
Abstract
Background
Displacement caused by the Russian invasion of Ukraine has subjected millions of Ukrainians to forced displacement, migration, exposing them not only to direct war-related trauma but also to substantial post-displacement stress. Refugees face disrupted employment, residential instability, and ongoing uncertainty in host countries. While prevalence of stress-related disorders is well established, less is known about how war-related stress and life satisfaction evolve over time in this population.
Methods
A longitudinal cohort study was conducted among Ukrainian refugees in Germany. The analytic sample comprised 164 participants who completed at least two of five survey waves over a six-month period (September 2022–March 2023). Post-traumatic stress symptoms were assessed with the Posttraumatic Symptom Scale at each wave and validated against the Impact of Event Scale – Revised at baseline and follow-up. Life satisfaction was assessed with the Satisfaction With Life Scale. Distinct adjustment patterns were identified through group-based multi-trajectory modelling. Descriptive statistics, group comparisons, and linear mixed-effects modelling were additionally used to contextualize data.
Results
Multi-trajectory analysis yielded four main groups: persistently high stress with poor satisfaction with life; broadly diverse, but stable profiles; stress reduction without parallel gains in life satisfaction; and combined stress reduction with later improvements in life satisfaction. More favourable courses were associated with younger age, higher education, urban residence, and prior public-sector employment. Across the full sample, post-traumatic stress symptoms declined sharply over time, with the proportion meeting the cutoff for probable PTSD decreasing, whereas mean life satisfaction remained low and showed no systematic change.
Conclusion
Adjustment following war-related displacement is highly heterogeneous. Although acute symptoms of traumatic stress tended to subside, life satisfaction showed little recovery, underscoring a divergence between symptom relief and overall well-being. Patterns of adaptation were shaped not only by individual resources but also by structural constraints such as job loss and residential downgrading. Interventions for displaced populations should therefore address both clinical needs and socioeconomic integration to enable sustainable recovery of refugees.
Keywords
Introduction
The ongoing war in Ukraine has set in motion a massive wave of refugees worldwide. The psychological burden of forced migration must be considered on par with the direct consequences of armed hostilities. Many refugees were exposed to air raids, bombings, artillery fire, and continuous hostilities before leaving Ukraine. 1 However war-related stressors do not end upon relocation. Difficulties in securing housing, and coping with an uncertain future may compound pre-existing trauma. 2 Refugees also face ongoing insecurity about their personal prospects and the future of their country. 3 Displaced populations are therefore subjected to a sequence of stressors – before, during, and after displacement.
Post-migration environments frequently introduce new forms of strain, including family separation, loss of social and cultural continuity, language barriers, restricted access to childcare and education, housing instability, and prolonged uncertainty regarding employment and legal status.4,5 Evidence from refugee populations in high-income host countries suggests that these stressors may function as chronic, sustaining post-traumatic stress symptoms and limiting recovery. 6 Even among relatively young and highly educated refugees, occupational downgrading, poor job quality, and mismatches between qualifications and available employment have been associated with lower mental health and reduced well-being. 7 Empirical studies further indicate that forced residential mobility, insecure working conditions, and erosion of social support networks are linked to higher rates of psychiatric disorders and persistent post-traumatic stress. Taken together, these findings support conceptualising refugee trauma as a dynamic and cumulative process, in which post-migration difficulties constitute an extension of traumatic exposure and may impede psychological adjustment long after physical safety has been achieved.
According to the DSM-5, indirect trauma exposure is narrowly defined and includes learning that a traumatic event occurred to a family member or friend, as well as exposure to aversive details of traumatic events in the course of professional duties, while excluding exposure through media or images. 8 Despite these diagnostic constraints, the contribution of indirect and cumulative traumatic experiences to PTSD symptom development remains debated. Recent evidence indicates that cumulative exposure to both direct and indirect large-scale traumatic events heightens PTSD risk.9,10 This indicates that even those who fled outside immediate combat zones may develop symptoms of post-traumatic stress disorder (PTSD).9,11 For instance, indirect experiences, such as repeated viewing of violent media coverage or hearing accounts of atrocities, may also provoke trauma responses.2,12 Evidence from multiple conflicts highlights its enduring mental health consequences. In State of Israel, following the October 2023 attacks, 13 Syrian Arab Republic, 14 Republic of Sierra Leone 15 and Republic of Kosovo. 16
In Ukraine, recent surveys indicate substantial psychological morbidity linked to prolonged traumatic stress. Serdiuk et al (2025) 17 reported that nearly one quarter of youth and young adults met diagnostic criteria for PTSD during the Russian invasion, while Lotzin et al (2023) 18 estimated a comparable pooled prevalence of complex PTSD. Additional assessments conducted at six and eight months after the outbreak of war likewise indicated persistently high levels of psychological distress,19,20 with similar prevalence rates of clinically significant symptoms reported in subsequent surveys in 2023 and 2024.21,22 Together, these findings suggest that war-related psychological distress among Ukrainians is not limited to the immediate aftermath of traumatic events but may persist over extended periods. Evidence from other chronic conflict contexts, such as Palestine, likewise indicates that repeated exposure substantially heightens long-term risk. 23 These dynamics require conceptualising trauma as cumulative and ongoing, rather than as an isolated or episodic event. 10
Consistent with this view, longitudinal research has demonstrated considerable heterogeneity in post-traumatic stress trajectories. For example, Brier et al (2020) 24 identified four common patterns – low and decreasing, rapid decreasing, slow decreasing, and persistently high symptoms – highlighting the importance of early symptom profiles for subsequent psychological and functional outcomes. Studies among refugee populations similarly suggest that initial symptom severity differentiates trajectories that tend to persist over time despite an overall tendency toward symptom reduction.25,26 Importantly, these studies also indicate that trajectories of well-being may diverge from symptom trajectories and are shaped by contextual and sociodemographic factors, including age, gender, social support, and resettlement conditions. 27
Despite this growing body of work, as Zasiekina et al (2025) 28 note, relatively few studies have examined how symptoms unfold during ongoing wars compared with post-conflict contexts. This study addresses this gap by examining longitudinal changes in post-traumatic stress symptoms and life satisfaction among Ukrainian refugees, who were displaced during the initial stages of the full-scale war and resided in Germany during the first six months following displacement. Specifically, the study aims to identify symptom trajectories and to describe their associations with sociodemographic characteristics of the study sample.
