
Abstract
Background
Trauma-focused psychotherapy is treatment of choice for post-traumatic stress disorder (PTSD). However, about half of patients do not respond. Recently, there is increased interest in brain criticality, which assesses the phase transition between order and disorder in brain activity. Operating close to this borderline is theorized to facilitate optimal information processing. We studied if brain criticality is related to future response to treatment, hypothesizing that treatment responders’ brains function closer to criticality.
Methods
Functional magnetic resonance imaging resting-state scans were acquired from 46 male veterans with PTSD around the start of treatment. Psychotherapy consisted of trauma-focused cognitive behavioral therapy, eye movement desensitization and reprocessing, or a combination thereof. Treatment response was assessed using the Clinician-Administered PTSD Scale, and criticality was assessed using an Ising temperature approach for seven canonical brain networks (ie, the visual, somatomotor, dorsal attention, ventral attention, limbic, frontoparietal and default mode networks) to measure distance to criticality.
Results
The brains of prospective treatment responders were closer to criticality than nonresponders (P = 0.017), while no significant interaction effect between group and brain network was observed (P = 0.486). In addition, average criticality across networks correlated with future treatment response (P = 0.028).
Conclusion
These results show that the brains of prospective PTSD psychotherapy treatment responders operate closer to criticality than nonresponders, and this occurs across the entire brain instead of in separate canonical brain networks. These results suggest that effective psychotherapy is mediated by brains operating closer to criticality.
Keywords
Introduction
Post-traumatic stress disorder (PTSD) is a mental health condition that may develop after experiencing or witnessing a traumatic event. Key characteristics of PTSD are reliving the trauma, avoiding triggers associated with the trauma, negative changes in thoughts and emotions, and heightened arousal and reactivity. 1 Typically, PTSD treatment involves trauma-focused psychotherapy. 2 However, response rates are less than optimal, with 30%–50% of patients experiencing persistent symptoms after treatment. 3 Enhancing our comprehension of the neurobiological factors that differentiate responders from nonresponders prior to treatment is crucial for improving treatment outcomes.
Recent advancements in the field of brain criticality have prompted researchers to argue that this concept could serve as a valuable tool for investigating psychiatric disorders. 4
Brain criticality refers to the concept that neural activity organizes itself close to the borderline between order and disorder, which optimizes information processing.5,6 There is growing evidence of neural critical dynamics. For instance, in vitro and in vivo studies have shown neuronal ensembles firing at near-critical states,7–10 neuroimaging studies have observed critical dynamics in humans,11–13 and operating close to criticality ensures that neural communication can span the greatest distance. 14 Also, complex adaptive systems (eg, the brain) are more efficient in handling complex environmental conditions when operating near a critical point. 15 Overall, these findings point to healthy brains operating close to criticality. Indeed, several neural illnesses have been shown to deviate from near criticality, including epilepsy and neurodegenerative disease.16–19 Additionally, several psychiatric disorders have also been reported to deviate from an optimal critical point, 19 which can be improved by targeted interventions. For example, brains of patients with PTSD showed abnormal critical dynamics, which could be improved by neurofeedback, 20 and brains of patients with major depressive disorder also showed aberrant critical dynamics, which could be restored by mindfulness and stress education training 21 as well as electroconvulsive therapy. 22 Interestingly, brain criticality in treatment responders and nonresponders in the latter study were different prior to the start of treatment, suggesting that brain criticality may influence the effect of a psychiatric intervention.
In the present study, we build upon these findings by investigating if brain criticality in patients with PTSD is associated with prospective psychotherapy treatment response.
Since operating near criticality is linked with optimal information processing, and information processing is a cardinal component of effective psychotherapy, we hypothesize that prospective treatment responders operate closer to criticality than nonresponders around the start of treatment.
