
Abstract
Psychological stress, a subjective perception of an adverse environmental change, is a hallmark of modern society. Although psychological stress has previously been established as a risk factor for cardiovascular disease (CVD), it is unclear whether stress influences cardiovascular risk differently in men versus women. Gender disparities exist in the prevalence of stress as well as in the prevalence and prognosis of CVD; therefore, associations between stress and CVD risk and mortality may vary by sex. The purpose of this review was to summarize the evidence from recent and landmark studies on gender differences in the associations of stress with CVD risk factors and end points and to highlight clinical and public health implications as well as future research directions in this field. Taken together, research to date indicates that while stress is associated with poorer cardiovascular health metrics in both men and women, the influence of stress on measures of glucose regulation and dyslipidemia and on overall CVD risk may be stronger among women. However, men may be more susceptible to the influence of stress on body adiposity, blood pressure, and CVD mortality. In terms of behavioral risk factors for CVD, associations between stress and diet quantity and quality appear to be stronger among women, but the influence of stress on sedentary behaviors and sleep may be stronger among men. Given that gender disparities exist in the prevalence of overall and different types of stress (eg, financial stress, caregiving stress, and occupational stress), future studies should decipher the potential differential associations between types of stress and cardiovascular risk among men and women to identify vulnerable populations and develop targeted interventions.
Introduction
Stress is conceptualized in the literature in different ways: psychological stress and stress from environmental exposures. 1,2 Psychological stress can occur when there is a perception by an individual that environmental demands exceed his or her adaptive capacity. An individual’s response to events that are representative of this overload represent perceived stress and negative emotions. 1 Stress can also occur from exposure to acute and chronic environmental factors, which tax an individual’s ability to cope. 2 Chronic psychological stress, a subjective perception of an adverse environmental change, is a hallmark of modern society. 3 Every individual at some point in his or her life experiences chronic stress 4 due to job pressure, money concerns, health-related issues, poor nutrition, sleep deprivation, relationships, and other factors. 5
In 2014, approximately 77% of the US population reported experiencing some form of stress. 5 Chronic, daily stressors at work and in one’s personal life can increase the risk of developing and dying from cardiovascular disease (CVD) and are linked to poor prognosis among individuals with CVD. 6 Cardiovascular disease is the leading cause of death in the United States and is influenced by clinical factors and lifestyle/behavioral risk factors. 7 Emerging evidence is suggestive that daily stressors may also influence lifestyle behaviors such as diet, sleep, physical activity patterns, and cardiometabolic risk factors, which represents an important potential mechanism through which stress may increase CVD risk. 8 Additional biological mechanisms through which stress can alter cardiovascular risk include increased hypothalamic–pituitary–adrenal (HPA) axis activity, heightened autonomic nervous system reactivity, inflammation, oxidative stress, endothelial dysfunction, and increased catecholamine-induced lipolysis leading to an increase in dyslipidemia. 9
Although psychological stress is an established risk factor for CVD, it is unclear whether stress influences cardiovascular risk differently in men versus women. 10 Women may be more prone to experiencing stress than men. A 2017 survey conducted by the American Psychological Association (APA) showed that women reported significantly higher levels of overall stress than men. 11 According to the 2017 APA survey, in which stress was assessed on a scale of 1 to 10, women experienced an increase in stress levels from 5.0 to 5.1 over the previous year, while men experienced a decline from 4.6 to 4.4. 11 Similarly, although CVD is a leading cause of death in both sexes, recent data suggest that gender disparities also exist in the prevalence and prognosis of CVD. 12 In particular, rates of myocardial infarction and fatal coronary heart disease (CHD) are higher among elderly women, and there has been a stagnation in improvements in CHD incidence and mortality among younger women (<55 years). 13 Conversely, men have conventionally experienced an approximate 2-fold greater incidence of CHD and related mortality than women, but the gap in morbidity narrows with increasing age as elderly women experience greater incidences of heart disease. 14
Although gender disparities exist in the prevalence of stress and CVD, it is unclear whether the cardiovascular effects of stress are more or less pronounced among women compared to men. Understanding gender differences in the role of stress in CVD etiology may help to explain some of the observed disparities in CVD prevalence and prognosis and illuminate new perspectives for CVD prevention. The purpose of this review was to review published research from landmark studies on stress and cardiovascular risk that were conducted in single-sex populations or that examined sex differences, with a focus on studies conducted in the last 10 years. Studies were included in this review if they evaluated any form of psychological stress including chronic stress, perceived stress, psychosocial stress, job strain, job dissatisfaction, and marital strain in relation to cardiovascular health metrics including: blood pressure (BP), body adiposity, dyslipidemia, glycemic regulation, diet, physical activity, and sleep. These studies are summarized in Tables 1 –5. In addition to summarizing the evidence base, we highlighted clinical and public health implications of study findings to date and identified research gaps and necessary future research directions.
Observational Studies on Gender Differences in the Association of Stress With Blood Pressure.
