
Abstract
Background
This study compares open reduction and internal fixation (ORIF) versus hemiarthroplasty (HA) in the management of proximal humerus fracture-dislocations and complex articular humeral head fractures.
Methods
The records of consecutive patients with Neer 3- and 4-part fracture-dislocations, surgical neck fracture-dislocations with severe articular impaction, and any head-split fracture treated surgically at our institution were studied retrospectively. Constant–Murley scores, Disability of the Arm, Shoulder and Hand (DASH), American Shoulder and Elbow Surgeons Shoulder (ASES), and Short Form Health Survey (SF-36) scores were obtained and compared between ORIF versus HA treatment.
Results
Thirty patients were included in the analysis: 15 treated with ORIF were compared to 15 treated with HA with an average follow-up of 60 months. The mean Constant score (72 ± 15 vs 54 ± 19; P = .007), DASH score (13 ± 17 vs 29 ± 18; P = .006), ASES score (87 ± 13 vs 66 ± 22; P = .003), and SF-36 physical composite score (PCS) (50 ± 11 vs 40 ± 11; P = .02) all favored the ORIF group. Because of the potential confounding variable posed by including younger patients, we performed a subgroup analysis of patients older than 50 years. In this group, the Constant, DASH, ASES, and PCS scores remained significantly better in the ORIF group.
Conclusion
Results of this retrospective study show improved patient-reported outcomes and quality of life scores in patients undergoing ORIF for complex proximal humerus fractures as compared to patients undergoing HA, despite a higher revision rate in the ORIF cohort. When considering patients older than 50 years, outcomes after ORIF were better than HA.
Keywords
Introduction
Proximal humerus fractures are common and are often complex and challenging for the treating surgeon. These fractures represent a spectrum of injury ranging from low-energy osteoporotic fractures in the elderly to high-energy fracture-dislocations.1,2 Despite an expanding belief that many proximal humerus fractures should be treated nonoperatively, 3 complications commonly occur when treating complex proximal humerus fractures nonoperatively, which can cause significant functional disability for patients. 4 While low-energy, minimally displaced, or valgus-impacted fractures are often treated nonoperatively with a relatively low rate of nonunion, 5 displaced and comminuted fractures have a greater risk of malunion and nonunion of the humeral head.4,6
Surgical management strategies for complex proximal humerus fractures include open reduction and internal fixation (ORIF) or arthroplasty—either hemiarthroplasty (HA) or reverse total shoulder arthroplasty (RTSA).2,4,7–12 There is controversy regarding whether ORIF or HA is superior when treating complex proximal humerus fractures and fracture-dislocations, and few studies examine the difference in outcomes.4,11,13 Many surgeons agree that young patients should be treated with anatomic reduction and plate osteosynthesis in order to preserve bone stock, improve tuberosity healing, and prevent glenoid erosion and arthrosis that could result from HA despite the lack of studies comparing ORIF to HA in young patients (<50 years of age). Recent studies suggest that RTSA for 3- and 4-part proximal humerus fractures may have improved outcomes and a lower failure rate compared to HA. 14
The purpose of this study was to compare the clinical outcomes of all patients treated at a single institution with complex proximal humerus fractures, including fracture-dislocations and head-split fractures, with either ORIF or HA. We hypothesized that despite a high rate of osteonecrosis of the humeral head, ORIF would demonstrate significantly better functional outcome scores and health-related quality of life scores when compared to HA.
Materials and Methods
The records of 459 consecutive patients in whom a proximal humerus fracture was treated surgically at our institution between the years 2002 and 2012 were studied retrospectively. Fractures were identified by Current Procedural Terminology code: 23615, 23616, 23670, and 23680. All fractures were classified according to the Neer 15 classification method by the primary author (RT). Fractures identified for further analysis included Neer 3- and 4-part fracture-dislocations, surgical neck fracture-dislocations with severe articular impaction, and any head-split fracture. Clinical outcomes included the Constant–Murley score as a primary outcome, with secondary outcomes including the DASH and ASES scores. Health-related quality of life was assessed with the use of the SF-36. Measurements of strength, range of motion, and all other outcome measures were recorded by the primary author (RT) or a senior physical therapist with extensive experience with the outcome measures utilized (KO). All outcome scores and health-related quality of life scores were obtained at the patient’s final follow-up visit. Preoperative scores were not available.
