
Abstract
Background
Mass conflict and related displacement in South Sudan has created a significant mental health need, however extant research on the impact of conflict is limited among South Sudanese people and has predominantly relied on Western-developed self report measures.
Method
A total of 195 South Sudanese adults who work in both civil society and government leadership positions participated in a psychophysiological assessment of heart rate variability (HRV) and self-reported PTSD and emotion dysregulation symptoms to participation in the Trauma-Informed Community Empowerment (TICE) Framework, developed and implemented by the Global Trauma Project (GTP). We utilized measures of heart rate variability to determine parasympathetic activity, which may be associated with difficulties responding to stressors as well as long-term physical health morbidity and mortality.
Results
Findings suggest pervasive difficulties in emotion regulation abilities among all participants and, consistent with the existing literature on PTSD in South Sudan, over a third of participants meet the clinical cut-off for PTSD. The majority of participants’ physiological profiles indicate unexpected levels of parasympathetic nervous system activity given age and gender norms, demonstrating a sample with serious health risk. HRV did not correspond to self-reported PTSD symptoms, but did correlate with emotion dysregulation variables.
Conclusions
These results demonstrate the feasibility and utility of using a multimethod approach to assessment in a community-based environment and highlight the psychophysiological burden of chronic socio-political strife.
Keywords
As of 2021, the United Nations Refugee Agency identified 94.7 million persons of concern worldwide: refugees, asylum seekers, internally displaced persons (IDPs), stateless persons, and others requiring protection. 1 Mass conflict and related displacement are collective experiences that affect the daily lives of a whole society while the effect on individuals varies. 2 As of 2018, 2.4 million refugees have migrated from South Sudan over the prior five years. Since 2013, nearly 400,000 people have died as a result of South Sudan's ongoing conflict with about half of these deaths estimated to be from violence 3 ; in the same time period, most people reported having experienced at least two war-related potentially traumatic events with 100% of individuals reporting at least one potentially traumatic event in their lifetimes and 90% reporting a lifetime incidence of more than 10 potentially traumatic events. 4 Yet, a limited number of studies have assessed the mental health of South Sudanese people, and most have relied on self-report measures and interviews,5,6 which may yield an incomplete picture owing, at least in part, to the utilization of measures derived in a different cultural context. The present assessment aims to add to the research on South Sudanese mental health by complementing self-reported mental health symptom measures with the novel use of a physiological measure associated with stress and self-regulation, which provide a useful lens that complements more culturally-determined self report and interview measures. This work will aid not only intervention development but our understanding of chronic stress, while demonstrating the feasibility of utilizing psychobiological measures in field-based contexts.
Since 2013, civil war has been waged in South Sudan with ongoing intracommunity violence, 7 leaving most of the population exposed to traumatizing events, such as recruitment of child soldiers and lack of food and resources, which in turn leave them psychologically vulnerable without sufficient mental health services to cope. One recent study found that all participants living within the IDP camp had a DSM-defined “PTSD-qualifying” traumatic event, with participants reporting an average of six different types of traumatic events, with destruction of homes, murder of family members, witnessing murder of loved ones, and exposure to combat each affecting over half the population. 4 In other words, the exposure to stress and trauma in South Sudan are both chronic and ubiquitous, increasing the likelihood of enduring PTSD symptoms due to a gradual diminishing of individuals’ abilities to cope with further potentially traumatic life events. 8
Indeed, emerging reports document around 28–36% of the South Sudanese population meet symptom criteria for PTSD. 9 Using a combination of both locally-developed and Western-developed tools, the Harvard Trauma Questionnaire (HTQ) 10 and Mini International Neuropsychiatric Interview, 11 Ayazi 6 found that 37.5% of South Sudanese people met criteria for either a PTSD-only or comorbid PTSD-depression diagnosis, which were significantly associated with exposure to traumatic events and socioeconomic disadvantage.
