
Abstract
Background
The populations of middle- and low-income countries are exposed to many stressors, and these are associated with worse mental health. The ICD-11 includes a section “Disorders specifically associated with stress” and there are many validated measures for the assessment of stress-related disorders. However, there is no self-reported measure of ICD-11 adjustment disorder available for use in Arabic-speaking populations. This study aimed to translate and validate the Arabic version of the self-reported International Adjustment Disorder Questionnaire.
Methods
Data was collected from Iraqi patients with physical illness and their families from October 6 to October 14, 2024, through a cross-sectional study conducted at Baghdad's Teaching Hospital and the Oncology Teaching Hospital. The R Environment for Statistical Programming was utilized for analysis.
Results
Findings from confirmatory factor analysis were consistent with previous studies by identifying two strongly correlated factors (r = 0.72), representing the ‘preoccupation’ and ‘failure to adapt’ symptom clusters. These factors showed reliable scores (α = 0.695 and 0.814) and significant relations to depression and anxiety. To avoid multicollinearity, a total symptom scale can be used, based on similarly positive relations to psychological states and high reliability (α = 0.798).
Conclusion
The Arabic translation demonstrates good psychometric properties and can be utilized in clinical and research settings.
Keywords
Introduction
According to the latest International Statistical Classification of Diseases and Related Health Problems (ICD-11), adjustment disorder (AjD) constitutes a maladaptive response to a stressor(s), including illness, disability, family conflict, socio-economic problems, and educational difficulties occurring in the last month. 1 This reaction is characterized by preoccupation with the stressor or its consequences and failure to adapt, significantly impairing different facets of life. AjD is not a discrete mental disorder, but rather it represents the upper end of a maladaptive response continuum that is associated with distress and functional impairment.
The prevalence of AjD is unknown globally and highly variable across national studies due to differences in the symptoms used for classification, whether daily life impairment is considered, alternative diagnoses, such as depression or anxiety, are excluded per the ICD-11 recommendations, and demographic heterogeneity of the samples. 2 A nationwide German survey, utilizing the ICD-10, found a prevalence of 1.4%, dropping to 0.9% after including the impairment criterion. 3 The difference between the estimates reported by two Israeli studies, one using the Adjustment Disorder-New Module 20 scale (ADNM-20) (17.5%) and the other using the International Adjustment Disorder Questionnaire (IADQ) (10.2%), shows that differences occur even within the same population, despite both not excluding alternative diagnoses.4,5 Physical conditions, especially if chronic or incurable, can also increase maladaptive adjustment in patients and their families. In a study from 2022, AjD affected 13% to 15% of cancer patients, with higher rates among those with recent diagnoses. 6 In 2023, another study from Saudi Arabia noted that 43.9% of adult cancer patients had AjD, without excluding alternative diagnoses. 7
Yet, despite the importance of assessing AjD among patients with physical conditions, diagnosis might not be straightforward. First, choosing a diagnostic criterion can be complicated. Second, the presence of alternative diagnoses, including major depression, PTSD, and generalized anxiety disorder, can further blur the clinical picture. Hence, if the stressor disappears, symptoms should be resolved within 6 months. Otherwise, an alternative diagnosis should be considered. Thirdly, different screening questionnaires might cover different clinical issues or are administered differently. These include ICD-based screeners (IADQ, ADNM-20, and ADNM-8) and the DMS-5-based SCID-5.2,8–10 SCID-5, for example, involves a semi-structured interview with pre-specified questions, where psychiatrists are also allowed to explore symptoms in greater detail. 10 Meanwhile, the ADMN-20 assesses avoidance behaviors and emotional disturbance frequencies in the last week and for how long they have been present. 8
In recent years, the use of self-reported scales to assess psychiatric conditions has increased, guided by the need to screen larger populations, acquire more homogenous samples for research, and address low mental health coverage in middle- and low-income countries. 11 For AjD, the IADQ instrument was developed and validated for this purpose. 2 Its self-reported approach and fewer items make it more appropriate for research and primary healthcare, where access to psychiatric expertise is uncertain. Furthermore, the closer adherence to the ICD-11 improves clinical utility due to a focus on daily impairment and solves a shortcoming in the ADMN-20, where both failures to adapt and impairment are assessed using a single item. 2
In Iraq, using a structured interview based on the Diagnostic and Statistical Manual for Mental Disorders, fourth Edition (DSM-IV) criteria, AjD was found in 11.5% of those attending an outpatient psychiatric clinic in Duhok, a northern province. 12 However, no study has investigated the prevalence among patients with physical conditions. Iraq has only 2 mental health workers per 100 000 individuals, a third of whom are non-professionals who might not be qualified to diagnose AjD. 13 This coverage, which is below the global average of 9 mental health workers per 100 000 individuals, increases the demand for validated self-reported screening tools, as most care centers might not have sufficient capacity to assess AjD and other psychological issues, especially among individuals with physical conditions.