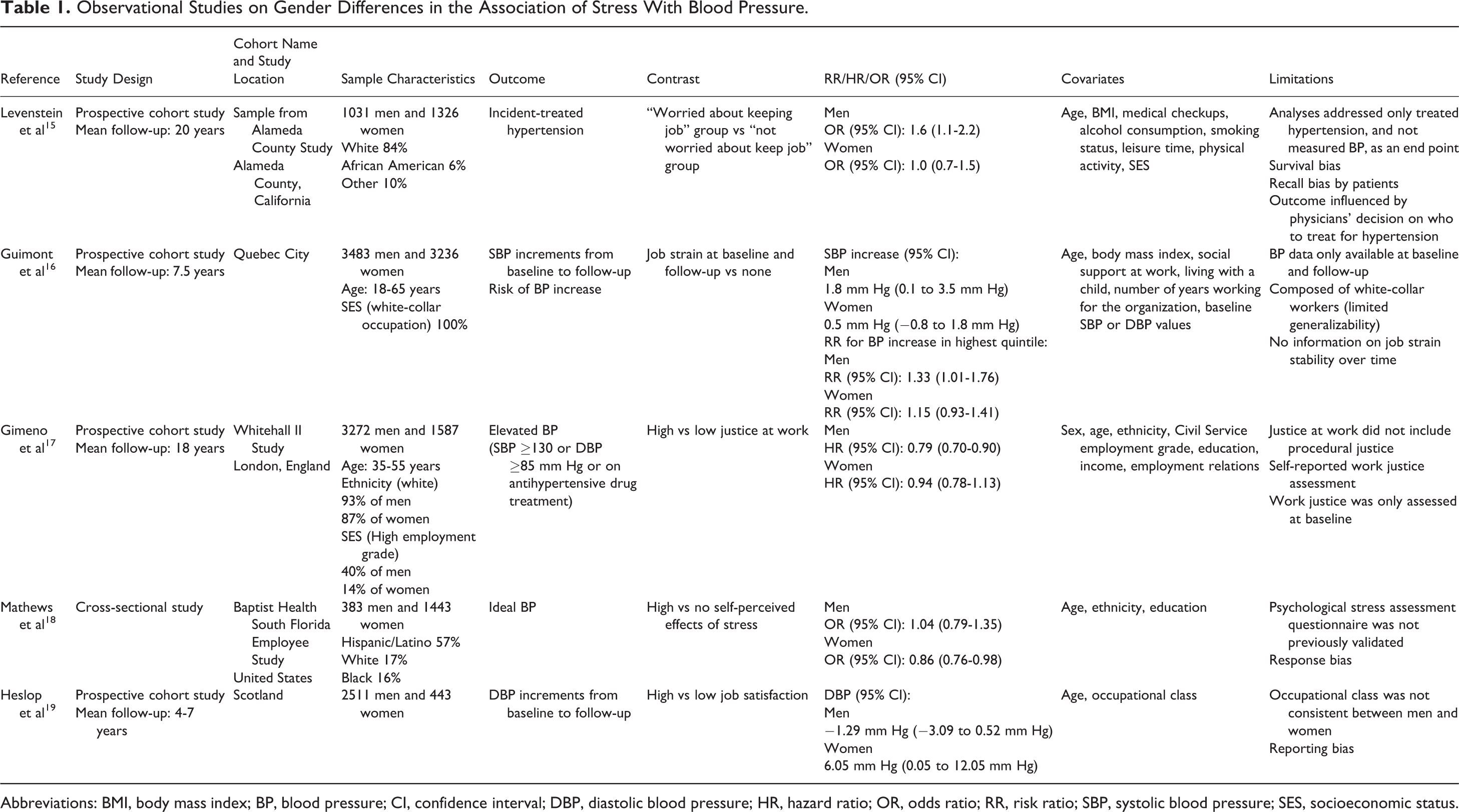
Abbreviations: BMI, body mass index; BP, blood pressure; CI, confidence interval; DBP, diastolic blood pressure; HR, hazard ratio; OR, odds ratio; RR, risk ratio; SBP, systolic blood pressure; SES, socioeconomic status.
Observational Studies on Gender Differences in the Association of Stress With Body Adiposity.
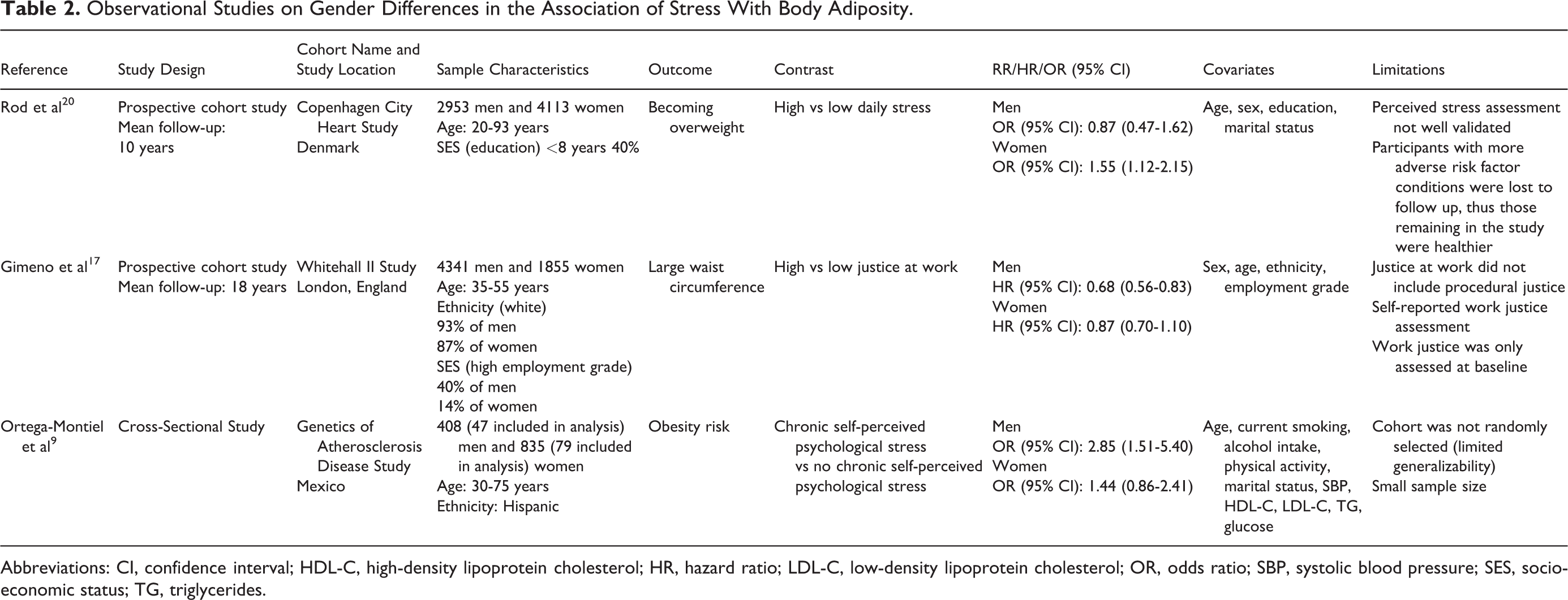
Abbreviations: CI, confidence interval; HDL-C, high-density lipoprotein cholesterol; HR, hazard ratio; LDL-C, low-density lipoprotein cholesterol; OR, odds ratio; SBP, systolic blood pressure; SES, socioeconomic status; TG, triglycerides.
