
Abstract
Background
Distress tolerance is the ability to pursue one’s goals in the presence of (chronic) stressors, hardship, adversities and negative internal states, and psychological distress. By contrast, distress intolerance is a transdiagnostic indicator of mental illness and a mediator in coping with problems in life, work demands, or stress in general. There is a lack of data regarding intervention strategies. The objective of the present study is to test the differential effects of two treatment approaches: “regeneration fostering” versus “resistance training.”
Methods
Inpatients of a psychosomatic hospital were randomly allocated to either a resistance training group therapy (n = 65)—that is, active coping with demands and endurance—or a regeneration fostering group therapy (n = 62)—that is, recovery, mindful indulgence, and creative activities. They were compared with a group of patients who received treatment as usual (n = 43), without special treatments for distress intolerance, and the outcome was measured with the “Distress Intolerance Scale.” One-way and repeated measure analyses of variance and paired t tests were used for the analysis.
Results
The “regeneration” group showed a significant improvement in distress intolerance, whereas there was no significant change for the treatment-as-usual group and in the “resistance” group. Post hoc tests were conducted with paired sample t tests for pre–post comparisons for each group. No differences were found for the treatment-as-usual group (mean difference: 0.03, SD (mean difference): 0.89; t(42) = 0.266, p = 0.792, d = 0.04) and for the resistance group (mean difference:−0.07, SD (mean difference): 0.73; t(63) = −0.736, p = 0.464, d = 0.08). The regeneration group showed a significant decline in distress intolerance (mean difference: 0.29, SD (mean difference): 0.72; t(61) = 3.156, p = 0.002, d = 0.38).
Conclusions
In the treatment of distress intolerance, it seems promising to focus on positive psychology interventions and resources. Limitations of the study are that it was conducted with psychosomatic inpatients only and that no follow-up data are available.
Introduction
Distress tolerance is the ability to pursue one’s goals in the presence of (chronic) stressors, hardship adversities and negative internal states, and psychological distress. 1 Global distress tolerance includes subdimensions such as tolerance of ambiguity, tolerance of uncertainty, frustration tolerance, tolerance of negative emotional states, and discomfort tolerance.2,3
By contrast, distress intolerance is an indicator of psychological malfunctioning, and it is understood as a vulnerability factor in mental disorders.4–9 Persons with a high level of distress intolerance are more likely to use maladaptive regulation and coping strategies such as avoiding, denying, or escaping and a dysfunctional emotion regulation if confronted with stressors. Research has shown that low distress tolerance or higher distress intolerance significantly predicts the greater use of suppression, avoidance, and rumination when a person is confronted with stressors. 10 Persons with a high level of distress intolerance also perceive and evaluate stressors more threatening than persons with a low level of distress intolerance. This leads to the persistence and intensification of feelings to be stressed and negative reactions to stress, such as anxiety or depression. It is correlated with reduced self-efficacy. A moderator between emotion regulation and distress tolerance is attention control. 11
There are two main approaches to improving distress tolerance. One is to train the acceptance of and coping with stressors and hardship, which can be achieved by cognitive-behavioral therapy through cognitive reframing, training of tolerance against hardship, hardiness, emotional control, coping behavior, active engagement, commitment, frustration tolerance, or endurance.12–17 This treatment can be understood as training distress tolerance directly. McHugh et al. 13 demonstrated a significant decline of distress intolerance in patients from a day care hospital who were treated with multidimensional cognitive therapy, including group therapies with a skill group, behavior activation, cognitive techniques, and stress management and mindfulness training, and an average treatment duration of eight days. There was significant decline over time (main effect) with a partial η2 = 0.17, which means a medium effect size.
Another treatment approach to improve distress tolerance follows theories of positive psychology and salutogenesis, which means concentrating on enhancing health and well-being instead of reducing ill-being. 18 Interventions include fostering self-care, well-being, a sense of coherence and purpose in life, environmental mastery, personal growth, autonomy, self-acceptance, positive relations with others, distraction and distancing from stressors, an increase in recreational and personal meaningful activities, mindfulness, induction of positive emotions, or regeneration and strength.18–24 The theoretical concept is that dealing with the emotional reaction as a consequence of stress is more promising because many stressors cannot be changed. This approach tries to improve distress tolerance indirectly. Medina et al. 25 showed the benefit of yoga training on distress tolerance in comparison with a waiting list control. Similarly, mindfulness-based interventions have also shown promising results.26–28 The focus of these interventions is the emotional response of the individual to stressors.