The IADQ has been translated from English to German, Hebrew, Danish, and Italian,5,14,15 showing a stable 2-factor structure corresponding to the ICD-11 criteria. During the conceptualization of this study, no Arabic version was listed on the International Trauma Consortium website. 16 As of February 2025, an Arabic version is listed. However, no validation has been reported for this translation or any other Arabic version. Furthermore, no study has tested IADQ's validity in a clinical sample of patients with physical conditions.
This study aimed to translate the IADQ into Arabic and validate it among Iraqi patients with physical conditions and their families. We hypothesized that the Arabic IADQ would demonstrate a 2-factor solution, with two strongly correlated factors that show a positive relation to depression and anxiety scales. These factors represent the continuous underlying dimensions of preoccupation and failure to adapt symptom clusters. As a secondary aim, the prevalence of AjD was also calculated.
Patients and Methods
Study Design and Setting
A cross-sectional study was conducted from September 1 to December 25, 2024, at Baghdad Teaching Hospital and Oncology Teaching Hospital in Baghdad, the capital city of Iraq. The data collection part of the study was conducted between October 6 and October 14, 2024. These tertiary healthcare centers were selected as they tend to receive patients from different provinces and, therefore, provide the potential to test the validity of the IADQ on a more diverse sample. Moreover, patients presenting to tertiary centers typically exhibit more complex conditions. Consequently, it is imperative to evaluate AjD in these patients and their families. Equator Network's COSMIN guidelines for studies on the measurement properties of patient-reported outcomes were followed to reduce reporting bias. 17 No exclusion criteria were used to obtain a sample that closely resembles the target population. The only inclusion criteria were that participants should be over the age of 18 years and be able to read and complete the survey questions.
Minimum Sample Size Requirements
The number of participants required for each type of analysis was calculated. As six symptoms are included in the IADQ, a minimum of 120 participants was deemed sufficient for confirmatory factor analysis, based on the recommended minimum participants-to-items ratio between 10:1 and 20:1 (Kline; 18 Tanaka 19 ). For the multiple linear regression, G*Power version 3.1.9.7 indicated a minimum of 107 participants based on 2 predictor variables, a medium effect size (f2 of 0.15), statistical power of 95%, and an alpha error of 5%. 20
Measurement Tools
Data was collected using a structured self-reported questionnaire consisting of four sections (see Supplemental Materials). The first section included participants’ demographics, including age, gender, ethnicity, province, marital status, educational level, residence, home ownership, and smoking status. The second section included the IADQ starting with a 9-item stressor events scale, where each item can be answered with either “Yes” (1) or “No” (0). The next six items assess preoccupation and failure to adapt severity on a 5-point Likert scale from 0 (not at all) to 4 (extremely). An additional question inquires whether symptoms have begun within one month of the stressor, and three final items assess functional impairment on a similar 5-point Likert scale. Total scale scores can be computed to represent symptom severity, and a probable diagnosis is made if the participant meets all the following:
The presence of at least one stressor (items 1-9). At least one preoccupation symptom rated ≥2 (items 10-12). At least one failure to adapt symptom rated ≥2 (items 13-15). Symptoms began within 1 month of the stressor (item 16). At least one functional impairment rated ≥2 (items 17-19).
The IADQ was initially translated into Arabic by the authors (MA-G, MAW, and GA-G) through two cycles, each with a translation phase and a review phase where the standing Arabic version was compared to the English. An independent English-to-Arabic translation bureau approved the pre-final version on October 5, 2024, after verifying its accuracy (see Supplemental Materials).