Observational Studies on Gender Differences in the Association of Stress With Dyslipidemia.
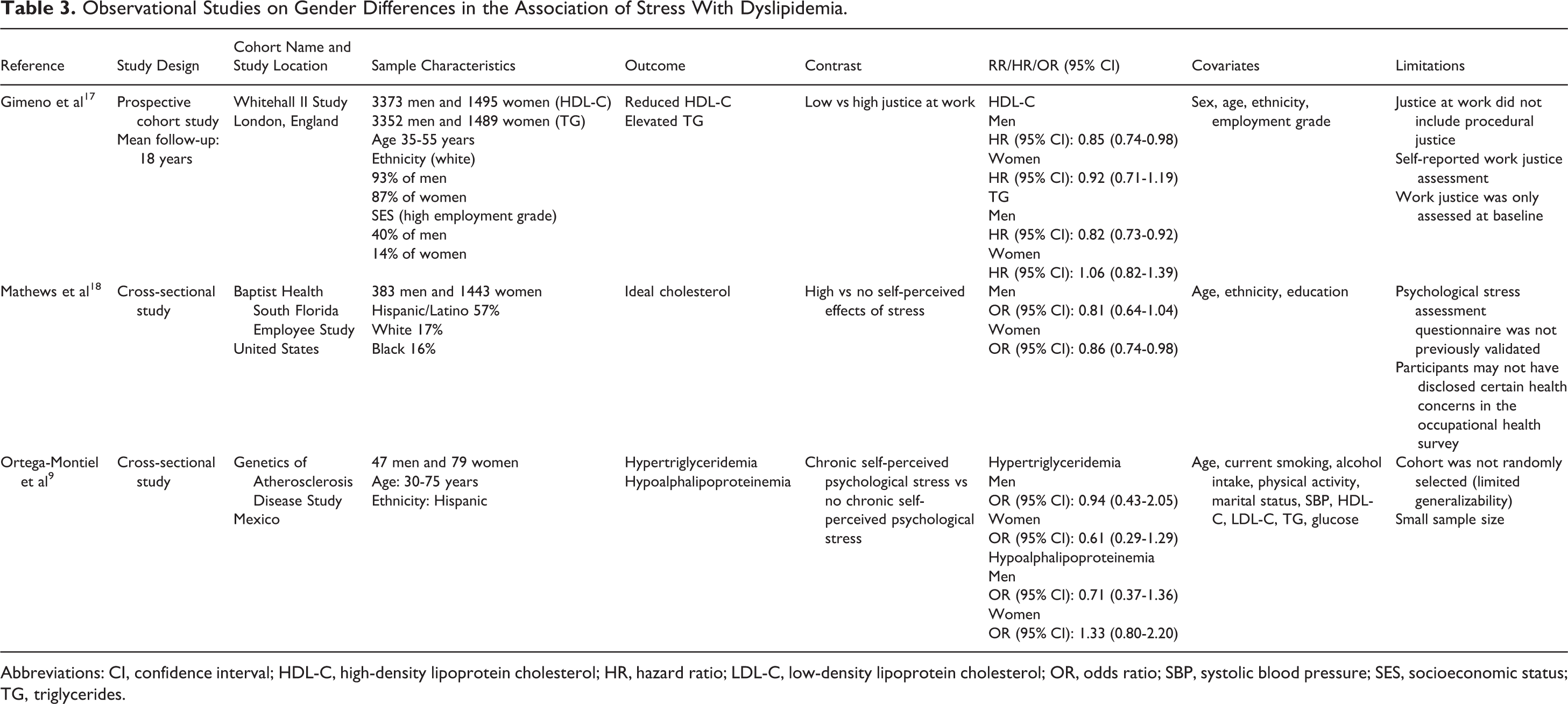
Abbreviations: CI, confidence interval; HDL-C, high-density lipoprotein cholesterol; HR, hazard ratio; LDL-C, low-density lipoprotein cholesterol; OR, odds ratio; SBP, systolic blood pressure; SES, socioeconomic status; TG, triglycerides.
Observational Studies on Gender Differences in the Association of Stress With Glycemic Regulation and Insulin Resistance.
