
Abstract
Background
Adolescent suicide is a leading cause of death globally and remains a major public health concern in the United States. Chronic stress perspectives suggest that suicidal behaviors emerge from cumulative and interacting stress exposures that become biologically and psychologically embedded across development. This study applies an integrated chronic stress framework to examine how adverse childhood experiences (ACEs), victimization, and protective relational resources jointly shape suicide-related behaviors among U.S. high school students.
Methods
We conducted a cross-sectional analysis of the 2023 combined National Youth Risk Behavior Surveillance System dataset (N = 254,675). National-level proportional outcomes included serious suicidal ideation, suicide planning, suicide attempts, and medically treated suicide attempts. Standardized composite indices were constructed for ACEs, victimization, and protective resources (school connectedness and parental monitoring). Fractional logistic regression models estimated average marginal effects (AMEs), adjusting for persistent sadness/hopelessness, poor mental health, sleep duration, unstable housing, and demographic characteristics. Interaction terms tested cumulative and conditional stress processes.
Results
Higher ACE and victimization indices were independently associated with greater prevalence of all suicide-related outcomes. A one-unit increase in the ACE index was associated with increased ideation (AME = 0.0534, 95%CI [0.0411, 0.0656]) and attempts (AME = 0.0240, 95%CI [0.0148, 0.0332]). Victimization demonstrated comparable or stronger associations, particularly for planning (AME = 0.0723, 95% CI [0.0605, 0.0841]) and attempts (AME = 0.0571, 95%CI [0.0472, 0.0670]). Protective resources were inversely associated with planning (AME = −0.0130, 95%CI [−0.0192, −0.0067]) and attempts (AME = −0.0110, 95%CI [−0.0159, −0.0060]). Interaction analyses revealed diminishing marginal effects at higher combined levels of ACEs and victimization (eg, ACE × victimization for ideation AME = −0.0395, 95% CI [−0.0567, −0.0223]), indicating nonlinear accumulation of stress burden. A significant three-way interaction for ideation (AME = 0.0193, 95%CI [0.0045, 0.0342]) suggested conditional buffering by protective resources. Persistent sadness/hopelessness remained the strongest correlate across outcomes.
Conclusions
Adolescent suicidality reflects cumulative and interacting stress processes rather than isolated risk factors. Early adversity establishes foundational stress load, ongoing victimization compounds risk, and protective relational assets provide partial—but not complete—buffering. These findings support multilevel prevention strategies that reduce chronic stress exposure while strengthening relational protection across developmental contexts.
Keywords
Introduction
Suicidal behavior among adolescents and young adults remains a critical public health challenge globally, with rising prevalence observed across multiple regions over the past decade. Although trends vary by country, suicide is consistently ranked among the leading causes of death for young people worldwide. According to the World Health Organization (WHO), suicide is among the top three causes of death for individuals aged 15–29 years globally, accounting for more than 720,000 deaths annually. In many high-income countries—including the United States, Canada, Australia, and several European nations—self-harm and suicide rank as either the first or second leading cause of death among adolescents. 1 Population-based school surveys further indicate substantial levels of nonfatal suicidal behaviors across diverse settings. For example, recent data from the Global School-based Student Health Survey show that serious consideration of suicide among adolescents ranges from approximately 10%–25% across countries in Africa, Latin America, and Southeast Asia, with suicide attempts frequently reported by 5%–15% of youth depending on national context.2,3
Within the United States, prevalence has increased markedly over the past decade, with substantial disparities persisting across demographic and social groups. National surveillance data indicate that large proportions of U.S. high school students report suicidal ideation, planning, and attempts. For example, the Centers for Disease Control and Prevention (CDC) 2023 Youth Risk Behavior Survey reports that 20.4% of high school students seriously considered attempting suicide and 9.5% attempted suicide. 4 Comparable patterns have been observed in Canada and parts of Western Europe, where adolescent self-reported suicidal ideation commonly exceeds 15% in national school-based surveys, underscoring that this is not solely a U.S.-specific crisis but part of a broader international mental health challenge among youth.
Emerging cross-national evidence suggests that adolescent suicidality is rarely driven by isolated risk factors. Instead, it reflects cumulative and interacting exposures spanning early life adversity, interpersonal victimization, and structural stressors. Adverse childhood experiences (ACEs)—including abuse, household dysfunction, and exposure to violence—represent a foundational source of chronic stress with enduring implications for mental health and suicidality across diverse cultural contexts.5,6 International meta-analyses demonstrate dose–response associations between cumulative ACE exposure and suicidal ideation and attempts among adolescents in North America, Europe, and Asia. Recent analyses of U.S. high school students indicate that ACEs account for a substantial share of the population-attributable risk for suicidal ideation and attempts, with estimates exceeding 80% for some outcomes in 2023. 6 Consistent with a large and growing literature, cumulative ACE exposure has been linked to heightened emotional distress, maladaptive coping, and increased risk of suicidal behaviors among adolescents.7–9 Importantly, these associations appear to intensify during periods of societal disruption—including the COVID-19 pandemic—when stressors related to family instability, social isolation, and economic strain become more pronounced globally.10–12
Beyond early household adversity, multidemensional victimization experiences during adolescence—such as bullying, cybervictimization, physical assault, sexual violence, and harassment—constitute salient stress exposures that independently and cumulatively elevate suicide risk across countries. International meta-analytic and umbrella reviews indicate that peer victimization and cyberbullying are consistently associated with internalizing symptoms, including depression and hopelessness, which are proximal predictors of suicidal ideation and attempts. 13 Cross-national studies from Europe, East Asia, and Latin America similarly show that youth exposed to repeated bullying or violence report significantly higher odds of suicidal thoughts and behaviors compared to non-victimized peers. Exposure to violence in schools, relationships, and neighborhoods further compounds risk by normalizing fear, eroding perceptions of safety, and increasing stress reactivity. These experiences are often patterned by social and structural inequalities—including poverty, migration stress, discrimination, and housing instability—thereby disproportionately affecting marginalized youth across global contexts.