Mental health measures were included in the third section. The Arabic version of the Generalized Anxiety Disorder 7-item Scale (GAD-7) was used due to its reliability (α = .763), validity, and high accuracy against the DSM-5 criteria for generalized anxiety disorder.21–23 Participants are asked about how bothered they are from each symptom in the last two weeks, on a 4-point Likert scale from 0 (not at all) to 3 (nearly every day). Items’ scores are added to provide a total score, with 0-4 indicating no or minimal anxiety, 5-9 for mild, 10-14 for moderate, and 15-21 for severe.
The Arabic Patient Health Questionnaire-9 (PHQ-9) was used due to its reliability (α = .857) and validity in assessing the presence and severity of depression and more optimal performance in case identification compared to other measures.21,24 A four-point Likert scale, similar to the GAD-7, is used for each symptom. A total score would be calculated from item scores, where 0-4 indicates no or minimal depression, 5-9 for mild, 10-14 for moderate, 15-19 for moderately severe, and ≥20 for severe.
Ethical Considerations
Informed consent was required for participation. Individuals were informed of the study's purposes, assured of data privacy, and given the option to refuse or participate. Individuals who agreed were given a paper copy of the questionnaire. To avoid applying pressure, data was collected by individuals not involved in providing healthcare, and participants were reassured that their or their relatives’ healthcare would not be affected by participation or withdrawal. The ethical committee of the Iraqi Ministry of Health reviewed the study protocol, and approval was obtained on the 16th of September 2024 in decision no. 39.
Statistical Analysis
Descriptive statistics were performed with SPSS version 27, while the R Environment for Statistical Programming ver. 4.4.2 and its associated packages were utilized for psychometric analyses.25–29 Both the Shapiro-Wilk test and the less sample-size-sensitive D’Agostino-Pearson K2 test showed non-normal distributions (Supplemental Materials: Table S1). 30 Therefore, nonparametric methods were used.
The IADQ conceptual framework has already been studied across different cultures.2,5,14,15 Therefore, hypothesis-driven confirmatory factor analysis, with a robust maximum likelihood (MLR) estimator, was used to test the structural validity of the AjD symptoms (items 10-15). Item endorsement rates were calculated, similar to the original validation, by classifying items with a moderate score of ≥2 as “present” and the robust diagonally weighted least squares (WLSMV) estimator was used to analyze these rates. 2 Four models were tested (Figure 1), the 1-factor and 2-factor solutions from the initial validation 2 and two models from the Danish validation, one with two items for preoccupation and four for failure to adapt, 14 and the other where item 12, “fear of the future”, had a cross-factor loading.