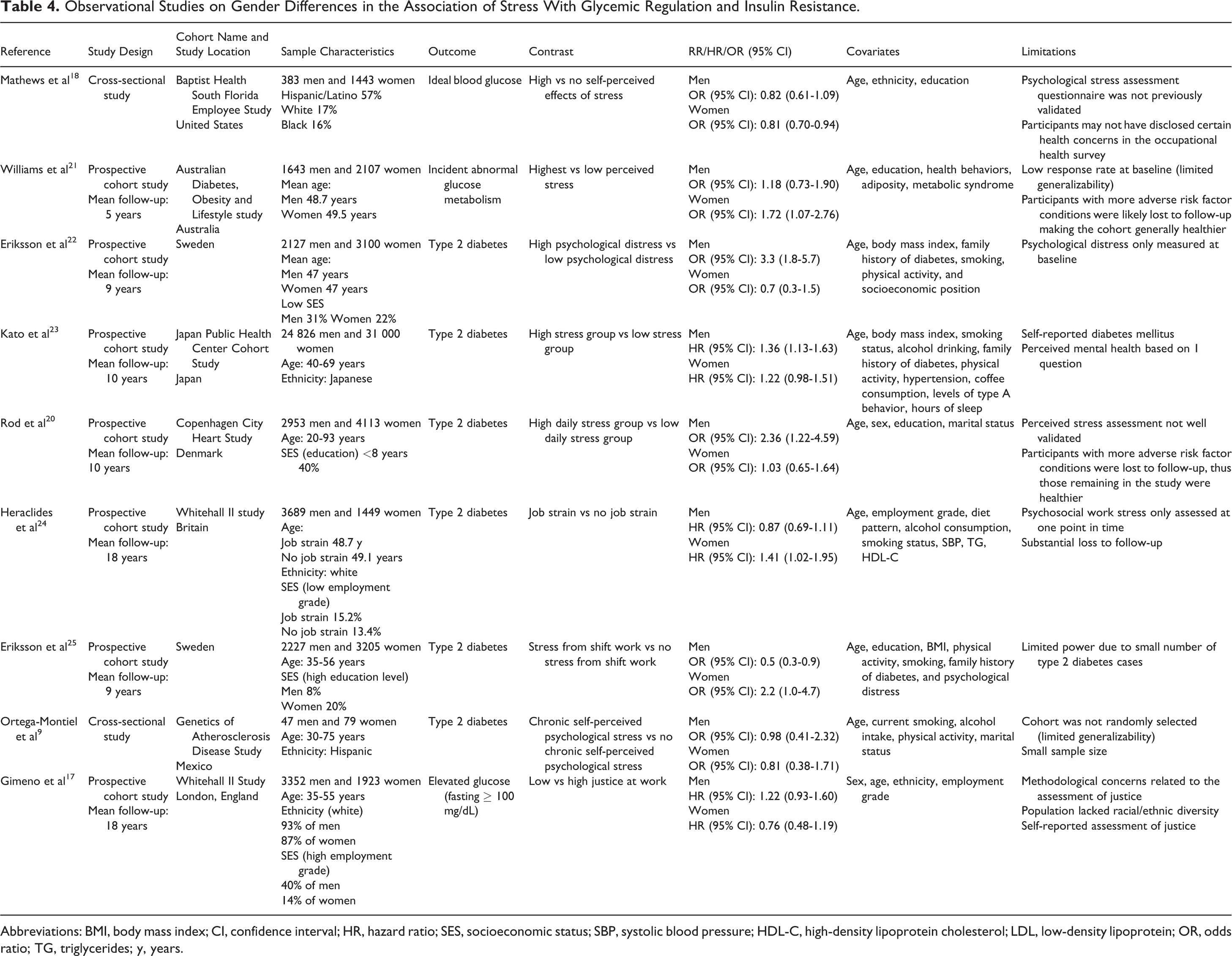
Abbreviations: BMI, body mass index; CI, confidence interval; HR, hazard ratio; SES, socioeconomic status; SBP, systolic blood pressure; HDL-C, high-density lipoprotein cholesterol; LDL, low-density lipoprotein; OR, odds ratio; TG, triglycerides; y, years.
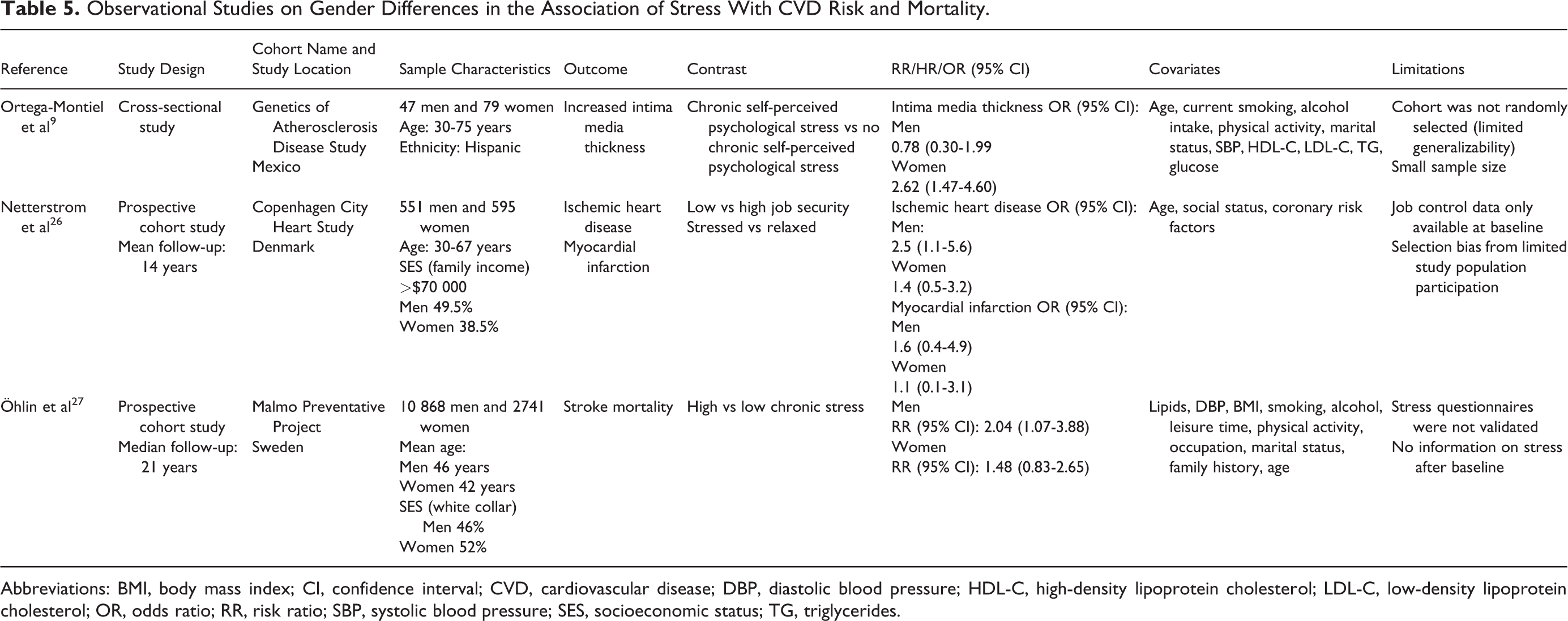
Observational Studies on Gender Differences in the Association of Stress With CVD Risk and Mortality.
