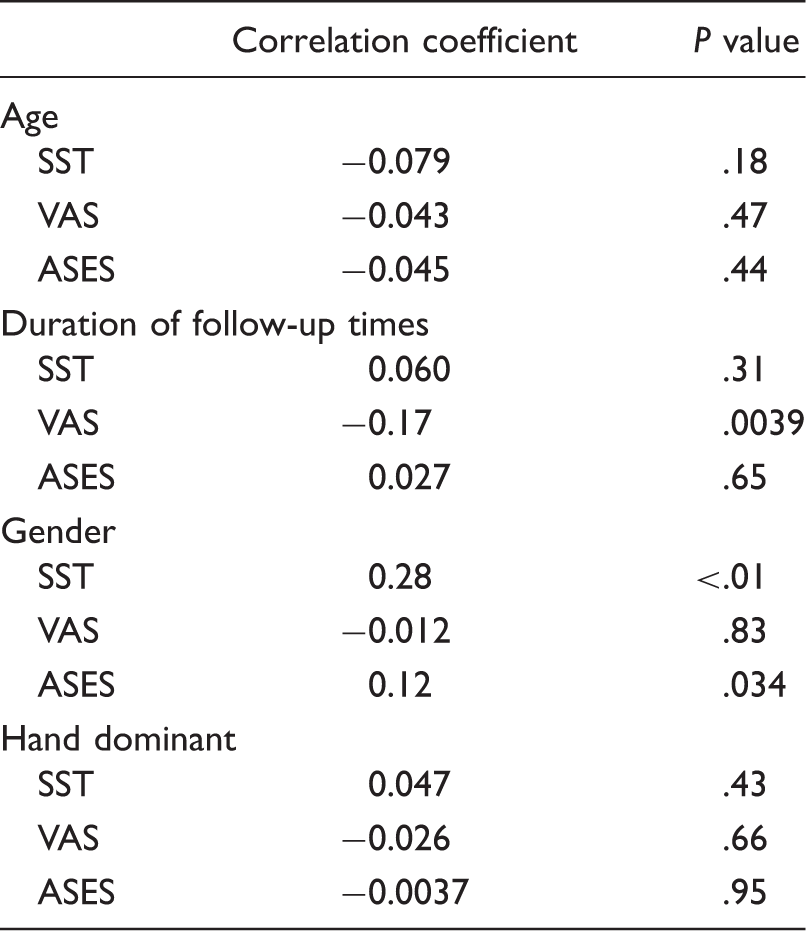
ASES, American Shoulder and Elbow Surgeons; PASS, Patient Acceptable Symptomatic State; SST, Simple Shoulder Test; VAS, Visual Analog Scale.
Associations Between Baseline SST, VAS, ASES Scores Above or Below the Median and Achievement of PASS.

The below median group was used as reference. ASES, American Shoulder and Elbow Surgeons; PASS, Patient Acceptable Symptomatic State; SST, Simple Shoulder Test; VAS, Visual Analog Scale.
Discussion
The ASES, SST, and VAS pain scales are common measures used to assess outcomes of patients undergoing shoulder arthroplasty. In this study, we have demonstrated that patients who respond with an ASES score of 76 or higher have achieved an acceptable symptomatic state. Similarly, patients with an SST score of at least 8.4 and VAS pain score of 1.5 or higher have achieved an acceptable symptomatic state.
To our knowledge, no previous study has reported on the PASS estimates for ASES, SST, and VAS pain scales in the setting of shoulder arthroplasty to manage shoulder arthritis. There is a paucity of existing published data that reports the results for PASS estimates in patients with shoulder disorders. Tubach et al. 7 published PASS estimates for VAS scale in the nonoperative management of “acute rotator cuff syndrome.” They reported on 271 patients at baseline and after 1 week of anti-inflammatory or placebo treatment. Results were PASS estimates ranging from 1.6 to 2.4 cm on a 10-cm VAS pain scale.
PASS estimates have also been reported for VAS pain scales in other disease processes including knee and hip arthritis, anterior (patellofemoral) knee pain, rheumatoid arthritis, and neck pain.3,10–12 PASS estimates for these conditions ranged from 2 to 3.5 on a 10-cm scale. This is similar to the PASS estimate of 1.5 we report in this cohort of patients treated with shoulder arthroplasty.
We evaluated numerous various factors that may affect PASS estimates. From our analysis, duration of follow-up affected the VAS but not the ASES or SST scores. As patients are further from their surgery, they seem to tolerate less pain in order to consider their symptom state to be acceptable. Gender also significantly affected PASS estimates in SST and ASES scores. No effect of age and hand dominance was identified.
This study has several limitations. We analyzed a relatively limited number of potential factors that could affect PASS estimates. Other factors not analyzed in this study that might affect the PASS estimates include labor versus sedentary occupation, psychiatric disease, or cultural background. Occupational information and cultural/demographic information was not consistently collected on all patients. Finally, no analysis was performed to evaluate the effect of other concomitant disease processes that cause shoulder pain and dysfunction not treated by shoulder arthroplasty (ie, pain disorders, cervical spine pathology, myalgias, etc). Medical histories inquiring about these pathologic processes were not uniformly performed. We feel, however, that these medical comorbidities would contribute to a negligible degree given that patients in this cohort were treated for degenerative disease of the shoulder not routinely associated with these other potential causes of pain and dysfunction.
Conclusion
This study determines the PASS estimates for ASES, SST, and VAS pain in patients who have undergone shoulder arthroplasty. The PASS value provides greater understanding of patient-derived outcomes and acceptable state in terms of legacy outcome scales. This understanding will improve providers’ interpretation of legacy outcome scores in terms of what a patient finds acceptable and can inform future studies that evaluate patient satisfaction.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the Washington University Institute of Clinical and Translational Sciences grant UL1 TR000448 from the National Center for Advancing Translational Sciences (NCATS) of the National Institutes of Health (NIH). The content is solely the responsibility of the authors and does not necessarily represent the official view of the NIH.