Patients were included in the analysis if they were of a minimum age of 18 years, the fracture pattern was classified as a Neer 2-, 3-, or 4-part fracture of the proximal humerus involving the surgical or anatomic neck with an associated anterior or posterior dislocation, or any head-splitting fracture; the patient must have been managed with primary fixation with plate and/or screws or primary HA for management of the fracture. Patients required a minimum 1-year follow-up for inclusion. Patients were excluded if they were younger than 18 years of age, if death occurred during the review period, or if any reoperation on the ipsilateral shoulder occurred during the review period, including revision arthroplasty or conversion of failed ORIF to arthroplasty. Patients were also excluded if dementia or other mental health illness prevented the ability to adequately complete questionnaires. Greater and lesser tuberosity fracture-dislocations were excluded.
Postoperative radiographs were analyzed at final follow-up. For the ORIF cohort, radiographs were assessed for the presence of osteonecrosis, malunion, nonunion, head-to-tuberosity height (HTH), the presence of varus collapse, and screw cutout (Figures 1 and 2). Tuberosity malunion was defined as displacement > 5 mm or a HTH outside of 0–12 mm. Proximal humerus malunion was defined as varus collapse of more than 10°. For the HA cohort, radiographs were assessed for tuberosity nonunion, tuberosity resorption, and HTH. Nonunion was defined as failure to heal by 9 months postoperatively. Tuberosity resorption was categorized as partial or complete.
Complex anterior fracture-dislocation of the proximal humerus. Head-splitting proximal humerus fracture with anterior subluxation of the anterior head fragment over the glenoid articular margin.

In an attempt to account for differences in age, a subgroup analysis was performed for patients aged 50 years and older. Clinical outcomes and health-related quality of life scores were compared as per the above methods.
Statistical analysis was carried out using SPSS v.19 (Armonk, NY) software. Student t-tests were used to compare means, while Fisher exact test was used to compare categorical data, with significance set at P < .05. All values are presented as mean ± standard deviation.
Results
Fracture Characteristics.

With regard to functional outcomes, the mean Constant score at the time of final follow-up was significantly better in the ORIF group (72 ± 15) compared to the HA group (54 ± 19) (P = .007). Similarly, the mean DASH score (13 ± 17 and 29 ± 18; P = .006) and ASES score (87 ± 13 and 66 ± 22; P = .003) were significantly better in the ORIF group compared to the HA group.
With regard to health-related quality of life scores, the SF-36 scores of physical functioning (PF) (82 ± 22 and 56 ± 28; P = .008), bodily pain (BP) (84 ± 21 and 66 ± 22; P = .02), and physical composite score (PCS) (50 ± 11 and 40 ± 11; P = .02) were all significantly better in the ORIF group compared to the HA group. No differences between the groups were observed for the remaining SF-36 subscores, including physical role, general health, vitality, social functioning, emotional role, mental health, or mental composite score.
Mean Constant, DASH, and ASES Scores as Well as SF-36 Component Scores in Patients > 50 Years of Age Treated With ORIF or Primary HA in the Management of Fracture-dislocations or Head-Split Fractures of the Proximal Humerus.
