
Abstract
Background
Greater unhelpful thinking is associated with greater musculoskeletal discomfort and incapability. Cognitive-behavioral therapy (CBT) fosters healthy thinking to help alleviate symptoms.
Questions
In a meta-analysis of randomized control trials (RCT) of CBT for unhelpful thinking among people with musculoskeletal symptoms, we asked: 1) Does CBT reduce unhelpful thinking and feelings of distress, and improve capability, in individuals with musculoskeletal symptoms? 2) Are outcomes affected by CBT delivery methods?
Methods
Following QUOROM guidelines, we searched databases using keywords of pain catastrophizing, kinesiophobia, cognitive-behavioral therapy, musculoskeletal and variations. Inclusion criteria were RCT's testing CBT among people with musculoskeletal symptoms. Study quality was assessed with Cochrane Review of Bias 2. Meta-analysis of means and standard deviations was performed.
Results
CBT led to modest reductions in catastrophic thinking (−0.44 CI: −0.76 to −0.12; P = .01, kinesiophobia (−0.60 CI: −1.07 to −0.14; P = .01) and anxiety symptoms (−0.23 CI: −0.36 to −0.09; P < .01) over six months compared to usual care. There were no improvements in levels capability (−0.28 CI: −0.56 to 0.01; P = .05). CBT led by mental health professionals reduced catastrophic thinking more than CBT led by other clinicians (QB Test = 4.73 P = .03). There were no differences between online and in-person sessions, group versus individual therapy, or surgical versus non-surgical interventions.
Conclusion
The evidence that CBT delivered by various clinicians in various settings fosters healthier thinking in people presenting for care of musculoskeletal symptoms, supports comprehensive care of musculoskeletal illness. More research is needed to develop indications and interventions that also improve levels of capability. Level-I, meta-analysis of RCT's
Keywords
Introduction
Background
Unhelpful thinking and feelings of distress account for a notable amount of the variation in levels of discomfort and incapability among people with musculoskeletal symptoms.1–4 Unhelpful thinking related to pain–a product of human mental short-cuts (heuristics) or automatic thoughts–includes catastrophic or worst-case thinking, 5 fear of painful movement (kinesiophobia), 6 negative pain thoughts, 7 and intolerance of uncertainty.8,9 As an example of unhelpful thinking, patients recovering from back surgery do better when they regard the surgical pain as an expected part of recovery rather than as a threat. 1 Given the relationship of unhelpful thinking to greater levels of discomfort and incapability for musculoskeletal conditions, psychological interventions that can reduce catastrophic thinking have the potential to improve health.10–12 One such intervention, cognitive behavioral therapy (CBT), comprises mindset exercises that can foster healthy thinking. 13
Rationale
A systematic review of randomized trials among people with ongoing low back pain found that CBT was associated with a long-term reduction in levels of discomfort and incapability relative to no treatment or other guideline approved treatments. 14 Another systematic review among patients undergoing lumbar spine surgery found that patients who participated in CBT experienced greater capability and lower kinesiophobia compared to people who received usual care or other treatments. 5 Both these analyses addressed specific circumstances and included one study by a senior author that had 3 studies retracted due to concerns regarding research misconduct. 15 Using funnel plots we confirmed that these studies were outliers that could cause distortions.
Questions
We reviewed prospective randomized trials comparing a CBT intervention with other interventions among people with any musculoskeletal illness and asked: 1 Is CBT associated with reduction of unhelpful thinking and feelings of distress, and an increase in capability? And 2) Are there differences based on how the CBT is delivered?
Materials and Methods
We followed the QUOROM (Quality of Reporting of Meta-analyses) guidelines. 16
Search Strategy and Criteria
A database and reference list search of PUBMED, Google Scholar, and Cochrane Library was performed using the keywords: “pain catastrophizing”, “kinesiophobia”, “intolerance of uncertainty”, “negative pain thoughts”, “cognitive behavioral therapy”, “musculoskeletal”, and “unhelpful thinking”. The database search was supplemented with hand-searching through bibliographies. No restrictions were applied to the date of publication.
Inclusion and Exclusion Criteria
Studies included in the analysis were (1) randomized control trials, (2) used CBT interventions, (3) treated patients with musculoskeletal symptoms, (4) published in English and (5) measured outcomes related to unhelpful thinking (pain catastrophizing, kinesiophobia, negative pain thoughts, intolerance of uncertainty).
Studies were excluded if they (1) had a level of evidence 2-5, (2) were published only as an experimental protocol or abstract, or (3) if standard deviations were not available. Two reviewers applied these criteria. Disagreements were discussed and resolved by the senior author.