While higher than global norms, which hover at 4–12%,12,13 these rates may nonetheless reflect an under-representation of trauma-related symptoms due to lack of questions addressing culturally appropriate expressions of distress 14 or the full scope of symptoms associated with ongoing stress. While conflict is widely accepted to impact psychological well-being, documenting the mental health of people in South Sudan has barriers to its validity and cultural appropriateness 15 due in part to reliance on self-report data 16 and frameworks involving Western diagnoses. 17 A further problem is that chronic trauma is especially associated with emotion dysregulation,18,19 including use of harmful tension-reduction coping (eg, self-harm20,21;), difficulty pursuing goals, 22 difficulty controlling emotions, 23 and, importantly for this study, difficulties with experiencing or describing emotions. 24 This latter difficulty describing emotion may rise via both avoidance-related coping 25 and an interruption of awareness of emotional states. 26 The symptoms of trauma themselves, then, increase the complexity of self-report.
One way to ameliorate such problems with symptom assessment is to complement the use of self-report with physiological assessment, such as heart rate variability (HRV), which can help researchers obtain further insights into the experiences faced by target groups, independent of culture or language. HRV is a commonly used measurement of autonomic nervous system (ANS) function in a wide variety of settings ranging from medical and well-being to behavioral research domains. 27 Autonomic alterations are associated with stress,28,29 emotion, 30 and emotion regulation 31 and thus may provide a language-free means of assessing stress-related functioning at the intersection of psychology and biology. High frequency (HF) HRV is well-suited to provide a simultaneous lens on wellbeing given its relationship to relevant physical constructs, such as cardiac flexibility 32 –an indicator of healthy responses to stress33–35)–alongside psychological constructs such as emotion regulation 36 and empathic capacity. 37 In contrast, low HRV (eg, less fluctuation in HR over time) has been linked to autonomic dysregulation38,39 which can be characterized by overactive sympathetic nervous system, generally associated with fight and flight behavior 40 or ineffective parasympathetic activity. 41 Low HRV also predicts negative health outcomes, such as early mortality and cardiovascular issues,42,43 and has been documented in trauma-exposed individuals, indicating physiological and socio-functional dysregulation.44,45
In combining HRV measurement with field-comparable, standardized self-report measures of post-traumatic stress symptoms (PTSS)–including symptoms of affect dysregulation more commonly associated with chronic trauma exposure,
19
we may be able to capture risk that extends beyond self-report, and to understand physiological mechanisms which create such risk. Accordingly, the aims of this manuscript are as follows:
To describe, using self report, the trauma-related symptoms of individuals within South Sudan; Describe the indicators of physiological stress among adults in South Sudan; Examine the correspondence between self-report and physiology.
This work accomplishes several goals: 1. of providing further context to the mental health and wellbeing of chronically-stressed communities in South Sudan; 2. of incorporating a broader range of representation into chronic stress and psychophysiological research (whose norms, like self-report, skew from the Western world); while 3. simultaneously providing a foundation for future work about how to interpret each measure in context; and 4. demonstrating feasibility of undertaking psychophysiological investigations within resource-sparse regions.
Method
Overview
The present report outlines baseline psychophysiological well-being among South Sudanese individuals prior to participation in the Trauma-Informed Community Empowerment (TICE) intervention, developed and carried out by the Global Trauma Project (GTP), described here briefly for contextual purposes. TICE aims to facilitate community-driven healing in response to collective trauma, increase self-regulation capacities, enable connection and personal empowerment, reduce interpersonal and community violence, and increase existing providers’ capacity to provide culturally relevant, evidence-based support to their community members. The model assumes that trusted, local lay facilitators are best suited to support their community, and the training will in turn further facilitate their abilities. The South Sudan program consisted of two phases: three weeks of intensive, interactive, in-person training certified by the Ministry of Education for TICE community facilitators who work (and live) in the IDP setting; and six weeks of ongoing support for these facilitators while facilitating community wellness and healing workshops. GTP enlisted a team at The New School for Social Research with expertise in program evaluation in global settings. These data are from both community facilitators as well as untrained members of the IDP (internally-displaced people) community. The data presented here are a portion of their program evaluation.
