
Abstract
Background
Discrimination is a pervasive societal issue that monumentally impacts people of color (POC). Many Black, Asian, and Hispanic/Latinx individuals report experiencing race-based discrimination in their lifetime. Discrimination has previously been linked to adverse health outcomes among POC, including stress, depressive, and posttraumatic stress disorder symptoms. These health disparities are posited to have become exacerbated by COVID-19 and the racial awakening of 2020. The current study examined the short- and long-term effects of discrimination on stress, depression, and oppression-based trauma among POC.
Methods
Participants were (n = 398) who identified as Black, Indigenous, Hispanic/Latinx, and Asian completed an online self-report survey assessing discrimination, depression, stress, and oppression-based trauma collected at 3 time points: (T1) beginning of the COVID-19 pandemic (May 2020), (T2) 6 weeks later during the racial awakening of 2020 (June 2020), (T3) one year later (June 2021).
Results
Significant positive paths were revealed from T1 discrimination to T2 depression, T2 stress, and T3 oppression-based trauma. The association between T1 discrimination and T3 oppression-based trauma was partially mediated by T2 depression, but not by stress; total and total indirect effects remained significant. The final model accounted for a significant proportion of the variance in T3 oppression-based trauma, T2 depression, and T2 stress.
Conclusion
Findings are consistent with prior research linking discriminatory experiences with mental health symptomatology and provide evidence that race-based discrimination poses harmful short-and long-term mental health consequences. Further research is necessary to better understand oppression-based trauma to improve the accuracy of clinical diagnosis and treatment of POC.
Introduction
Discrimination
Although discrimination can occur across various facets of identity (e.g., age, gender, race/ethnicity, sexual orientation, national origin), people of color (POC) face unique burdens, especially those who sit at the intersection of multiple marginalized identities.1,2 Recent research shows that about three-quarters of Black and Asian individuals and nearly 60% of Hispanics/Latinx individuals have experienced discrimination. 3 Research also demonstrates that POC experience interpersonal racism in wide and varied ways (i.e., microaggressions at schools and work4,5). POC are continuously subjected to ongoing negative stereotyping, the consequences of which include demeaning treatment, opportunity loss, and even death.6,7
Scholars and activists regularly point out the ways in which racism is embedded within our societal institutions across criminal justice, education, housing, and healthcare systems.8,9 Indeed, Black people are 3.5 times more likely to die at the hands of police than their White counterparts, 10 many White health professionals believe Black individuals have a higher pain tolerance than White patients, 11 and Black women experience significantly higher maternal morbidity rates than White women. 12 Experiences of discrimination have compounding effects on POC, leading to chronic stress, adverse health outcomes, and trauma symptoms. These effects have intensified since the onset of COVID-19 and the racial awakening of 2020, disproportionately impacting the health of POC, and thereby increasing the need to investigate the impact of these constructs. The present study sought to investigate the impact of discriminatory experiences during COVID-19 and the racial awakening of 2020 on perceived stress, depression, and trauma symptoms.