In contrast, protective factors operating within family and school environments demonstrate cross-cultural relevance in mitigating the psychological impact of adversity. School connectedness—characterized by supportive relationships, a sense of belonging, and engagement in the school environment—has been consistently associated with lower levels of emotional distress and reduced likelihood of suicidal behaviors in North America, Europe, and parts of Asia, even among adolescents exposed to multiple stressors.14–17
Similarly, parental monitoring and emotionally responsive caregiving promote adaptive coping and emotional regulation, buffering the psychological consequences of chronic stress across diverse sociocultural contexts.5,18 These protective processes operate across ecological levels, reinforcing social bonds and fostering resilience during a developmental period marked by heightened neurobiological sensitivity to stress. Taken together, global and U.S.-based evidence converge on a central conclusion that adolescent suicidal behaviors reflect layered and interacting stress exposures rather than singular risk pathways. Situating U.S. findings within this broader international landscape underscores both the universality of chronic stress processes and the importance of examining how cumulative adversity, concurrent victimization exposure, and protective social resources jointly shape suicide-related behaviors during adolescence.
Conceptual Framework of Adolescent Suicidality
Building on the international evidence presented above, the present study is guided by a cumulative and interactive stress framework that conceptualizes adolescent suicidal ideation, planning, and attempts as downstream outcomes of layered adversity operating across developmental and ecological contexts (Figure 1). Rather than isolating individual risk factors, this framework positions early adversity, concurrent victimization, and relational resources within a single stress-accumulation process in which risk unfolds through both additive and synergistic mechanisms.

Flowchart illustrating the relationships Among adverse childhood experiences (ACEs), victimization, protective factors, and covariates in predicting adolescent suicidality.
ACEs are conceptualized as foundational stress exposures that become biologically and psychologically embedded over time.19,20 Chronic exposure to abuse, household dysfunction, and violence recalibrates stress-response and emotion-regulation systems, increasing vulnerability to depressive symptoms, hopelessness, and maladaptive coping.21–23 During adolescence—a period of heightened neurobiological sensitivity—these embedded adaptations may elevate susceptibility to suicidal thoughts and behaviors.
Victimization experiences during adolescence function as proximal stressors layered onto earlier adversity. Consistent with cross-national findings linking bullying and violence exposure to suicidal behaviors, 13 victimization is conceptualized as an independent contributor to suicide-related outcomes. Importantly, the framework also specifies an interaction between ACEs and victimization. Early adversity is hypothesized to sensitize stress-response systems such that subsequent victimization exerts stronger effects among youth with higher ACE exposure, reflecting stress amplification rather than simple accumulation.
Protective social resources operationalized as school connectedness and parental monitoring are positioned as relational buffers within adolescents’ ecological contexts. These assets promote belonging, reinforce emotion regulation, and dampen stress reactivity.5,15,16 In the model, protective resources are expected to demonstrate inverse associations with suicide-related outcomes and to moderate stress pathways in two ways, first by weakening the association between ACEs and suicidality and second, by reducing the impact of victimization on suicide-related outcomes.
