
Abstract
Objective
To overview the phenomenology, etiology, assessment, and treatment of psychotic-like symptoms in trauma-related disorders focusing on the proposed role of temporal lobe dysfunction.
Method
We describe the literature pertaining to (i) psychotic-like symptoms and temporal lobe dysfunction in trauma-related disorders and (ii) psychological testing profiles in trauma-related disorders. We define trauma-related disorders as borderline personality disorder, post-traumatic stress disorder, and the dissociative disorders. Our search terms were dissociative disorders, temporal lobe, trauma, post-traumatic stress disorder, borderline personality disorder, psychosis, and malingering.
Results
Trauma-related psychotic-like symptoms are common and can differ in phenomenology from primary psychotic symptoms. Hallucinations consist of auditory and nonauditory content that may or may not relate to traumatic content. Child voices are highly suggestive of complex dissociative disorders. Critically, not only do these symptoms resemble those seen in temporal lobe epilepsy, but the temporal lobe is implicated in trauma-related disorders, thus providing a plausible neurobiological explanation. Despite such evidence, these symptoms are frequently considered atypical and misdiagnosed. Indeed, common structured psychological assessment tools categorize these symptoms as possible indicators of invalid testing profiles.
Conclusion
Psychotic-like symptoms are common in trauma-related disorders, may be related to temporal lobe dysfunction, and are frequently misinterpreted. This may lead to ineffective treatment and inappropriate determinations of malingering in the forensic system.
Introduction
Dissociation is defined by the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) as a “discontinuity in the normal integration of consciousness, memory, identity, emotions, perception, body representation, motor control, and behavior”. 1 Dissociative symptoms include trance-like states, out-of-body experiences (depersonalization), and a sense of unreality (derealization). Complex dissociative disorders fall at the more severe end of this spectrum and include dissociative identity disorder (DID), which is characterized by marked identity alteration (e.g., experiences of multiple personalities and dissociated self-states) and amnesia, and DID-like presentations of other specified dissociative disorder (OSDD) (previously known as DDNOS). Critically, these disorders are typically associated with a history of significant psychological trauma (post-traumatic stress disorder (PTSD) is a frequent comorbidity) and/or disruptions in early attachment relationships, which lead to disorganized attachment and dissociation.1–3
A recent meta-analysis by Lyssenko et al. 4 examined the severity of dissociative symptoms, as measured by the Dissociative Experiences Scale (DES), across a range of psychiatric diagnoses. Dissociative disorders were associated with the highest levels of dissociation, followed by PTSD, borderline personality disorder (BPD), and conversion disorder. These findings support a strong transdiagnostic link between trauma-related disorders and dissociation, a connection explored previously, for example, in the linkage between conversion disorder and the dissociative disorders.5,6 Compared to healthy controls, however, mean scores on the DES were elevated across almost all diagnoses, including substance-related disorders, schizophrenia, and mood and anxiety disorders. Clearly, dissociative phenomena are transdiagnostic and limited not only to the dissociative disorders or indeed even to trauma-related disorders.
Patients with high levels of dissociation typically present with a broad range of psychopathology that includes explicitly dissociative phenomena such as depersonalization, derealization, dissociative amnesia, and identity alteration. These dissociative symptoms, however, typically occur in the context of complex, polysymptomatic presentations characterized by high morbidity, and comorbidity. For example, in one sample of 280 patients with DID or DDNOS (based on DSM-IV criteria), 89% also had PTSD, 83% had a mood disorder, 54% had a cluster B personality disorder, 30% had an eating disorder, 22% had a substance use disorder, and 22% had a somatoform disorder. 7 Similarly, in an Australian sample, 48% of patients with a dissociative disorder had been hospitalized, of which 68% had been hospitalized more than five times. 8 In the same sample, 68% reported self-harm, and 69% reported suicide attempts, with 26% endorsing more than five past attempts. 8 Psychotic-like symptoms, which are not typically considered dissociative, are also observed frequently and may present in ways that are considered unusual or inconsistent with primary psychosis.1,9–17
Notably, these types of symptoms are also well described in the temporal lobe epilepsy (TLE) literature and are thought to emerge as a consequence of temporal lobe dysfunction. 18 Located bilaterally and inferior to the lateral fissure, the temporal lobe is one of the major lobes of the cerebral cortex. The medial temporal lobe is comprised of structures including the hippocampus, amygdala, uncus, dentate gyrus, and the parahippocampal gyrus that are involved in, or closely connected to, the limbic system, which is central to emotion, motivation, and memory. The lateral temporal lobe contains the primary auditory cortex as well as areas involved in visual processing, language processing, and complex object recognition. 18 The lateral temporal lobe also includes the temporoparietal junction (TPJ), which is believed crucial to self-processing, self-location, and perceived spatial unity of self and body, as well as multisensory integration of body-related information. Because of its role in “own-body” processing, the TPJ has been linked closely to dissociative symptoms such as depersonalization (e.g., out-of-body experiences) and identity disturbance.19–21
There is an urgent need to better understanding the occurrence of psychotic-like and dissociative symptoms in psychiatric disorders. In particular, the framing of these symptoms within a neurobiological context may facilitate not only improved assessment but also the treatment of patients across a range of psychiatric disorders presenting with dissociative and psychotic-like symptoms.
Aims of the Study
We will review the extant literature describing TLE-like symptoms (primarily psychotic-like and dissociative symptoms) observed across trauma-related disorders (PTSD, BPD, and the dissociative disorders) and the evidence for temporal lobe dysfunction in these patients. We then identify the clinical implications of this literature and discuss critical areas of future research.
Materials and Methods
The aim of this clinical overview is to discuss the phenomenology, etiology, assessment, and treatment of psychotic-like symptoms in trauma-related disorders (BPD, PTSD, and dissociative disorders) with attention to the proposed role of temporal lobe dysfunction. We have reviewed the literature via a PubMed search of articles published between 1980 and March 2018 using the following search terms: dissociative disorders, temporal lobe, trauma, post-traumatic stress disorder, borderline personality disorder, psychosis, and malingering.