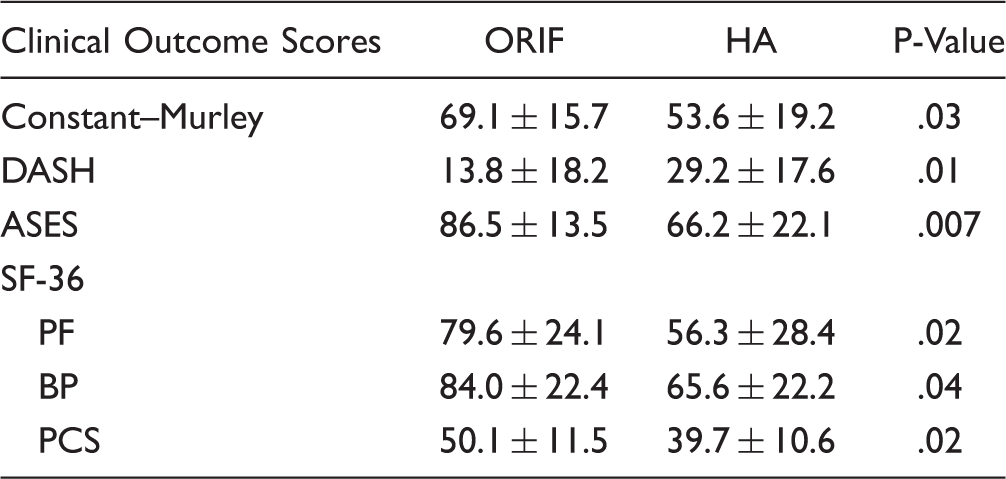
ASES, American Shoulder and Elbow Surgeons Shoulder; BP, bodily pain; DASH, Disability of the Arm, Shoulder and Hand; HA, hemiarthroplasty; ORIF, open reduction and internal fixation; PCS, Physical composite score; PF, physical functioning.
PCS is a normative value relative to the Unites States population.
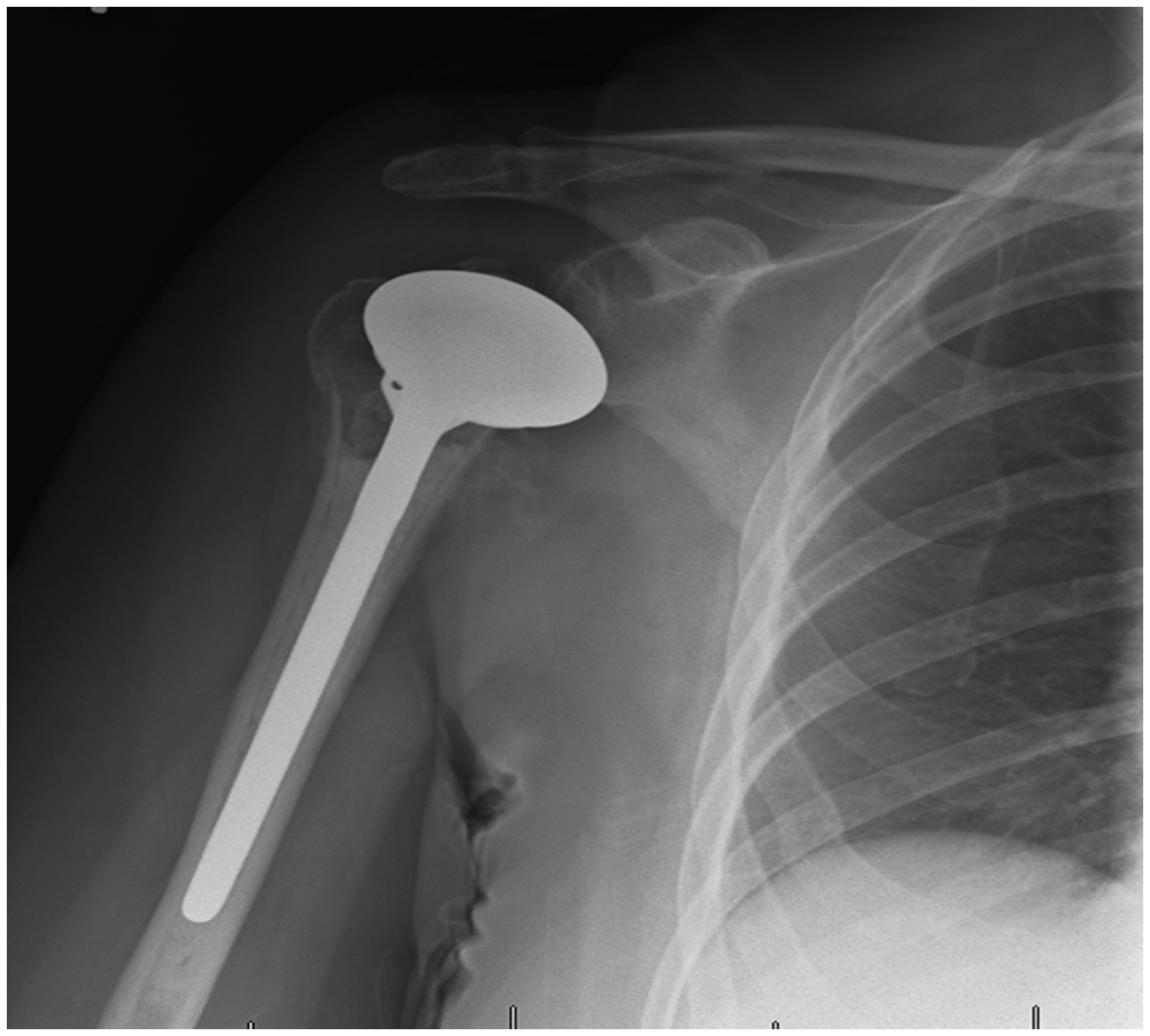
Regarding radiographic outcomes, among the ORIF group, all fractures healed with a tuberosity malunion rate of 33%, osteonecrosis rate of 20%, and screw cutout rate of 7%. The mean head-shaft angle was 131°, with a mean varus collapse of 5° ± 5° at final follow-up. The mean HTH was 9 ± 8 mm. Among the HA group, 8 of 15 patients (53%) suffered tuberosity complications, including 5 nonunions (33%), 3 instances of complete tuberosity resorption (20%), and 5 instances of partial tuberosity resorption (33%). The mean HTH was 15 mm ± 7 mm. Examples of postoperative radiographs from patients in the ORIF and HA groups are seen in Figures 3 and 4.
Postoperative radiograph of a proximal humerus fracture with locking plate fixation. Postoperative radiograph of a hemi-arthroplasty utilized for a proximal humerus fracture.
With regard to complications, all patients were included. Among the 32 patients who underwent ORIF, there were 6 cases of osteonecrosis (19%), 9 cases of hardware complications including cutout (28%), 1 neurovascular injury (3%), and 2 deep infections (6%). Reoperation was necessary in 7 patients (22%), with 18 reoperations necessary, the majority of which were for a single patient who suffered a brachial plexus and axillary arterial injury with compartment syndrome. Among the 34 patients who underwent HA, there were 4 cases of neurovascular injury (12%), no deep infections (0%), and reoperation was necessary in 2 patients (6%), with 3 reoperations in 2 patients. The difference in re-operations between ORIF and HA groups trended toward statistical significance (P = .07).
Discussion