Methods
Study Design
Data for the present study were collected over a six-month period beginning on 21 September 2022, across five measurement waves among refugees in Germany. Participants were recruited through in-person presentations at state-funded integration courses for Ukrainian refugees in several cities in Upper Franconia, as well as through the distribution of study information at Tafel food distribution points. To extend recruitment beyond the regional context, official requests were sent from the University of Bayreuth to refugee support organisations across Germany, followed by the dissemination of information flyers and posters. Data was collected online using the Tivian Unipark survey platform.
A total of 584 Ukrainian refugees completed the baseline survey. Of these, 164 participants completed at least two measurement waves and were therefore included in the longitudinal analyses (Table 1), as repeated observations were required for model estimation. Because participants with only a single observation provide no information on change over time, imputing longitudinal trajectories from baseline-only data was not considered methodologically reasonable. Reasons for attrition across subsequent waves were not systematically collected. Attrition was examined by comparing baseline characteristics of participants retained in the longitudinal sample with those completing only the baseline assessment (see Supplementary 1). Differences were observed for several sociodemographic variables, whereas baseline post-traumatic stress symptoms and life satisfaction did not differ between groups.
Data Collection Schedule.

Note. Wave intervals indicate time elapsed since the previous data collection point. Cumulative time is calculated from the initial wave. Respondent numbers reflect participants who provided valid data in at least two waves.
Eligibility criteria required participants to be aged 18 years or older and to have resided in Ukraine up to February 2022. Completion of demographic items was mandatory, resulting in a full demographic dataset. Follow-up was conducted at each wave, with participants recontacted via email. The study design was approved by the University of Bayreuth Ethics Committee (approval no. 22-2022) on August 24, 2022. Written informed consent was obtained from all respondents for participation in the study, collection of personal information, and publication of anonymised health-related data in this article and in a data repository. 29
Potential sources of bias included attrition across survey waves and reliance on self-reported measures. All outcomes were assessed using validated Ukrainian versions of standardised scales, reducing measurement error, although self-report bias cannot be excluded. The study was conducted and reported in accordance with the STROBE guidelines for observational studies and the GROLTS recommendations for longitudinal trajectory research; completed checklists are provided in Supplementary 2 and 3.
Measures
Displacement-Related Stressors
Changes in residential location and professional status were treated as indicators of displacement-related stressors arising in the context of forced displacement. In particular, relocation to less urbanised settings and transitions into unemployment were considered markers of increased post-relocation socioeconomic strain. These indicators were derived from self-reported pre- and post-relocation status and were used to characterise heterogeneity in exposure to stressors associated with the relocation process.
Post-Traumatic Stress Symptoms
Overall severity of post-traumatic stress was assessed using the Posttraumatic Symptom Scale (PTSS-10), 30 comprising 10 items rated on a 7-point Likert scale. Higher total scores indicate greater severity of trauma-related symptoms. A total score exceeding 35 was applied as the cut-off for probable PTSD. 31 This PTSS-10 was originally developed in accordance with DSM-III-R diagnostic criteria; its criterion validity has been supported against DSM-5 diagnostic interviews. 31 The Ukrainian adaptation employed in this study demonstrated acceptable psychometric properties across all waves (ω = .60-.87, α = .58-.87, item–total correlations r = .11-.41), reflecting the heterogeneous symptom content of the brief screening measure and with a modest decline in reliability indices at later waves, consistent with increasing attrition and reduced variability over time.
Specific symptom clusters were assessed using the Impact of Event Scale – Revised (IES-R), 32 which consists of 22 items rated on a 5-point Likert scale. The IES-R measures three core symptom domains – intrusion, avoidance, and hyperarousal – as conceptualised within the DSM-IV framework. Although partial correspondence with DSM-5 symptom criteria has been discussed in recent work (Chang et al, 2024), the original three-factor structure was retained in the present study to ensure comparability. The Ukrainian version used in this study, validated by Krupelnytska et al (2025), 33 demonstrated satisfactory psychometric properties for total scores (ω = .92, α = .91) and satisfactory reliability for the subscales (ω = .75-.84, α = .75-.84). A total score exceeding 30 was applied as the cut-off for probable PTSD. 33 Respondents were instructed to rate their symptoms with reference to a predefined index event, operationalised in this study as the experience of ‘active hostilities in Ukraine’.
The PTSS-10 was used exclusively for longitudinal analyses, as it was administered at all waves and provided consistent measurement (Table 1). The IES-R, conceptually aligned with the PTSS-10, 33 but offering multidimensional traumatic stress profiles, was used as an external validity reference for trajectory classification and as the primary outcome for descriptive and comparative analyses.
Life Satisfaction
Life satisfaction was assessed using the Satisfaction With Life Scale (SWLS), 34 which comprises 5 items, each rated on a 7-point Likert scale. Higher total score values indicate greater life satisfaction, with scores below 20 indicate low life satisfaction, encompassing the slightly to extremely dissatisfied categories. The Ukrainian adaptation employed in this study demonstrated acceptable internal consistency across all the waves (ω = .72-.78; α = .71-.77; item–total correlations r = .32-.43).
Data Analysis
Analyses were conducted in R (4.5.1, 2025-06-13) on macOS Tahoe 26.0. Descriptive statistics summarised sociodemographic characteristics and psychological measures for the full sample and for subgroups identified via trajectory modelling. All quantitative variables were analysed in their original continuous form without scaling or standardisation. Categorial groupings were created only where required for descriptive or inferential comparisons.