Results
Dissociative Symptoms in TLE
A large body of literature has sought to examine the association between TLE and a variety of dissociative symptoms, motivated in part by Feindel and Penfield’s 22 initial observation of a “dreamy state” reported by their patients with TLE and, critically, reproducible with electrical stimulation of the temporal lobe. More recent work points toward a frequent association between TLE and dissociation. For example, in one case series, 33% of patients with TLE reported some form of interictal dissociative episodes. 23 In line with this observation, a series of large studies of patients with epilepsy found elevated scores on the DES, which is a widely used measure of pathological dissociation.24–27
Similarly, in a case series of patients with complex partial seizures, dissociative symptoms were reported by a significant portion of patients and included body part dissociation (19%), perception of surroundings as bizarre (11%), depersonalization (19%), and derealization (16%). 28 These observations were mirrored in a sample of 20 patients with TLE who completed the Cambridge Depersonalization Scale: 80% endorsed symptoms of depersonalization. 29 In a related review, the majority of patients with depersonalization that stemmed from an organic cause (including epilepsy, traumatic brain injury, and migraine) also showed evidence of temporal lobe dysfunction. 30 Taken together, these findings suggest a clear association between organic temporal lobe dysfunction and dissociative symptoms that are markedly similar to those seen in dissociative disorders.
Perhaps most strikingly, there have been numerous case series and reports connecting organic temporal lobe pathology (particularly TLE) to identity alteration identical to that seen in DID.31–33 It is notable that these case series include both experiences of multiple personalities and experiences of supernatural possession, both of which are known forms of identity alteration in DID. 1 For example, in one case series of 40 patients with electroencephalogram (EEG)-verified TLE, 13 patients reported experiences of multiple personalities and/or possession, including several cases of syndromal multiple personality disorder. 23 Similarly, in Mesulam’s 34 case series of 12 patients with TLE, 7 met criteria for multiple personality disorder (now called DID) and 5 reported experiences of supernatural possession. Critically, there is also mounting evidence that temporal lobe dysfunction other than TLE can produce DID-like symptoms. In one case study, a patient with traumatic brain injury and with evidence of biparietal and left temporal hypoperfusion on single photon emission computed tomography (SPECT) reported an episode of “multiple personality.” 35 This literature suggests that temporal lobe dysfunction is not only associated with dissociative symptoms, in general, but that it may also underlie the complex dissociative symptoms seen in disorders like DID.
Psychotic-Like Symptoms in Trauma-Related Disorders
TLE is associated with psychiatric presentations that resemble closely both dissociative disorders and psychotic disorders. It is notable that the psychiatric disorders with the most prominent dissociative and psychotic-like symptoms, including the complex dissociative disorders, BPD, and the dissociative subtype of PTSD, have been linked not only to psychological trauma but also to alterations in temporal lobe structure and function.14,36–40 The temporal lobe theory of dissociation provides a unifying account of these findings, pointing toward the transdiagnostic neurobiological underpinnings of these symptoms, with key implications for assessment and treatment.
Psychological Trauma
Strikingly, even in the absence of a diagnosable psychiatric disorder, psychological trauma has been associated with psychotic symptoms.41–44 For example, in one study, individuals with auditory verbal hallucinations (but without any DSM diagnosis) reported experiencing significantly more sexual and emotional abuse than healthy controls. 41 In other samples of trauma exposed but healthy individuals, associations have been reported between experiences of bullying and of unwanted sexual contact and subthreshold psychotic symptoms (e.g., brief duration symptoms or symptoms not causing distress or impairment).42–44 Although the relation between the nature of the trauma itself and the onset of specific psychotic symptoms remains unclear, traumatic events associated with intent to harm (i.e., perpetrated deliberately by another person) are more strongly associated with psychotic symptoms than nonintentional traumatic events (e.g., involvement in a life-threatening accident).42,45 A number of smaller studies have associated sexual abuse specifically with hallucinations and neglect/attachment-disrupting events (e.g., separations from caregivers) specifically with paranoia.42,46,47
In non-Western cultures (and some Western subcultures), dissociative and/or psychotic-like symptoms may be expressed as experiences of possession (identity alteration characterized by feeling taken over by an outside force, e.g., a spirit or demon, as opposed to internal self-states) and/or paranormal phenomena (e.g., contact with ghosts or spirits, telekinesis, telepathy, or precognitive dreams). These experiences typically occur in cultures where nonpathological possession is more normative, and they can be considered culturally specific representations of known dissociative syndromes. As such, pathological possession has been included in the diagnostic criteria for DID alongside the more Western experience of internal self-states.6,48 These symptoms, however, have been associated with trauma in general as well as specifically with DID. In one sample of women from the general population in Turkey, experiences of childhood or adulthood trauma were associated with possession and childhood abuse or neglect with paranormal phenomena. 49
Multiple studies have also found associations between traumatic life events and the development of primary psychotic disorders with odds ratios ranging from 2.8 to 7.3 reported in traumatized people compared to nontraumatized people.47,50 Trauma has also been associated with progression to psychotic disorders in clinically high-risk populations (e.g., individuals with prodromal symptoms or a family history of psychotic disorder), with the presence of psychotic features in affective illnesses (e.g., bipolar disorder and major depressive disorder), and with the intensity, persistence, and severity of psychotic symptoms in patients with schizophrenia.42,51–53 Thus, rather than being merely a specific etiological factor for the development of primary psychotic disorders, there is a transdiagnostic association between trauma and the presence and severity of psychotic symptoms (particularly abnormal sensory experiences) across a broad range of disorders and even in the absence of any diagnosable psychiatric illness.
Notably, in both clinical and nonclinical samples, dissociation has been identified as a mediator between trauma and psychotic experiences. Dissociation, as measured by the DES, has been associated both with psychotic experiences, in general, and with auditory hallucinations, particularly symptoms of depersonalization.47,54,55 Several cognitive pathways for this relationship have been proposed, including the proposal that dissociation may increase distance from internal experiences, rendering them more likely to be perceived as external/hallucinatory. 55 Moskowitz et al. 56 further suggest that in the context of trauma, not just hallucinations, but other psychotic symptoms, that is, disorganized speech, disorganized behavior, and possibly delusions, may be conceptualized as dissociative phenomena stemming from decontextualized traumatic content or intrusions of dissociated self-states.