Perceived Stress
Stress is known to affect biological and psychological processes that play a role in coping. Exposure to acute stressors triggers neuroendocrine responses that extend over time, 13 can impact emotion regulation, and increase the likelihood of engaging in avoidance behaviors. 14 Past research indicates stressful events involving explicit racism evoke large cortisol responses among POC.15–17 Furthermore, exposure to various stressors elicits repeated activation of physiological stress responses, which are found to negatively impact health outcomes.18,19 This has significantly impacted health outcomes among Black Americans who experience prolonged cumulative stress from social and economic inequity, contributing to a disproportionately high prevalence of chronic diseases.18,19 Thus, it is posited that the experience of discrimination and social exclusion elicits strong stress responses among POC, leading to deleterious health effects. 20 This is supported by various meta-analyses, which have found a large effect of stress appraisal on health outcomes as a result of discrimination.21,22
Depression and Other Health-Related Outcomes
Discrimination is a significant determinant of health disparities among POC, as it perpetuates health inequalities, impacting life expectancy, access to health services, and prevalence of chronic diseases.20,21,23 Racial discrimination has negatively impacted well-being, psychological health, leading to increases in anxiety and depressive symptoms.24–28 One meta-analysis found that increased exposure to racism leads to increased reports of mental distress among Black Americans. 25 Among Asian and Hispanic/Latinx groups, discrimination has been strongly correlated with depression and anxiety, poorer overall health, and psychological distress.26,27
Interpersonal racism is a significant risk factor for depression across the life span among POC. 29 Among Black Americans, discrimination has predicted stress and depressive symptoms through heightened vigilance. 30 Additionally, repeated exposure to discrimination-related stressors is posited to contribute to negative schemas about oneself, the world, and others, triggering the onset and maintenance of depressive symptoms.31,32 This is salient since depression is considered one of the leading causes of disability across the world, with even subclinical symptoms negatively impacting physical health, quality of life, and mental health.33–36 It is also important to note that discrimination impacts help-seeking behaviors, including mistrust of the healthcare system. This has been found to be especially prevalent since COVID-19 among POC, thereby generating exceptional vulnerabilities to negative health outcomes.21,23
Oppression-Based Trauma
Experiences of discrimination can contribute to the development of trauma symptoms among POC. 37 Various theoretical models posit that racism can trigger stress reactions similar to posttraumatic stress disorder (PTSD) symptoms, leading many researchers to suggest a new classification of PTSD.38–40 This is particularly salient among POC, who are found to be more susceptible to PTSD symptoms stemming from experiences of racism and oppression, a phenomenon known as oppression-based trauma.41,42 Racial violence and police brutality against POC are examples of events that can result in oppression-based trauma, with continued coverage and public action surrounding these events increasing the likelihood of vicarious individual and collective oppression-based trauma.43–46
A recent systematic review found strong positive associations between discrimination and a range of PTSD measures. 2 Longitudinal evidence suggests that discrimination uniquely predicts PTSD outcomes, particularly among Black and Hispanic/Latinx Americans relative to White Americans. 47 Additionally, experiences of discrimination are posited to be a stronger predictor of trauma symptoms than other stressful experiences. 48 Although not all experiences of discrimination will lead to trauma symptoms, experiencing certain vulnerabilities (e.g., microaggressions, multiple traumas, multiple stigmatized identities), is posited to reshape one's perceptions, leading to low self-esteem and self-efficacy, psychological distress, depression, suicidal ideations, and higher mortality rates.49–54 Thus, following a triggering discriminatory experience, the perception of the event as a personal threat, coupled with invalidating experiences, exacerbates the onset of trauma symptoms. 44 Thus, the debilitating health outcomes stemming from racism are important to consider in the context of the social climate in the United States, particularly at the onset of the COVID-19 pandemic and the racial awakening of 2020.
COVID-19 Pandemic and Racial Awakening
The COVID-19 pandemic had significant impacts on the lives of people worldwide. In the United States, the difficulties experienced had an even more acute impact on POC, exacerbating systemic health and social inequalities. Black, Hispanic/Latinx, Indigenous, and Pacific Islanders are disproportionately infected with, hospitalized for, and have died from COVID-19.55–57 Not only did COVID-19 expose disparate outcomes for POC but it also resulted in significant increases in discrimination and violence against Asian people. 58 As such, COVID-19 represents a significant source of race-related stress for POC.