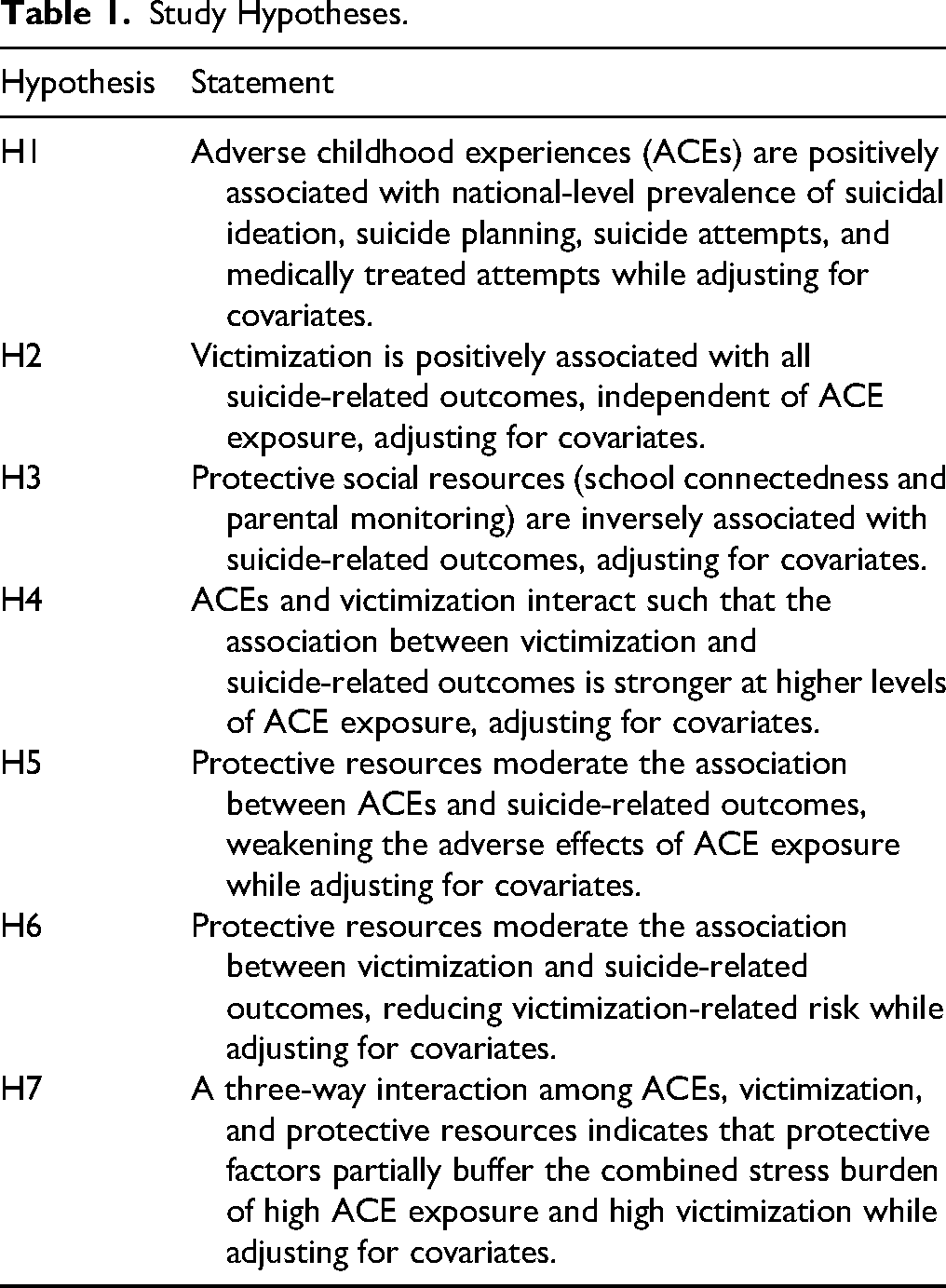
The framework further specifies a three-way interaction among ACEs, victimization, and protective resources (Table 1). This higher-order term reflects the proposition that protective assets may partially buffer the compounded burden of high early adversity and high victimization. However, consistent with cumulative stress theory, 24 buffering effects may attenuate under conditions of severe or multilayered stress exposure.
Study Hypotheses.
Recognizing that suicidal behaviors emerge within broader developmental systems, the model incorporates covariates representing proximal psychological distress (sadness/hopelessness, poor mental health), health-related behaviors (sleep duration ≥8 h), structural instability (unstable housing), and developmental stage (age 13 years). These factors capture concurrent emotional and contextual conditions that shape risk while allowing clearer estimation of primary and interactive stress effects.
Current Study
Figure 1 depicts this cumulative stress process: ACEs and victimization are modeled as primary exposures; protective social resources function as direct and moderating influences; and covariates represent concurrent psychological and structural conditions. The analytic strategy tests independent associations (H1–H3), two-way interactions among stressors and protective factors (H4–H6), and a three-way interaction reflecting cumulative stress buffering (H7), while adjusting for covariates (Table 1).
Together, this framework advances the view that adolescent suicidality reflects interacting stress processes embedded within relational and ecological systems. By examining both independent and synergistic associations using nationally aggregated YRBSS data, the study moves beyond single-factor explanations to test how layered adversity and protective resources jointly shape suicide-related outcomes.
Methods
Data Source and Study Design
This cross-sectional study used secondary data from the 2023 combined National Youth Risk Behavior Surveillance System (YRBSS), administered by the U.S. Centers for Disease Control and Prevention (CDC). The YRBSS combined datasets contain data from YRBS surveys conducted from 1991–2023 nationwide for the United States (N = 254,675) to increase analytic sample size and assess trend and patterns of behaviors among young people. 25 The purpose of the combined datasets is to facilitate YRBS data analyses that require data from multiple years and/or multiple surveys. The project is a biennial, school-based surveillance system established in 1991 to monitor health-related behaviors among U.S. high school students.
It employs a three-stage cluster sampling design (primary sampling units, schools, and classrooms) to generate nationally representative estimates. Students complete anonymous, self-administered questionnaires during a regular class period using standardized procedures to ensure comparability across survey cycles.
The combined dataset aggregates weighted prevalence estimates across participating jurisdictions. Accordingly, the unit of analysis in this study is at the national level, and all variables represent population-level percentages, rather than individual-level responses.
Ethical Considerations
This study used publicly available, de-identified secondary data and was therefore exempt from institutional review board review.
Measures
Outcome Variables: Suicide Behaviors
Four suicide-related outcomes were examined, each measured as the percentage of students in the participating US states reporting the behavior in the past 12 months: (1) seriously considering suicide/ ideation (`qn27`), (2) suicide planning (`qn28`), (3) suicide attempt (`qn29`), and (4) injurious suicide attempt requiring medical treatment (`qn30`). Consistent with best practices for bounded outcomes, all suicide variables were rescaled to proportions (0-1) prior to analysis.