Post-Traumatic Stress Disorder
Even in the absence of a primary psychotic disorder, patients with PTSD frequently report psychotic-like symptoms (e.g., in one sample of 568 patients with a lifetime diagnosis of PTSD, about 19% of patients with a history of PTSD reported hallucinations) and such endorsement is associated with greater overall PTSD severity.57,58 Indeed, “auditory pseudohallucinations” are discussed in the DSM-5 as an associated feature supporting the diagnosis of PTSD, with some trauma experts constructing these symptoms as frankly psychotic and calling for the addition of a “with psychotic features” specifier to the diagnostic criteria.1,58 A recent review of the evidence (mainly in a military population) found some evidence for a “PTSD with secondary psychotic features” construct, with phenomenological and biological differences from both PTSD and schizophrenia. 59
Across a series of studies, patients with PTSD, typically with complex trauma including war, childhood trauma, and refugee trauma, report a broad range of psychotic symptoms, including delusions, visual and auditory hallucinations, as well as more unusual sensory modalities, including olfactory and tactile hallucinations.10–12 In their clinical assessments of patients, particularly those involving women with childhood trauma histories, Frewen and Lanius 9 note that pseudohallucinations are common and are typically olfactory and tactile (e.g., sensations of bugs crawling on the skin). Some, but not all, of these patients report psychotic content that is related to the trauma, and it is experienced differently from traumatic reexperiencing.11,60,61 Moreover, compared to patients with psychotic disorders, these experiences tend to be briefer and include sensory modalities other than, or in addition to, auditory. Notably, in one study, the majority of traumatized participants reported a single voice coming from inside their head.10,11
In key recognition of the importance of dissociative symptoms in the psychopathology of PTSD, the DSM-5 has recently included a dissociative subtype. The dissociative subtype is characterized by primarily depersonalization and/or derealization responses to trauma-related cues, which contrast sharply with the hyperarousal and sympathetic nervous system activation observed in individuals with PTSD without the subtype. 1 Critically, psychotic-like experiences may be linked in particular to the dissociative subtype of PTSD, where psychotic symptoms have been associated with higher scores on the DES in multiple studies.11,47,54,55,60 Notably, trauma is also associated with measures of somatoform dissociation, which encompasses symptoms that could be seen as psychotic-like or TLE-like (alterations of taste, smell, and visual perception, and seizure-like episodes). 62
Borderline Personality Disorder
BPD is associated with traumatic life events (particularly childhood abuse) with some authors proposing that childhood trauma serves as part of a multifactorial etiology for the disorder.36,63 Among individuals with BPD, estimates of the prevalence of childhood maltreatment typically range from 76% to 90% for childhood neglect and from 80% to 81% for childhood abuse (physical, sexual, or emotional), which is higher than the prevalence in patients with other personality disorders, although one recent review identified some heterogeneity in these rates and suggested that prevalence may range from 30% to 90% for any kind of childhood trauma.36,63–65
In a pattern similar to that observed in studies of patients with PTSD, BPD is associated with both dissociative and psychotic symptoms. Indeed, severe dissociative symptoms are included in the diagnostic criteria, and the prevalence of comorbid dissociative disorders in BPD has been estimated between 59% and 76%, with 10% to 27% meeting criteria for DID.1,66,67 The most common psychotic symptoms observed in BPD are auditory verbal hallucinations, which occur in 20% to 40% of these patients.13,42 These hallucinations are long-standing, generally identified as negative and distressing, come from inside the head, and are sometimes (but not always) associated with traumatic memories (e.g., hearing the voice of a past abuser).68–70 Despite their common conceptualization as “pseudohallucinations” that are clearly distinct from primary psychosis in phenomenology, when compared to the auditory hallucinations experienced by patients with schizophrenia or schizoaffective disorder, no significant difference has been found in duration, degree of distress, or location (inside vs. outside the head) of BPD-associated hallucinations, and both groups at times report content related to past traumatic experiences.69,70 Moreover, much like in PTSD, unusual sensory modalities are reported frequently. For example, in one sample of patients with BPD, 30% reported delusions, 20% reported visual hallucinations, 13% reported tactile hallucinations, and 10% reported olfactory hallucinations. 13
Dissociative Depression
The key literature points to a critical link between childhood trauma and the onset of increased levels of dissociation in patients with major depression. 71 Indeed, the concept of “dissociative depression” has been proposed recently in an attempt to better classify a subset of patients with major depression who also exhibit concurrent dissociative symptoms. In one sample of Turkish women with no differences in comorbidity profile from individuals with nondissociative depression (i.e., no increase in comorbid BPD, PTSD, or dissociative disorder), dissociative depression was associated with a positive trauma history, PTSD-like cognitive distortions, frequent mood swings, and impulsivity. These patients also reported psychotic-like symptoms similar to those seen in other trauma-related disorders such as hallucinations, amnesias, experiences of possession, and identity alteration symptoms. 72
Depersonalization Disorder
Depersonalization disorder is a dissociative disorder characterized by chronic feelings of detachment from or unreality of the body or self, a common experience in TLE. Depersonalization disorder can also be associated with childhood trauma. 73 Although complex partial-seizure-like symptoms other than depersonalization/derealization themselves have yet to be explored fully in patients with diagnosed depersonalization disorder, nevertheless, in a sample of patients with BPD or PTSD, depersonalization/derealization symptoms were strongly associated with the presence of pseudohallucinations independent of diagnosis, and scores on the depersonalization subscale of the DES were the most strongly associated with psychotic symptoms.55,74
DID and OSDD
DID and DID-like presentations of OSDD have been related to severe and prolonged early life trauma. 14 These disorders are strongly associated with psychotic-like symptoms, including voices and, in a pattern similar to that observed in PTSD and BPD, hallucinations involving multiple sensory modalities, particularly unusual ones such as tactile, gustatory, or olfactory hallucinations.1,15 Some of these symptoms can be difficult to distinguish from schizophrenia. For example, patients with DID frequently report voices that are both internally and externally perceived, as well as Schneiderian first-rank symptoms (most commonly voices conversing with each other or commenting on the person’s actions, made thoughts, and made actions).15–17