This study was therefore deemed exempt by The New School Institutional Review Board. The project and authors complied with APA and Declaration of Helsinki guidelines. All participants provided general written informed consent in English, Arabic, or the local dialect in the initial intake; subsequent, specific task consent was provided via verbal assent.
Recruitment and Participants
Participants for the intervention were identified and recruited by local South Sudanese GTP partners, affiliated with the United Nations Development Programme (UNDP). Recruitment was conducted locally and through snowball sampling. Participants were either residing in the domestic equivalent of refugee camps as IDP, or were professionals interfacing with IDP camps regularly, occasionally both. Professional staff were drawn from both civil society and government leadership positions ranging from education, social work, medical health, religious institutions, judiciary branches, police, military, and peacebuilding. All recruited participants were verified as adults, prior to the program's recruitment. All program participants were invited to participate in the program evaluation on a voluntary basis and were included only if they provided written consent to do so. All program participants elected to participate in evaluation.
Measures and Materials
The HTQ 10 is a self-report assessment of a variety of traumatic events as well as reactions to these events, yielding a total score of endorsed trauma-related symptoms and criteria met for clinical thresholds of PTSD. The current intervention utilizes both English and Arabic translated and back-translated versions of the HTQ. 46 For the current intervention, modifications were made so that only the trauma-related symptomatology were assessed due to cultural appropriateness. Specifically, we did not request participants to report on their exposure to traumatic events. It has been established through population-based studies in South Sudan that 100% of the country's IDP residents have experienced a PTSD-qualifying trauma-exposure event, 4 and there is no reason to expect this number to be lower among people living in the particular domestic refugee camps and communities we engaged. Further, asking participants to detail their exposure when our goal was not diagnostic was perceived by lived-experience experts as an exceptional burden with potential for distress with little gain and is inconsistent with best practices within contexts where trauma exposure is widely known (eg, within domestic violence shelters). 47 That said, consistent with recommendations by Mollica et al, 48 we used a cutoff of 2.5 to indicate probable PTSD diagnosis; however, this is used only to provide context of the present sample, not to indicate a formal diagnosis; the core of our analyses focus on continuous symptom reporting. In this study, Cronbach's alpha = .793.
The Difficulties in Emotion Regulation Scale (DERS-short form) 49 is an 18-item self-report measure that taps into an individual's degree of emotion dysregulation. The scale can be separated into six dimensions: 1. use of emotion regulation strategies ('Strategies’); 2. acceptance of emotions (‘Nonacceptance’); 3. impulse control (‘Impulse’); 4. goal-directed behavior (‘Goals’); 5. awareness of emotions (‘Awareness’); 6. and clarity of emotional experience (‘Clarity’). The DERS was offered in English; where dialect-specific translations were requested, participants were offered dialect-specific translations. Prior work has demonstrated separation of clinical from nonclinical populations using total scores and subscale sum scores with the long form of the DERS,50,51 and additional work has shown satisfactory convergence between short- and long-forms of the measure. 52 In this study, Cronbach's alpha = .817. The DERS has been translated to both Arabic 53 and Swahili 54 and utilized in a variety of cultural contexts.55,56
Procedure
Following the provision of written consent, participants completed the HTQ and DERS individually in a group setting with facilitation by a group facilitator in an appropriate language to minimize staff burden in a program whose primary purpose was intervention. Additionally, the group facilitator collected participants’ physiological measures in separate sections of the group facility to ensure a quiet environment for a two-minute baseline collection period.57,58 HRV data were collected with the HeartMath emWave ear-clip plethysmograph over a two-minute resting baseline collection period with a sampling rate of 370 Hz per second.