Group differences were tested using Pearson's chi-squared test, Fisher's exact test with Monte Carlo simulation and effect sizes estimated using Cramér's V, non-parametric tests with Bonferroni-adjusted post hoc procedures and effect sizes reported as η2. Potential confounding by age, gender, and education was examined descriptively. Within-person change was examined using linear mixed-effects models with random-intercept and random-slopes, linear and quadratic time effects. Models were estimated using maximum likelihood, allowing all available observations to contribute to estimation without imputing missing outcomes. Competing models were compared by likelihood-ratio tests.
Group-based multi-trajectory modelling (GBMTM) was employed to identify distinct trajectories of post-traumatic stress symptoms and life satisfaction. PTSD symptoms and life satisfaction were modelled jointly using group-based multi-trajectory modelling with shared class membership. This approach assumes that individuals follow coherent adjustment patterns across both outcomes and allows the identification of subgroups characterised by combined mental health profiles.
Analyses were conducted using the gbmt R package, 35 which estimates multiple continuous outcome trajectories with shared latent class membership. Time was modelled as a continuous variable, coded 0-4, and outcomes were retained in unstandardised form. Estimation was performed using maximum likelihood, with missing outcome data handled via full information maximum likelihood. No imputation was applied, as trajectory estimation relied on available repeated measures and attrition was not assumed to be completely random.
While GBTM is typically recommended for larger samples (eg, N > 500), 36 our approach is supported by evidence showing that maximum likelihood estimation can perform adequately with smaller samples when model specification and class separation are appropriate. 37
Multiple specifications were estimated varying group numbers, degrees and scaling; full results are available in the data repository. 29 To identify the optimal number of latent trajectory groups, we estimated a series of GBMTM models specifying between two and six classes. Model selection was guided by Bayesian Information Criterion and Akaike Information Criterion, following recommendations of Lu (2024). 38 Model adequacy was assessed against established thresholds: average posterior probability ≥ .70, odds of correct classification ≥ 5, and narrow confidence intervals with preferred width of .20. 39 The five-class model was selected as the most parsimonious solution that met established fit and classification criteria. Up to five latent trajectory groups were specified (ng = 5), with time effects modelled using polynomial terms up to degree four (d = 4) to capture potential non-linear trends. Scaling was set to 4, and pruning was disabled to retain all specified groups. No covariates were included in either the trajectory or class membership models. Trajectory group membership was assigned based on the highest posterior probability from the unconditional GBMTM model. Annotated scripts, generated datasets, and detailed subgroup classification criteria are available in the data repository. 29
Results
Sample Characteristics
The sample was predominantly composed of women, accounting for 70.6% (n = 122) of participants. The majority of them fell within the 31-45 year age bracket (Figure 1). The educational attainment of the sample was relatively high, with 73.8% having completed at least a bachelor's degree or higher. Furthermore, respondents were predominantly urban residents, comprising 92.7% of the overall sample. The demographic profile of respondents is presented in Table 2.

Heatmap of sociodemographic composition of the sample. Note. M denotes the number of respondents identified as men; W denotes the number of respondents identified as women.
Sociodemographic Characteristics of the Sample.

Note. Values are reported as frequency (n) and percentage (%). All data reflect self-reported characteristics. “Other (Unspecified)” includes missing or refused responses. Pre- and post-relocation characteristics refer to the same respondents. Percentages may not total 100% due to rounding.
To characterise displacement-related circumstances, residential location and professional status were assessed before and after relocation. Residential transitions following displacement were relatively balanced (Figure 2). Specifically, 30.5% of respondents (n = 50) relocated to settlements with lower urban status (eg, from a large city to a small town or rural area), while 32.9% (n = 54) moved toward more urbanized environments. The remaining 36.6% (n = 60) experienced no change in settlement type following relocation. Indicators of distributional inequality exhibited only marginal variation following relocation, with the Gini coefficient increasing from .16 to .17, Shannon entropy rising from 1.15 to 1.26, and Blau's index from .62 to .69. These minor shifts suggest limited change in the heterogeneity of residential status within the sample.

Alluvial diagram of residential transitions.
In contrast, changes in professional status reflected pronounced occupational disruption (Figure 3). The most common outcome was job loss following displacement, affecting 57.9% of respondents (n = 95). Occupational redirection beyond unemployment was limited. A small proportion of individuals formerly employed in the private sector moved into other industries (10.4%, n = 17), while retention of the original occupational status was uncommon (1.8%, n = 3). Similarly, participants from the public sector and entrepreneurial backgrounds exhibited limited occupational mobility, with fewer than 3% entering new employment sectors or educational programs. Individuals who were students (11.6%, n = 19), previously unemployed (3.7%, n = 6), or retired (7.3%, n = 12) largely maintained their pre-relocation statuses. The Gini coefficient declined from .26 to .17, indicating a reduction in inequality. Additionally, both Shannon entropy (from 1.65 to 1.29) and Blau's index (from .76 to .62) decreased, reflecting a contraction in the overall diversity of occupational statuses following displacement.

Alluvial diagram of professional status transitions.
Cross-Sectional Differences
Job loss, involuntary industry shifts, and relocation to less urbanised areas were treated as displacement-related stressors, reflecting adverse socioeconomic consequences of forced relocation (Table 3). Cross-tabulation showed that relocation to less urbanised areas was frequently accompanied by job loss (65.8%, n = 52). Among those who remained in the same type of residential area, 55.0% (n = 33) reported job loss, with a notably higher proportion maintaining their pre-relocation professional status (31.7%, n = 19) compared to those who moved to less urbanised areas (13.9%, n = 11). Patterns of occupational shifts also varied: 20.3% (n = 16) of downward movers experienced lateral changes in employment (eg, sector or industry shifts), compared to 13.3% (n = 8) among those with no residential change. Respondents who relocated to more urbanised areas had the lowest rate of job loss (40.0%, n = 10), and comparatively higher rates of lateral shifts (28.0%, n = 7) and occupational continuity (32.0%, n = 8), despite representing the smallest proportion of the sample. An association between residential direction and occupational outcome was observed (χ2(4) = 10.11, P = .039), confirmed by Fisher's exact test (P = .031).