Paranormal phenomena and experiences of possession are sometimes seen in dissociative disorders, particularly in cultures where nonpathological possession is culturally normative, and can be interpreted as psychotic. Epilepsy, particularly TLE, has also been associated with religious and mystic experiences. 75 The DSM-5 now includes possession as part of the diagnostic criteria for DID, in order to increase cross-cultural applicability of the diagnosis.1,6 In one sample of women in the general population in Turkey, 33% of those with a dissociative disorder reported at least one type of paranormal experience compared to 17.3% of those without and 10.4% of those with a dissociative disorder reported experiences of possession compared to 0.2% of those without. 49 In another study, compared to unmatched samples of psychiatric outpatients and members of the general population, a sample of patients with DID reported more trance, sleepwalking, possession, and paranormal experiences. 76
The recent literature has attempted to identify those symptoms that may be particularly useful in differentiating psychotic disorders from complex dissociative disorders. Although Schneiderian first-rank symptoms were originally thought to be pathognomonic for a primary psychotic disorder, in one study, patients with DID endorsed an average of 6.4 Schneiderian first-rank symptoms, far more than the 1.3 endorsed by patients with schizophrenia. 17 In another sample of 30 patients with multiple personality disorder by DSM-III criteria, all patients endorsed at least one first-rank symptom at some point in the course of treatment, with the average number endorsed being 3.6. 16 There are, however, some key features of psychotic symptoms (specifically auditory hallucinations) that distinguish complex dissociative disorders. For example, Dorahy et al. 15 found that compared to patients with schizophrenia, patients with DID were more likely to hear multiple voices, to hear child voices, and to have started hearing voices before the age of 18 years. Patients with DID were also more likely to experience visual, olfactory, and tactile hallucinations than were patients with schizophrenia. 15
Temporal Lobe Dysfunction in Trauma-Related Disorders
Psychological Trauma
Recent data support a strong association between childhood psychological trauma (either in the absence of overt psychopathology or with mixed psychiatric diagnoses) and structural and functional alterations of the temporal lobe. In studies of children and adolescents with low psychopathology, a history of abuse is associated with decreased temporal cortical thickness and reduced right temporal volume.77,78 In line with these findings, magnetic resonance imaging (MRI) studies of psychiatrically ill samples of traumatized children (with a broad range of diagnoses including PTSD) reveal increased gray matter volumes in the superior temporal gyrus.79,80 On qEEG, children who have been abused show differences in hemispheric coherence and asymmetry, with the temporal region being among those regions most prominently affected.81,82 Functionally, alterations in resting state activity in the superior temporal gyrus have been reported in adults without psychiatric illness exposed to early life trauma. 83 Finally, exposure to trauma-related cues may provoke temporal lobe activation in traumatized populations; a study of youth with a history of emotional neglect revealed increased activity of the medial temporal lobe on exposure to threatening cues. 84
Post-Traumatic Stress Disorder
Related studies reveal temporal lobe abnormalities among individuals with a formal diagnosis of PTSD. For example, in one MRI study, compared to healthy controls, patients with PTSD (not separated by subtype) showed decreased gray matter volume in the right temporal lobe, including the middle and inferior gyri and the fusiform gyrus, which together are involved in perception and memory. Compared to a sample of psychiatric patients with obsessive compulsive disorder (OCD), this sample also had decreased right temporal gray matter volume. 85 Other MRI studies have corroborated the finding of decreased right temporal lobe volume and neuron density across a variety of types of index traumas86–88 and, critically, one has linked volume loss in the right inferior temporal gyrus specifically to the dissociative subtype of PTSD. 89 In keeping with these observations, another study found an association between increased flashbacks and volume loss in the middle temporal gyrus in patients with PTSD. 90 These findings suggest a highly specific role of the temporal lobe in abnormal processing of somatosensory information (e.g., self-other differentiation errors in dissociative symptoms and decontextualized sensory material in flashbacks). Similarly, one study of sexually abused adolescents, overall those with PTSD had smaller hippocampal and amygdala volume bilaterally, and within that group, a smaller right amygdala was associated with passive influence phenomena, one of the psychotic-like symptoms seen in trauma-related disorders, further linking the temporal lobe to these symptoms. 91
Notably, symptom provocation studies have consistently revealed an association between reexperiencing symptoms and decreased temporal lobe activation.92,93 In a functional MRI (fMRI) study of adults with PTSD who dissociated when exposed to trauma-related cues, however, there was an increased activation in the superior and middle temporal gyri and altered right temporal connectivity.37,38 Another study of PTSD patients’ response to fearful faces also demonstrated an association between dissociative symptoms and increased temporal lobe activation. 94 Finally, in a sample of patients with lower overall dissociation proneness and primarily single-incident trauma (motor vehicle accident), dissociation in response to traumatic scripts nevertheless remained positively correlated with right temporal activation and negatively correlated with left temporal activation. 95 On balance, these data support strongly the assertion that both the dissociative subtype of PTSD and state dissociation in PTSD are associated specifically with altered temporal lobe activity in response to trauma-related cues.
These alterations in temporal lobe structure and function have been observed within the context of an emerging body of the literature that highlights altered functional connectivity in PTSD, which, importantly, is present even in the absence of overt trauma-related stimuli/reexperiencing. For example, there is a strong evidence of altered temporal connectivity and activity (particularly the right temporal lobe) on resting state fMRI across a variety of index traumas, despite the clear absence of provocation stimuli.96–100 In the dissociative subtype specifically, increased functional connectivity has been observed between the amygdala and areas involved in consciousness, awareness, and proprioception, as well as those thought to be involved in depersonalization and derealization symptoms (the superior parietal lobe, dorsal posterior cingulate, and precuneus). 101
Similarly, patients with and without the dissociative subtype demonstrate increased connectivity at rest between the periaqueductal gray matter in the midbrain, which is involved in defensive responses, and the fusiform gyrus, which is involved in scanning the environment, and is also connected with the amygdala. 20 There is also an evidence of increased resting state connectivity between the superior colliculus, which is involved in threat detection, and the right TPJ, which is implicated in depersonalization and derealization. 21 These patterns of connectivity suggest changes in subconscious threat processing that are evident even in the absence of overt threat or trauma-related stimuli and that together may affect day-to-day engagement with the external environment.