Methods
Participants
A cohort of 57 treatment-seeking military veterans with PTSD participated. Study procedures were identical to those described in Van Rooij et al 23 and Van Lutterveld et al. 24 To provide a brief overview, PTSD diagnosis was established by qualified psychologists and psychiatrists at the four Military Mental Health outpatient clinics in the Netherlands. Upon entry into the study, participants were around the start of trauma-focused psychotherapy. This encompassed trauma-focused cognitive behavioral therapy (tf-CBT) and/or eye-movement desensitization and reprocessing (EMDR) therapy, which are both recognized as recommended or suggested interventions for PTSD. 2 Trained researchers utilized the Clinician-Administered PTSD Scale (CAPS) 25 for Diagnostic and Statistical Manual of Mental Disorders (DSM)-IV to assess PTSD symptom severity at baseline and after 6–8 months. A structured clinical interview for DSM-IV axis I disorders (SCID-I/P) 26 was also administered at these timepoints to identify any comorbid psychiatric conditions. Baseline fMRI scans and clinical interviews were conducted as closely as possible to the onset of treatment. In this cross-sectional study with a longitudinal clinical component, data were acquired at University Medical Center Utrecht, the Netherlands and the Research Centre Military Mental Healthcare, Ministry of Defence, Utrecht, The Netherlands from 2010–2013. Inclusion criteria included deployment to a warzone and an age range of 18–60 years, while patients with a history of neurological disorders were excluded. Responders and nonresponders were categorized based on a threshold of a 30% reduction in CAPS scores at the second assessment following prior research.23,27,28 Out of the original group of 57 patients, two did not undergo treatment, four were lost to follow-up, and one was excluded as the being the sole female participant in the sample. Additionally, one participant was excluded because no resting-state scan was acquired. Three participants were further omitted from the study due to excessive head movement during data acquisition (see supplementary text S1 for further details), resulting in a final sample size of 46 PTSD patients. The study was approved by the Medical Research Ethics Committee of the University Medical Center Utrecht (approval nr NL29550.041.09) and all participants gave their written informed consent before participation in the study.
Image Acquisition and Data Preprocessing
Imaging and preprocessing were conducted identical to Van Lutterveld et al. 24 Supplementary text S1 provides detailed information.
Criticality Analysis
Brain criticality was assessed using an Ising temperature approach similar to Ruffini et al, 29 which is an equilibrium model for dynamical data. In short, the Ising model of ferromagnetism is a model from statistical physics, in which the system undergoes a phase transition from order (ie, ferromagnetism) to disorder (ie, paramagnetism) at a critical temperature. 30 Ising models can robustly and accurately be fitted to resting-state fMRI data, and reflect anatomical connections more accurately than conventional functional connectivity. 31 Ising models have been applied to fMRI data within the context of intelligence, alternate states of consciousness due to sedative ingestion, and lysergic acid diethylamide (LSD) intake.29,32,33 Supplementary text S2 provides detailed information regarding criticality analysis. Briefly, the entire resting-state dataset was fitted to an Ising model, after which the obtained model was personalized by adjusting the model for each individual. Ising temperatures were assessed separately for seven canonical brain networks, using the cross-reference list provided by DPARSFA that labels each Brainnetome ROI according to Yeo's seven canonical brain networks (ie, the visual, somatomotor, dorsal attention, ventral attention, limbic, frontoparietal and default mode networks). 34 Supplementary figure S3 provides a visual representation of these canonical networks.
Statistical Analysis
Main Analysis
Outliers were identified using Tukey's inner fences and removed from analysis. 35 Relationships of Ising temperature with age were assessed using standard linear regression with the lm function in RStudio and R (versions 2023.12.1 + 402 and 4.3.1 respectively). As there is evidence that criticality is associated with intelligence,32,36 relationships with education level were also assessed. Because the baseline assessment took place around the onset of psychotherapy, some patients had already undergone therapy sessions before this initial measurement (see Table 1). As such, the relationship of Ising temperature with the number of pre-baseline therapy sessions was tested similarly. Significant-covariate adjusted effects were analyzed using the Anova Type Statistic (ATS) of the R package nparLD, which is specifically designed for non-parametric analysis of repeated measures data in factorial designs (between-subjects factor: group and within-subjects factor: brain network). 37 Analyses were repeated with outliers included.