At the same time as the pandemic was unfolding, social unrest exploded across the United States in response to the murder of George Floyd, which happened only months after the shooting deaths of Ahmaud Arbery and Breonna Taylor. These high-profile cases of unarmed Black Americans killed by police and White violence ignited protests and outrage around the United States and world. 59 Police violence against Black Americans dates back to the creation of police units from slave patrols 60 and represents a significant source of race-related stress for not only Black people but other minoritized groups as well. Overall, Black, Hispanic/Latinx, and Indigenous Americans are more likely than their White peers to experience both lethal and nonlethal violence by police.61,62 The social unrest in response to the murder of George Floyd ignited what some call a “racial awakening.” 63 However, while Floyd's murder resulted in unprecedented levels of anger and sadness among Americans, the impact was greater for Black people and other POC who faced greater increases in anxiety, depression, and psychological distress. 64 These findings point to a significant public health issue, warranting further investigation in order to comprehensively understand the impact of both the COVID-19 pandemic and the racial awakening of 2020 on health outcomes, including depression, stress, and trauma symptoms, among POC.
Study Overview
The current study used a longitudinal design to examine the effect of discrimination on perceived stress, depression, and oppression-based trauma symptoms among POC during the COVID-19 pandemic and the racial awakening of 2020. Thus, this study examined the link between discrimination at Time 1 (T1; onset of COVID pandemic May 2022) and oppression-based trauma at Time 3 (T3; one year later) via changes in perceived stress and depression at Time 2 (T2; onset of racial awakening). It was hypothesized that discrimination at T1 would be associated with changes in depression and perceived stress at T2. Research has clearly linked discrimination to the development and exacerbation of mental health including depression and stress. Given that prior research has shown that race-related mental health issues are linked to the onset of future oppression-based trauma, it was further hypothesized that those changes would mediate the links between discrimination at T1 and oppression-based trauma at T3.
Methods
Participants
Participants were (n = 398) a subsample from a larger study (N = 963) focused on discrimination and health experiences during the COVID-19 pandemic. 23 Participants were included in the current study analyses if they completed both a baseline and follow-up survey one year later and indicated that they were a POC. Race/ethnicity of participants in the final analytic sample is as follows: 37.44% (n = 149) Black-not Hispanic/Latinx, 10.05% (n = 40) Black-Hispanic/Latinx, 32.16% (n = 128) Asian-not-Hispanic/Latinx, 13.07% (n = 52) White Hispanic/Latinx, and 7.29% (n = 29) American Indian or Alaska Native-not-Hispanic/Latinx. Participants’ age ranged from 18 to 73 years (M = 35.42, SD = 11.39), 53.5% (n = 213) endorsed being a cisgender female, 42.1% (n = 167) endorsed being a male (6 transgender, 380 cisgender), and 2.8% (n = 11) identified as genderqueer, genderfluid, or another gender identity not listed. The majority of participants indicated they were heterosexual (82.6%; n = 328).
Procedures
Data collection took place at 3 timepoints via an online self-report survey. First, Time 1 (T1) data were collected during the first 2 weeks of May 2020, when most states enacted COVID-19 stay-at-home orders and other government mandates. Time 2 (T2) data were collected approximately 6 weeks later, soon after the killing of George Floyd and widespread Black Lives Matters protests. Time 3 (T3) data were collected approximately one year later in summer 2021. To be included in the analytic sample for the current study, participants must have completed both the T1 and T3 surveys; the majority of the participants also completed the T2 survey a . All participants who completed the T1 survey were eligible to participate in T2 and T3; completing the T2 survey was not required for T3 eligibility.
Participants were recruited from the CloudResearch MTurk Toolkit, which integrates pro features to block low quality and “bot-like” responses automatically (e.g., duplicate IP addresses) and ensures recruitment from a vetted group of individuals who pass system attention checks to enhance data quality. Individuals were eligible if they were 18 years of age or older and lived in the United States. Individuals were directed to the survey on Qualtrics and were provided with an IRB-approved consent form. Participants who consented to participate proceeded with the T1 survey. Participants who completed the T1 survey were invited to participate in the T2 and T3 surveys directly through the CloudResearch system without the collection of any identifying information, each of which included a new informed consent process.