Borderline Personality Disorder
Structural imaging studies of male and female patients with BPD reveal strikingly similar patterns of decreased gray matter volume and density in the temporal lobes, with one study further illustrating a specific decrease in right temporal lobe volume among individuals with BPD and a history of abuse.102–104 Consistent findings of decreased amygdala and hippocampal volume have also emerged in BPD.105–107 Functional imaging of a sample of patients with BPD and histories of childhood abuse and severe dissociative symptoms similarly demonstrated right-sided temporal hypometabolism. 108 Finally, on neuropsychological testing, patients with BPD have show profiles suggestive of right temporal lobe dysfunction. 109
Depression With Dissociative Features
Further research is necessary to identify specific neurobiological correlates of this depressive phenotype. However, one SPECT study on patients with DID with a 66.7% prevalence of comorbid depression (i.e., dissociative depression) noted left lateral temporal hyperperfusion in the sample as a whole. 110
Depersonalization Disorder
In a pattern similar to that observed in other trauma-related disorders, on structural imaging, depersonalization disorder is associated with decreased right temporal cortical thickness and with right temporal hypometabolism on functional imaging.111,112 Recent work has also demonstrated altered white matter structural connectivity between the right middle temporal gyrus, which may be involved in sensory integration, and the right supramarginal gyrus, which is a part of the somatosensory association cortex, as well as decreased structural connectivity between the left temporal pole, which is thought to be an association area, and the left superior temporal gyrus, which is involved in auditory processing. 113 Depersonalization has also been associated with temporal slowing on EEG. 114
DID and OSDD
Studies of patients with DID and comorbid PTSD reveal decreased temporal lobe cortical volume and cortical surface area compared to healthy controls.115,116 For example, an MRI study of 15 female patients with DID revealed a 19.2% decrease in hippocampal volume and a 31.6% decrease in amygdala volume compared to controls. 117 Case reports, along with small SPECT studies of patients with DID, have demonstrated consistently that compared to healthy controls and DID simulators, patients with DID show increased perfusion in the left temporal lobe and that temporal perfusion increases while in a dissociated self-state.110,118–120 In a related case report, EEG differences between a series of dissociated self-states were most prominent in the left temporal area. 121 The exact neurobiological underpinnings of switching between self-states remain under investigation. Notably, an fMRI of one patient performed during the process of voluntarily switching between self-states revealed right medial temporal inhibition, suggesting the possibility of temporal lobe involvement in this process. 122
A growing body of recent literature has examined neurobiological differences between DID self-states. For example, one study compared two types of self-states in DID: trauma-fixated self-states that personally identified with, and were highly physiologically reactive to, the individual’s traumatic memories and trauma-avoidant self-states that were amnestic for, or disowned, traumatic experiences. When exposed to masked neutral faces (that may have been perceived as threatening stimuli), trauma-fixated self-states showed increased activation in a range of areas including the occipitotemporal junction and parahippocampal gyrus when compared to DID-simulating controls. 123 Another study that differentiated the response of trauma-fixated and trauma-avoidant self-states to written traumatic scripts found that the trauma-avoidant self-states demonstrated activation patterns similar to those observed in patients with the dissociative subtype of PTSD. 40 Moreover, compared to trauma-fixated self-states, these trauma-avoidant self-states activated areas involved not only in overmodulation of emotional arousal but also areas with a proposed relationship to dissociative amnesia, including parahippocampal and right-sided temporal areas, as well as posterior association areas that included the fusiform and parahippocampal gyri. 40
Assessment of Temporal Lobe Abnormalities: Limbic Irritability and the Limbic System Checklist-33
Limbic irritability has been identified as a key measure of altered temporal lobe function. 124 Limbic irritability may be assessed using the Limbic System Checklist (LSCL-33), which measures symptoms associated with ictal TLE, including somatic, sensory, behavioral, and mnemonic disturbances. Individuals exposed to childhood maltreatment score high on the LSCL-33 compared to controls who have not experienced maltreatment, providing further support for temporal lobe dysfunction in traumatized populations. 124
Elevations on the LSCL-33 are also observed in samples of patients with pathological dissociation. In these studies, higher scores on the DES correlate with not only with elevated LSCL-33 scores but also with elevated scores on the Iowa Interview (a measure of complex partial seizure-like symptoms, such as dysnosmias, auditory hallucinations, anesthesias, and visual distortions) and other complex partial epileptic-like signs (visual anomalies, auditory-vibrational experiences, automatic behaviors, depersonalization, and “sense of a presence”).125–127 Notably, patients with BPD, which includes dissociation among its diagnostic criteria, also exhibit elevated scores on the LSCL-33 compared to patients with depression and anxiety, along with scores comparable to those seen in patients with TLE. 109 On balance, the LSCL-33 appears a useful tool for quantifying the presence and severity of these symptoms among traumatized individuals.
Assessment of Malingering
The literature clearly indicates that patients with trauma-related disorders frequently experience psychotic-like symptoms, that these symptoms overlap substantially with the symptoms of TLE, and, finally, that there is a strong evidence of organic temporal lobe dysfunction among these patients. As such, clinicians should not be surprised by the presence of psychotic-like and TLE-like symptoms in patients with trauma-related disorders. Nevertheless, because these symptoms remain underexplored and often underdocumented and are atypical of the primary psychosis that clinicians may be more familiar with, these symptoms are typically misunderstood and misdiagnosed as either primary psychosis or as malingering. Indeed, these patients can be mistakenly classified as malingering not only by those instruments designed specifically to detect exaggeration of symptoms and malingering but also by the validity scales present in more general psychological tests.128–135 As discussed earlier, these patients also typically present with a wide range of severe symptoms that span multiple diagnostic categories, which contributes further to invalid testing profiles and positive malingering screens.7,8 For example, in one study of male combat veterans with PTSD and psychotic-like symptoms, 46% were classified as above the cutoff for malingering on the Miller Forensic Assessment of Symptoms Test (MFAST), mainly due to endorsement of unusual hallucinations (e.g., tactile hallucinations and visual hallucinations in black and white) and rare combinations of symptoms. However, when these patients were given the Structured Interview of Reported Symptoms (SIRS), only two scored within the malingering range. 11 Thus, although the presence of psychotic-like symptoms resembling those seen in TLE (i.e., tactile and visual hallucinations) was directly responsible for trauma patients being classified as malingering on the MFAST, when these symptoms were explored more fully, it was apparent that these represented false-positive classifications of malingering in the vast majority of patients, calling into question the utility of this screening tool in traumatized populations.