Characteristics of Respondents Exposed to Relocation-Related Stressors.

Note. Values represent frequencies (n) and percentages (%), or means (M) and standard deviations (SD), as indicated. Percentages may not total 100% due to rounding.
Older age was associated with lower odds of in-field employment. Specifically, individuals aged 31-45 (b = −2.83, SE = .85, OR = .06, 95% CI [.01; .29]) and 46-60 (b = −1.83, SE = .93, OR = .16, 95% CI [.03; .88]) were less likely to retain their pre-relocation professional status compared to those under 30. Gender also emerged as a significant predictor, with women exhibiting substantially lower odds of occupational retention relative to men (b = −2.07, SE = .70, OR = .13, 95% CI [.03; .50]).
Significant differences in post-traumatic stress symptoms were observed across respondents exposed to displacement-related stressors. A Kruskal–Wallis test indicated that IES-R scores varied significantly by professional status transition following displacement (χ2(2) = 9.43, P = .008). Post hoc pairwise comparisons with Bonferroni correction indicated that individuals who retained their pre-relocation professional status reported significantly lower symptoms severity (M = 44.6, SD = 13.7) compared to those who experienced job loss (M = 51.2, SD = 10.2, P = .005), a pattern illustrated in Figure 4. Significant group differences also emerged for intrusion (χ2(2) = 11.77, P = .003) and avoidance (χ2(2) = 12.37, P = .002) symptom clusters. In both cases, participants employed in their original field post-relocation reported lower scores than those who became unemployed (P = .002). No significant differences were found for hyperarousal symptoms (χ2(2) = 5.75, P = .056), nor between those who changed professional fields and other groups.
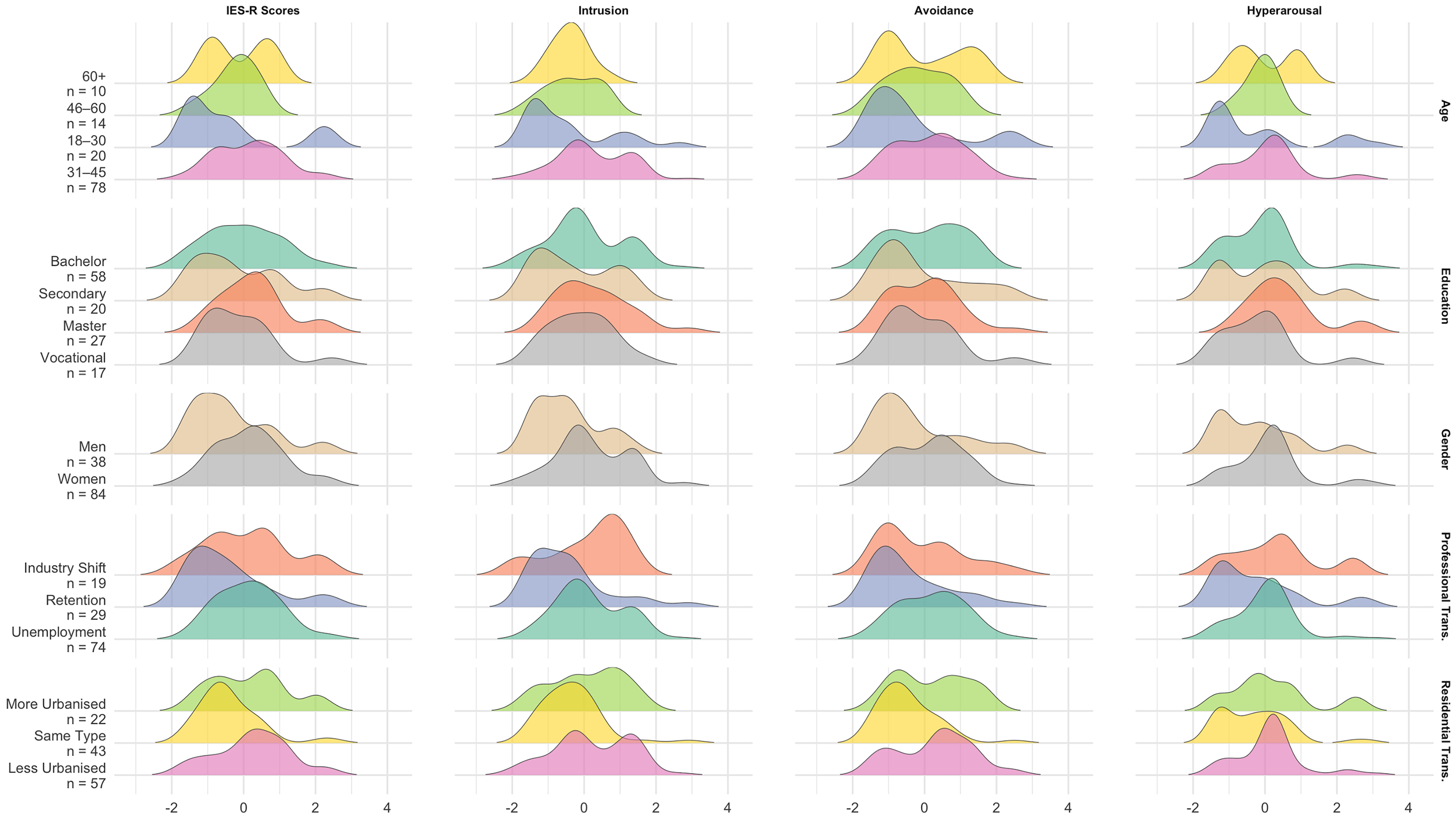
Density ridgeline plots of cross-sectional comparison of post-traumatic stress symptoms.