Demographics and clinical data

CAPS: clinician administered PTSD scale, EMDR: eye movement desensitization and reprocessing, ISCED: international scale for education, IQR: interquartile range, SARI: serotonin antagonist and reuptake inhibitor, SCID: structured clinical interview for DSM IV Axis I disorders, SSRI: Selective Serotonin Reuptake Inhibitor, tf-CBT: trauma-focused cognitive behavioral therapy.
*Number of cases with missing data: education mother responders n = 1; education mother non-responders n = 2; education father responders n = 2; education father non-responders n = 1; time since last deployment non-responders n = 1; number of times deployed non-responders n = 1; early traumatic experiences responders n = 2; early traumatic experiences non-responders n = 1; total number of received therapy sessions responders n = 5; SCID post-treatment non-responders n = 1.
Mann Whitney U test.
Fisher-Freeman-Halton exact test.
Fisher's exact test.
χ2-test.
Exploratory Correlation Analyses
Significant findings in the main analysis were further explored using Spearman's rho. Outliers were identified using Tukey's inner fences and removed from analysis.
Sensitivity Analysis of Residual Head Motion as a Potential Confounder
To investigate whether residual head motion was associated with brain network Ising temperature, average framewise displacement (FD) was correlated with Ising temperature of each brain network using Spearman's rho.
Results
Participants
Twenty-four patients were classified as treatment responders and 22 as nonresponders. Two responders and three nonresponders were identified as outliers in criticality values based on Tukey's inner fences and removed from the main analysis. At baseline, no significant differences were observed between groups regarding any demographics, therapy parameters, comorbidities, or medication usage. Table 1 provides information regarding demographics and clinical data per group. Improvement in symptoms in the responder compared to the nonresponder group was observed across all three PTSD symptom clusters: re-experiencing, avoidance, and hyperarousal.
Criticality Analysis
Supplementary text S4 and figure S5 provide detailed information about Ising model validation, showing that the model was accurate. Age was a significant covariate for six out of the seven brain networks (F(1,39)=-values ranging from 5.849–19.605 and P-values ranging from <0.001–0.020) except the limbic network (F(1,39) = 0.465, P = 0.499), while education level and number of pre-baseline treatment sessions were not (F(1,39) values ranging from 0.001–1.415 and P-values ranging from 0.241–0.972). As such, age was included as a covariate for all networks except the limbic network, and education level and pre-baseline treatment were not. A main effect of group was observed (ATS = 5.704, P = 0.017), while no significant interaction effect between group and brain network was observed (ATS = 0.884, P = 0.486). Figure 1 provides a graphical overview of criticality per brain region. The median increase in Ising temperature in nonresponders compared to responders across networks was 6.69% (range 3.86-8.28). Across all networks, individual Ising temperatures ranged from 0.80 to 1.24. As criticality (the border between order and disorder) was observed at temperatures of around 0.3 to 0.4 for the various brain networks (see supplementary figure S6), these results show that the brain networks of both treatment responders and nonresponders operated above criticality (ie, in a disordered, or paramagnetic phase), and responders were closer to criticality than nonresponders. Repeating the analysis without outlier removal yielded similar results (significant main effect of group: ATS = 4.570, P = 0.033) and no significant interaction effect: ATS = 0.557, P = 0.732).