Structured Interview of Reported Symptoms
On the SIRS, a widely used structured interview intended to identify feigned psychological symptoms, high levels of diffuse pathology, and supposedly “rare” symptoms are taken as indicators of possible feigning. Critically, however, these so-called rare symptoms include common and expected manifestations of trauma-related disorders such as depersonalization and other dissociative symptoms. It is therefore not surprising that people with trauma-related disorders are at risk of being misidentified as feigning by the SIRS. Indeed, in one study of a DID population, 35% of patients with actual DID were misclassified by the SIRS as feigners. 128 Similarly, in a related study of severely traumatized patients, about half of whom also met criteria for DID, 31% were misclassified as feigners. 133
In response to the limitations of the SIRS in assessing patients with trauma-related disorders, a revised version of the SIRS, the SIRS-2, was created. The SIRS-2 contains the same items as the SIRS but utilizes revised scoring and interpretation criteria. 129 In a recent study of the SIRS-2, more than half of the patients with DID scored above the total cutoff score for feigning (indicating endorsement of a wide range of severe symptoms) and higher than the genuine range on its Rare Symptoms Scale. 129 Moreover, 88% of patients with genuine DID endorsed at least one of the items on the Rare Symptoms Scale likely because this scale continues to includes dissociative symptoms (depersonalization and derealization). Ultimately, a combination of the SIRS-2 and the Trauma Index (TI) demonstrates the highest specificity in distinguishing genuine from feigned DID. 129 Taken together, this research clearly illustrates the urgent need to revise these instruments in a trauma-informed manner that allows for more accurate classification of this population and in doing so prevents potentially unjust adverse outcomes in disability and forensic proceedings.
Minnesota Multiphasic Personality Inventory
On the Minnesota Multiphasic Personality Inventory (MMPI-2), patients with DID can sometimes be mistaken for psychotic due to their reports of hearing voices (e.g., of their dissociated self-states). In some cases, DID patients score higher on the schizophrenia subscale than patients with diagnosed schizophrenia.131,136 Patients with DID and patients with histories of complex trauma also tend to have elevated scores on the MMPI-2’s validity scale, the F scale, which encompasses symptoms reported by less than 10% of the population against whom the test was normed.130,131 F-scale items include experiencing bizarre sensations and unusual thoughts, although F-scale elevations were thought to be valid predictors of malingering. In one sample of female childhood sexual abuse survivors, F-scale elevations were associated with depression, dissociation, and posttraumatic stress, with dissociative symptoms being the best predictor for elevation on this scale. 137 Similarly, in a sample of patients with DID, F-scale elevations were associated with endorsement of known dissociative symptoms, including blank spells, doing things without remembering them, and ideas of mind control, which are not rare in severely dissociative populations.131,136 This research shows that in trauma-related disorders, the ability of the MMPI-2 to identify invalid profiles is severely limited by the overlap between F-scale items, which were uncommon in the normative sample on which the MMPI-2 was developed, and the dissociative and psychotic-like symptoms that are in fact common in trauma-related disorders.
Personality Assessment Inventory
The Personality Assessment Inventory (PAI) has three feigning indicators, including the Negative Impression (NIM) scale that is intended to measure rare or unusual symptoms, including memory loss and dissociative self-states, lack of positive memories in childhood, and the sense that others do not understand the severity of one’s problems. Critically, the NIM is elevated significantly in samples of traumatized veterans, patients with PTSD, and patients with PTSD and DID, and unsurprisingly given their severe trauma exposure, the highest elevations occur in patients with DID.134,138 In a pattern similar to that observed with the MMPI-2, these elevations in NIM appear affected by depression, dissociative symptoms, and borderline personality features. 135 Hence, it is clear that the PAI also overclassifies patients with trauma-related disorders as malingerers rather than as suffering from legitimate symptoms that are consistent with evidence-based findings about the impact of trauma.
Implications for Assessment
Across a wide range of psychological tests, including both screening malingering measures and more structured assessment tools, complex dissociative symptoms lead frequently to elevations on malingering scales.128,129,131,133,134,136,137 These elevations are found consistently in a wide range of traumatized populations by numerous researchers in a variety of contexts, which suggests that the elevations are not due to malingering but rather due to the impact of trauma, including high levels of dissociation, and a severe, wide range of symptoms, leading to a significant burden of illness. Unfortunately, many clinicians and test developers are unaware of the high levels of legitimate psychopathology associated with trauma exposure, including seemingly rare and severe symptoms such as dissociative and “psychotic” symptoms. Moreover, the symptoms that are labeled as rare and unusual by these scales are instead typical and expected in traumatized population and are frequently part of the DSM-5 diagnostic criteria for trauma-related disorders (Table 3). For example, a common item on such subscales is experiences of leaving or feeling outside of one’s body. In comparison, the DSM-5 (pp. 302–303) describes depersonalization (which is a part of the diagnostic criteria for PTSD) as “experiences of unreality, detachment, or being an outside observer” of oneself and specifically gives the example of “out of body experiences.” 1 As has been previously reviewed, the literature on TLE and on temporal lobe dysfunction in patients with trauma-related disorders points strongly toward the temporal lobe hypothesis as a plausible explanation for these symptoms.
By misidentifying traumatized patients as malingerers, these instruments contribute to substantial delays in accurate diagnosis and effective treatment of trauma-related disorders. There may also be significant practical consequences. Notably, childhood trauma exposure and high levels of dissociation are common in forensic populations, and dissociative disorders are overrepresented compared to the general population. For example, one study found that 25% of a forensic sample had a dissociative disorder, which is more than twice the rate found in the general population. 139 Forensic patients, whose criminal responsibility may be assessed in part on the basis of psychological testing, and in whom dissociative disorders are overrepresented, may therefore be at particularly high risk for being misidentified as malingering. These decisions may have devastating forensic implications. For example, traumatized individuals may receive unjustly harsh sentences, including, in some countries, the death penalty, if the jury is not given the opportunity to consider fairly the impact of their genuine mental illness. Moreover, misclassifications of malingering can have serious medicolegal implications, for example, patients could have disability insurance claims unjustly denied if they are felt to be malingering, despite their legitimate and disabling symptoms. It is important to emphasize the life-altering pragmatic impact that an attribution of malingering can have in such circumstances.
If psychological testing is used in trauma-related disorders either for the purposes of diagnosis or in the forensic system in assessments of malingering, it is an ethical imperative to carefully consider the limitations of validity scales in these populations and to utilize classification rules with established validity in trauma-exposed populations (e.g., the TI from the SIRS or SIRS-2). Otherwise, assessors may draw conclusions that are not only inaccurate but have the potential to be highly damaging.
Discussion
Clinical Implications
Key features of primary psychosis, trauma-related disorders, and TLE.