We initially identified 428 articles, 396 did not meet criteria and were excluded. (Figure 1) This review included 19 randomized control trials consisting of 2361 patients assessing the effect of CBT on both mindsets (pain catastrophizing, kinesiophobia, symptoms of anxiety) and capability. (Table 1)
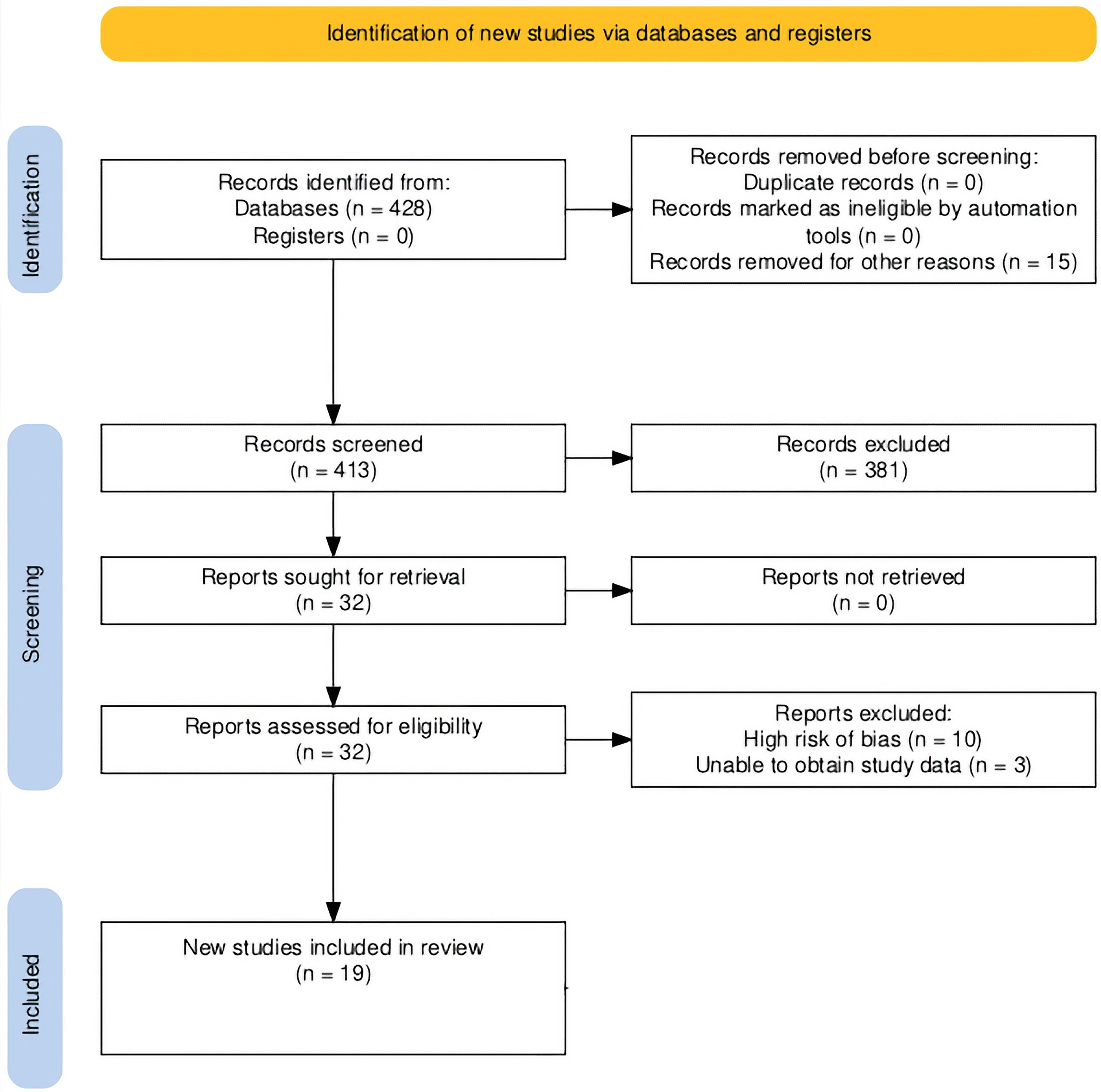
This flowchart shows article selection according to the preferred reporting items for systematic reviews and Meta-analysis guidelines. 17
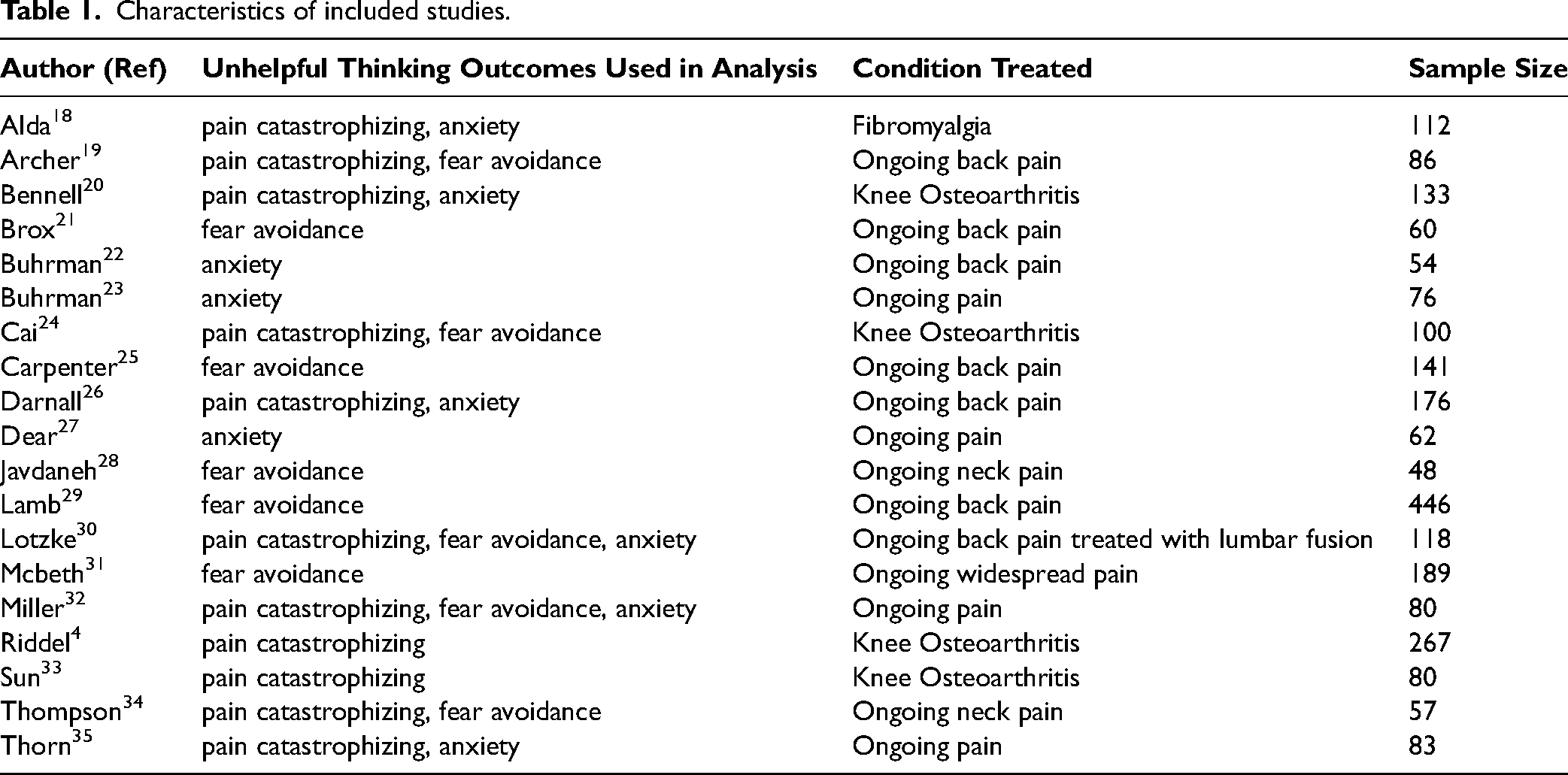
Characteristics of included studies.