There remains debate regarding whether ORIF or HA is superior in adults with complex proximal humerus fractures, and few studies examine the difference in clinical outcomes.4,11,13 Many surgeons argue that younger patients should undergo primary fixation of displaced fractures, even fracture-dislocations and head-split fractures with notoriously high osteonecrosis rates. However, the optimal treatment for more complex fractures including Neer 3- and 4-part fractures and fracture-dislocations in older patients with reduced bone quality remains controversial. If anatomic reduction can be achieved, locking plate fixation of these fractures is reasonable, and evidence suggests that medial column support is essential.16,17 However, complications are common when treating these complex fractures with locked plating including loss of fixation with varus collapse and subsequent screw cutout, and osteonecrosis of the humeral head.4,11,18 Because of these complications, some authors recommend HA in the management of 3- and 4-part proximal humerus fractures, especially fracture-dislocations and head-split fractures. This is especially true in elderly patients who are low demand with osteopenic bone, varus malalignment, or when anatomic reduction cannot be achieved intraoperatively.1,4,7 While studies evaluating HA have consistently demonstrated predictable pain relief, they have unfortunately also demonstrated inconsistent functional outcomes.8,19–24 The variable clinical results of HA are likely multifactorial, relating to surgeon experience, the degree of postoperative rehabilitation, anatomic positioning of the stem, anatomic healing of the tuberosities. Further, other factors that are associated with outcomes after HA include age, hand dominance, rotator cuff status, and implant type.25–29
Because proximal humerus fracture-dislocations and head-split fractures have a notoriously high rate of osteonecrosis and hardware complications,11,13,30 they often present a treatment dilemma for surgeons, especially in young patients where preservation of native anatomy and avoidance of arthroplasty is preferable. This study sought to evaluate the clinical outcomes and health-related quality of life scores when treating patients with these injuries. We identified that, when successfully performed, ORIF can have a substantial benefit on outcome scores and quality of life scores even in the most severe proximal humerus fractures. Further, these scores were significantly improved when compared to HA. Despite these improved outcomes, however, ORIF does carry a significantly higher revision rate when compared to HA.