While the majority of investigations into risk parameters determined through autonomic measures utilize longer measurement epochs (eg, five minutes or twenty-four hours), two-minute epochs converge well with these longer time frames. 59 Several investigations have specifically examined population norms and risk stratification using short cardiac activity recordings, with demonstrated clinical utility,59–63 and shown valid as emotion regulation measures. 31
Data Reduction
The heart rate signal which derives HRV indices was visually inspected and cleaned through individual assessment of successive RR intervals within each subject in Kubios HRV. 64 Samples with artifact corrections greater than 20% were excluded to ensure sufficient length of remaining measurement epochs, ie, no included samples contain more than 30 consecutive seconds of corrected data. Overall, six measures of cardiac activity were computed: heart rate, SDNN, rmSSD, lf-HRV, vlf-HRV, and hf-HRV. We provide two of the most common in the current investigation: SDNN, because of its widespread use in physical health settings 65 ; and hf-HRV, because of its clearly articulated utility in psychological settings. Other measures are reported in the supplement.
SDNN, referred to as a “time domain” statistic, is the standard deviation of time between normal heartbeats, in milliseconds, and reflects the influence of the parasympathetic and sympathetic activity on the heart's rhythm, 66 with SDNN especially associated with parasympathetic activity during short recordings. SDNN values taken over shorter (eg, 5 min) 66 and longer (eg, 24 h) epochs have been employed in studies of cardiac risk stratification 59 ; values below 50 ms are considered “critical”, between 50 and 100 ms are “concerning,” and above 100 ms are generally healthy or “non-concerning”. 67 RMSSD is the root mean squared of SDNN. 65
Frequency domain measures provide more specificity around autonomic influences on HRV. 32 Because sympathetic and parasympathetic activity influence the heart with different time courses, determinations about respective influences on the heart can be determined by how fast HRV changes over time–a type of measurement called a frequency domain statistic. Slower changes in HRV, called low-frequency HRV (lf-HRV), have been hypothesized to reflect a mix of sympathetic and parasympathetic nervous system activity and are computed in the .04 - .15 Hz frequency bands. Faster changes in HRV, called high-frequency HRV (hf-HRV) are thought to reflect parasympathetic nervous system activity and are computed in the .15 - .40 Hz frequency range.
Several studies have indicated that SDNN and hf-HRV both provide predictive value with respect to all-cause mortality, including but not limited to cardiac morbidity and mortality.42,43,59,66 In the psychological realm, hf-HRV has been highlighted in studies of mental health and other constructs41,68–70; however, thresholds using hf-HRV are less clearly established, as most studies are looking at its association with other constructs (eg, stress or emotion regulation) rather than as a risk index. Thus, here we present both time and frequency domain measures, to situate data on risk stratification using the widely-validated SDNN measures; we also examine how these measures correlate with self-report data.
Results
A total of 219 individuals completed some portion of the assessment: physiological measures (n = 168), PTSD symptoms (n = 202), and emotion dysregulation symptoms (n = 176). After artifact correction was applied, 159 had both usable physiological data and self-report data. The participants came from three cities: 110 residents from Juba, 56 from Aweil, and 53 from Bor. On average, participants were 36.4 years old (SD = 9.53, range 18-63). There were approximately twice as many males (N = 163, 62%) as females (N = 74; 34%) (nine did not report sex). Approximately half (51%, n = 11) were fluent in English and 38% (n = 83) were fluent in Arabic.