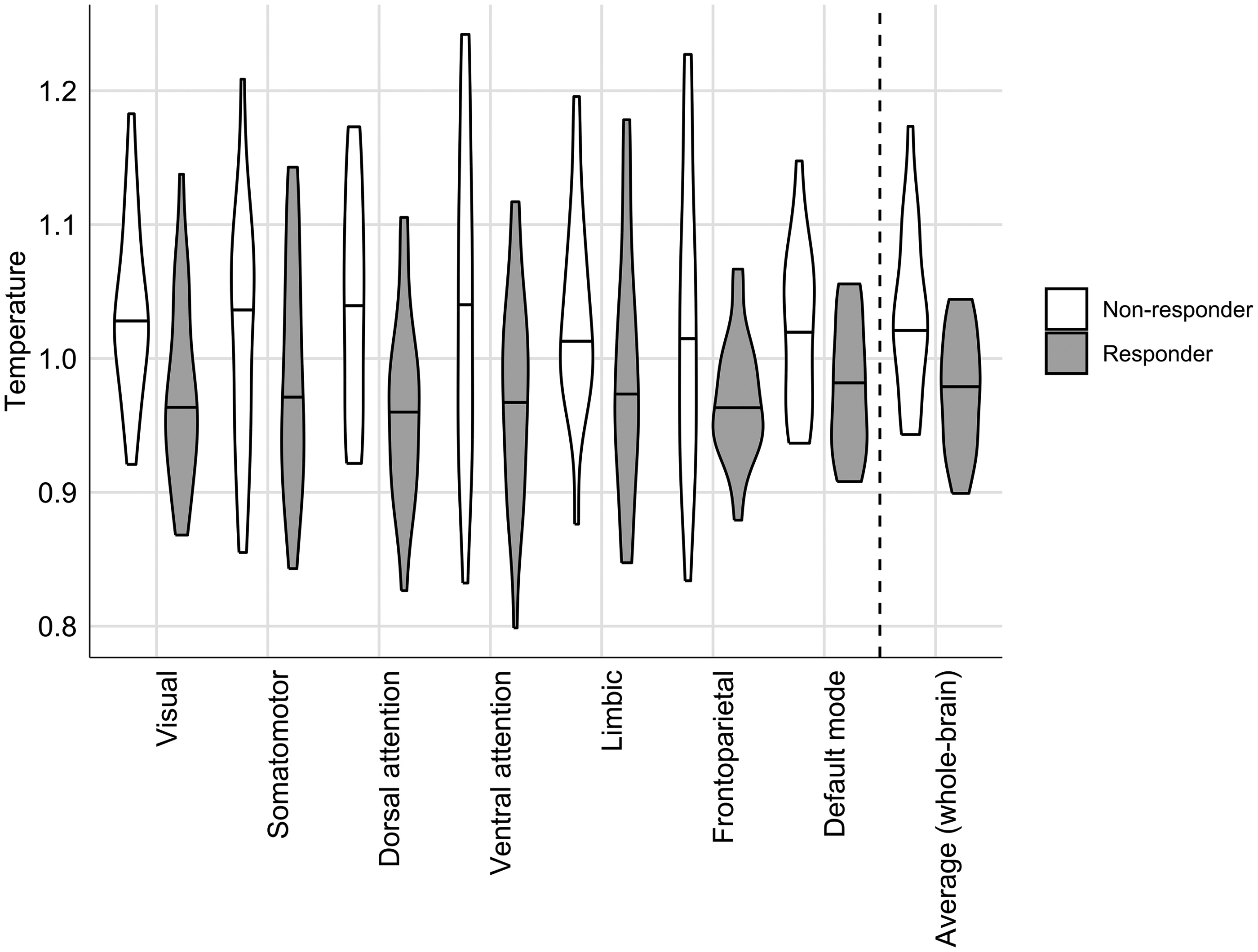
Criticality per network and average criticality across networks.
Exploratory Correlation Analyses
Spearman's correlation analyses revealed positive correlations between average brain criticality and change in total CAPS score (ρ = 0.328, P = 0.028) as well as change in the hyperarousal scale of the CAPS interview (ρ = 0.373, P = 0.014). No significant correlations were observed for changes with the re-experiencing and avoiding subscales (ρ = 0.152, P = 0.324) and ρ = 0.245, P = 0.105 respectively). Although significant associations of age with criticality in 6 out of 7 networks were observed (see previous paragraph), no significant correlations were observed between age and changes in total CAPS scores and its subscales, and as such no partial correlation analyses correcting for age were performed. Supplementary table S8 provides statistics regarding correlations between criticality of each network and change in CAPS total and subscale scores.