Assessment of Study Quality
Selected studies were independently assessed, without masking the source of authorship, by two authors using the Cochrane Review of Bias 2 (Rob2) tool. 36 Disagreements were discussed and resolved by the senior author.
Data Collection and Abstraction
For each eligible study, we extracted baseline and 6-month (or the nearest time point) means and standard deviations for both the treatment and control group for all measures of unhelpful thinking and function found within the study. We also recorded treatment approach (surgical or conservative), format of CBT delivery (group or individual), mode of CBT administration (in-person or online), whether studies screened for unhelpful mindsets, and whether CBT session leaders were mental health providers or physical therapists. The two reviewers extracted data from all eligible studies. Disagreements were discussed and resolved by the senior author. If the relevant data could not be derived from the publication, the corresponding author was emailed, and the relevant data was requested.
Meta-Analysis Methodology
Heterogeneity was assessed using I2, which indicates percentage of variance in the meta-analysis that can be attributed to study heterogeneity for studies pertaining to both research questions. Given that there was considerable heterogeneity, a random-effects model was used.
Forest plots were created to better visualize the impact of CBT on reducing unhelpful thinking (pain catastrophizing, kinesiophobia) and feelings of distress (symptoms of anxiety) and aspects of capability (strength, mobility, range of motion, or ability to complete activities of daily living such as bathing and doing chores around the home) when compared to control treatments in randomized trials.
To understand what settings and factors are associated with the effectiveness of CBT, random effects model Forest plots were created to visualize the surgical/non-surgical intervention, group/individual therapy, online/in-person sessions, mental health provider versus physical therapist led sessions, and the use of a maladaptive thinking cutoff. A P value of < .05 was considered statistically significant. Analyses were performed using STATA 15.1 (Stata Corporation, College Station, TX). Adequate data for meta-analysis was not available for comparing 1) the effect of CBT on functional outcomes, kinesiophobia (fear avoidance), anxiety, and pain catastrophizing in pre-operative versus post-operative settings; and 2) online CBT sessions versus in-person sessions for kinesiophobia (fear avoidance), anxiety, and pain catastrophizing. Funnel plots were created for each of the primary outcomes measured in this study to assess for positive outcome bias (See Figure, Online Supplemental Material1).
Results
Is CBT Associated with Reduced Unhelpful Thinking, Reduced Feelings of Distress, and Increased Capability?
Patients participating in CBT experienced modest reductions in pain catastrophizing (mean difference (MD) = −0.44; 95% CI: −0.76 to −0.12; P = .01), kinesiophobia (MD = −0.60; 95% CI: −1.07 to −0.14; P = 0.01), and symptoms of anxiety (MD = −0.23; 95% CI: −0.36 to −0.09; P < .01) 6 months after initiation of treatment compared to usual care (Figures 2, 3 and 4). Aspects of capability, including strength, mobility, and activities of daily living, were not significantly different between CBT and usual care (MD = −0.28; 95% CI: −0.56 to 0.01; P = 0.05; Figure 5).