A similar pattern emerged with regard to residential transition. Total IES-R scores differed significantly by post-displacement settlement type (χ2(2) = 12.41, P = .002), with higher symptom levels reported by those who relocated to less urbanised areas (M = 52.5, SD = 12.1) compared to those whose settlement type remained unchanged (M = 44.8, SD = 10.1, P = .002). This trend was especially pronounced in intrusion (χ2(2) = 8.67, P = .013) and avoidance (χ2(2) = 14.40, P < .001) symptoms. Post hoc comparisons confirming elevated scores on both (P = .014, P > .001, respectively).
Sociodemographic variables were associated with variation in posttraumatic stress symptoms. Women reported significantly higher total IES-R scores (M = 51.5, SD = 11.2) than men (M = 45.3, SD = 12.7; P = .004), as well as higher intrusion (P < .001), avoidance (P = .016), and hyperarousal (P = .017). Age differences in total IES-R scores reached significance (χ2(3) = 8.13, P = .043), with respondents under 30 tending to report lower symptoms, although this did not survive Bonferroni correction. A similar trend was observed for intrusion (χ2(3) = 14.81, P = .002), which remained significant after adjustment. Avoidance approached significance (χ2(3) = 7.17, P = .067), while no age-related differences were observed for hyperarousal (χ2(3) = 4.81, P = .186). Educational attainment was not significantly associated with total IES-R scores (χ2(4) = 4.52, P = .341). Subscale analyses revealed no significant differences for intrusion (χ2(4) = 3.94, P = .415) or avoidance (χ2(4) = 3.54, P = .471). Hyperarousal varied modestly (χ2(4) = 9.94, P = .041), but no pairwise comparisons survived correction.
Within-Person Changes
The unconditional random-intercept model indicated that the baseline mean score for PTSS-10 was 29.09 (SE = .50), which was slightly below the diagnostic cutoff. Nevertheless, at baseline, 68.9% of participants (n = 113) met the cutoff for probable PTSD according to the PTSS-10. The proportion of participants meeting this criterion decreased markedly over time, with only 4.9% meeting the cutoff at the final assessment wave (n = 6). Between-person variance was 22.44 (SD = 4.74), and within-person variance was 75.50 (SD = 8.69), yielding an intraclass correlation coefficient (ICC) of .23. Thus, the majority of variation in PTSS-10 scores reflected fluctuations within individuals across waves rather than stable between-individual differences. For SWLS, the baseline mean score was 17.21 (SE = .28), with between-person variance of 10.30 (SD = 3.21) and within-person variance of 11.52 (SD = 3.39), corresponding to an ICC of .47. In this case, approximately half of the total variance was attributable to stable individual differences, pointing to greater stability in SWLS scores relative to PTSS-10 scores.
Introducing a quadratic time term improved model fit relative to the linear specification (χ2(1) = 68.22, P < .001), with lower AIC and BIC values. The model capture a steep early linear decline in PTSS-10 scores (b = −8.38, SE = .55, t = −15.20, P < .001) followed by a small but significant quadratic deceleration (b = 1.16, SE = .13, t = 8.63, P < .001). In contrast, SWLS showed no significant temporal change. The linear time effect was small and non-significant in both the random-intercept model (b = −.12, SE = .09, t = −1.28, P = .202) and the random-slope model (b = −.12, SE = .12, t = −1.03, P = .303). Slope variance was modest (σ2 = .87, SD = .93), with a weak negative correlation (r = −.24) between slopes and intercepts. Quadratic time terms were also non-significant (b = .14, SE = .30, t = .46, P = .64; b = −.07, SE = .07, t = −.94, P = .35), and model fit did not improve. Variance estimates remained stable across SWLS models.
Overall, these findings indicate pronounced within-person reductions in PTSS-10 scores across the study period, best captured by a curvilinear trajectory with steep initial decreases followed by modest levelling-off (Figure 5). By contrast, life satisfaction remained largely stable, with substantial between-person differences but no systematic linear or quadratic trends over time (Figure 6).