Competing Structural Models for the IADQ.
Absolute goodness-of-fit indices included the comparative fit index (CFI) and the Tucker-Lewis Index (TLI) at >0.90 and >0.95 for acceptable and excellent fit, respectively. The Root Mean Square Error of Approximation (RMSEA) and the Standardized Root Mean Square Residual (SRMR) with values <0.08 and <0.05 indicated an acceptable and excellent fit. A chi-square divided by degree of freedom (x2/df) ≤ 3 and ≤2 indicating acceptable and excellent fit.31–34 A non-significant χ2 test also indicates fitness, especially with the WLSMV estimator. However, due to sensitivity to sample size, it should be interpreted only alongside other indices. 19
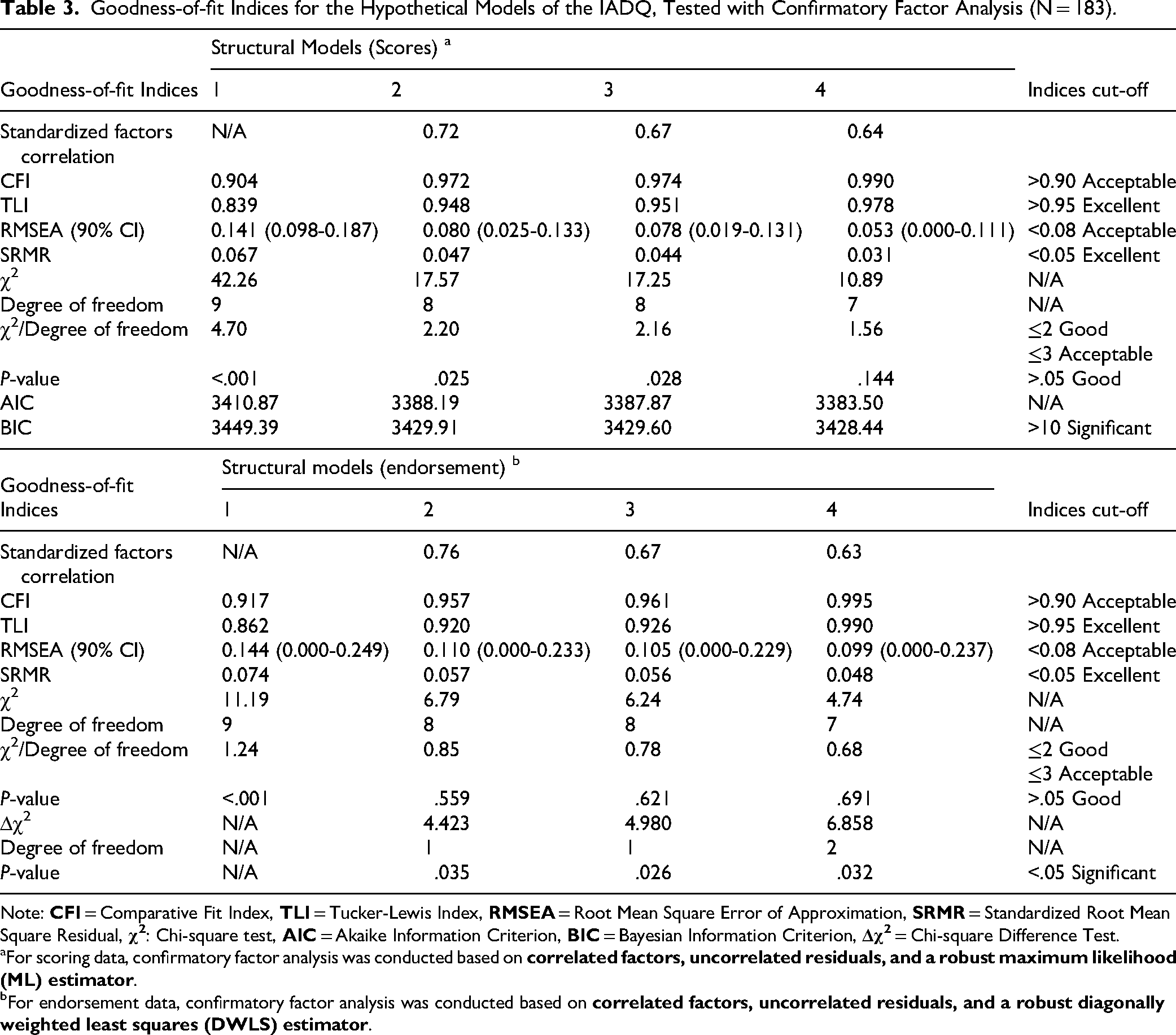
To compare models, reductions in the Bayesian Information Criterion (BIC) between 2-6 points, 6-10 points, and >10 points have indicated some, strong, and very strong evidence of model superiority, respectively. 35 Better fitness was also indicated by a > 0.015 difference in RMSEA and a lower Akaike Information Criterion (AIC), with no threshold described for the latter.36,37 As BIC cannot be calculated for the WLSMV models, RMSEA was supplemented with the scaled Δχ2 test. 38 Model 2 was selected for further testing based on parsimony, as it showed acceptable and excellent absolute fitness and non-inferior relative fitness.
The internal concurrent validity was assessed by investigating the relationship between the stressor events and the symptoms subscales, while the external was assessed by examining the relations between the symptom subscales (individually and in combination) and the mental health scales (PHQ-9 and GAD-7). Robust multiple linear regression was used for univariate and a robust MANOVA with a Pillai Trace estimator for multivariate analyses at a cut-off of 0.05 for statistical significance. 39
Composite reliability was measured for each subscale and the total symptoms scale, with >0.7 indicating good reliability. Composite reliability was selected instead of Cronbach's alpha, as it does not assume similar items’ loading. 40 The relation between items and each of the factors was also explored by calculating the corrected item-total Spearman's rank correlation and the correlation between each item and the other scale.