Primary Exposure: Adverse Childhood Experiences (ACEs)
Guided by stress theory, 26 eight ACE indicators were included: parental emotional abuse, parental physical abuse, sexual abuse by an adult or older person, parental incarceration, adult intimate partner violence in the home, living with a parent/guardian with substance abuse, living with a parent/guardian with mental illness, and household difficulty meeting basic needs. Each ACE variable was measured as national-level prevalence percentage (%).
To capture cumulative childhood stress exposure, all ACE indicators were standardized (z-scores) and combined into a composite ACE index (`ace_index_z`) calculated as the mean of standardized items. Records with fewer than six non-missing ACE components were excluded from index construction to ensure measurement reliability.
Multidimensional Victimization
Victimization was conceptualized as a multidimensional stressor, encompassing physical bullying, cybervictimization, physical assault, sexual victimization, dating violence, race-based harassment, and neighborhood violence exposure. Eleven (11) indicators from the dataset were included, all measured as prevalence percentages. 25 Each variable was standardized and aggregated into a victimization index, representing cumulative exposure to interpersonal and environmental stressors.
Protective Factor
Two protective variables were examined: feeling close to people at school and parental monitoring. These variables reflect social and familial buffering resources relevant to chronic stress processes. Both indicators were standardized and combined into a protective index, calculated as the mean of standardized items when both components were available in the dataset.
Emotional and Mental Health Variables
Three indicators were included to account for proximal emotional and mental health states: persistent feelings of sadness or hopelessness, poor mental health in the past 30 days (including stress, anxiety, and depression), and adequate sleep (≥8 h on school nights). All were treated as continuous covariates.
Demographic and Housing Covariates
Models adjusted for national-level distributions of age, biological sex, sexual and gender identity, race/ethnicity, and unstable housing (percentage of students experiencing housing instability in the past 30 days). These variables were included to account for structural and compositional differences across the country.
Statistical Analysis
The combined 2023 YRBSS dataset is pre-weighted and standardized across survey years; therefore, no additional sampling weights were applied. 27 All analyses were conducted at the national level using Stata 19. 28
Descriptive statistics were generated to characterize study variables prior to modeling. For proportional outcomes (0-1), percentage variables (0-100), and standardized continuous indices (ACE, victimization, and protective indices), we reported means, standard deviations, medians, interquartile ranges, minimum–maximum values, and sample sizes (N). Frequencies and column percentages were calculated for categorical variables (age group, sex, transgender identity, and race/ethnicity). These summaries informed assessment of distributional properties and model specification.
Multicollinearity was evaluated using Spearman rank correlations (ρ). Given evidence of non-normality, suicide-related outcomes were modeled using fractional logistic regression estimated via generalized linear models with a logit link and quasi-binomial variance structure. 29 This approach was selected because outcomes were jurisdiction-level proportions bounded between 0 and 1, with no boundary mass, and because fractional logit accommodates such data without requiring strict distributional assumptions or exclusion of near-boundary values. Compared with beta regression, this method avoids sensitivity to boundary violations and provides consistent quasi-maximum likelihood estimates for aggregated surveillance data. Primary models simultaneously included ACEs, victimization, protective resources, emotional and mental health variables, and demographic and housing covariates for each suicide outcome.
Results are reported as average marginal effects (AMEs) with 95% confidence intervals, representing the change in the expected outcome proportion associated with a one-unit change in each predictor, holding other variables constant. Positive AMEs indicate increased expected prevalence, whereas negative AMEs indicate reduced prevalence. Robust (heteroskedasticity-consistent) standard errors were used for statistical inference. 29
Results
Descriptive Characteristics
Descriptive statistics for the analytic sample are summarized in Supplementary Table S1 for demographic characteristics and in Table 2 for continuous variables. The combined 2023 National YRBSS included over 250,000 adolescents, providing substantial variation in suicide-related behaviors, cumulative adversity, victimization, and protective resources at the national level. Suicide-related outcomes mean proportions range from 0.018 to 0.020 on a scale of 0–1 which is equivalent to 18%–20% on 0–100% scale. Standardized exposure indices demonstrated meaningful dispersion, indicating heterogeneity in adverse and protective experiences across the population. Emotional distress indicators, sleep duration, and housing instability showed moderate prevalence, consistent with prior national surveillance estimates (Table 2).
Descriptive Statistics of Suicide Behavior, Exposure Indices, and Emotional/Mental Health Variables.