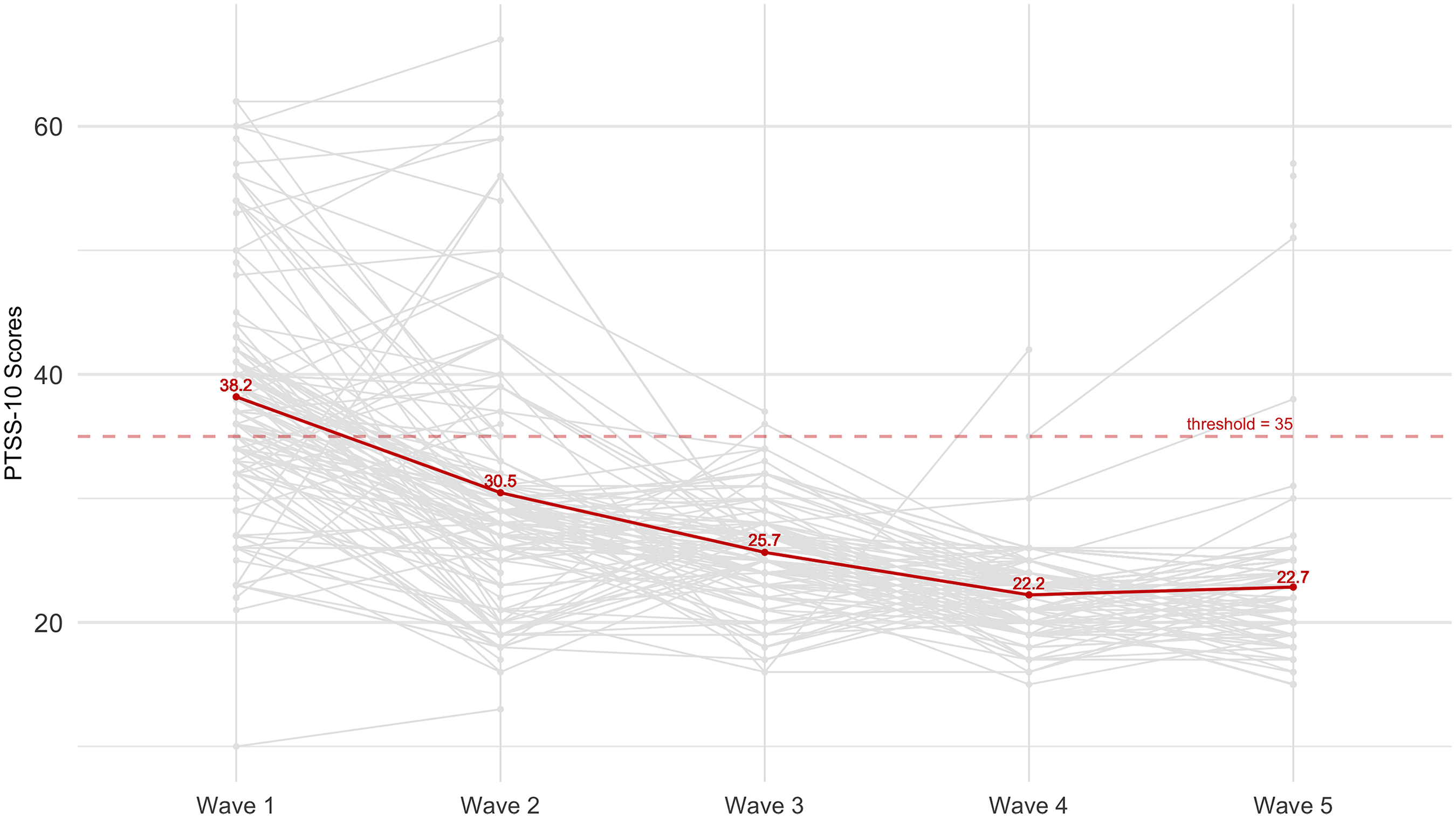
Spaghetti plot of individual trajectories of post-traumatic stress symptoms. Note. The red solid line represents the sample mean; the red dashed line indicates the clinical threshold for probable PTSD based on PTSS-10 scores; grey lines depict individual respondents’ changes in traumatic stress over time.

Spaghetti plot of individual trajectories of life satisfaction. Note. The green line indicates mean values for the overall sample at each wave; grey lines depict individual trajectories; the red dashed line marks interpretation thresholds.
Longitudinal Trajectories
Five distinct longitudinal trajectories of post-traumatic stress symptoms and life satisfaction were identified (Figure 7). Classification quality was excellent, with average posterior probabilities ranging from .91 to 1.00, narrow confidence intervals (.055-.095), and odds of correct classification well above conventional thresholds. The smallest class, Group 5 (2.4%, n = 4) displayed extreme non-linear change, with a pronounced early decline in PTSS and strong shifts in SWLS scores. Given its negligible size, Group 5 was excluded from inferential group comparisons to avoid unreliable inference. Table 4 provides an overview of group characteristics and between-trajectory comparisons.

Estimated trajectories from group-based multi-trajectory modelling.
Sociodemographic Characteristics of Groups Identified Through Multi-Trajectory Modelling.

Note. Values represent frequencies (n) and percentages (%), or means (M) and standard deviations (SD), as indicated. “Other (Unspecified)” includes missing or refused responses. Percentages may not total 100% due to rounding. Group 5 was excluded from between-group comparisons due to insufficient sample size (<5% of the total sample).
Group 1 (13.4%, n = 22) was characterised by persistently low PTSS-10 and SWLS scores with modest non-linear fluctuations. Demographically, members were disproportionately represented among PhD holders (18.2%, padj = .043) and were less likely to reside in large cities following relocation (4.5%, padj = .005). Professionally, they were over-represented in “Other (unspecified)” category prior to relocation (31.8%, padj < .001) and in in-field employment after relocation (18.2%, padj < .001). No significant differences were observed in age or gender composition. This group exhibited comparatively elevated traumatic stress as measured by the IES-R (χ2(3) = 12.45, P = .006, η2 = .061), although none of the pairwise comparisons remained significant after adjustment for multiple testing. Nonetheless, group differences were of moderate magnitude for intrusion symptoms (χ2(3) = 15.43, P = .002, η2 = .079) and small for hyperarousal (χ2(3) = 10.88, P = .012, η2 = .051). Post hoc analyses indicated significantly higher intrusion scores compared with Groups 2 (padj = .021), 3 (padj = .019), and 4 (padj = .027), as well as higher hyperarousal relative to Group 4 (padj = .023), with marginal differences observed in comparison to Groups 2 (padj = .061) and 3 (padj = .063).
Group 2 (25%, n = 41) comprised participants with heterogeneous individual trajectories that, when aggregated, produced a near-stable pattern with a slight decreasing trend on both PTSS-10 and SWLS scores. Demographically, the group did not differ significantly from the overall sample in age, gender, education, residence, or profession. Still, members reported lower intrusion scores compared with the previous group of stable trajectory, while no other contrasts reached significance.
Group 3 (23.8%, n = 39) demonstrated a pronounced early decline in PTSS-10, followed by later flattening. The SWLS scores showed the complementary pattern of an early decrease with some fluctuations and lower scores at final stages. This class was disproportionately composed of adults aged 60 years and older (20.5%, padj = .018). Members were more likely to have originated from large cities (35.9%, padj = .038) or regional centres (30.8%, padj = .014).