Abbreviations: BMI, body mass index; CI, confidence interval; CVD, cardiovascular disease; DBP, diastolic blood pressure; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; OR, odds ratio; RR, risk ratio; SBP, systolic blood pressure; SES, socioeconomic status; TG, triglycerides.
Stress and Cardiometabolic Risk Factors
Stress and BP
Gender differences in the associations between stress and BP were noted in 5 studies, 15 -19 and although inconsistent, studies are generally indicative of stronger associations in men. A US prospective study of 1031 men and 1326 women who were followed for 20 years found that worrying about keeping a job was associated with 60% higher odds of developing hypertension in men (odds ratio, OR [95% confidence interval, CI]: 1.6 [1.1-2.2]) but not women (OR [95% CI]: 1.0 [0.7-1.5]). 15 Consistent with these findings, a Canadian prospective study of approximately 3483 men and 3236 women with white-collar jobs observed that job strain was modestly associated with an increase in BP over approximately 7.5 years in men (risk ratio, RR [95% CI]: 1.33 [1.01-1.76]) but not women (RR [95% CI]: 1.15 [0.93-1.41]). Further, the increase in BP from baseline to follow-up due to stress was significant and of higher magnitude in men (systolic BP [95% CI]: 1.8 mm Hg [0.1-3.5 mm Hg]) versus women (systolic BP [95% CI]: 0.5 mm Hg [−0.8 to 1.8 mm Hg]). 16 These findings were also corroborated in an analysis of 3272 men and 1587 women within The Whitehall II study, in which high justice at work, defined by feelings of value and fair treatment, was associated with 21% lower risk of elevated BP (systolic ≥130 or diastolic ≥85 mm Hg) among men (hazard ratio, HR [95% CI]: 0.79 [0.70-0.90]) but not women (HR [95% CI]: 0.94 [0.78-1.13]). 17
It is noteworthy that not all studies reporting gender differences in the relation between stress and BP showed stronger associations among men. For instance, in the Baptist Health South Florida (BHSF) Employee Study of 383 men and 1443 women, self-perceived psychological stress was associated with 14% lower odds of having ideal BP among women (OR [95% CI]: 0.86 [0.76-0.98]) but not men (OR [95% CI]: 1.04 [0.79-1.35]). 18 However, results may have been affected by the largely female versus male sample composition. Similarly, in a prospective European study of 2511 men and 443 women who were followed up for 4 to 7 years, low versus high job satisfaction at baseline and follow-up was associated with a significant increase in diastolic BP over time among women (OR [95% CI]: 6.05 mm Hg [0.05-12.05 mm Hg]) but not men (OR [95% CI]: −1.29 mm Hg [−3.09 to 0.52 mm Hg]). 19
Stress and Body Adiposity
Conflicting results were reported in studies evaluating the association between stress and body adiposity that stratified results by sex, as 2 studies 20,28 reported significant associations between psychological stress and environmental stress and body adiposity among women only, while 3 other studies 9,17,29 showed moderately significant results among men only. A cross-sectional analysis of the Copenhagen City Heart Study, following 2953 men and 4113 women for 10 years, found that self-reported perceived stress was associated with a 55% increased likelihood of becoming overweight in women (OR [95% CI]: 1.55 [1.12-2.15]) but not in men (OR [95% CI]: 0.87 [0.47-1.62]). 20 Similarly, in another study of 288 male and 102 female police officers, a 10-unit increase in job-related stress rating among female officers was associated with 37% higher odds of excess central adiposity (OR [95% CI]: 1.37 [1.04-1.81]), but null results were observed for men. 23 In contrast, a review of 3 longitudinal studies suggests a potentially stronger association between chronic stress and weight gain over time in men compared to women, 24 although additional long-term studies are needed to make definitive statements. In the Genetics of Atherosclerosis Disease Study of 408 men and 835 women, chronic self-perceived psychological stress was associated with ∼3-fold higher odds of obesity in men (OR [95% CI]: 2.85 [1.51-5.40]), but associations were not significant among women (OR [95% CI]: 1.44 [0.86-2.41]). 9 However, analysis of obesity only consisted of 47 men and 79 women. Consistent with these findings, in the Whitehall II study, which examined justice at work in relation to central adiposity, in 4341 men and 1855 women followed up for 18 years, high versus low justice at work was associated with 32% lower risk of having an at-risk waist circumference (men ≥40 inches; women ≥35 inches) in men (HR [95% CI]: 0.68 [0.56-0.83]) but not women (HR [95% CI]: 0.87 [0.70-1.10]). 17
Stress and Dyslipidemia