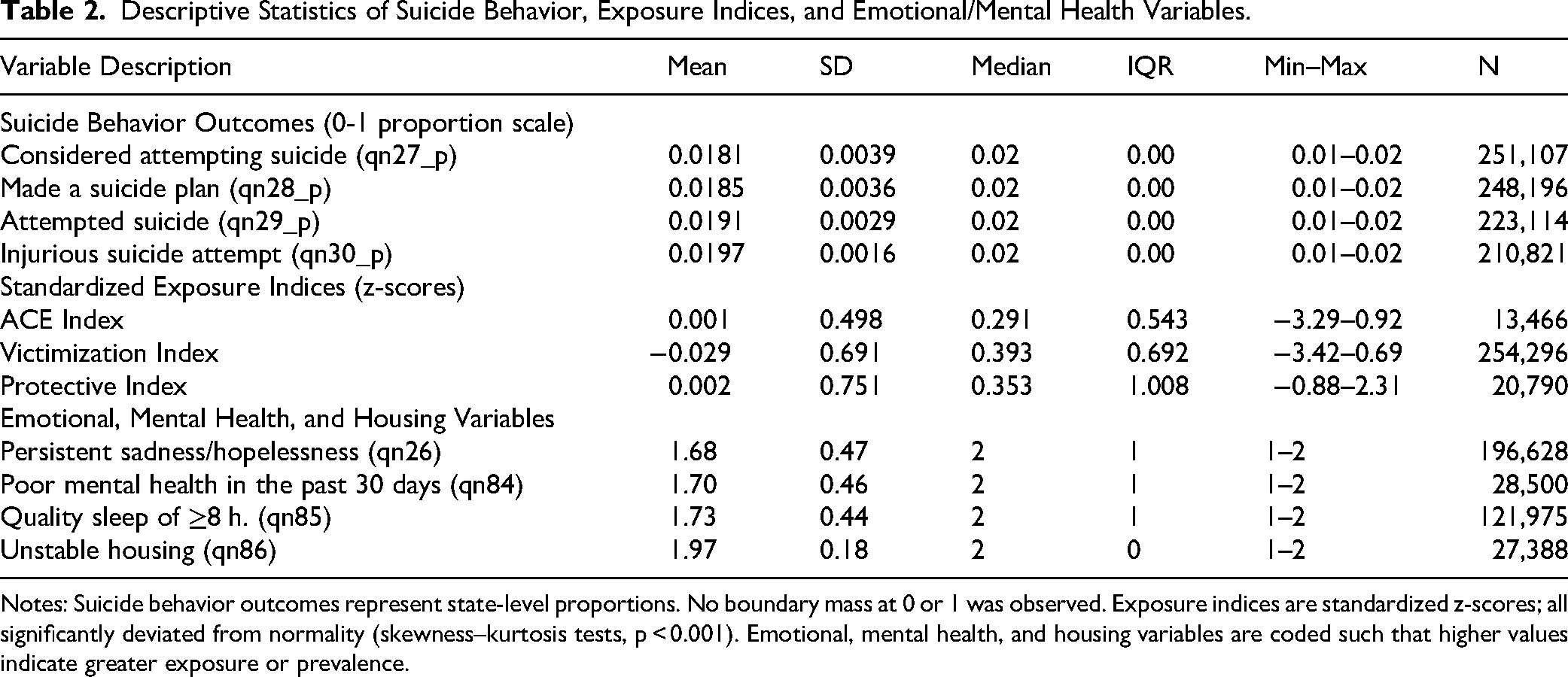
Notes: Suicide behavior outcomes represent state-level proportions. No boundary mass at 0 or 1 was observed. Exposure indices are standardized z-scores; all significantly deviated from normality (skewness–kurtosis tests, p < 0.001). Emotional, mental health, and housing variables are coded such that higher values indicate greater exposure or prevalence.
Correlations and Model Diagnostics
Spearman's rank correlations (Figure 2; Table S1) indicated moderate positive associations among suicide-related outcomes. Suicidal ideation was strongly correlated with suicide planning (ρ = 0.646) and moderately correlated with suicide attempts (ρ = 0.540), while injurious attempts showed weaker but positive correlations with ideation (ρ = 0.261) and attempts (ρ = 0.462). ACE exposure and victimization were moderately associated with suicidal ideation (ρ = 0.350 and ρ = 0.349, respectively) and planning (ρ = 0.315 and ρ = 0.325), whereas protective resources reduces ideation (ρ = −0.175) and planning (ρ = −0.164). Emotional distress demonstrated the strongest associations with suicide outcomes: persistent sadness/hopelessness correlated with ideation at ρ = 0.492 and planning at ρ = 0.425, and poor mental health correlated with ideation at ρ = 0.402. All correlations were below conventional multicollinearity thresholds (|ρ| < 0.70), supporting inclusion of all predictors in multivariable models. Distributional diagnostics confirmed significant non-normality of proportional outcomes and exposure indices (p < 0.001), justifying fractional logit estimation.