Sensitivity Analysis of Residual Head Motion as a Potential Confounder
No significant correlations between head motion and Ising temperature were observed for 6 out of 7 brain networks (ρ-values ranging from −0.123-0.214 and P-values ranging from 0.178-0.719), while a significant correlation was observed for the default mode network (ρ = 0.328, P = 0.037). Repeating the criticality analysis without this network yielded similar results to the main analysis, with a significant main effect of group (ATS = 5.153, P = 0.023) and no significant interaction effect (ATS = 0.939, P = 0.440). Repeating this analysis without outlier removal also yielded similar results (a significant main effect of group: ATS = 3.86, P = 0.050) and no significant interaction effect (ATS = 0.543, P = 0.716). These results suggest that the preprocessing procedure was relatively effective in mitigating motion effects for six out of seven brain networks.
Discussion
To our knowledge, this is the first study to investigate brain criticality related to future psychotherapy treatment response. We confirmed our hypothesis that responders to trauma-focused psychotherapy operated closer to criticality than nonresponders around the start of therapy. In addition, this effect occurred across the entire brain instead of in separate canonical brain networks.
These results suggest that brain regions operating closer to criticality predispose patients with PTSD to benefit from psychotherapy. There is some evidence that operating close to criticality is associated with cognitive flexibility and cognitive control,38,39 which are important factors in effective interventions for PTSD.40–42 Both of these factors are building blocks of intelligence.43,44 Indeed, a recent study observed that patients with higher intelligence scores showed a greater reduction in PTSD symptoms after finishing cognitive therapy. 45 Interestingly, two recent resting-state fMRI studies observed a relationship between distance to criticality and fluid intelligence,32,36 which is the ability to think abstractly and solve novel reasoning problems without relying on prior knowledge or experience, and is correlated with learning. 46 This relationship persisted after age and education achievement regression. 36 This may provide a potential explanation for the link between criticality and treatment response observed in the current study. Although the current study did not observe a significant association between education level and criticality, and there were no significant differences in education level between groups at α = 0.05, education level of responders was higher than nonresponders at the trend-level. As education and intelligence are associated (eg, see 47 ), this also points to intelligence possibly explaining (partly) the association between treatment response and distance to criticality. A notable difference between the Xu et al study and the current findings is however that their measure of critical dynamics (synchronization entropy) showed significant associations mainly with frontoparietal areas (including the inferior parietal lobule), while the current study observed an effect across all canonical brain regions. Importantly, as the current study did not test for fluid intelligence or cognitive flexibility, the effects of these factors could not be established. There is however some support for cognitive control, as in an overlapping sample brain activity in the inferior parietal lobule (which was also implicated in the Xu et al study) predicted future PTSD psychotherapy treatment response in a contextual stop-signal task. 48
Prior research has demonstrated that neurofeedback training can enhance brain criticality. In a study utilizing electroencephalography (EEG), participants engaged in neurofeedback aimed at reducing alpha-band power, which led to improvements in critical brain dynamics. A subsequent experiment investigated criticality in patients with PTSD, revealing that these individuals exhibited atypical critical dynamics relative to healthy controls. When the PTSD patients completed the neurofeedback protocol, their critical dynamics normalized, with the observed changes correlating with reductions in arousal symptoms (Ros et al, 2017). Interestingly, the current study also identified a link between criticality and arousal, with criticality being predictive of future change in hyperarousal symptoms. Although significant methodological differences exist between the neurofeedback study and the present one (eg, criticality measurement with EEG vs fMRI, and using Detrended Fluctuation Analysis vs an Ising model), these findings raise the possibility that neurofeedback could serve as a preparatory intervention to enhance brain criticality prior to trauma-focused psychotherapy, potentially increasing the probability of a favorable therapeutic outcome.