Evidence on the association of chronic stress with risk of dyslipidemia is mixed, with findings ranging from no evidence of gender differences (1 study), to stronger associations among men (1 study), and stronger associations among women (2 studies). 9,17,18,28 The cross-sectional analysis of 47 men and 79 women from the Genetics of Atherosclerosis Disease study noted that there was no association between chronic self-perceived level of stress and lipid in hypertriglyceridemia and hypoalphalipoproteinemia levels, in both sexes. 9 The Whitehall II study, however, showed that over 18 years of follow-up, high justice at work was associated with 15% lower odds of having reduced high-density lipoprotein cholesterol (HDL-C) levels (HR [95% CI]: 0.85 [0.74-0.98]) and 18% lower odds of having elevated triglycerides (HR [95% CI]: 0.82 [0.73-0.92]) in men but not in women. 17 In contrast, the BHSF Employee Study of 383 men and 1443 women found that women with higher levels of self-perceived stress had 14% lower odds of having ideal total cholesterol (<170 mg/dL) in accordance with the American Heart Association’s Life’s Simple 7 metrics (OR [95% CI]: 0.86 [0.74-0.98]), but findings were not significant among men (OR [95% CI]: 0.81 [0.64-1.04]). 18 Similar findings were observed among police officers, as every 10-unit increase in stress rating, assessed by a 60-item police stress survey, was associated with 33% higher odds of having reduced HDL-C (OR [95% CI]: 1.33 [1.06-1.69]) and 57% higher odds of having elevated triglycerides (OR [95% CI]: 1.57 [1.02-2.43]) in female officers. 28
Stress, Glycemic Regulation, and Insulin Resistance
Similar to the findings reported above, gender differences in the associations of stress with measures of glycemic regulation and insulin resistance were also inconsistent. In some studies, stress was associated with glycemic dysregulation in women only. 18,21 The BHSF Employee Study showed that stress was associated with 29% reduced odds of having an ideal blood glucose level in women (OR [95% CI]: 0.81 [0.70-0.94]) but not men (OR [95% CI]: 0.82 [0.61-1.09]). 18 Consistent with these findings, in a study of 3700 Australian men and women, high levels versus low levels of perceived stress were associated with 72% higher odds of developing incident abnormal glucose metabolism among women (OR [95% CI]: 1.72 [1.07-2.76]) but not men (OR [95% CI]: 1.18 [0.73-1.90]) after adjusting for sociodemographic factors and health status. 21
However, in other studies, associations between stress and glycemic regulation were stronger among men. 20,22,23 In the Copenhagen City Heart Study, men who experienced stress had >2-fold higher odds for developing diabetes over 10 years (OR [95% CI]: 2.36 [1.22-4.59]), but null results were observed among their female counterparts (OR [95% CI]: 1.03 [0.65-1.64]). 20 In another European study that examined psychological distress in relation to development of diabetes in 5000 Swedish men and women, high levels of psychological distress were associated with >3-fold increased risk of developing type 2 diabetes mellitus in men (OR [95% CI]: 3.3 [1.8-5.7]) but not women (OR [95% CI]: 0.7 [0.3-1.5]). 22 Similarly, in a Japanese prospective cohort of 55 286 participants, only men experiencing stress had a 36% higher risk of developing type 2 diabetes over the 10-year follow-up period (HR [95% CI]: 1.36 [1.13-1.63]), as null results were observed for women (HR [95% CI]: 1.22 [0.98-1.51]). 23
Interestingly, some studies of workplace stress in relation to risk of type 2 diabetes were indicative of protective associations in males. In the Whitehall II study, job strain versus no job strain was associated with 30% lower likelihood of developing diabetes among British men with a BMI under 30 (HR [95% CI]: 0.70 [0.53-0.93]). 24 However, among women with BMI >30, job strain was associated with 2-fold increased risk of diabetes (HR [95% CI]: 2.01 [1.06-3.92]). 24 These findings are suggestive of a potential interaction between sex and weight status, as the association of job-related stress with risk of type 2 diabetes varied by BMI category among men and women in this study. Another prospective European study of 5432 middle-aged Swedish men and women followed for 8 to 10 years, also showed that job strain was associated with 50% reduced odds of developing type 2 diabetes among men (OR [95% CI]: 0.5 [0.3-0.9]). However, in that study, a borderline significant 2-fold increase in odds of type 2 diabetes was observed in women with high job strain (OR [95% CI]: 2.2 [1.0-4.7]). 25 In fact, among women, job strain in combination with low decision latitude, representative of one’s personal control over decisions at work, were associated with >4-fold higher odds of diabetes (OR [(95% CI]: 4.2 [2.0-8.7]). 22 This study suggests that differential associations may exist in the associations of stress with type 2 diabetes and that work-related stress in combination with adverse psychosocial risk factors may be particularly detrimental for risk of type 2 diabetes among women.