Measures
Demographics
Participants self-reported their race and ethnicity, age, gender identity, sexual orientation, relationship status, length of time living in the United States, citizenship, annual household income, and level of education.
Discrimination (T1)
Participants’ experiences of discrimination were assessed using the Everyday Discrimination Scale (Williams et al, 1997), which assesses the frequency of 9 common experiences of discrimination (e.g., threatened or harassed, treated with less respect than other people) on a scale ranging from 1 = never to 6 = almost every day. Scores across the 9 items were averaged, such that higher scores indicated a greater frequency of discrimination (α = .95). For participants who reported any discrimination, a tenth item assessed their primary attribution for their experiences. Participants could choose from various categories, such as “ancestry or national origin” or “race.”
Depression Symptoms (T1 and T2)
Participants’ depression symptoms were assessed with the Patient Health Questionnaire-9 (Kroenke, Spitzer, & Williams, 2001). Participants reported the frequency of 9 symptoms over the past month on a scale ranging from not at all to nearly every day over the past 2 weeks (T1) or since the previous survey (T2). The 9 items were averaged, such that higher scores indicated the greater frequency of depression symptoms (T1 α = .92; T2 α = .90).
Perceived Stress (T1 and T2)
To assess perceived stress, participants completed the Perceived Stress Scale-4 (PSS-4; Cohen & Williamson, 1988), a validated brief version of the original PSS (Cohen, Kamarck, & Mermelstein, 1983). Participants reported the frequency of each item with response options ranging from 1 (never) to 5 (very often) over the past month (T1) or since the previous survey (T2). Responses were averaged, such that higher scores indicated higher perceived stress. The 6-item version included in the current study demonstrated adequate internal consistency (T1 α = .81; T2 α = .84).
Oppression-Based Trauma (T3)
Trauma resulting from prior discrimination experiences was assessed using the Trauma Symptoms of Discrimination Scale (Williams et al 2018). Participants reported the frequency of 21 trauma symptoms (e.g., “cannot control my emotions,” “feel afraid as if something awful might happen,” “feel constantly on guard, watchful, or easily startled”) caused by discrimination, with response options ranging from 1 (never) to 4 (often). Responses were averaged, such that higher scores indicated more frequent trauma symptoms (α = .97).
Analytic Strategy
The dataset included observations from individuals across 3 waves of data. We restricted the analysis to POC that participated in T1 and in either T2, T3, or both. There was a total of n = 398 participants that had data at T1 as well as T2 and/or T3. Among this sample, n = 166 (42% of total sample) provided data at T1 and T2 but not at T3, n = 69 (17% of total sample) provided data at T1 and T3, but not at T2, and n = 163 (41% of total sample) provided data at all 3 waves. To form the latent variables, observed variables indicators were used for the T1 and T2 stress, 3 parcels were formed using the means of discrimination items at T1, 3 parcels were from the means of the depression indicators at T1 and T2, and 3 parcels were formed from the 21 oppression-based trauma indicators at T3.
We used structural equation modeling to examine distal predictors of oppression-based trauma. First, we specified a measurement model. We examined measurement parameters for method variance to develop an adequate measurement model of the hypothesized constructs. Next, we specified a structural equation model in which discrimination at T1 predicts depression and perceived stress at T2 (6 weeks later) as well as oppression-based trauma at T3 (a year later). We used a Bayesian approach to estimate model parameters. Bayes uses all available data to calculate distributions of model parameters based on available information and is robust to small samples and missing data. 65 All parameters used noninformative priors. The MCMC estimation proceeded in 2 chains, burn-in chain and an estimation chain. Final convergence was determined by potential scale reduction (PSR). Following convergence, trace plots were examined to identify potential issues in the mixing of the MCMC chains. Below we report 95% Bayesian Credibility Intervals (95% BCI) for the posterior distributions. Model fit statistics used traditional indices of fit.