Aim 1: Describe the Mental Health Burden
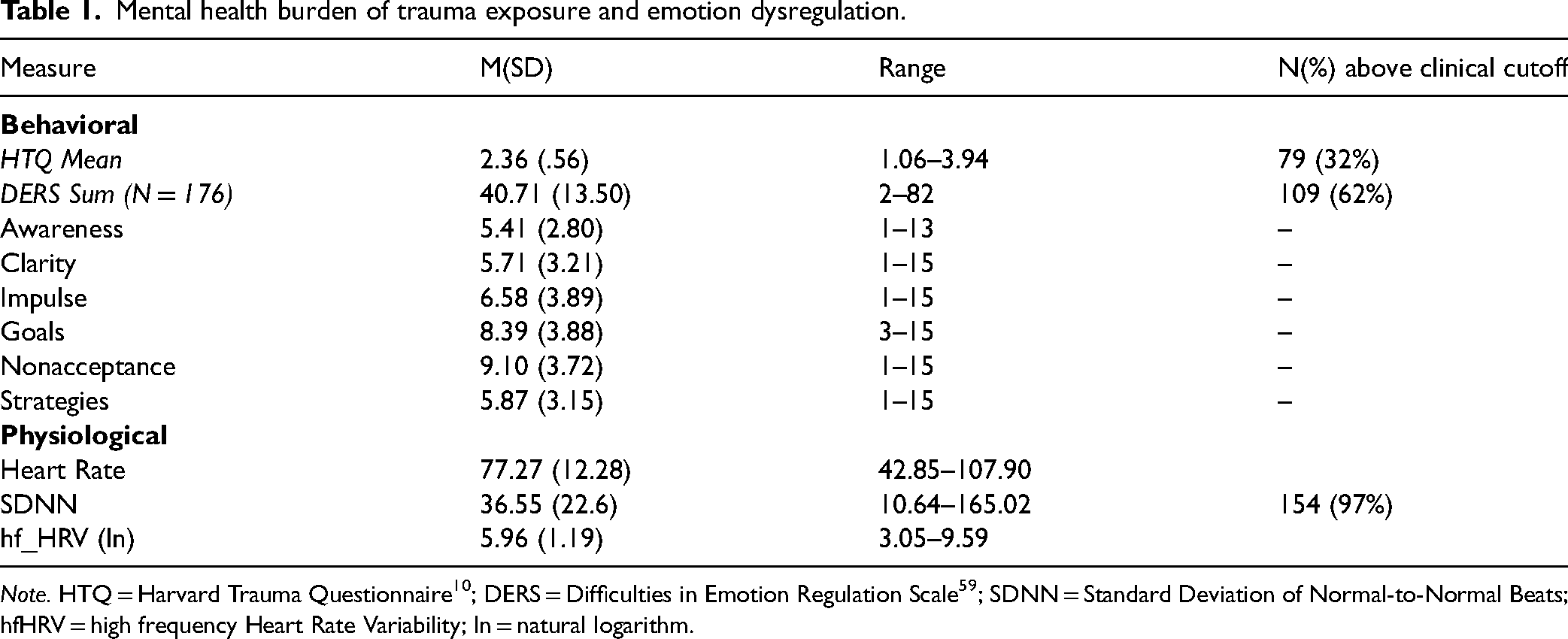
Subscale data are provided in Table 1. HTQ scores were on average 2.36 (SD = 0.56, range =1.06-3.94) on a 4-point Likert-scale. Seventy-nine (32%) participants met the clinical cut-off score of 2.5 for distress regarding presenting symptoms related to traumatic stress, the most endorsed being “feeling that you are the only one who suffered these events,” “avoiding thoughts or feelings associated with the hurtful events,” and “recurrent thoughts of memories of the most hurtful or terrifying events.” The DERS-18 yielded an average score of 2.48 (SD = 0.68, range 1-4.56) and mean total sum score of 40.7 (SD = 13.51) ; 109 (62%) met the suggested clinical cutoff for significant emotion dysregulation when calculated using mean scores. 51 Within the subscales, participants most frequently endorsed difficulties with emotional awareness and pursuing goals.
Mental health burden of trauma exposure and emotion dysregulation.
There were no differences in PTSD based on sex (t(189) = .22, p = .822) or age (r = .001, p = .991). Regarding emotion dysregulation, female participants had higher DERS-18 total scores (M = 42.42, SD = 13.07, t(170) = -1.29, p = .099) than males (M = 39.66, SD = 13.85) though this difference was insignificant. Similarly, DERS-18 total scores were uncorrelated with age (r = −.06, p = .466).