AjD prevalence was first calculated without the exclusion of alternative diagnoses (depression and anxiety), based on the IADQ guidelines. 2 Then a second time with the exclusion of individuals with PHQ-9 and GAD-7 scores of ≥15 and ≥10, similar to prior validations, based on meta-analyses reporting high specificities of 0.96 and 0.82 for depression and anxiety at these cut-off points.41,42 To acquire three additional estimates, depression and anxiety were excluded at different severities: ≥ 15 (severe), ≥ 10 (moderate), and ≥5 (mild).
Results
Inclusion and Exclusion
196 participants were recruited, but 13 did not endorse any of the IADQ stressors and, as a result, did not complete the rest of the questionnaire. Hence, 183 participants are included in the analysis: 116 (63.4%) from the oncology teaching hospital, 45 (24.6%) from the surgical wards of Baghdad's teaching hospital, and 22 (12%) from the medical.
Sample Characteristics
There were fewer patients (n = 38; 20.8%) than family members (n = 145; 79.2%). The median age was 37 years [IQR: 27-38], and 111 (60.7%) of the participants were male. Other demographic characteristics are summarized in Table 1. As anticipated, personal and a loved one's health were the most common stressors, with endorsement of 45.9% and 77.0%, respectively (Table 2), followed by financial and caregiving issues at 37.2% and 36.1%.
Demographic Characteristics (N = 183).

Missing value: marital status (4 responses), province (1 response).
Items and Subscales’ Score and Endorsement (N = 183).
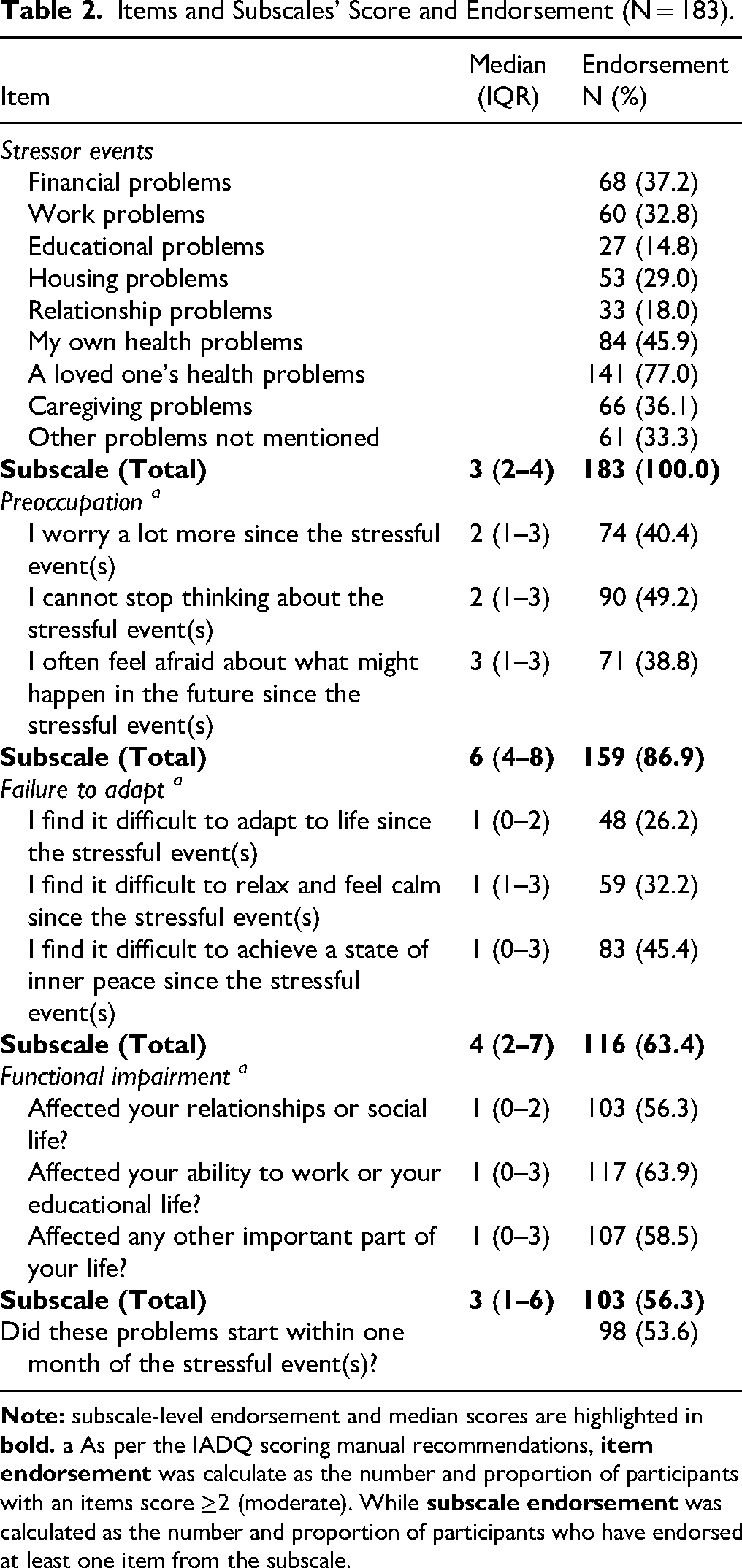
In terms of symptoms, being unable to stop thinking about stressful events was the most endorsed symptom of preoccupation (90, 49.2%), and being unable to establish inner peace was the most endorsed symptom of failure to adapt (83, 45.4%) (Table 2). Overall, preoccupation had higher endorsement and median scores.