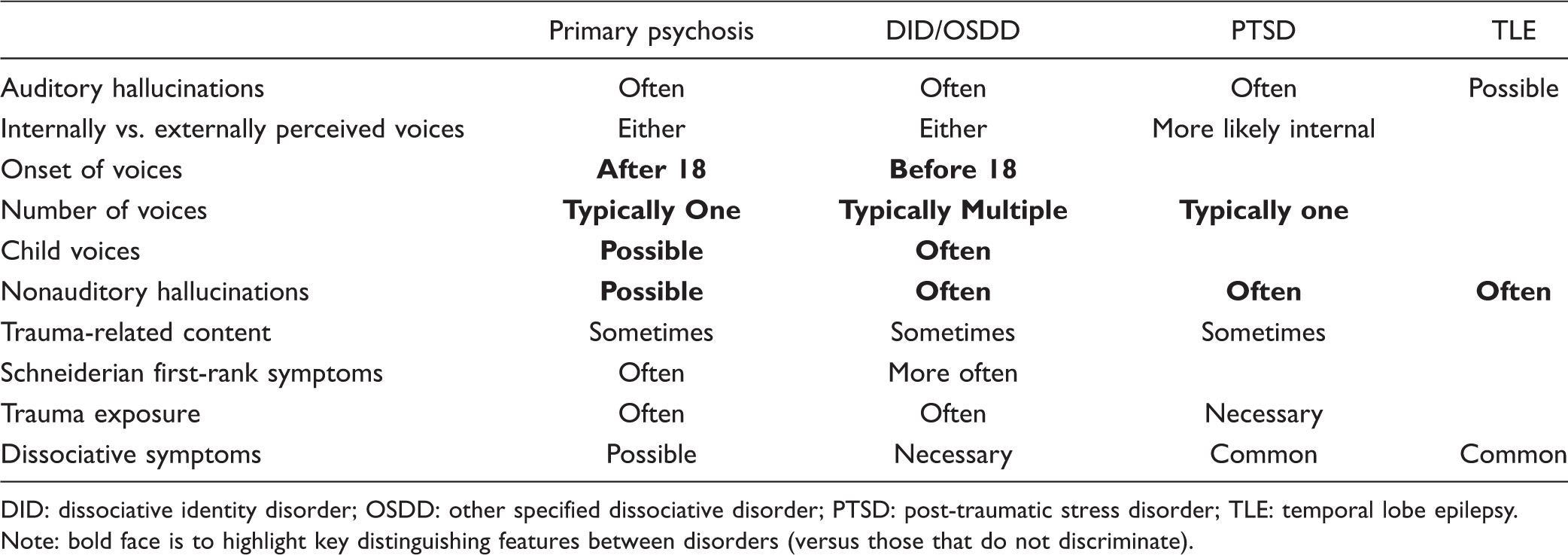
DID: dissociative identity disorder; OSDD: other specified dissociative disorder; PTSD: post-traumatic stress disorder; TLE: temporal lobe epilepsy. Note: bold face is to highlight key distinguishing features between disorders (versus those that do not discriminate).
Temporal lobe dysfunction in trauma-related disorders.

BPD: borderline personality disorder; DID: dissociative identity disorder; OSDD: other specified dissociative disorder; PTSD: post-traumatic stress disorder.
Areas of substantial overlap between validity scale items, dissociative symptoms, and temporal lobe epilepsy-like symptoms.
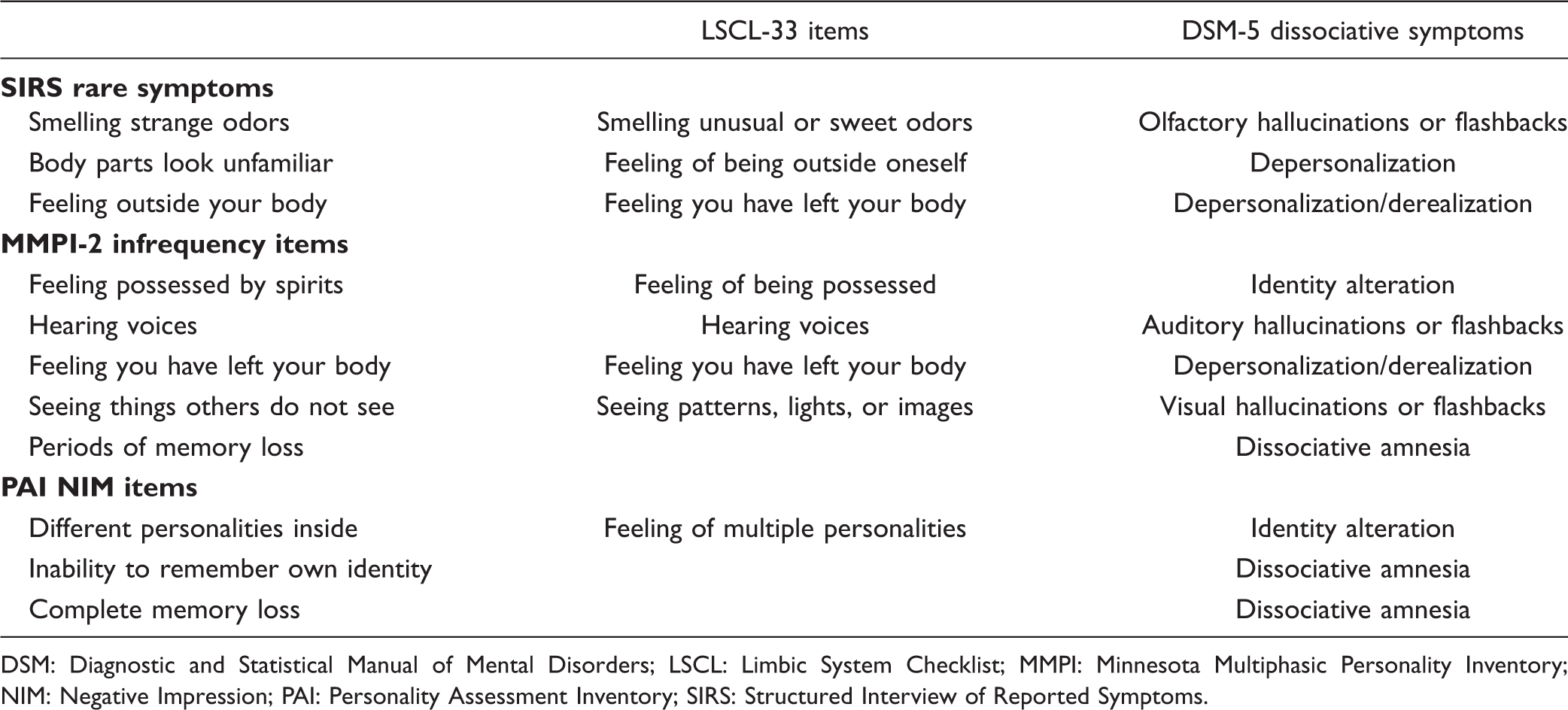
DSM: Diagnostic and Statistical Manual of Mental Disorders; LSCL: Limbic System Checklist; MMPI: Minnesota Multiphasic Personality Inventory; NIM: Negative Impression; PAI: Personality Assessment Inventory; SIRS: Structured Interview of Reported Symptoms.