Aim 2: Describe the Indicators of Psychophysiological Stress among Adults in South Sudan
As expected, HR was inversely correlated with SDNN and hf-HRV (See Table 2). The majority of participants (86%, n = 137) in the sample had SDNN under the clinical cutpoint of 50 indicating elevated risk of cardiac event. 67 The average SDNN for the 159 participants with quality physiological data was 36.90 (SD = 22.29). Other parameter estimates are provided in Table 1 for descriptive purposes. Sex and age differences are included in the supplement.
Correlations between self-report and physiological measures.

Aim 3. Examine the Correspondence Between Self-Report and Physiology
PTSD symptoms were significantly positively correlated with overall affect dysregulation scores (see Table 2), as well as with the scores of each DERS subscale. PTSD symptoms were not correlated with any physiological measure (SDNN, hf-HRV), nor was overall DERS score (See Table 2). However, at the subscale level, the DERS subscale of “limited use of regulation strategies” was correlated with hf-HRV, such that people with higher parasympathetic activity also reported more difficulty with regulation strategies (See Table 3). Results were still significant when adjusting for age, which may affect hf-HRV. The DERS subscale of “lack of awareness” was significantly inversely correlated with mean HR, such that as difficulties with emotional awareness increased, mean HR decreased. (See Table 3) No nonlinear relations emerged.
Correlations between physiological variables and DERS subscales.

Note. DERS-SF = Difficulties in Emotion Regulation Scale Short Form 49 ; HR = Heart Rate; SDNN = Standard Deviation of Normal-to-Normal Beats; hf_HRV = high frequency Heart Rate Variability. Bold values indicate a result where p < .05.
Discussion
Of the approximately 200 participants who we assessed, over a third met the clinical cut-off for PTSD, which is three times higher than worldwide assessments, 71 but consistent with other estimates from South Sudan. Our PTSD findings support those of Ayazi 5 and Roberts’ 9 who found that 28% and 36% percent of South Sudanese participants met clinical cutoff for PTSD, respectively, demonstrating PTSD rates that are significantly higher than the global norm. Complementing this finding is the endorsement that all South Sudanese participants met the clinical cut-off for emotion dysregulation, indicating an inability to manage difficult emotion states, with their most prominent symptoms in the areas of emotional awareness and pursuing goal-directed behavior.
The psychophysiological findings pertaining to resting parasympathetic cardiac regulation speaks to the chronicity of South Sudan's inter and intra-tribal and ethnic regional conflicts spanning over three decades. Resting parasympathetic activity corresponds to individual ability to cope flexibly in response to stress. 72 Nearly 90% of the present sample had concerningly low scores on SDNN, when using benchmarks of norms from other samples, indicating autonomic dysregulation.59,66,67 This index further corresponds to the likelihood of experiencing a cardiac event in the near future, which is concerning given the relatively young age of the sample. These data highlight the critical need to understand and intervene upon contributions of stress to potentially shortened life spans within South Sudanese individuals, particularly combining interventions which address risk detection while simultaneously reducing sources of stress, including psychological stress and unattainable resources.
Regarding Aim 3, examining the relation of self report to psychophysiology: no cardiac index was correlated to self-reported PTSD symptoms. Nor were psychophysiological measures associated with overall emotion dysregulation measures, other than mean HR, though they were associated with subscales assessing limited use of regulation strategies. These findings offer several possible interpretations, conclusions, and directions for future research. First, the divergence between physiology and self-report raises the question of which is “right”. We suggest that they are both correct: they have both independently been shown to confer risk for quality of life and disease and lifespan mortality and morbidity. Future prospective work, particularly in this area, should examine these measures in aggregate and further parse how risk unfolds over time. Similarly, as the physiological data here suggest that participants had cardiovascular activity outside of expected age- and gender-adjusted ranges as measured by SDNN, 61 it is important to question whether the predictive value of these measures still functions the same in this context as it has been shown in other contexts. For example, work by Thayer and others73,74 has demonstrated higher HRV in marginalized groups. Since HRV is related positively to health and minoritized identities are related to poorer health, we must question whether HRV functions the same way in all contexts. An alternative is that these data capture a lifespan process as it unfolds, and, thus, prospective work on mental health and physiological risk is essential in settings highly saturated with trauma, stress, and conflict.