These two approaches correspond to the distinction between “problem focused” and “emotion focused” stress coping as described by Lazarus and Folkman. 29 To our knowledge, there are no controlled clinical trials comparing the effects of both approaches regarding distress intolerance.
Against this background, we designed two different treatments to improve distress intolerance: resistance training, which can be assigned to “problem focused” strategies, and regeneration fostering, which can be assigned to “emotion focused” strategies. The objective of the present study was to test the effects of both approaches on distress intolerance in comparison with each other as well as with a treatment-as-usual (TAU). The research questions are as follows:
What effect does a general psychosomatic inpatient treatment have on distress intolerance? Can resistance group (ResG) and regeneration group (RegG) be realized and discriminated from each other? (Is it possible to implement these different groups in a clinical setting and do patients perceive these different contents?) Do resistance training, regeneration fostering, and TAU have different effects on distress intolerance?
Experimental Section
Setting and Patients
Patients were recruited in a department of psychosomatic medicine. The patients suffer from all types of mental disorders and are admitted by health or pension insurance when their ability to work is threatened or they have occupational problems (such as bullying or deficits in work-related performance). All participants were treated as inpatients on average for five weeks, including individual and group psychotherapy, medication, social therapy, sport therapy, and occupational therapy.
Patients were asked after admission to attend the inpatient unit to take part in an additional “stress-coping” group. After giving their written informed consent, the patients were randomly allocated to two treatment groups, that is, resistance training and regeneration fostering. Randomization was done according to even/uneven administrative ID numbers, which are given to patients before admission to the hospital and which are not related to patient characteristics. Further patients were recruited during the last week of the treatment. These patients gave their written informed consent for data usage and served as the TAU group. The study protocol was approved by the internal review board and data protection department of the Federal German Pension Agency.
Therapeutic Interventions
The group treatment comprised 15 sessions with 90-min duration. The focus of the ResG was the training of frustration tolerance, stamina, endurance, accuracy, flexibility, and discomfort tolerance. Patients were told that they should learn to cope with adversities and strains in the group setting and that hardiness and endurance are important resilience factors that can be learned in the micro context of the group session and transferred to everyday life. Using techniques such as handicraft work, origami, or soap stones, patients were given difficult tasks with no simple solution and high demands. They were put under time pressure and evaluated by therapists and other patients. The therapists also focused on mistakes and motivated the patients to think about alternatives. Furthermore, learning from others was an important part. Similar to the principles of exposure treatment, 30 the patients were supported to experience and stand negative arousal. The overall therapeutic behavior was supportive in the sense that the patients were motivated to proceed with tasks despite negative feelings such as exhaustion, arousal, or frustration.
Content of resistance and regeneration treatment.

Measurements
Distress intolerance was measured with the distress intolerance scale. 31 The participants were told to think about stressful times and recount their reactions. Examples of items are “It scares me when I am nervous” and “I can’t stand situations where I might feel upset.” The answers were given on a five-point Likert-type scale, ranging from 1 (“strongly disagree”) to 5 (“strongly agree”). An average score could be calculated, ranging from 1 to 5. In our study, Cronbach’s α was 0.87 in the first and 0.92 in the second assessment. Social and clinical data were taken from the routine assessments of the hospital. 32
The protocol adherence of treatments was measured in reference to the behavior therapy competency checklist for resistance and regeneration training (BTCC-RR). 33 For each group, 10 items describe pivotal interventions, for example, in the RegG, “I was able to have moments of indulgence” or in the ResG, “I was able to train my frustration tolerance.” After the last group session and at the end of their stay, the patients were asked to offer a rating on a seven-point Likert-type scale from 1 (“not at all”) to 7 (“completely”), whereby an average score was calculated. Cronbach’s α was 0.90 for the regeneration scale and 0.93 for the resistance scale.