Results
Descriptive
Descriptive statistics are in Table 1; bivariate correlations are in Table 2. Discrimination was significantly correlated with T1 and T2 perceived stress, T1 and T2 depression, and T3 oppression-based trauma. Similarly, T1 and T2 perceived stress were each significantly correlated with T1 and T2 depression and T3 oppression-based trauma. T1 and T2 depression were each significantly correlated with oppression-based trauma. Table 3 displays participants’ discrimination attributions across various domains (e.g., race, sexual orientation, age). Race (n = 138; 42.59%) and ancestry/national origin (n = 50; 15.43%) were the most common types of discrimination experienced.
Descriptive Statistics.

Note. n = 398; T1 = Time 1, onset of COVID = 19 pandemic; T2 = Time 2, 6 weeks later; T3 = Time 3,1 year later.
Bivariate Statistics.

Note. n = 398; T1 = Time 1, onset of COVID = 19 pandemic; T2 = Time 2, 6 weeks later; T3 = Time 3,1 year later. *p < .05; **p < .001.
Attribution of Discrimination.
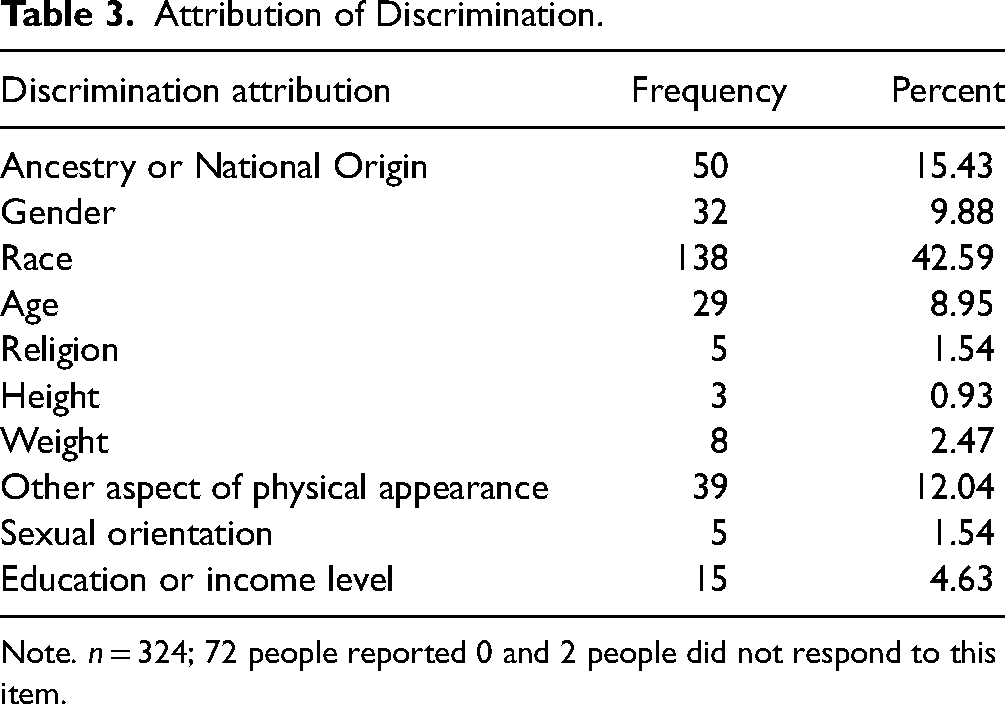
Note. n = 324; 72 people reported 0 and 2 people did not respond to this item.
Primary Analysis
Measurement Model
We first specified a measurement model of the latent constructs. The model showed adequate fit to the data, with 95% CI for the difference between observed and replicated χ2 = 641.55, 750.86, RMSEA = 0.102 (90% CI = 0.101-0.104), CFI = .89, TLI = .87. However, there were robust covariances among each T1 indicator and the same indicator at T2 across the depression and stress latent variables, indicative of common-method variance. These were freed, and the model was reestimated. The revised measurement model showed adequate fit to the data, with 95% CI for the difference between observed and replicated χ2 = 202.48, 321.45, RMSEA = 0.060 (90% CI = 0.057, 0.063), CFI = .96, TLI = .95.