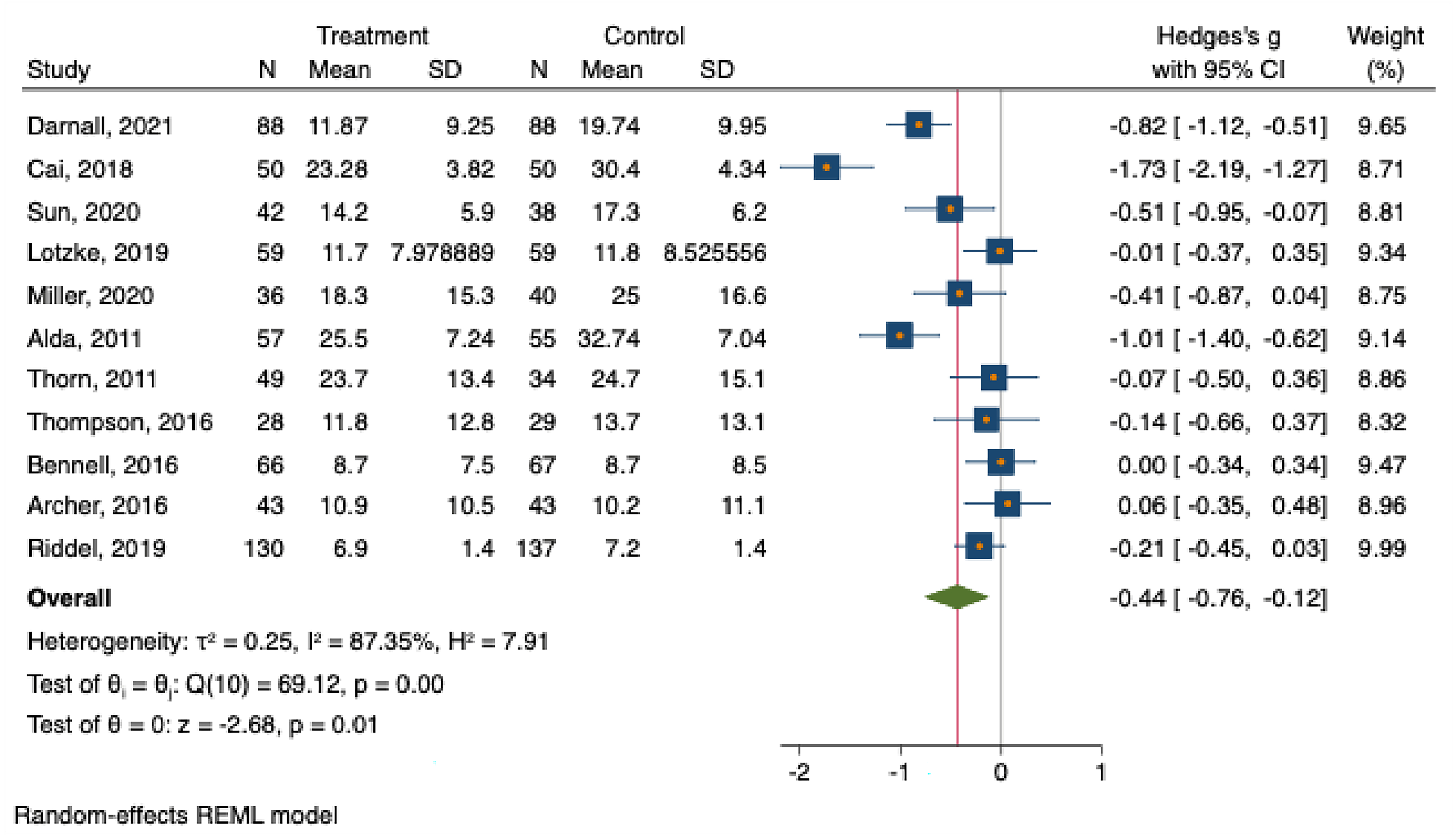
This forest plot shows the difference in pain catastrophizing scale score between groups treated with CBT compared with controls.
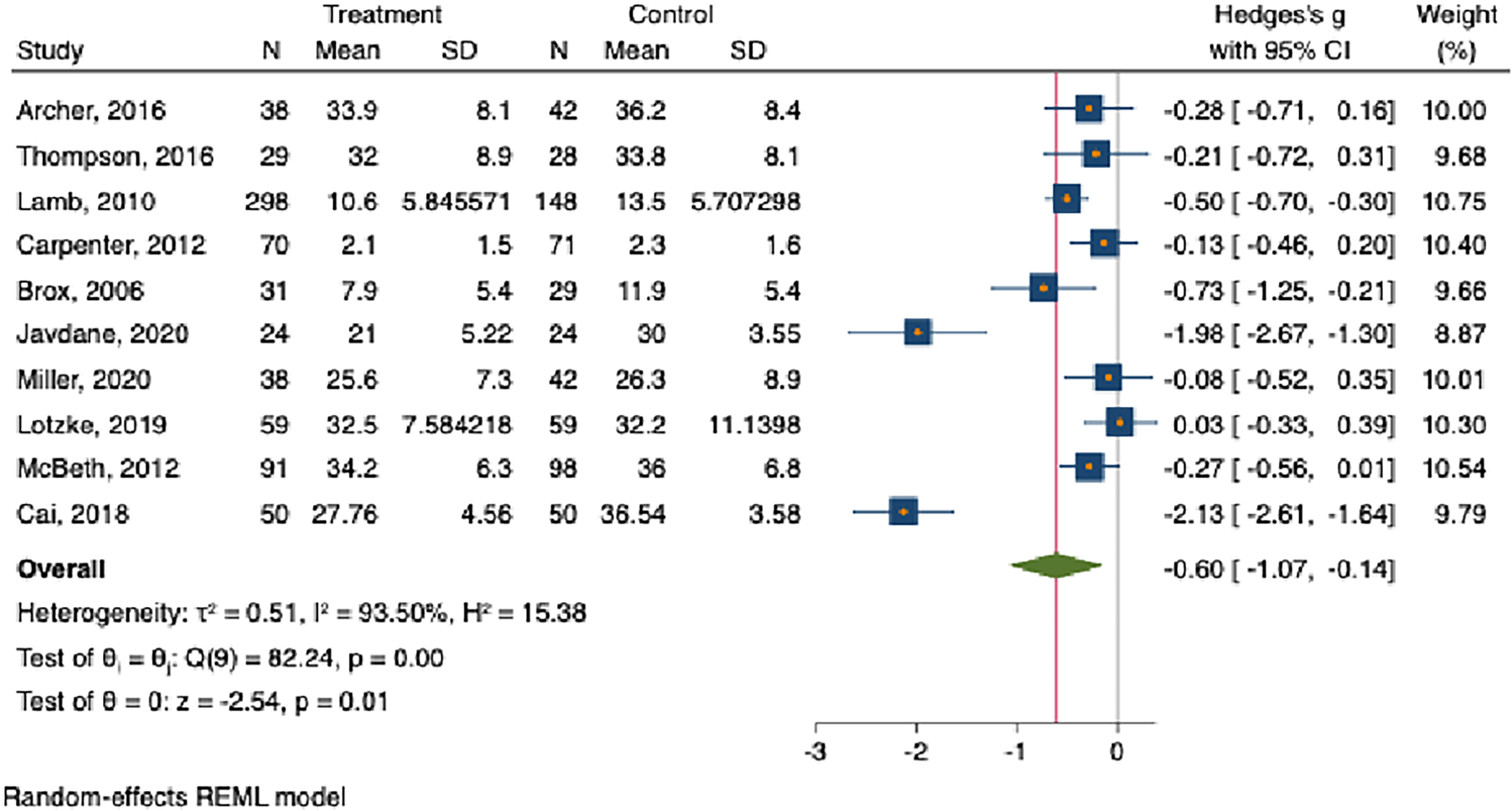
This forest plot shows the difference in levels of fear avoidance between groups treated with CBT compared with controls.