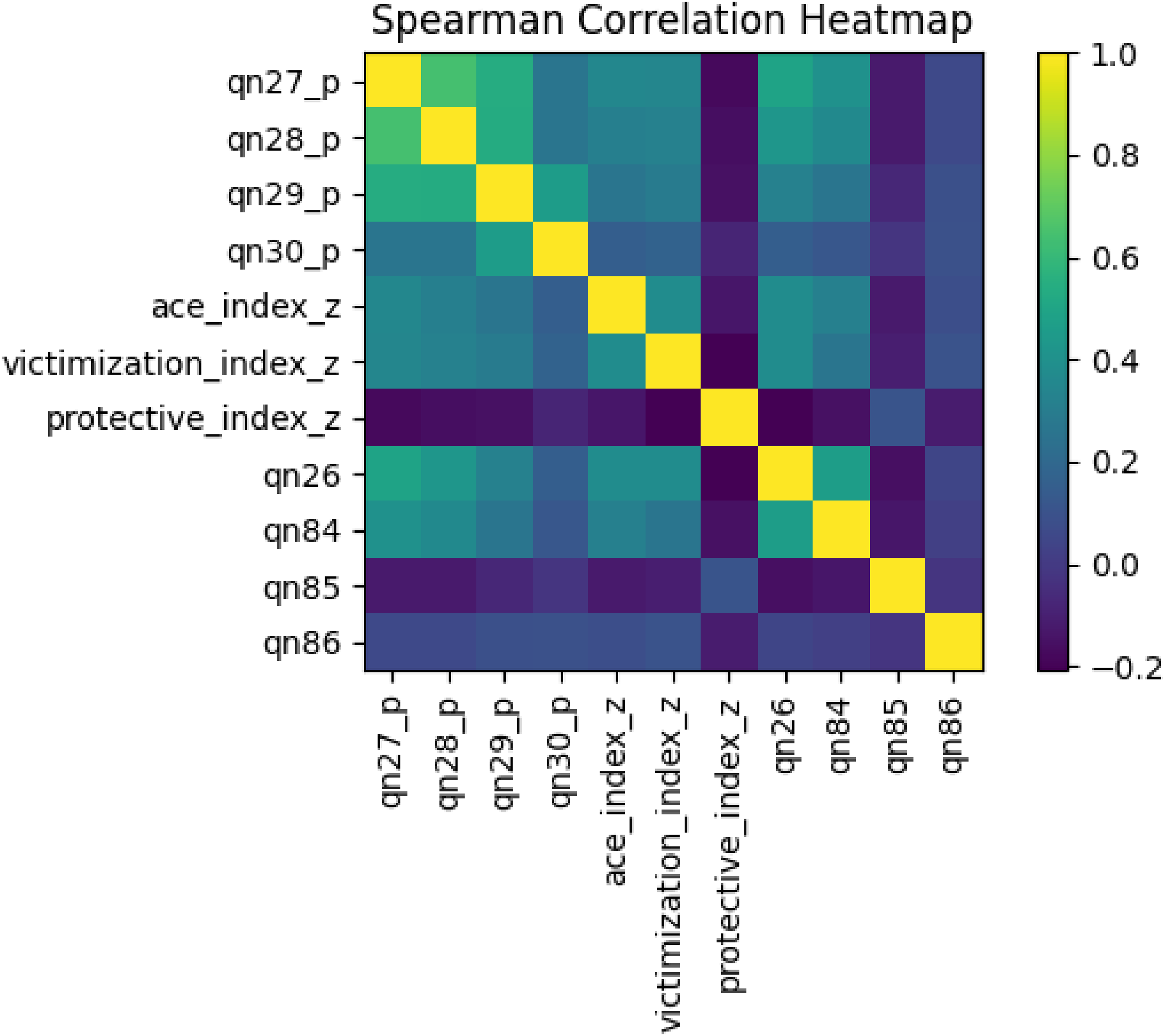
Spearman's correlation of nonnormality continuous variables*.
Fractional Logistic Model
Main Effects
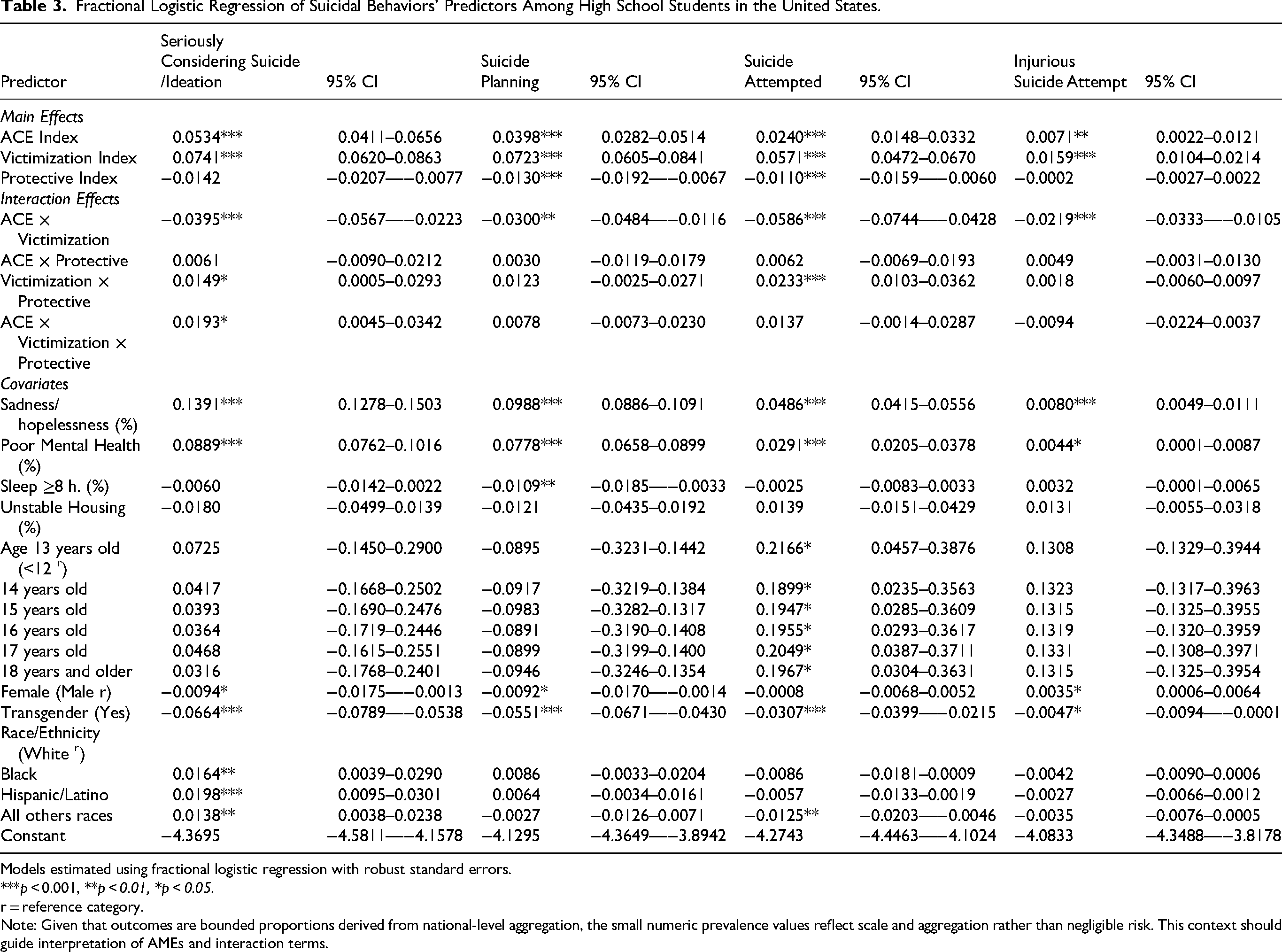
Fractional logit models (Table 3) revealed consistent positive associations between cumulative stress exposures and suicide-related outcomes. A one-unit increase in the ACE index was associated with higher proportions of suicidal ideation (average marginal effects (AME) = 0.0534, 95% CI [0.0411, 0.0656], p < 0.001), planning (AME = 0.0398, 95% CI [0.0282, 0.0514], p < 0.001), attempts (AME = 0.0240, 95% CI [0.0148, 0.0332], p < 0.001), and medically treated injurious attempts (AME = 0.0071, 95% CI [0.0022, 0.0121], p < 0.01). Victimization exhibited comparable or larger effects, particularly for planning (AME = 0.0723, 95% CI [0.0605, 0.0841], p < 0.001) and attempts (AME = 0.0571, 95% CI [0.0472, 0.0670], p < 0.001). Protective resources statistically reduces suicide planning (AME = −0.0130, 95% CI [−0.0192, −0.0067], p < 0.001) and attempts (AME = −0.0110, 95% CI [−0.0159, −0.0060], p < 0.001), though associations with ideation were smaller (AME = −0.0142, 95% CI [−0.0207, −0.0077]) and non-significant for injurious attempts.
Fractional Logistic Regression of Suicidal Behaviors’ Predictors Among High School Students in the United States.
Models estimated using fractional logistic regression with robust standard errors.
***p < 0.001, **p < 0.01, *p < 0.05.
r = reference category.
Note: Given that outcomes are bounded proportions derived from national-level aggregation, the small numeric prevalence values reflect scale and aggregation rather than negligible risk. This context should guide interpretation of AMEs and interaction terms.
Among covariates, persistent sadness/hopelessness showed the largest effect sizes across outcomes (eg, ideation AME = 0.1391, 95% CI [0.1278, 0.1503], p < 0.001), followed by poor mental health (ideation AME = 0.0889, 95% CI [0.0762, 0.1016], p < 0.001). Sleep of ≥8 h was inversely associated with planning (AME = −0.0109, 95% CI [−0.0185, −0.0033], p < 0.01), while unstable housing was not significantly associated with most outcomes.
Interaction Effects