Structural Validity of the Arabic IADQ
Table 3 displays the goodness-of-fit indices for the tested models. The 1-factor solution had poor fit in both the item scores and endorsement models, while all the 2-factor solutions (models 2 to 4) showed acceptable model fit. The modified 2-factor solutions of models 3 and 4 showed excellent fitness. However, there was a < 2 BIC difference from model 2 and a non-significant scaled Δχ2 test between models 4 and 2 (Δχ2 = 2.174, Δdf = 1, p = .140). Model 2 consisted of two correlating factors (r = .72) and was selected for further analysis based on parsimony.
Goodness-of-fit Indices for the Hypothetical Models of the IADQ, Tested with Confirmatory Factor Analysis (N = 183).
Note:
For scoring data, confirmatory factor analysis was conducted based on
For endorsement data, confirmatory factor analysis was conducted based on
Concurrent Validity of the Arabic IADQ
Internally, the stressor events scale showed significant positive relations with the preoccupation and failure to adapt subscales in both univariate (P < .01) and multivariate analyses (P < .001) (Table 4). Externally, preoccupation was only significantly related to PH-9 and GAD-7 when included alone during regression (P < .001). Meanwhile, failure to adapt had statistically significant relations (P < .001) both alone and in combination with preoccupation.
Internal and External Concurrent Validity of the IADQ Subscales (N = 183).

Reliability of the Arabic IADQ
A good composite reliability of .814 was demonstrated for the failure to adapt and the total symptoms scale (.798). While preoccupation showed a borderline value (.695) (Supplemental Materials: Table S2). All the items loaded positively and had a higher correlation with their hypothesized factors, except for item 12, which correlated less to preoccupation (0.417 vs 0.474) (Supplemental Materials: Table S3).