Structural Model
Next, we specified the structural model (see Figure 1). The initial model converged in 4000 chain iterations (2000 burn-in followed by 2000 estimation iterations). We increased the number of iterations by a factor 10 (20 000 burn-in, 20 000 estimation). The final PSR was 1.001, which did not increase in the chain and did not increase above 1.003 in the final 10 000 chains. Kolmogorov-Smirnov statistic, comparing posterior distributions across chains 1 and 2 using 100 draws, was nonsignificant.
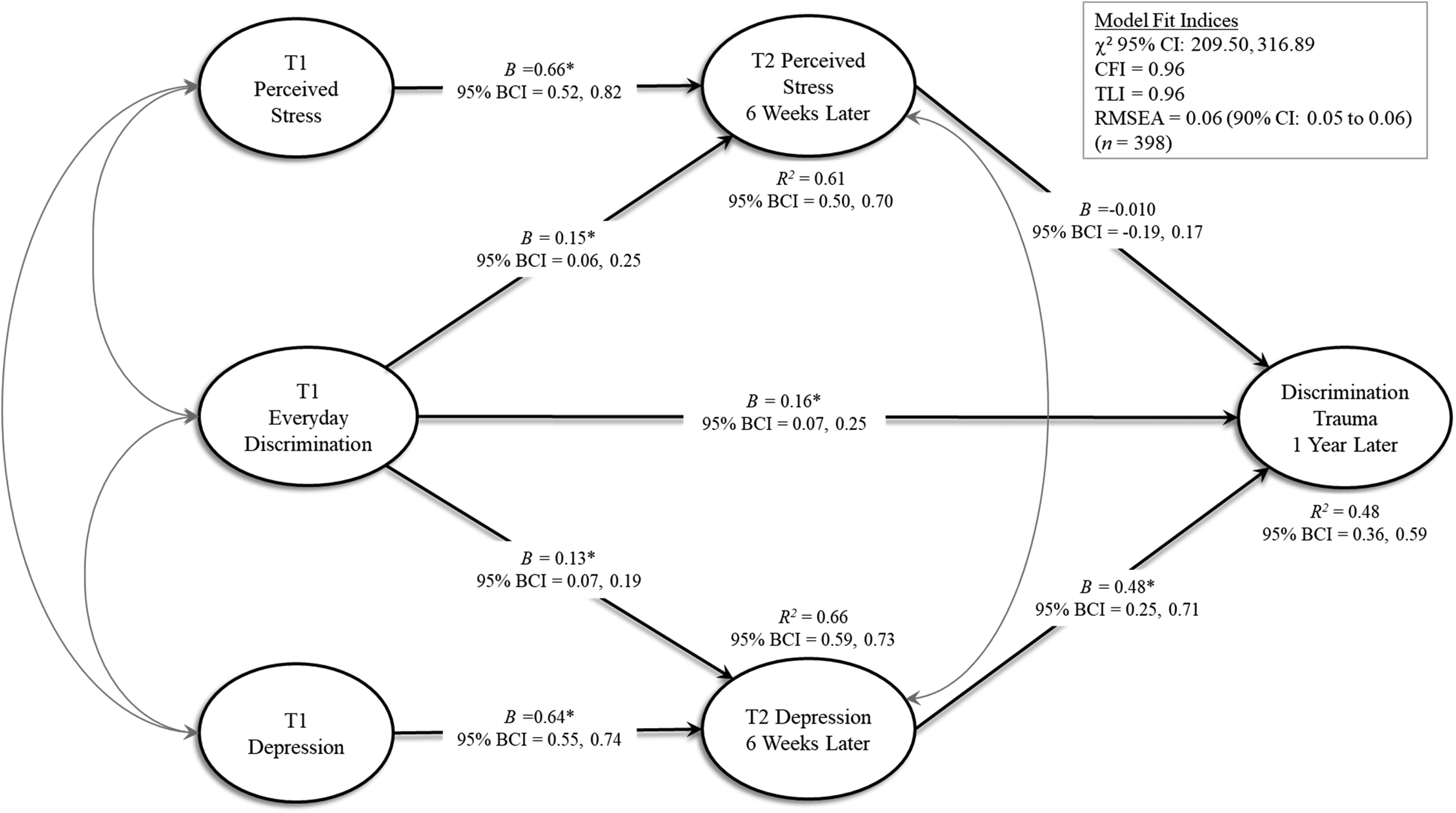
Structural model. Note. T1 = Time 1, onset of COVID = 19 pandemic; T2 = Time 2, 6 weeks later; T3 = Time 3, 1 year later. *P ≤
Oppression-based trauma was specified as the endogenous outcome and was regressed onto the T2 depression and perceived stress mediators and T1 discrimination. T2 depression and perceived stress were both regressed onto T1 discrimination. T2 depression was regressed into T1 depression and T2 perceived stress was regressed onto T1 perceived stress. This model showed excellent fit to the data, with 95% CI for the difference between observed and replicated χ2 = 209.50, 316.89, RMSEA = 0.060 (90% CI = 0.057-0.063), CFI = .96, TLI = .96. There were significant positive paths from discrimination at T1 to both depression and perceived stress at T2 and oppression-based trauma at T3. Perceived stress at T2 did not predict oppression-based trauma at T3; however, depression at T2 did predict T3 oppression-based trauma. The association between discrimination at T1 and oppression-based trauma at T3 was partially mediated by T2 depression (specific indirect effect = 0.060, 95% BCI = 0.025-0.109) but not by T2 perceived stress (specific indirect effect = −0.001, 95% BCI = −0.032, 0.028). Despite the nonsignificant indirect effect through T2 perceived stress, the total indirect effect from T1 discrimination to T3 oppression-based trauma (through both mediators) was still significant (total indirect effect = 0.059, 95% BCI = 0.027-0.100) as was the total (indirect + direct) effect (total effect = 0.218, 95% BCI = 0.135-0.302). The final model accounted for 48% (95% BCI: 36%-59%) of the variance in T3 oppression-based trauma, 66% (95% BCI: 59%-73%) of the variance in T2 depression, and 61% (95% BCI: 50%-70%) of the variance in T2 perceived stress.
Discussion