Interaction analyses demonstrated that ACEs and victimization were not strictly additive. The ACE × victimization interaction was negative and significant for ideation (AME = −0.0395, 95% CI [−0.0567, −0.0223], p < 0.001), planning (AME = −0.0300, 95% CI [−0.0484, −0.0116], p < 0.01), attempts (AME = −0.0586, 95% CI [−0.0744, −0.0428], p < 0.001), and injurious attempts (AME = −0.0219, 95% CI [−0.0333, −0.0105], p < 0.001), suggesting diminishing marginal increases in suicide-related behaviors at higher combined stress levels. A significant three-way interaction among ACEs, victimization, and protective resources was observed for ideation (AME = 0.0193, 95% CI [0.0045, 0.0342], p < 0.05), indicating that protective factors conditioned the association between cumulative stress and suicidal ideation. However, similar three-way effects were not statistically significant for planning, attempts, or injurious attempts.
Demographic Patterns
Age was associated with suicide attempts but not consistently with ideation or planning. Compared with the youngest reference group, adolescents aged 13–18 years showed elevated associations with suicide attempts (eg, age 17: AME = 0.2049, 95% CI [0.0387, 0.3711], p < 0.05). Female sex was modestly associated with lower ideation (AME = −0.0094, p < 0.05) but higher injurious attempts (AME = 0.0035, p < 0.05). Transgender identity was significantly associated with higher suicide risk across all outcomes (eg, ideation AME = −0.0664, 95% CI [−0.0789, −0.0538], p < 0.001; note coding direction reflects comparison category). Racial and ethnic differences were statistically significant for select outcomes but smaller in magnitude than those associated with cumulative stress exposures.
Discussion
This study advances a unified chronic stress framework to explain how layered and interacting stress exposures shape adolescent suicide-related behaviors. Rather than treating early adversity, ongoing victimization, and protective social resources as separate theoretical domains, we conceptualize them as components of a cumulative stress system operating across development. Within this framework, adverse childhood experiences (ACEs) represent foundational stress load, victimization reflects contemporaneous stress activation during adolescence, and protective resources function as relational regulators that may recalibrate—but not eliminate—stress-related risk. Using nationally representative 2023 YRBSS data and fractional logit models, we found consistent evidence that suicidality reflects the accumulation and conditional interplay of these stress processes.