Group 4 (35.4%, n = 58), the largest class, was characterised by a marked decline in PTSS that gradually stabilised, alongside SWLS that remained largely stable before showing a notable late increase. Members were strongly overrepresented among bachelor's degree holders (63.8%, padj < .001), more likely to have lived in regional centres prior to relocation (74.1%, padj = .002), and more often resided in large cities post-relocation (56.9%, padj = .015). Public sector employment was also markedly overrepresented prior to relocation (50.0%, padj < .001). Traumatic stress symptoms in this group were lower than those of Group 1, while final life satisfaction scores exceeded those of all other groups.
Differences emerged among the five symptom trajectories in the proportion of participants meeting the PTSS-10 cutoff over time. Although high baseline rates of probable PTSD were observed across most trajectories, approximately 59%-80% at first wave, the trajectories diverged substantially thereafter. By the second wave, some trajectories showed a rapid decline in the proportion meeting the cutoff, to approximately 3%-24%, indicating early symptom reduction. From this point onward, cutoff exceedance was rare in most trajectories, whereas residual or recurrent clinically relevant symptoms were confined primarily to Groups 1 and 2 and affected only a small proportion of participants. Overall, the trajectories differed mainly in the speed and completeness of symptom reduction, despite comparable levels of acute distress at baseline.
Discussion
The central finding of the present study is the pronounced heterogeneity in longitudinal courses of post-traumatic stress symptoms and life satisfaction among Ukrainian refugees during the early period of resettlement. Mean-level analyses provided clear evidence of systematic within-person change over time, thereby justifying longitudinal modelling. Specifically, post-traumatic stress symptoms showed a pronounced overall decline, best represented by a curvilinear trajectory characterised by a steep initial reduction followed by levelling-off. This trend corresponds to the expected plateau effect. 40 Comparable patterns have been documented among Syrian refugees, 41 Yazidi survivors, 42 and diverse refugee populations. 26 Such findings suggest partial recovery from acute stress, consistent with longitudinal models of trauma recovery. 43 In contrast, life satisfaction remained consistently low, with mean levels below established thresholds for well-being. This result is consistent with Brücker et al (2023), 44 who reported average life satisfaction of 5.8 on an 11-point Likert scale among Ukrainian refugees in Germany – nearly two points lower than the German population. Although the present study lacked a direct comparison group, the persistently low life satisfaction observed here suggests a similar trend: even as traumatic stress symptoms abate, overall well-being does not substantially improve.
Group-based multi-trajectory modelling identified four meaningful subgroups, broadly corresponding to Brier et al's (2020) 24 trauma recovery typology: (1) persistently high post-traumatic stress with low life satisfaction; (2) diverse but largely stable post-traumatic stress and life satisfaction profiles; (3) declining post-traumatic stress without significant improvement in life satisfaction; and (4) declining post-traumatic stress with concomitant gains in life satisfaction. The most favourable trajectory was characterised by gradual post-traumatic stress reduction coupled with significant improvement in life satisfaction towards the end of the study period. Joint modelling of post-traumatic stress symptoms and life satisfaction captures distinct patterns of decoupling and convergence between psychological distress and well-being, thereby providing context for adaptation following war-related displacement similarly to results of 10-year longitudinal study by Opaas et al (2020). 45 In contrast to much of the existing literature, which has often examined adjustment at later stages following trauma, the present study focuses on the early period of full-scale war and initial resettlement. Although this phase is difficult to capture empirically, it may be particularly informative for understanding how early symptom change relates to broader well-being. The findings suggest that reductions in post-traumatic stress symptoms during this period do not necessarily coincide with improvements in life satisfaction, indicating that these processes may unfold asynchronously under conditions of ongoing contextual uncertainty.
Importantly, in contrast with those who remained at persistently high stress levels, differences emerged in the distribution of specific symptom clusters – particularly intrusion and hyperarousal. Although causal mechanisms cannot be established, these findings are consistent with Specker et al (2024), 46 who highlighted the central role of hyperarousal symptoms in driving longitudinal stability in PTSD and Giacco et al (2013), 47 who highlighted the importance of hyperarousal in quality of life improvements. This supports the interaction between recovery trajectories and the symptomatic composition of stress-related states. It should also be noted that the proportion of participants classified into each trajectory group differed somewhat from the distributions reported by Galatzer-Levy et al (2018). 48 Given the modest sample size, caution is warranted in generalising these proportions. Nevertheless, the observed pattern of participant distribution across resilient, recovery, delayed, and chronic trajectories aligns with established trajectory typologies and may serve as a useful basis for further investigation in larger samples.
Demographic and contextual characteristics were strongly associated with trajectory membership. The group with the most favourable outcomes was overrepresented by individuals with higher education, previous residence in urban areas, and public-sector employment. Conversely, the subgroup with persistently high stress and low life satisfaction contained a disproportionate number of PhD holders, who may have been particularly vulnerable to occupational downgrading. Meanwhile, the subgroup with declining stress but no improvement in life satisfaction consisted mainly of older adults, suggesting that age-related barriers and reduced adaptive resources may limit recovery in subjective well-being despite symptom reduction. These findings underscore the importance of both individual human capital and broader resettlement contexts. Younger age, higher education, and continuity of urban residence appear to foster resilience, whereas older age and occupational downgrading are associated with more vulnerable trajectories, as previously documented in other refugee cohorts.14,23,49
It is also noteworthy that many structural conditions contributing to stress symptoms remained unfavourable during the study period. Although 35.4% of respondents were allocated to the most favourable trajectory, 64.6% followed less adaptive courses. The observed decline in inequality indices after relocation did not reflect greater equity, but rather a structural compression of occupational statuses due to widespread job loss and limited re-employment opportunities. This socioeconomic homogenisation shifted refugees from diverse urban labour markets into more uniform and precarious forms of employment. These findings indicate that trajectories of post-traumatic stress symptoms are shaped not only by individual resources but also by enduring structural constraints. In this sense, persistent contextual adversity may cap recovery and channel refugees into plateaued or adverse stress trajectories, even when acute symptoms initially decline.