Results
Patients
Over a period of 11 months, 876 patients were asked to participate in an additional group to improve coping with stress; 194 (22.14%) agreed to participate, of whom 10 (5.15%) dropped out before the first session. There was no significant difference in pretreatment distress intolerance between the collaborating and not-interested patients (t866 = 1.62, p = 0.11). Based on their internal ID (even numbers: RegG and odd numbers: ResG), the participants were then assigned to the RegG (N = 83) or the ResG (N = 101). During the course of the treatment, 18 (21.7%) patients from the RegG and 33 (32.7%) from the ResG dropped out, leaving 65 persons to complete the RegG and 68 the ResG. There were no significant differences with respect to the distress intolerance between the dropouts and completers (ResG t(100) = −1.15, p = 0.25; RegG t(82) = −0.49, p = 0.62). Additionally, 43 persons were recruited for the TAU group. Due to missing data, six cases had to be excluded from further analysis. The final sample comprised 62 patients in the RegG, 65 in the ResG, and 43 in the TAU group (total N = 170).
The clinical diagnoses of the 170 patients were mood disorders (ICD-10 F3) in 47.6% of cases; neurotic, stress-related, and somatoform disorders (ICD-10 F4) in 26.6%; personality and developmental disorders (ICD-10 F6, F8, and F9) in 14.0%; organic mental disorders (ICD-10 F0) in 4.9%; eating or sleep disorders (ICD-10 F5) in 4.2%; substance abuse disorders (ICD-10 F1) in 1.4%; and schizophrenic disorders (ICD-10 F2) in 1.4% of cases. Due to the small numbers per cell, baseline group differences in the frequencies of ICD diagnoses could only be tested for mood disorders (p = 0.061, χ2(2) = 5.592); neurotic, stress-related, and somatoform disorders (p = 0.095, χ2(2) = 4.701); eating or sleep disorders (p = 0.737, χ2(2) = 0.611); personality disorders (p = 0.280, χ2(2) = 2.546); and developmental disorders (p = 0.636, χ2(2) = 5.592), whereby there were no significant differences.
There were no statistically significant differences between the groups regarding mean age in years (RegG: 50.77, SD: 8.70; ResG: 49.45, SD: 8.74; TAU: 50.91, SD: 8.85; p = 0.606, F(2,166) = 0.502), gender (RegG: 53% females, ResG: 64%, TAU: 53%; p = 0.145, χ2(2) = 3.859), and mean baseline distress intolerance levels (RegG: 3.45, SD: 0.69; ResG: 3.45, SD: 0.80; TAU: 3.47, SD: 0.88; p = 0.989, F(2,166) = 0.011).
Protocol Adherence
Measures of protocol adherence and distress intolerance.
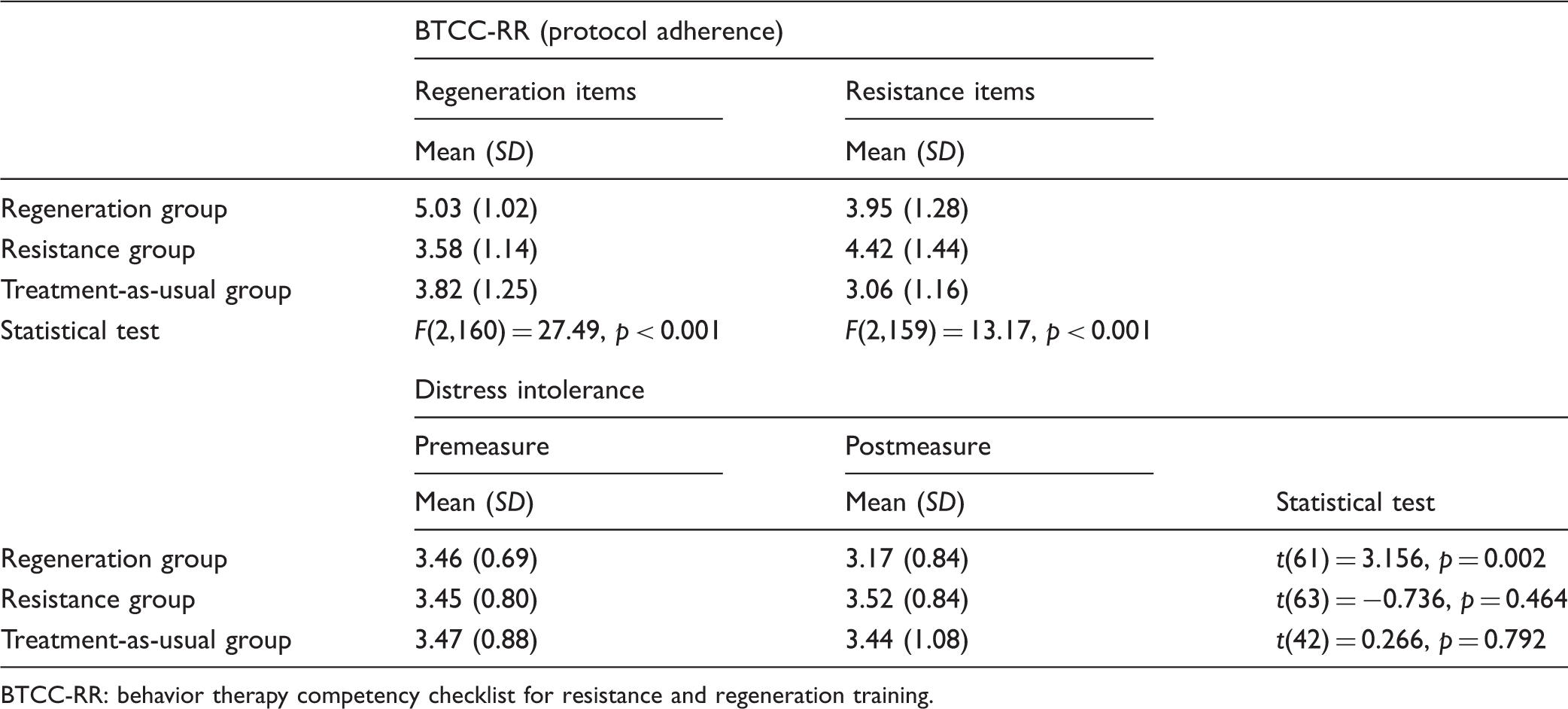
BTCC-RR: behavior therapy competency checklist for resistance and regeneration training.
Distress Intolerance
In order to test for differences in distress intolerance, we calculated a repeated measure analysis of variance (ANOVA) with the three groups as between-subject factor time (pre- and postintervention), as within-subject factor, and distress intolerance as the dependent variable.