Previous studies investigating the best method for surgical treatment of more complex proximal humerus fractures have had varying conclusions. Solberg et al. 11 found significantly improved Constant scores in patients treated with locked plating for 3- and 4-part fractures, including fracture-dislocations. However, another more recent study found no difference in Constant scores or SF-36 scores between patients treated with ORIF or HA for fracture-dislocations of the proximal humerus. 13 Similar to our data, a number of studies reporting complications predominantly found osteonecrosis and screw cutout to be the most frequent complications following ORIF.11,13 Reoperation rates after ORIF were high in our study, and have been reported to be even higher in previous work, ranging from 29% to 45%.11,13 While it appears that treatment of these fractures with HA results in a lower reoperation rate,11,13our data suggest a similar trend despite lacking statistical significance (ORIF 21.9% vs HA 5.4%, P = .07).
New technology may eventually change the standard of care for management of proximal humerus fractures, especially in the elderly. Despite new technology, however, nonoperative treatment remains a very reasonable option in the elderly. 3 RTSA is gaining popularity in treating elderly patients who sustain proximal humerus fractures. Forward elevation and abduction do not rely on an intact rotator cuff with the RTSA design,31,32 indicating that anatomic tuberosity healing is not necessary for functional motion. Following HA treatment, suboptimal outcomes have been linked to malunion and nonunion of the greater tuberosity. 33 When comparing RTSA and HA, the best available evidence suggests that RTSA performs better than HA based on ASES scores, Constant scores, as well as forward flexion and abduction motions.34,35 Further data suggest that forward flexion, abduction, and functional outcome scores are not hindered with greater tuberosity malunion or nonunion when RTSA is performed. 36 Given these promising outcomes, RTSA may eventually replace HA as the standard arthroplasty technique for the treatment of these “complex articular” fractures.
The results of this study need to be interpreted with caution. There was a significant difference in age between the patients, which likely represents surgeon preference for primary ORIF versus HA in these fractures in younger patients. Clearly, when presented with a comminuted fracture, a head-splitting fracture, or a fracture-dislocation, surgeons appear to be making treatment decisions based upon age. It would be preferable to perform primary fixation in young patients with the possibility of avoiding osteonecrosis and poor outcomes but primary arthroplasty in a young patient presents its own challenges. We chose to limit patients to age > 50 years to help control for the age difference between patients, which was still significant between ORIF and HA (mean age 64 vs 73, respectively). While the primary and secondary outcome scores and SF-36 scores remained remarkably better in the ORIF cohort in this subgroup analysis, this still represents a significant limitation to the results. This study also excluded patients who underwent revision surgery on the operative extremity with regard to outcomes measures. This remains a substantial limitation as the ORIF cohort had a significantly higher revision rate; however, we feel there is a greater tendency for a poorly functioning HA to be managed nonoperatively, while a poorly functioning ORIF can be more readily revised to an arthroplasty. A significant number of patients undergoing primary ORIF of their fracture required revision surgery for a number of reasons including failed fixation. Inclusion of these patients would likely confound the results with regard to outcome scores.
Conclusion
Results of this retrospective study show improved patient-reported outcomes and quality of life scores in patients undergoing ORIF for complex proximal humerus fractures as compared to patients undergoing HA, despite a higher revision rate in the ORIF cohort. When considering only patients older than 50 years, outcomes after ORIF were significantly better than HA.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Ilya Voloshin is a paid consultant for “Zimmer,” “Arthrex,” and “Smith & Nephew.” Ilya Voloshin receives speaking fees from “Zimmer,” “Arthrex,” and “Smith & Nephew.” The rest of the authors have no potential conflicting interests to declare. No other financial payments or benefits from any other commercial entity related to the subject of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Level of Evidence
3