Until recently, large-scale war-related displacement was predominantly concentrated in low- and middle-income countries. The Russian invasion of Ukraine fundamentally altered this pattern, resulting in the relocation of millions of war survivors to high-income European contexts. In this sense, the present findings should be interpreted not as individual recovery patterns but as embedded within a broader societal exposure to prolonged war-related stressors. The decoupling observed between declining post-traumatic stress symptoms and persistently low life satisfaction may therefore reflect both refugee-specific adversities and wider contextual strains within host societies.
Limitations
Attrition across waves may have introduced selection bias, as participants who remained in the study may differ systematically from those lost to follow-up. Because reasons for non-participation and dropout were not assessed, it remains unclear whether attrition was related to mental health status, post-migration stressors, or other unobserved factors, leaving the direction of potential bias uncertain.
The absence of comprehensive data on war-related exposure, lifetime stress, and post-relocation stressors also limited provided findings. Prior research consistently shows that both pre-migration trauma severity and post-migration adversities – such as housing insecurity, legal uncertainty, social isolation, discrimination, and barriers to healthcare – substantially shape mental health trajectories. Without such data, it is not possible to determine whether observed heterogeneity reflects differential exposure histories, contextual stressors, or recovery processes. Consequently, the study cannot explain why some individuals fared better than others over time, substantially limiting causal interpretation.
The study further relied on self-report measures, which are vulnerable to recall bias, social desirability, mood-congruent reporting, and individual differences in symptom interpretation. Although Ukrainian-language versions were used to ensure linguistic accessibility, language adaptation does not mitigate these biases. In the present context, reporting may also have been influenced by stigma, perceived expectations in institutional settings, or concerns about disclosure. Accordingly, symptom levels should not be interpreted as equivalent to clinical diagnoses, and future studies should incorporate multi-method assessments where feasible. A related measurement limitation is that some instruments were developed within DSM-IV conceptualisations of post-traumatic stress. Due to longstanding structural constraints and the historical underdevelopment of Ukrainian-language psychometric tools, validated DSM-5-aligned instruments remain limited. While this reflects broader systemic inequities rather than study-specific choices, it may affect construct coverage and diagnostic alignment.
Regarding analysis, trajectory modelling was conducted with a modest longitudinal sample, constraining model complexity and limiting the stability of smaller classes. Although sufficient for exploratory group-based modelling, the identified trajectories should be interpreted as descriptive representations of heterogeneity during the early phase of full-scale war and resettlement, rather than as definitive subgroup estimates. As noted by Nagin and Odgers (2025), 38 such analyses occupy a space between exploratory and confirmatory inference and require replication in larger cohorts. In addition, between-trajectory comparisons were based on most likely class membership from an unconditional model, which does not account for classification uncertainty and may bias group-level estimates. While comparisons were exploratory and supported by acceptable classification diagnostics, more robust three-step or conditional modelling approaches were not feasible given the sample size and are recommended for future research.
Finally, generalisation is limited by the recruitment strategy. Participants were primarily recruited through integration courses and support services, likely over-representing refugees engaged with institutional assistance and under-representing more marginalised individuals with limited access to such services. Accordingly, findings should not be interpreted as population-representative but as reflecting longitudinal patterns within a reachable subgroup of Ukrainian refugees resettled in a high-income European context.
Conclusion
This study shows that war-related displacement produces heterogeneous adjustment pathways among Ukrainian refugees. Stress and life satisfaction followed divergent trajectories, with symptom reductions not accompanied by comparable gains in well-being. Outcomes were shaped by demographic and contextual factors, with education, urban residence, and public-sector employment linked to resilience. These findings underscore the need for integrated interventions that combine mental health care with structural support in employment, housing, and social integration to promote sustainable recovery.
Supplemental Material
sj-docx-1-css-10.1177_24705470261422385 - Supplemental material for Longitudinal Trajectories of Post-Traumatic Stress Among Ukrainian Refugees: A Cohort Study
Supplemental material, sj-docx-1-css-10.1177_24705470261422385 for Longitudinal Trajectories of Post-Traumatic Stress Among Ukrainian Refugees: A Cohort Study by Liudmyla Krupelnytska, Nazar Yatsenko and Olha Morozova-Larina in Chronic Stress
Supplemental Material
sj-docx-2-css-10.1177_24705470261422385 - Supplemental material for Longitudinal Trajectories of Post-Traumatic Stress Among Ukrainian Refugees: A Cohort Study
Supplemental material, sj-docx-2-css-10.1177_24705470261422385 for Longitudinal Trajectories of Post-Traumatic Stress Among Ukrainian Refugees: A Cohort Study by Liudmyla Krupelnytska, Nazar Yatsenko and Olha Morozova-Larina in Chronic Stress
Supplemental Material
sj-docx-3-css-10.1177_24705470261422385 - Supplemental material for Longitudinal Trajectories of Post-Traumatic Stress Among Ukrainian Refugees: A Cohort Study
Supplemental material, sj-docx-3-css-10.1177_24705470261422385 for Longitudinal Trajectories of Post-Traumatic Stress Among Ukrainian Refugees: A Cohort Study by Liudmyla Krupelnytska, Nazar Yatsenko and Olha Morozova-Larina in Chronic Stress
Footnotes
Acknowledgments
We gratefully acknowledge Dr Laura M. König and Dr Olena Lytvynenko for their support throughout this research.
Ethical Considerations
The study was approved by the University of Bayreuth Ethics Committee (approval no. 22-2022) on August 24, 2022.
Consent to Participate
Written informed consent was obtained from all participants for their involvement in the study, including the collection of their personal information, and the deletion of it afterwards.
Consent for Publication
Written informed consent was obtained from all participants for the publication of anonymised health-related information in this article and in an open science data repository.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.