34
The p value was 0.05, one tailed, due to the expectation of a decline in distress intolerance because of the treatment. There was no significant main effect of the group (F(2,166) = 0.90, p = 0.48, partial η2 = 0.011) and no significant main effect over time (F(2,166) = 2.04, p = 0.15, partial η2 = 0.012). There was a significant interaction between group and time (F(2,166) = 3.53, p = 0.03, partial η2 = 0.041) with a small effect size.
35
Figure 1 gives an overview.
Means of the distress intolerance scale (y-axis) for groups, pre- and posttreatment (x-axis). Means and standard error of the mean error bars of the Distress Intolerance Scale for every group, pre- and posttreatment. In the paired sample t test, the following results were found: TAU group: mean difference: 0.03, SD (mean difference): 0.89; t(42) = 0.266, p = 0.792, d = 0.04), and for the resistance group (mean difference: −0.07, SD (mean difference): 0.73, t(63) = −0.736, p = 0.464, d = 0.08). The regeneration group showed a significant decline in distress intolerance (mean difference: 0.29, SD (mean difference): 0.72; t(61) = 3.156, p = 0.002, d = 0.38).
In order to test the relative effects of both interventions, a repeated measure ANOVA with the two intervention groups only was calculated. There was no significant main effect of the group (F(1,124) = 1.86, p = 0.176, partial η2 = 0.015) and no significant main effect over time (F(1,124) = 2.965, p = 0.088, partial η2 = 0.023) with an α ≤ 0.05, but a marginally significant result for α ≤ 0.10. There was a significant interaction between group and time (F(1,124) = 7.611, p = 0.007, partial η2 = 0.058).
Post hoc tests were conducted with paired sample t tests for pre–post comparisons for each group. No differences were found for the TAU group (mean difference: 0.03, SD (mean difference): 0.89; t(42) = 0.266, p = 0.792, d = 0.04), and for the ResG (mean difference: −0.07, SD (mean difference): 0.73; t(63) = −0.736, p = 0.464, d = 0.08). The RegG showed a significant decline in distress intolerance (mean difference: 0.29, SD (mean difference): 0.72; t(61) = 3.156, p = 0.002, d = 0.38).
Discussion
The data on protocol adherence show that different interventions were applied in the two intervention groups. As the ratings were provided by the patients, they reflect what happened in the treatment and not only what therapists might have intended to do. This is important for the interpretation of the study results, as differences in outcomes can be attributed to different treatments. It also holds interest for clinical practice at large, as it demonstrates that the group treatment can be targeted and apply specific interventions, in contrast to general and unspecific treatment modes.