This study examined the impact of discrimination on depression, stress, and trauma symptoms across time during the COVID-19 pandemic and the racial awakening of 2020 among POC. Consistent with the extant literature, we found support for most hypotheses. Discrimination at T1 predicted both depressive symptoms and perceived stress 6 weeks later. Discrimination also predicted oppression-based trauma one year later. The relationship between discrimination at T1 and oppression-based trauma at T3 was partially mediated by depression at T2, but not by perceived stress. These findings highlight the unique effects of discrimination on key health factors among POC. To our knowledge, this is only one of few studies that have examined the impact of discrimination in the context of COVID-19 and racial awakening.
First, it is important to interpret the finding of discrimination predicting depression and perceived stress 6 weeks later in the social context in which it occurred. This was an unprecedented time where POC was disproportionately dying as a result of systemic and structural racism, both from COVID-19 and violence perpetuated by white supremacy.57,61,64 Thus, it is not surprising that experiences of discrimination predicted both depressive and perceived stress symptoms 6 weeks later among POC. These findings suggest that discrimination may trigger significant stress and depressive symptoms in this population. This is consistent with the extant literature, which has long-established links between discrimination, stress, and depression.21,22,66
Second, discrimination significantly predicted oppression-based trauma a year later. This is consistent with previous findings, as well as the notion that racism is a significant stressor that can lead to the development of trauma symptoms, which is currently not recognized by psychological or psychiatric diagnostic systems.39,67 Furthermore, evidence suggests that POC have a higher prevalence of PTSD that is not explained by the event or other factors. Carter 39 posits these experiences stem from events that occur suddenly, are perceived to be out of one's control, and are emotionally painful, rather than seen as a threat to one's life. As a result, this experience is different from the theoretical model of PTSD37,39,67; further justifying the need for oppression-based traumatic stressors to be properly recognized, assessed, and treated in the field.