Cumulative Stress Exposure and Suicide-Related Outcomes
ACEs were positively associated with suicidal ideation, planning, attempts, and injurious attempts, even after adjusting for emotional distress and contextual covariates. These findings are consistent with research showing that early adversity produces enduring dysregulation in affective, cognitive, and physiological systems, increasing vulnerability to later psychopathology and self-harm.30–32 The persistence of ACE effects net of current sadness and poor mental health suggests that early stress becomes biologically and psychologically embedded, shaping risk trajectories beyond proximal symptomatology.
Victimization independently predicted all suicide-related outcomes, with particularly pronounced associations for planning and attempts. Within a chronic stress framework, ongoing interpersonal stressors—such as bullying, harassment, and violence—can activate sensitized stress systems and escalate ideation into behavioral enactment during a developmentally vulnerable period. 26 These findings indicate that adolescent suicidality cannot be reduced to either distal adversity or immediate stressors alone; instead, it reflects layered exposure across time.
Interaction of ACEs and Victimization: Nonlinear Accumulation
A central contribution of this study is the identification of significant interaction effects between ACEs and victimization. The negative interaction terms indicate that the incremental effect of one stressor is smaller when the other is already high. Importantly, this does not imply reduced overall risk at high exposure levels. Rather, it suggests a nonlinear accumulation pattern in which adolescents exposed to extreme cumulative adversity may already be operating at elevated baseline risk, leaving less marginal increase detectable statistically. Such patterns are consistent with stress saturation or ceiling effects observed in chronic stress research.32,33
Protective Resources as Conditional Regulators
Protective social resources—school connectedness and parental monitoring—were inversely associated with suicide-related outcomes, particularly ideation and planning. Supportive relational environments are thought to enhance emotion regulation, foster belonging, and dampen stress reactivity under chronic strain.34,35 However, the magnitude of protective effects was smaller than that of ACEs and victimization, indicating that protection may reduce—but not fully counteract—entrenched stress exposure.
Moderation analyses further demonstrated that buffering effects were conditional and outcome specific. Protective resources attenuated some associations between cumulative stress and suicidality, and a significant three-way interaction for ideation suggested partial buffering under compounded stress. However, such buffering was limited for suicide attempts and injurious attempts. Within a cumulative stress framework, this pattern suggests that relational protection may be most influential earlier along the suicidality continuum, when cognitive and emotional processes remain more malleable. As stress becomes entrenched and behaviors progress toward enactment, buffering capacity may diminish.5,36,37
Developmental and Social Patterning
Age patterns indicated greater likelihood of attempts and injurious attempts among older adolescents, even when ideation differences were less pronounced. This aligns with developmental evidence suggesting that progression from ideation to action may increase with age due to greater autonomy, opportunity, and acquired capability.38,39
Pronounced disparities by gender identity were also observed, with transgender youth exhibiting elevated risk across outcomes. These findings are consistent with evidence that stigma, discrimination, and structural exclusion contribute to sustained stress burden among gender-diverse adolescents.25,40–42 Racial and ethnic differences were more modest but remained evident for select outcomes, underscoring how structural inequities shape exposure, vulnerability, and access to protective resources.43,44 Together, these demographic patterns reinforce that chronic stress operates within broader social and structural contexts.
Study Implications
The findings suggest that prevention strategies focused narrowly on a single domain—such as bullying prevention alone or depression screening alone—are unlikely to substantially reduce suicide risk.45,46 A cumulative stress perspective instead supports multilevel interventions that simultaneously (1) reduce early adversity, (2) interrupt ongoing victimization, and (3) strengthen protective relational systems. Trauma-informed school and community approaches integrating mental health services, peer connectedness, family engagement, and structural supports may be particularly effective in disrupting chronic stress pathways before they culminate in suicidal behavior.5,38,39,47
Limitations and Strengths
Several limitations warrant consideration. The cross-sectional design precludes causal inference and limits direct examination of temporal stress accumulation. Protective resources were measured using a limited set of available indicators, potentially underestimating the breadth of buffering influences. Additionally, the 2023 YRBSS does not include all states, and harmonization to the updated questionnaire introduces variable-specific missingness. 39 Despite these limitations, this study leverages a large, nationally representative dataset and applies fractional logit modeling appropriate for proportional outcomes, strengthening confidence in the observed patterns.
In conclusion, this study demonstrates that adolescent suicidality is best understood as the product of cumulative and interacting stress exposures rather than isolated risk factors. Early adversity establishes foundational stress load, ongoing victimization activates and compounds that burden, and protective resources condition—but do not eliminate—risk. By situating all findings within a unified chronic stress framework, the results underscore the necessity of early, sustained, and multidimensional prevention strategies to reduce suicide-related behaviors among adolescents.
Supplemental Material
sj-docx-1-css-10.1177_24705470261437060 - Supplemental material for When Stress Accumulates: Interacting Effects of Childhood Adversity, Multidimensional Victimization, and Protective Resources on Adolescent Suicidal Behaviors
Supplemental material, sj-docx-1-css-10.1177_24705470261437060 for When Stress Accumulates: Interacting Effects of Childhood Adversity, Multidimensional Victimization, and Protective Resources on Adolescent Suicidal Behaviors by Omowunmi Iyanda and Ayodeji E. Iyanda in Chronic Stress
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.