HF-HRV was, however, correlated with a sub-component of emotion dysregulation, particularly limited strategies for regulation. Perhaps paradoxically, hf-HRV correlated with limited emotion regulation strategies, suggesting that as individuals in this sample had increasing problems with utilizing regulation strategies, they also had increasing parasympathetic activation typically associated with better ability to regulate. 31 These findings appear consistent with the defense cascade framework 75 that hypothesizes a u-shaped relationship between parasympathetic activity and healthy regulation. Indeed, further work has uncovered evidence that as parasympathetic activity reaches a certain threshold, dissociative symptoms begin to increase.76,77 The particular DERS subscale that was correlated with SDNN and hf_HRV included items such as, “when I am upset, I believe that I will remain that way for a long time,” potentially capturing feelings of helplessness indicative of acute dissociation. We believe that our findings here suggest parasympathetic activity is psychobiologically protective to a point, but runs the risk of overcompensation particularly in the context of chronic exposure to traumatic conditions. Nevertheless, though consistent, these findings are preliminary and highlight the importance of further investigation of this relationship in such populations and across time.
Ultimately, these results paint a concerning yet complicated picture of mental health burden within a community in South Sudan, and yet demonstrate the impact of chronic stress and ongoing political violence on its residents. While the self-report and psychophysiological measures both were consistent with high levels of stress across the sample, minimal convergence of these measures may highlight the necessity of multi-method approaches to assessment in contexts with exceptionally high stress. Particularly given the complexity of the socio-political context within which this work occurred, the physiological measures were important in producing a more detailed assessment than is typically available in the literature outside of the Western context, and these data further demonstrate the feasibility of undertaking such assessment when partnering with local experts. Taken together, both the self-report and physiological results suggest a great need for context-specific and community-based intervention.
Supplemental Material
sj-docx-1-css-10.1177_24705470251324783 - Supplemental material for The Psychobiological Toll of Chronic Conflict: Posttraumatic Stress Symptoms, Emotion Dysregulation, and Physiology in a Conflict-Exposed Community in South Sudan
Supplemental material, sj-docx-1-css-10.1177_24705470251324783 for The Psychobiological Toll of Chronic Conflict: Posttraumatic Stress Symptoms, Emotion Dysregulation, and Physiology in a Conflict-Exposed Community in South Sudan by Kellie Ann Lee, Sarah Beranbaum, Vivian Khedari-DePierro, Ellen H. Yates, Ilya Yacevich, Anita Shankar, Condition Emmanuel Enosa, Tae Hwan Son, Greg J. Norman and Wendy D’Andrea in Chronic Stress
Footnotes
List of Abbreviations & Acronyms
Authors’ Contributions
IY and AS designed the program under evaluation. KAL, IY, AS, and WD designed the study, with WD serving as the senior author. CEE assisted with data collection and management. VKD assisted with data analysis. KAL, SB, and WD were primarily responsible for manuscript preparation, with assistance from AS, IY, and EHY. GJN assisted with physiological data interpretation. All authors reviewed the manuscript.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent for Publication
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Considerations and Consent to Participate
This study was conducted as the baseline portion of a program evaluation for GTP and was therefore deemed exempt by The New School Institutional Review Board. The project and authors complied with APA and Declaration of Helsinki guidelines. All participants provided general informed consent in English, Arabic, or the local dialect in the initial intake; subsequent, specific task consent was provided via verbal assent. To protect against any legal, political, or social repercussions, participants verbally assented to the TICE training and data collection rather than completing written consent forms.
Funding
Portions of this study, including the program being evaluated, were supported by UNDP- South Sudan, RFP Q-97/16 “Provision of Trauma Management and Psychosocial Support.” The senior author, WD, acknowledges the grant support of the Trauma Research Foundation in preparing this manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.