Not all studies demonstrated significant results or gender differences in the associations between stress and glycemic regulation. A cross-sectional analysis of the Genetics of Atherosclerosis Disease Study did not find any significant associations between chronic perceived psychological stress and diabetes mellitus in men (OR [95% CI]: 0.98 [0.41-2.32]) or women (OR [95% CI]: 0.81 [0.38-1.71]). 9 The lack of an association between stress and glycemic regulation was also reported in 2 prospective studies. 17,30 In an analysis of the Whitehall II Study, null results were observed for low justice at work in relation to having elevated glucose in both men (HR [95% CI]: 1.22 [0.93-1.60]) and women (HR [95% CI]: 0.76 [0.48-1.19]). 17
Stress and Behavioral Risk Factors of CVD
Stress and Diet
Stress may alter cardiovascular risk via its influence on modifiable lifestyle behaviors, including diet, though evidence on these associations is limited and has focused on specific diet components versus overall diet quantity and quality. In the cross-sectional analysis of the Copenhagen City Heart Study, stress was associated with 57% lower odds of limiting drinking alcohol to the sensible drinking limit in Denmark (14 drinks/week in women and 21 drinks/week in men; OR [95% CI]: 0.43 [0.24-0.79]). 20 Chronic stress has also been linked to a greater intake of energy and nutrient-dense foods, mainly sources of sugar and fat, and to poor diet quality. 29 In the Hispanic Community Health Study/Study of Latinos (HCHS/SOL) Socio-Cultural Ancillary Study of 5077 US Hispanic/Latino adults, increased chronic stressors (B [95% CI]: 83.5 [28.9-138.2]) and greater perceived stress (B [95% CI]: 109.2 [59.0-159.4]) were associated with higher daily total caloric intake. 31 Additionally, greater perceived stress was associated with lower diet quality, assessed by the alternative healthy eating index (HEI) 2010 (B [95% CI]: −0.61 [−1.18 to −0.03]). 31 Similar findings were observed in a cross-sectional study of 151 US men and women, in which individuals with higher early life adversity (ELA) or post-traumatic stress disorder (PTSD) severity had poorer diet quality as evidenced by their lower Dietary Approaches to Stop Hypertension and HEI scores (P < .01). 32 Individuals with higher ELA severity also had a greater consumption of trans-fatty acids (P = .003). 32 However, these studies did not stratify by gender.
In a study of 87 men and 176 women, those reporting high versus low stress from caregiving responsibilities had a higher percentage of saturated fat intake (11.5% vs 10.5%, P = .04). 33 Only 1 US study, the BHSF Employee Study of 383 men and 1443 women, evaluated sex differences in the associations between stress and diet quality. Findings showed that stress is associated with 35% reduced odds of adhering to an ideal diet based on servings sizes of fruits/vegetables, whole grains, protein, salt, and sugary drinks among women (OR [95% CI]: 0.65 [0.47-0.89]) but not men (OR [95% CI]: 1.12 [0.69-2.10]). 18 This finding suggests that the influence of stress on diet quality may be more pronounced among women but warrant confirmation in future studies given the limited literature on gender differences in these associations.
Stress and Physical Activity and Sedentary Behaviors
Physical activity and sedentary behaviors represent another mechanism through which stress may influence cardiovascular risk. Inconsistent findings from studies examining the relation between stress and engagement in activity and sedentary behaviors were reported with results ranging from similar associations in both sexes in some studies to potentially stronger associations among men or among female caregivers in other studies. In the BHSF Employee Study, stress was associated with 47% and 43% lower likelihood of having an ideal physical activity level, defined as at least 30 minutes of moderate activity for ≥5 days per week, in accordance with the American Heart Association’s Life’s Simple 7 metrics, in both men (OR [95% CI]: 0.53 [0.41-0.68]) and women (OR [95% CI]: 0.57 [0.50-0.65]), respectively. 18
In contrast, 2 European studies 34,35 and 1 US study 36 reported stronger associations between stress and physical activity among men. Higher levels of self-reported perceived stress were associated with lower levels of recreational exercise in men only (B = −0.20, P < .001) in a cross-sectional study of 6832 Scottish individuals. 34 Similarly, a study of 7169 Swedish individuals found that a higher level of self-reported daily stressors was associated with 2-fold higher odds of having low self-reported leisure time physical activity in men (OR [95% CI]: 2.0 [1.6-2.4]) but not women (OR [95% CI]: 1.1 [0.9-1.4]). 35 In the United States, the cross-sectional 1990 National Health Interview Survey of 12 919 older men and women demonstrated that men with low levels of perceived stress had 70% greater odds of engaging in regular physical activity, defined as ≥3 times per week of at least 30 minutes (OR [95% CI]: 1.7 [1.2-2.4]), but results were not significant among women (OR [95% CI]: 1.3 [1.0-1.6]). 36
Stress and Sleep
Differential associations between stress and sleep have been observed in men and women. In a study of 73 college-aged adults, gender-specific stress reactivity, assessed by cortisol response to sleep quality dysfunction, was observed in both sexes but greater dysfunction was reported among men. 37 Similarly, in a cross-sectional study of 8770 Japanese men and women, high occupational stress was significantly associated with ∼2-fold higher odds for insomnia in both men (OR [95% CI]: 2.45 [2.12-2.83]) and women (OR [95% CI]: 1.83 [1.39-2.41]). 38 However, increased occupational stress was associated with 38% higher odds of having short sleep duration in men (OR [95% CI]: 1.38 [1.13-1.68]) but not women (OR [95% CI]: 1.30 [0.95-1.78]). 38 Nevertheless, the Study of Women’s Health Across the Nation Sleep Study, a US prospective study of 330 women, demonstrated that high chronic stress was associated with lower sleep quality (P < .001), increased insomnia (P < .001), and increased polysomnography-assessed wake after sleep onset (P < .01). 39 It is important to note that the association between sleep as well as other lifestyle behaviors and stress may be bidirectional and that observed gender differences in the influence of sleep on cardiovascular risk could alternatively be mediated by stress. 40
Stress in Relation to CVD Risk