Prevalence of Adjustment Disorder
When the diagnostic IADQ rules were applied, 48 participants (24.5%) met the criteria for AjD. After excluding severe depression and anxiety (scores ≥15) and moderate levels (scores ≥10), the rates dropped to 26 (13.3%) and 8 (4.1%), respectively. No participant had AjD after excluding those with mild depression and anxiety (score ≥5). Similar to excluding moderate depression and anxiety, AjD was found in 8 (4.1%) when using the cut-off points from previous studies (PHQ-9 ≥ 15, GAD-7 ≥ 10).2,15
Discussion
This study aimed to assess the validity and reliability of an Arabic translation of the IADQ in a sample of Iraqi hospital patients and their families. Confirmatory factor analysis revealed poor fitness of the 1-factor solution and superiority of the 2-factor solutions, thereby arguing against the unidimensionality of AjD symptoms. This dimensionality has been previously investigated with both the ADNM-20 and the IADQ. Notably, following the original proposal of a 2-factor structure for the ICD-11 diagnostic narrative of AjD, 43 four studies, using the ADNM-20, argued instead for unidimensionality.8,43–45 In addition, although previous IADQ validations reported a bi-dimensional model as a better fit, results from the original validation indicate that a 1-factor model also shows an excellent fit. 2 In subsequent validations from Switzerland, Israel, and Italy, this unidimensional model had borderline fitness, and in the Danish validation, it had poor fitness in all the reported indices.5,14,15 Considering all of this, the IADQ's closer adherence to the ICD-11 might lead to its higher tendency to report bi-dimensionality. 1 Using the ADNM-8, a study showed that preoccupations and failure to adapt were distinct but highly related. 46 As ADNM-8 adheres more than ADNM-20 to the ICD-11, these results suggest that assessment tools affect the perceived dimensionality.
Our results support a 2-factor solution for Arabic IADQ. The non-significant BIC difference and Δχ2 test between models 2 and 4 indicate that allowing item 12 (fear of the future) to have a cross-factor loading leads to a marginal increase in fitness that cannot be justified. The superior fitness for this model during the Danish validation was attributed to differences in the Danish social security systems and ambiguity between preoccupation and failure to adapt in the healthy working population. 14 Therefore, the higher distinction between the two constructs in our study might be due to validating the IADQ among a clinical sample. However, the lower loading of this item to the preoccupation factor and its higher correlation to the failure to adapt subscale suggest that some evidence for this overlap is still apparent. Future studies should further investigate the relation between this symptom and the two AjD constructs, both within and outside the IADQ and in other populations.
Similar to previous IADQ validations, symptoms could be arranged into 2 factors with a strong positive correlation (r = .72), although to a lower magnitude than previously reported (>.80).2,5,14,15 The 2-factor structure of the ICD-11 provides a convenient system for diagnosing AjD in clinical settings. 1 The significant positive relation between the two symptom subscales and the mental health scales gives evidence that the Arabic adaptation of the IADQ has good concurrent validity and can be utilized in clinical settings, consistent with previous validations.2,5,14,15 However, multicollinearity between the two subscales may indicate that a unidimensional structure is better for research. 2 The fact that the positive relation between preoccupation and mental health scales was no longer significant when adding failure to adapt to the models provides evidence for multicollinearity and supports the previously hypothesized premise that AjD is primarily a failure to adapt to stressors. 14 The significant relations of the unidimensional total symptoms scale support its utilization in research.
Before excluding depression and anxiety, 24.5% of participants had AjD. This estimate would drop to 13.3%, 4.1%, and 0.0%, based on whether a score of 15, 10, or 5 indicated positivity on the PHQ-9 and GAD-7. Previous meta-analyses have reported that a cut-off around 10 points provides an optimal trade-off between sensitivity and specificity for these scales.42,47 Additionally, the ICD-11 lists symptoms of anxiety and depression as “additional clinical features” of AjD, 1 which can be present if they do not constitute the majority of psychopathology. Hence, an AjD prevalence of 4.1% is the most reliable in our sample. This estimate was also obtained when exclusion was performed using the cutoff described in the original and Italian validations, indicating that all individuals with moderate depression (scores: 10-14) had moderate anxiety. Hence, increasing the PHQ-9 cutoff from 10 (moderate) to 15 (severe) maximizes specificity without increasing individuals classified with AjD.2,15
As previously mentioned, AjD prevalence is difficult to compare because studies use different assessment methods and are not consistent in excluding alternative diagnoses or applying daily impairment criteria. 2 Even studies using IADQ show methodological differences. The Italian and Swiss validations focused on COVID-19 and found a prevalence of 18.8% and 8.2%5,15; the original and Israeli validations reported estimates of 7.0% and 10.2% in the general public2,4; and a prevalence of 16.7% was reported among Danish social educators. 14 Of these validations, only the original and the Italian excluded alternative diagnoses. Despite our focus on patients, the lower prevalence of 4.1% might suggest that burdens of serious physical conditions may lead to more severe mental disorders like depression and anxiety rather than AjD, which is often considered to be milder despite its high rate of transition to more severe mental conditions and its association with physical comorbidities.48,49 The six-fold decrease in prevalence after excluding depression and anxiety provides evidence for this. However, future studies should include a more thorough psychiatric evaluation of Iraqi patients with serious physical illness and their families to calculate the relative prevalence of different mental conditions.