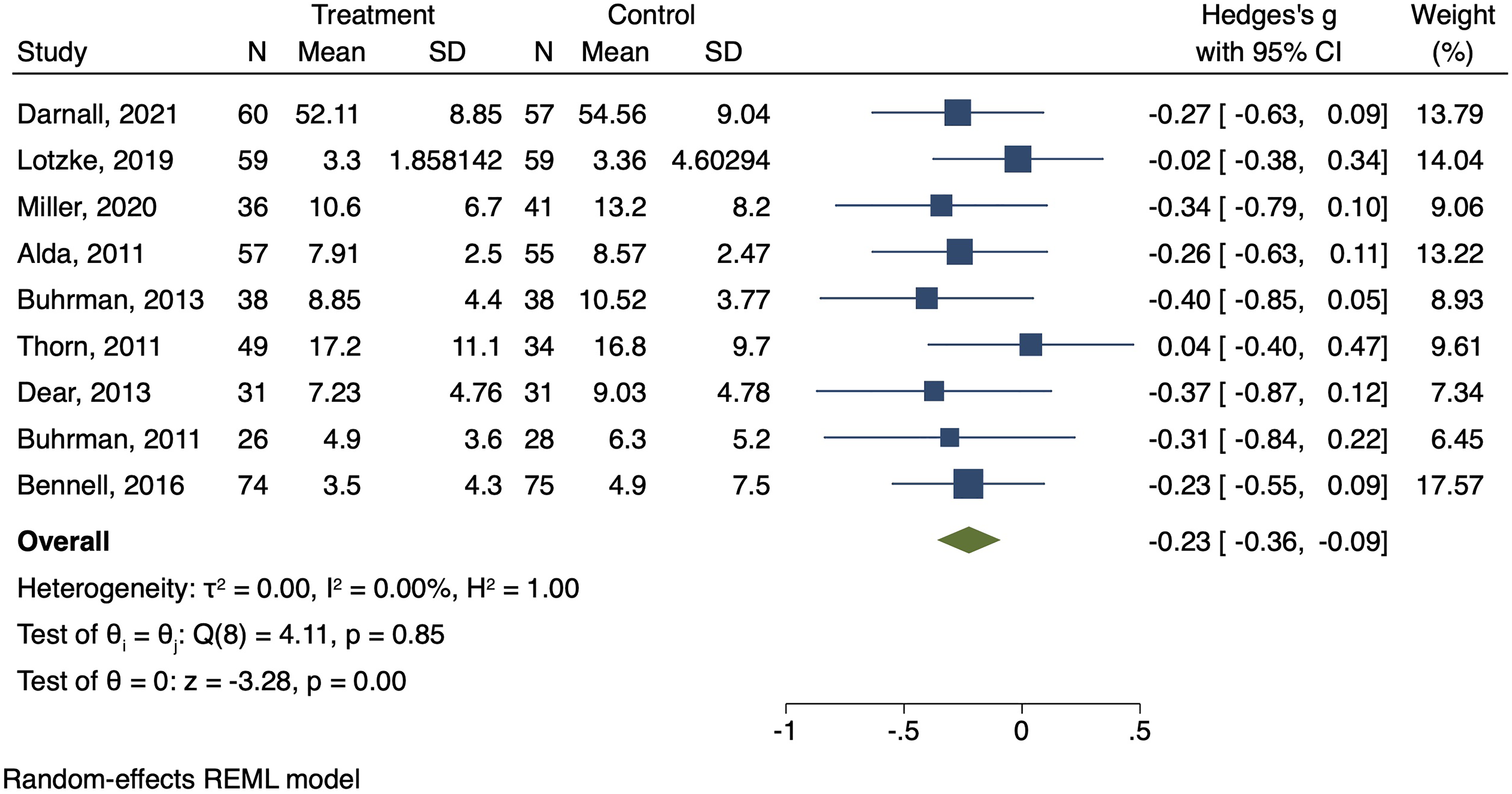
This forest plot shows the difference in levels of anxiety related to pain between groups treated with CBT compared with controls.

This forest plot shows the difference in outcomes related to function including strength, mobility, and activities of daily living between groups treated with CBT compared with controls.
Are There Differences Based on how CBT is Delivered?