Lastly, findings suggest that the combined experience of discrimination and depression elicited oppression-based trauma symptoms a year later. Emotion regulation is posited to play a role, as it is hypothesized that exposure to traumatic discriminatory experiences can lead to disturbances in emotion responses, including dysregulated shame and emotional numbing.39,68 This could lead to the development of initial depressive symptoms, as individuals from POC may experience increased emotional distress that place demands on emotion regulatory systems. Overtime, this can interfere with adaptive emotion regulation and goal-directed behaviors, increasing the risk of developing trauma symptoms. This finding highlights an important mechanism through which discriminatory experiences can exacerbate mental health and lead to trauma symptoms. Future research should continue to investigate the mechanisms through which discriminatory experiences lead to the onset of trauma symptoms in POC, and in particular, how stress plays a role.
Implications
The literature has identified serious impacts of discrimination on various health-related outcomes leading to significant health disparities for POC. The findings of the current study provide evidence regarding the short- and long-term effects of discrimination on POC. Understanding pervasive discrimination and its chronic effects on POC is critical in the diagnosis and treatment of individuals presenting for treatment for oppression-based difficulties. Moreover, continued investigation of the mechanisms through which discrimination leads to oppression-based trauma and the functional similarities between discrimination trauma and PTSD is crucial. This could have a monumental impact, as it could validate traumatic experiences, expand coverage of treatment, and improve diagnosis for POC.
Limitations
These results should be interpreted in the context of the following limitations. First, the sample was recruited only through CloudResearch MTurk Toolkit and therefore may not be representative of the general population of POC, as individuals who are recruited through MTurk tend to be younger and more educated. 69 Thus, it is possible that the studied sample may not fully represent the extent of racial health disparities that were particularly salient at the onset of the COVID-19 pandemic or other populations (eg, non-U.S. born Black individuals). Future studies should utilize a range of recruitment methods to yield a more representative sample. The study was also conducted completely online, and thus, self-selection bias should be considered. Moreover, due to the sample size, we were unable to analyze the findings across racial/ethnic groups. Therefore, the results may not generalize to POC subgroups. Another limitation is the length of time for the final measurement (12 months). There are several unmeasured intervening factors that could have happened during this time that has the potential to influence the final outcome. Lastly, our measurement of perceived stress was short and may not have sufficiently captured all domains of stress in this population, which may explain its nonsignificant effect on oppression-based trauma. Employing a more comprehensive measure of stress in future studies is warranted. Despite these limitations, the current study possesses several strengths, including the racial diversity of the sample and the timing of data collection. Thus, the present study was able to assess these constructs during 2 important time periods that have radically changed the experiences of Americans.
Conclusion
The present study aimed to examine the effects of discrimination on perceived stress, depression, and oppression-based trauma symptoms among POC. As hypothesized, discrimination predicted future perceived stress, depressive symptoms, and oppression-based trauma, with depression mediating the association between discrimination and oppression-based trauma. The present findings highlight a potentially important mechanism involved in the development of trauma symptoms among POC. This represents an important implication for the identification, understanding, and treatment of oppression-based trauma among POC. These advancements may ultimately contribute to the minimization of both mental and physical health disparities among POC that are exacerbated by the effects of discrimination.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health (grant number K23AA028515, R25DA035163, 1R15AA026420).