Strengths, Limitations, and Recommendations
Our study represents the first Arabic validation of the IADQ and the first validation among a clinical sample. Robust statistical methods were utilized to address data normality during structural validity, and regression instead of correlation was used for concurrent validity to address multicollinearity. However, certain limitations exist and should be addressed in future studies. Firstly, similar to previous validations, the diagnostic accuracy of the IADQ was not assessed. Reporting sensitivities and specificities might be misleading without prior validation. However, with those metrics established for the Arabic IADQ, future studies should focus on comparing with standardized clinical interviews to provide more information on clinical utility. Conducting future studies structured around testing against clinical interviews would also allow the exclusion of other disorders, including prolonged grief, uncomplicated bereavement, burnout, etc, as recommended by the ICD-11, without inappropriately prolonging the assessment tool and impact response authenticity. Secondly, test-retest reliability could not be assessed due to cross-sectional design. Finally, convenient sampling was utilized, and as such, our prevalence estimates are to be considered preliminary, and their generalizability cannot be established with absolute certainty.
Conclusion
The Arabic IADQ shows a valid structure with two strongly correlated factors corresponding to the preoccupation and failure to adapt latent constructs of the ICD-11. Individually, both subscales show good concurrent validity and a positive relation to depression and anxiety, which supports their use for AjD diagnosis in patients with physical conditions and their family members. Nevertheless, the total symptoms scale, which demonstrated comparable concurrent validity, may be more appropriate for research due to multicollinearity.
Supplemental Material
sj-docx-1-css-10.1177_24705470251332801 - Supplemental material for Translation and Validation of the Arabic International Adjustment Disorder Questionnaire Among Patients with Physical Illness and Their Families in Iraq
Supplemental material, sj-docx-1-css-10.1177_24705470251332801 for Translation and Validation of the Arabic International Adjustment Disorder Questionnaire Among Patients with Physical Illness and Their Families in Iraq by Mustafa Al-Gburi, Mustafa A Waleed, Mark Shevlin and Ghaith Al-Gburi in Chronic Stress
Supplemental Material
sj-docx-2-css-10.1177_24705470251332801 - Supplemental material for Translation and Validation of the Arabic International Adjustment Disorder Questionnaire Among Patients with Physical Illness and Their Families in Iraq
Supplemental material, sj-docx-2-css-10.1177_24705470251332801 for Translation and Validation of the Arabic International Adjustment Disorder Questionnaire Among Patients with Physical Illness and Their Families in Iraq by Mustafa Al-Gburi, Mustafa A Waleed, Mark Shevlin and Ghaith Al-Gburi in Chronic Stress
Supplemental Material
sj-docx-3-css-10.1177_24705470251332801 - Supplemental material for Translation and Validation of the Arabic International Adjustment Disorder Questionnaire Among Patients with Physical Illness and Their Families in Iraq
Supplemental material, sj-docx-3-css-10.1177_24705470251332801 for Translation and Validation of the Arabic International Adjustment Disorder Questionnaire Among Patients with Physical Illness and Their Families in Iraq by Mustafa Al-Gburi, Mustafa A Waleed, Mark Shevlin and Ghaith Al-Gburi in Chronic Stress
Footnotes
Acknowledgements
The authors would like to thank patients and their family members, attending Baghdad Teaching Hospital and Oncology Teaching Hospital, for their participation in this study.
Authors Contributions/CRediT
Conceptualization: MA-G; Methodology: MA-G, GA-G, MAW; Resources: MA-G, MAW; Investigation: all authors; Data curation: MA-G; Formal analysis: GA-G and MA-G; Software: GA-G, Visualization: GA-G, Validation: MS, Writing the original draft: all authors; revision and editing: all authors; Project administration: MA-G; Supervision: GA-G and MS.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.