Participants in mental health-led groups experience a greater reduction in pain catastrophizing (MD = −0.9; 95% CI: −1.56 to −0.2) compared to physical therapist-led groups (MD = −0.16; 95% CI: −0.30 to −0.02; Test of group differences: Qb = 4.73, P = 0.03; Figure 6A). Both groups showed similar improvements in kinesiophobia, symptoms of anxiety, and daily activities (Figure 6B, C and D). Both operative and non-operative groups exhibited similar reductions in pain catastrophizing (MD = −0.60; 95% CI: −1.35 to 0.14 vs MD = −0.35; 95% CI: −0.67 to −0.03) (Test of group differences: Qb = 0.37, P = .54; Figure 7A). Group and individual CBT sessions had comparable reductions in catastrophic thinking (MD = −0.28; 95% CI: −0.43 to −0.13 vs MD = −0.30; 95% CI: −0.71 to 0.10) (Test of group differences: Qb = 0.01, P = .91; Figure 8A). Both in-person and virtual sessions led to similar changes in function (MD = −0.43; 95% CI: −0.69 to −0.17 vs MD = 0.03; 95% CI: −1.08 to 1.15) (Test of group differences: Qb = 0.63, P = 0.43; Figure 9). Regarding studies screening for unhealthy mindsets, no significant differences were noted in pain catastrophizing, kinesiophobia, symptoms of anxiety, or functional outcomes (Figure 10A, B, C, and D). Participants with higher baseline unhelpful thinking levels experienced similar reductions in kinesiophobia compared to those with normal and higher baseline levels (MD = −1.45; 95% CI: −2.63 to −0.27 vs MD = −0.30; 95% CI: −0.71 to 0.10) (Test of group differences: Qb = 3.47, P = 0.06; Figure 10B). The largest effect sizes were found in 2 out of the 4 studies that screened and included only patients with the least healthy mindsets.24,28
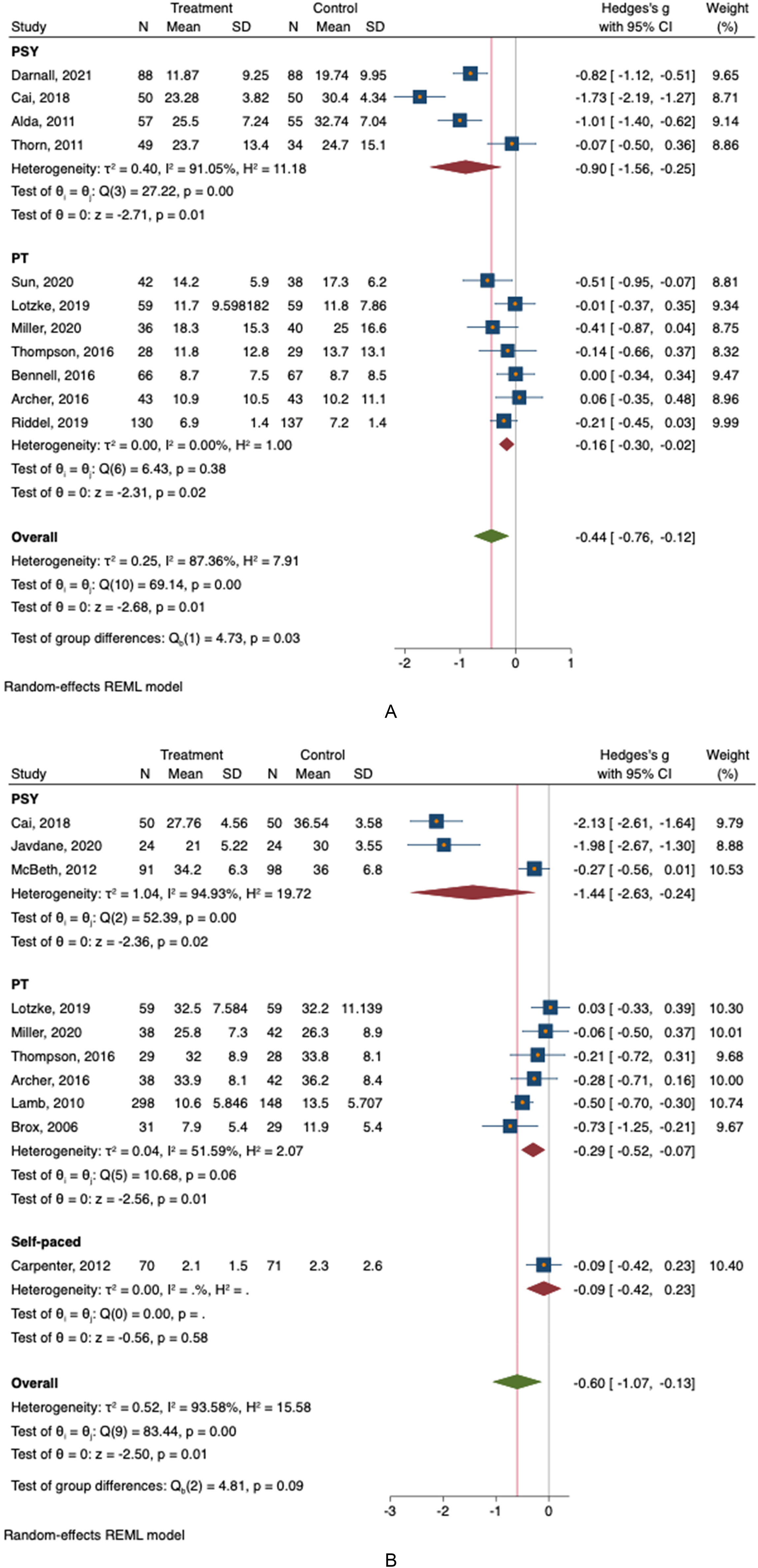
A. This forest plot shows the difference in levels of catastrophic thinking when CBT is led by physical therapists versus mental health providers, each against usual care. N = sample size, SD = standard deviation, REML = restricted maximum likelihood. B. This forest plot shows the difference in levels of fear avoidance when CBT is led by physical therapists versus mental health providers, each against usual care. N = sample size, SD = standard deviation, REML = restricted maximum likelihood. C. This forest plot shows the difference in levels of symptoms of anxiety related to pain when CBT is led by physical therapists versus mental health providers, each against usual care. N = sample size, SD = standard deviation, REML = restricted maximum likelihood. D. This forest plot shows the difference in outcomes related to function including strength, mobility, and activities of daily living when CBT is led by physical therapists versus mental health providers, each against usual care. N = sample size, SD = standard deviation, REML = restricted maximum likelihood.