In the current study, Ising model temperatures were above the critical point across all brain networks and participants. This finding aligns with other recent fMRI studies, which also reported supercritical dynamics.29,32,33
Limitations
The findings should be interpreted considering several limitations. Several patients had already initiated therapy prior to baseline assessment. Six treatment responders (out of 24) and seven nonresponders (out of 22) had received therapy prior to the baseline CAPS interview and fMRI scan. This was because of scheduling issues with the MRI scanner, and suspending treatment for research purposes was considered unethical. Nevertheless, the current results are not expected to be greatly influenced, as there were no significant differences between groups in the type or amount of these therapy sessions, and no relationship between the number of sessions and Ising temperature for any brain network was observed. Also, PTSD is a heterogeneous construct, and it was for example not known how many patients in the study were suffering from dissociation, which can influence treatment response49,50 or how many had PTSD that was childhood trauma related as the index trauma. In addition, eight occipital ROIs were excluded from analysis as they were not included in the field of view (FOV) in all participants, which may have affected results for the visual network. It is furthermore important to note that the present results should be interpreted in context of the applied spatial scale, as the choice for region-based or voxelwise approaches might influence results. Also, patients underwent a mix of trauma-focused psychotherapies, reflecting the personalized approach to trauma-focused therapy used in our clinics. Consequently, the findings of the study cannot be attributed to a singular therapy modality. It should be further emphasized that the current study focused on male veterans, and therefore, the findings may not be applicable to civilian populations or female individuals. Finally, the findings should be interpreted in light of the relatively small sample size, and should be considered preliminary until replication.
Conclusion
Brains of patients with PTSD who responded well to psychotherapy operated closer to criticality than nonresponders. These results suggest that effective psychotherapy is mediated by brains operating closer to criticality. Future research could focus on replicating this finding in a larger sample, investigate the effects of fluid intelligence, cognitive flexibility and cognitive control, and assess whether neurofeedback to improve brain criticality may enhance psychotherapy treatment response.
Supplemental Material
sj-docx-1-css-10.1177_24705470241311285 - Supplemental material for Criticality is Associated with Future Psychotherapy Response in Patients with Post-Traumatic Stress Disorder—A Pilot Study
Supplemental material, sj-docx-1-css-10.1177_24705470241311285 for Criticality is Associated with Future Psychotherapy Response in Patients with Post-Traumatic Stress Disorder—A Pilot Study by Remko van Lutterveld, Myrthe Sterk, Cristian Spitoni, Mitzy Kennis, Sanne J. H. van Rooij and Elbert Geuze in Chronic Stress
Footnotes
Acknowledgments
During the preparation of this work the authors used ChatGPT in order to improve readability and language. After using this tool/service, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
Author Contributions
Remko van Lutterveld: Conceptualization, Formal analysis, Writing—original draft, Writing—review and editing.
Myrthe Sterk: Formal analysis, Writing—original draft, Writing—review and editing.
Cristian Spitoni: Formal analysis, Writing—original draft, Writing—review and editing.
Mitzy Kennis: Conceptualization, Writing—original draft, Writing—review and editing.
Sanne J.H. van Rooij: Conceptualization, Writing—original draft, Writing—review and editing.
Elbert Geuze: Conceptualization, Writing—original draft, Writing—review and editing.
Consent to Participate
All participants gave their written informed consent before participation in the study.
Data Availability
Anonymized preprocessed fMRI data are available upon reasonable request from any qualified investigator.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The Editor-in-Chief of Chronic Stress is an author of this paper, therefore, the peer review process was managed by Sage's in-house editorial team, and the submitting Editor was not involved in the decision-making process.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Mental Health (grant number K01MH121653) and the Brain and Behavior Research Foundation (NARSAD Young Investigator Award) for SvR. The other authors received no specific grant from any funding agency, commercial or not-for-profit sector.
Ethical Considerations
The study was approved by the Medical Research Ethics Committee of the University Medical Center Utrecht (approval nr NL29550.041.09).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.