The temporal lobe theory of dissociation provides clarification in understanding these symptoms within a neurobiological framework as well as evidence for their transdiagnostic nature. The literature shows that psychological trauma and a wide range of trauma-related disorders are associated with strikingly similar alterations in the structure and function of the temporal lobe (Table 2). Patients with complex trauma often experience psychotic-like symptoms identical to those observed in patients with organic temporal lobe dysfunction (particularly TLE), but these symptoms are frequently understood as psychotic or reflective of malingering, rather than as dissociative symptoms originating from the temporal lobe. The temporal lobe theory of dissociation therefore unifies dissociative symptoms and psychotic-like symptoms as a group of trauma-related symptoms and points strongly to trauma-related temporal lobe dysfunction as a neurobiological underpinning of this often misinterpreted trauma-related symptom cluster. For example, a patient with PTSD may experience episodes of depersonalization, identity alteration, olfactory hallucinations, and auditory verbal hallucinations. By applying the temporal lobe theory of dissociation, the clinician can understand that, rather than having a series of unconnected and bizarre symptoms, this patient may in fact have multiple TLE-like features that are all explained by their trauma-related disorder and by alterations in their temporal lobe structure and function.
When indicators of complex trauma and dissociation are present, a careful trauma history as well as a full review of dissociative symptoms should be undertaken to clarify the diagnosis. Tools such as the DES or Loewenstein’s 140 semistructured Office Mental Status Examination for Chronic Complex Dissociative Symptoms can be invaluable in assessing these features. Complex partial seizure and TLE-like symptoms should also be specifically assessed, and, if TLE is ruled out as an etiology, these symptoms should be considered as the part of the trauma-related disorder rather than as indicative of a comorbid primary psychosis. They should therefore be managed according to the treatment guidelines for posttraumatic and dissociative disorders. 141 In the case of dissociative disorders, the prototypical example of trauma-related dissociation, we know that treatment targeted specifically at the dissociative disorder is associated with a range of improvements in symptoms and in functioning as well as with decreased psychiatric hospitalizations and decreased health-care utilization costs, making identification of these disorders even more paramount.142,143
Future Directions
Researchers are beginning to study, and when necessary, adapt, psychological tests to provide valid conceptualizations and classifications of patients with trauma-related disorders (e.g., the TI developed for the SIRS and SIRS-2). Much more research is needed to document and remediate existing deficiencies in the assessment of patients with trauma-related disorders, including those who present with psychotic-like symptoms (Table 3). Validity scales should be developed that do not rely on dissociative or TLE-like symptoms to identify malingering, thus allowing for more accurate assessment of malingering in this population.
Currently, there is a minimal literature on specific treatments for TLE-like symptoms in individuals who have experienced complex trauma. Expert opinion currently suggests that psychotic-like symptoms do not respond to the same treatments as primary psychotic disorders. 141 Although antipsychotics may assist with PTSD-related intrusions, thought organization, anxiety and irritability, they are not recommended for the treatment of hallucinations in patients with trauma-related disorders (either voices related to the intrusion of other dissociated self-states or complex partial seizure-like olfactory, tactile, and gustatory hallucinations). 141 Moreover, although antiepileptic mood-stabilizing medications such as lamotrigine, divalproex, and carbamazepine are sometimes used in this population to manage mood instability or comorbid bipolar disorder, the ability of antiepileptic medications to address TLE-like symptoms in nonepileptic complex trauma populations remains to be studied. 141 Future work may also focus on nonpharmacological treatments, such as psychotherapy, or emerging adjunctive treatments, such as real-time fMRI neurofeedback to upregulate or downregulate relevant areas of the temporal lobe. 144
Take Home Points
Psychotic-like symptoms, particularly nonauditory hallucinations, are common across trauma-related disorders, as are dissociative symptoms. The psychotic-like and dissociative symptoms observed in trauma-related disorders, including in some cases experiences of possession and supernatural experiences, resemble those observed in TLE. The recent literature points toward the temporal lobe dysfunction as a potential unifying mechanism behind trauma-related and dissociative psychopathology in trauma-related disorders. These symptoms are often not assessed by clinicians or are misattributed to malingering, when instead they are core symptoms of trauma-related disorders. Misunderstanding of these symptoms can lead to adverse clinical outcomes, including misdiagnosis, the use of inappropriate medications, and wide-ranging medicolegal consequences.
Clinical Recommendations
Patients with trauma-related disorders should be screened for psychotic-like symptoms, and, if present, they should be considered part of the trauma-related disorder, provided that TLE has been ruled out. Psychotic-like symptoms should be managed as per treatment guidelines for the trauma-related disorder in question, as antipsychotics are frequently not effective. Psychological testing profiles should be interpreted with caution in patients with a history of trauma, and available literature on typical testing profiles and limitations should be incorporated into the interpretation. Further research and revision are necessary to reduce the inclusion of dissociative, psychotic-like, and other trauma-related symptoms on exaggeration and malingering indices.
Additional Comments
The literature on specific treatments for psychotic-like symptoms in trauma-related disorders is limited, thus limiting the ability to make detailed treatment recommendations. There are limited neuroimaging studies that examine specifically the subpopulation of patients with psychotic-like symptoms and trauma-related disorders.
Footnotes
Acknowledgments
The authors thank Nancy Mazza for assistance with manuscript preparation and submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this review was from the Canadian Institutes of Health Research, grant #148784.