A. This forest plot compares the impact of CBT on catastrophic thinking in patients treated with operative care versus patients treated with non-operative care, each against usual care interventions. N = sample size, SD = standard deviation, REML = restricted maximum likelihood. B. This forest plot compares the impact of CBT on fear avoidance in patients treated with operative care versus patients treated with non-operative care, each against usual care interventions. N = sample size, SD = standard deviation, REML = restricted maximum likelihood. C. This forest plot compares the impact of CBT on anxiety related to pain thoughts in patients treated with operative care versus patients treated with non-operative care, each against usual care interventions.

A. This forest plot compares the impact of group CBT versus individual CBT sessions on catastrophic thinking, each against usual care interventions. B. This forest plot compares the impact of group CBT versus individual CBT sessions on fear avoidance, each against usual care interventions. C. This forest plot compares the impact of group CBT versus individual CBT sessions on anxiety related to pain, each against usual care interventions.

This forest plot compares the impact of online CBT versus in-person CBT sessions on outcomes related to function, including strength, mobility, and activities of daily living, against usual care interventions.
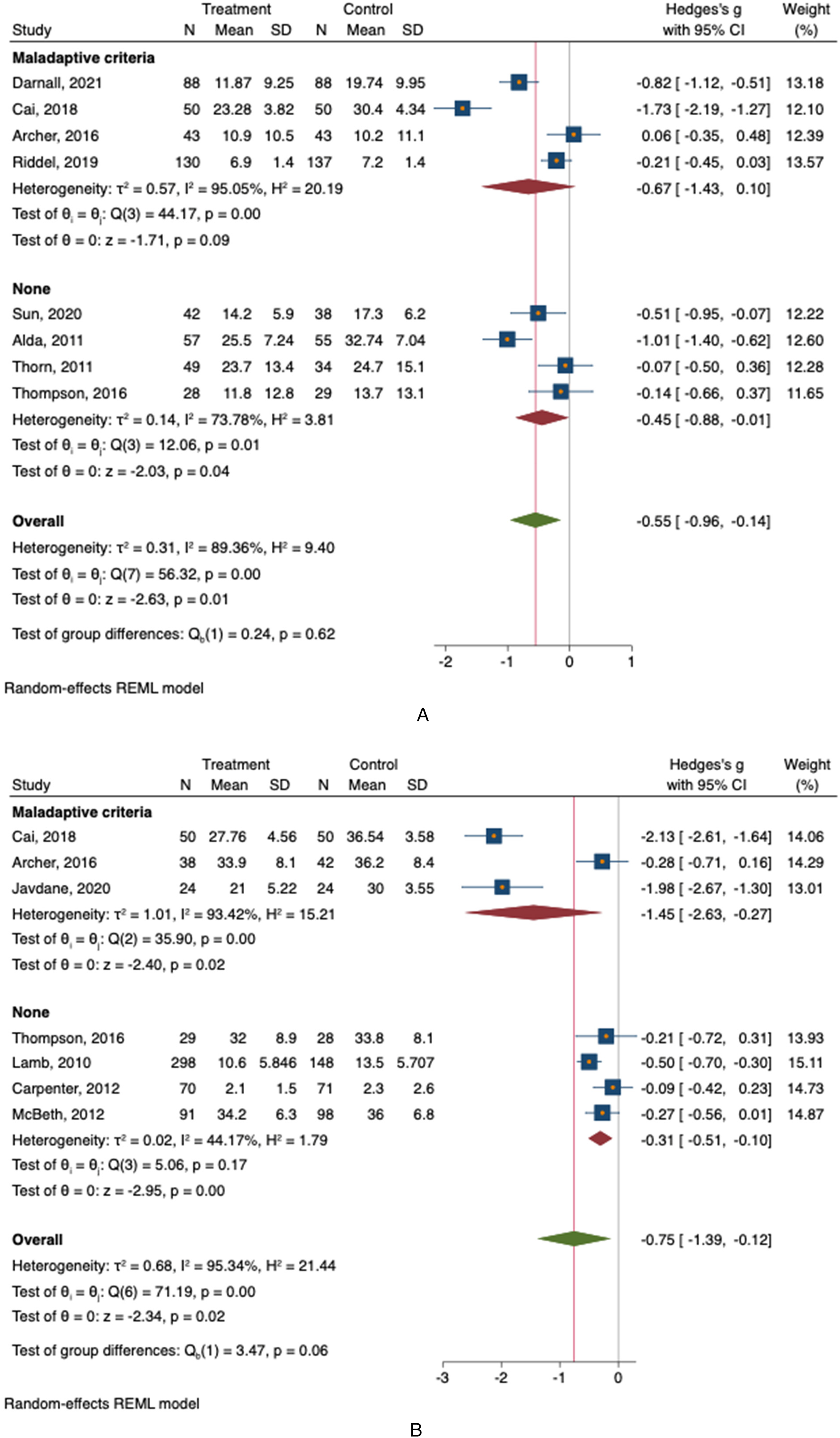
A. This forest plot compares the impact of CBT on catastrophic thinking in populations screened for unhealthy mindsets versus those not screened, each against usual care interventions. B. This forest plot compares the impact of CBT on fear avoidance in populations screened for unhealthy mindsets versus those not screened, each against usual care interventions. C. This forest plot compares the impact of CBT on anxiety related to pain in populations screened for unhealthy mindsets versus those not screened, each against usual care interventions. D. This forest plot compares the impact of CBT on outcomes related to function, including strength, mobility, and activities of daily living, in populations screened for unhealthy mindsets versus those not screened, each against usual care interventions.