Associations between stress and CVD incidence have been documented in a number of studies, but most studies focused on psychological trauma and PTSD as exposures rather than the influence of chronic but perhaps less severe stressors. 6 Among the population-based studies that evaluated the influence of chronic stress on CVD risk, the BHSF Employee Study showed that self-perceived psychological stressors were associated with 42% reduced odds of having adequate cardiovascular health, measured by the American Heart Association’s Life’s Simple 7, in the overall sample (OR [95% CI]: 0.58 [0.50-0.66]). 18 Similarly, the US prospective REasons for Geographic And Racial Differences in Stroke study of 24 443 participants also observed that high perceived stress was associated with a high risk of CHD for those individuals of a low-income (HR [95% CI]: 1.36 [1.04-1.78]). 41 However, these studies did not report estimates stratified by sex. Another cohort study demonstrated associations between stress and CVD risk in both sexes. In the study of health in Pomerania that included 1112 women and 1052 men, high psychological strain was associated with 55% and 38% higher odds of having carotid plaques in both women (OR [95% CI]: 1.55 [1.10-2.18]) and men (OR [95% CI]: 1.38 [1.12-1.75]), respectively. 42
Gender differences in the associations between stress and CVD risk may also vary by the type of stress. In the Copenhagen City Heart Study, job insecurity was associated with >2-fold higher odds of ischemic heart disease (OR [95% CI]: 2.5 [1.1-5.6]) and myocardial infarction (OR [95% CI]: 2.7 [1.2-6.1]) in men only, 26 suggesting that job-related stress may have a more pronounced influence on CVD risk in men. Similarly, the INTERHEART study of 24 767 individuals in 52 countries noted that permanent versus no work stress was associated with an ∼2-fold higher odds of acute myocardial infarction in men (OR [99% CI]: 2.34 [1.86-2.93]) but not in women (OR [99% CI]: 1.11 [0.60-2.06]). 43 However, chronic stress may be more strongly associated with CVD risk in women. In the Genetics of Atherosclerosis Disease Study, chronic self-perceived stress was associated with >2-fold greater odds of having high intima media thickness in women (OR [95% CI]: 2.62 [1.47-4.60]) but not men (OR [95% CI]: 0.78 [0.30-1.99]). 9 Chronic self-perceived stress was also associated with >2-fold greater odds of carotid atherosclerosis in women (OR [95% CI]: 2.26 [1.47-4.67]). 9 Similarly, the Stockholm Female Coronary Risk Study, a prospective study of 292 Swedish females found that marital stress was associated with ∼3-fold greater risks for recurrent CHD events (HR [95% CI]: 2.92 [1.30-6.54]). 44 A cross-sectional US study of 686 individuals found the odds for myocardial ischemia due to acute emotional stress exposure, assessed using mental stress testing, were more than doubled in women compared to men for each 10-year decrement in age (OR [95% CI]: 2.06 [1.12-3.79]). 45
Stress in Relation to CVD Mortality
Although most studies that investigated the role of stress in CVD mortality did not stratify by gender, evidence thus far is suggestive of potentially stronger associations in men. In US and European studies, job strain and perceived stress have been associated with greater mortality. 41,46 Among studies that stratified by sex, the Copenhagen City Heart Study did not report a significant association between stress and death from ischemic heart disease in both men (OR [95% CI]: 1.6 [0.4-4.9]) and women (OR [95% CI]: 1.1 [0.1-3.1]). 26 In contrast, the Malmo Preventative Project of 13 600 middle-aged Swedish participants followed up for ∼21 years demonstrated that men reporting chronic stress had >2-fold greater risk of fatal stroke (RR [95% CI]: 2.04 [1.07-3.88]), but no significant associations were observed among women (RR [95% CI]: 1.48 [0.83-2.65]). 27 Associations between stress and CVD mortality in men were also observed in the Multiple Risk Factor Intervention Trial. In that study of 12 236 men, chronic work stress increased the risk of cardiovascular mortality by 26% over a 9-year follow-up period (RR [95% CI]: 1.26 [1.07-1.48]). 47
Conclusion
In conclusion, differential associations between stress in relation to CVD risk factors and end points have been demonstrated in both men and women. In general, men may be more vulnerable to the influence of stress on body adiposity, BP, and CVD mortality. However, women may be more vulnerable to the potential influence of stress on measures of glucose regulation, dyslipidemia, and CVD risk. Evidence on stress in relation to behavioral risk factors for CVD is notably scarce, yet it appears that the influence of stress on sleep and engagement in physical activity may be stronger among men, and associations between stress and diet appear to be stronger among women.
Stress may alter CVD risk through a number of plausible biological mechanisms, beyond its influence on behavioral risk factors of CVD. Evidence from the Multi-Ethnic Study of Atherosclerosis is suggestive that pathogen burden and heightened immune response may be a potential biological pathway between chronic stress and increased CVD risk. 48 Chronic stress may result in maladaptive immune, endocrine, and metabolic responses that could affect CVD risk. 49 Few studies have explored the biological pathways that may account for gender differences in the influence of stress on cardiovascular risk factors. It has been proposed that elevated cortisol from stress via the HPA axis contributes to the activation of adipose tissue and accumulation abdominal fat 50 and that stress-induced cortisol release is greater in men 51 than in women. 52 Despite the proposed biological pathways, the mechanisms underlying the observed gender differences in associations of stress with cardiovascular risk are still not fully elucidated and warrant further investigation.
Given that gender disparities in the prevalence of overall and different types of stress exist, future studies should decipher the potential differential associations between total and types of stress in relation to cardiovascular risk among men and women to identify vulnerable populations and develop targeted interventions. It is notable that much of the evidence on stress in relation to cardiovascular behavioral and clinical risk factors has relied on a single measure of stress at baseline. Therefore, prospective studies with repeated measures of psychological stress, behavioral and biological factors, and cardiovascular outcomes or surrogate markers of CVD are needed to disentangle these complex relationships and establish the pathways linking stress and CVD. Finally, randomized controlled trials seeking to reduce CVD risk via stress management should incorporate sex-stratified analyses and may inform the development of gender-specific stress reduction interventions for CVD prevention.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by an American Heart Association Go Red for Women Strategically Focused Research Network Award to Dr Aggarwal (Grant # 16SFRN27960011), an AHA Soter Collaborative Award to Dr Makarem (Grant # 16SFRN27880000-1), and an R01 Award to Dr Shimbo (Grant #HL137818).