One could have expected that five weeks of inpatient treatment would improve distress tolerance, given that the patients were away from daily demands and hassles. They were in a therapeutic program, including individual and group behavior therapy, occupational therapy, and so on. The conclusion is that general psychotherapeutic interventions focusing on the treatment of anxiety, depression, or ability to work do not necessarily change distress intolerance. This was in contrast to McHugh et al. 13 who found an improvement of distress intolerance. Maybe the German rehabilitation setting also had an effect of the outcome, especially in the TAU group: a lot of patients have serious problems in the working life, so the direct aim of the treatment is a reintegration in the labor market and enhance workability or a decision if they are able to receive an invalidity allowance.
Furthermore, resistance training also did not improve but rather deteriorated distress intolerance. Training to withstand hardship, tolerate frustration, and cope with difficulties should have improved distress intolerance. This was not the case. By contrast, the RegG resulted in an improved distress tolerance.
Because many stressors cannot be changed in a direct problem-focused way, the increase in positive feelings can have a compensatory effect and thus contribute to a better distress tolerance and more adaptive way of coping, although with a small effect size. Dalebroux et al. 24 showed that focusing on positive emotions can lead to an improvement of well-being in general. This is in line with the results of Bardeen et al., 11 demonstrating that attention control is an important moderator in the connection between emotion regulation and distress tolerance. 36 This is comparable to what was done in the RegG, as the participants learned to focus on positive experiences and concentrate on positive emotions by fostering meaningfulness and a sense of coherence, supported by positive and meaningful activities and thinking about goals in daily life and the future.
An explanation for the fact that resistance training did not have positive effects could be that a sensitization process was induced. It may be the case that patients in psychosomatic inpatient treatment are in a vulnerable state of mind and overtaxed by hardiness training. Another explanation could be “distress overtolerance,” 37 which describes that some individuals tolerate distress in a manner that does not comply with their interests, leading to an inverse U-shaped relationship between distress tolerance and adaptive behavior. Such patients can have the feeling that they tolerated distress, but that it is now sufficient.
The treatment effects are significant but moderate in size. Nonetheless, they are clinically relevant as they come from the group treatment, which is embedded in a comprehensive inpatient treatment, including individual and group psychotherapy, somatic and medication treatment, social support, occupational therapy, and sport therapy. The results support research findings advocating the importance of specific interventions in psychotherapy. 38
Limitations of the study are that it was conducted with psychosomatic inpatients, who were treated in a rehabilitation setting with patients who have problems in their working life, and where one treatment goal is the enhancement of the ability to work. The response to resistance training and regeneration fostering may also be different among other, non-clinical populations, who may not need as much recovery and can stand more hardiness training.11,15 It would also hold interest to explore whether the interventions have different effects on different diagnosis groups. In our study, there were mixed diagnoses with predominantly depression and anxiety disorders. The duration of the study was limited to a maximum of five weeks, whereas longer treatments might have different outcomes. Moreover, the results refer to changes immediately after the treatment, while it might be the case that the further development after discharge from the hospital may be different. Furthermore, there was a comparatively high dropout rate, although we have no information on the reasons. This also did not allow intent-to-treat analyses due to strict data regulations. Additionally, studies with broader data would allow studying covariates of distress intolerance. Another limitation arises from the fact that distress intolerance was measured by self-report only, whereas there is empirical evidence that self-report and observation measure different phenomena.39,40
To our knowledge, this is the first study that compares the effects of regeneration therapy and resistance training on distress intolerance in a randomized controlled clinical trial. The data show that therapists can apply different treatments according to treatment manuals and that this results in different outcomes. As distress intolerance does not improve through general therapeutic interventions, specific treatments are necessary to achieve specific results.
Supplemental Material
Supplementary Material - Supplemental material for Reduction of Distress Intolerance With Salutotherapeutic Interventions: Results From a Randomized Controlled Clinical Trial
Supplemental material, Supplementary Material for Reduction of Distress Intolerance With Salutotherapeutic Interventions: Results From a Randomized Controlled Clinical Trial by Josephine Otto and Michael Linden in Chronic Stress
Footnotes
Acknowledgment
The language of the manuscript has been revised by Kelly proofreading services without changes of content.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research project was funded by the German Federal Pension Fund (DRV Bund, 8011–106–31/31.51.9).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.