Discussion
Background and Rationale
Since unhelpful thinking contributes to increased discomfort and incapability for musculoskeletal conditions, psychological interventions that can reduce catastrophic thinking have the potential to improve health. We reviewed prospective randomized trials comparing a CBT intervention with other interventions among people with musculoskeletal illness and found that 1. CBT is modestly associated with healthier mindsets but not greater capability on average, and 2. CBT is somewhat more effective when delivered by mental health clinicians.
Limitations
This study has a number of limitations. First, we combined data from studies addressing various diagnoses in various settings. Therefore, the findings might vary for specific conditions and settings. Despite the limitations of combining data from studies across various diagnoses and settings, the study's conclusions remain valid. The diverse inclusion enhances generalizability, offering a comprehensive view of CBT's impact on unhelpful thinking in patients with musculoskeletal conditions. Additionally, consistent and significant reductions in pain catastrophizing, kinesiophobia, and anxiety symptoms across various conditions supports the broader efficacy of CBT in fostering healthier mindsets. Second, the limited number of published randomized controlled trials of CBT for musculoskeletal conditions limited the ability to compare CBT across various settings. For instance, only one study evaluated pre-operative CBT and so we were unable to assess whether CBT was more effective pre-operatively or post-operatively and instead focused on comparisons that were significantly powered. By prioritizing these comparisons, we contributed to a more confident assessment of the impact of CBT within the available evidence. Third, the RCTs included in this analysis only investigated knee, spine surgery, ongoing back and neck pain, and daily widespread pain, leaving other areas such as trauma, shoulder, and hip conditions unstudied. Consequently, these findings do not extend to unstudied areas like trauma, shoulder, and hip conditions. However, multiple studies were found for each of our studied conditions. The multiple adequately powered studies within the analyzed conditions contribute to the confidence and reliability of the conclusions in the specified musculoskeletal contexts.
Is CBT Associated with Healthier Mindsets and Greater Comfort and Capability?
The findings that CBT is associated with modest reductions in catastrophic thinking, kinesiophobia, and symptoms anxiety, but these reductions in unhelpful thinking were not associated with greater comfort or capability or ability to complete activities of daily living such as bathing and doing chores around the home is consistent with previous individual studies and limited reviews.5,14 One potential explanation is that inclusion of people with both healthy and unhealthy mindsets in the studies may have limited an observed benefit of CBT. Looking more closely, the effect sizes were quite large for some of the studies which studied patients with a high baseline of unhelpful thinking. Considering the meta-results were only barely non-significant (P value of .06), the authors could not responsibly rule out that CBT may be more effective in patients with high levels of unhelpful thinking. A next step could be to evaluate whether CBT reduces unhelpful thinking significantly more in patients with notable levels of unhelpful thinking and whether this reduction translates to improved capability as observed in a recent randomized trial of people recovering from musculoskeletal injury. 37
Are There Differences Based on how CBT is Delivered?
The finding that CBT sessions led by mental health providers reduced catastrophic thinking and kinesiophobia more than sessions led by physical therapists might relate to the method of training physical therapists to deliver CBT, or it might relate to other factors such as openness to working with a mental health professional, which might enhance measured effectiveness. Patients tend to be relatively more open to referral to physical therapist than to a psychologist due to mental health stigma, so further development of psychologically informed physical therapy is worthwhile. 38
The findings that group CBT was as effective as one-on-one CBT and that online sessions were as effective as in-person sessions support flexibility in treatment strategies that can enhance accessibility. 39 The finding that earlier initiation of CBT was more effective supports anticipating difficult recoveries and strategizing comprehensive care rather than using CBT to salvage problematic recoveries when they are established.
Conclusions
The collective evidence from randomized trials of CBT in musculoskeletal illness, documents modest reduction in unhelpful thinking, more so in people experiencing notable unhelpful thinking. Unhelpful thinking can be measured using instruments such as the Pain Catastrophizing Scale, the Tampa Scale of Kinesiophobia, and the Negative Pain Thoughts Questionnaire and notable levels could prompt a discussion of referral for CBT. Given that mental health stigma can hinder patient appeal for addressing mindsets, another approach could be to train physical therapists to deliver CBT-based mindset exercises incorporated with physical exercises and tailor the approach to the specific patient and their level of unhelpful thinking. In any case, more research is needed to determine how to use mindset training such as CBT to help people feel better and do more by guiding them to the healthiest possible inner narrative regarding their body's sensations.
Supplemental Material
sj-docx-1-css-10.1177_24705470241304252 - Supplemental material for Cognitive Behavioral Therapy Reduces Unhelpful Thinking Among People with Musculoskeletal Symptoms: A Meta-Analysis
Supplemental material, sj-docx-1-css-10.1177_24705470241304252 for Cognitive Behavioral Therapy Reduces Unhelpful Thinking Among People with Musculoskeletal Symptoms: A Meta-Analysis by Deven Niraj Patel, Rajeev Pathapati, Catherine Hand, Ashwin Varma, Sina Ramtin and David Ring in Chronic Stress
Footnotes
Author Contributions
Deven Patel: Conceptualization, literature review, data collection, and writing
Rajeev Pathapati: literature review, methodology, data collection, and writing
Catherine Hand: Data curation and statistical analysis.
Ashwin Varma: Data curation and statistical analysis
Sina Ramtin: supervision of statistical analysis
David Ring: Supervision, project administration, and writing—review and editing.
All authors have approved the final version of the manuscript and agree to be accountable for all aspects of the work.
Declaration of Conflicting Interests
Please separate ICMJE forms attached for each author details on conflicting interests.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.