
Abstract
In Europe as well as the United States, nonalcoholic fatty liver disease (NAFLD) is the most common cause of chronic liver disease and is strongly associated with obesity and type 2 diabetes mellitus (T2DM). Nonalcoholic fatty liver disease is defined as a hepatic manifestation of the metabolic syndrome. Being a very powerful and independent cardiovascular risk factor, NAFLD increases cardiovascular and overall mortality to a significant degree. The purpose of this review was to determine sex- and gender-specific differences in the prevalence and pathogenesis of NAFLD and delineate the specific characteristics of NAFLD as a systemic disease in men and women. Postmenopausal women and women with endocrine disorders such as the polycystic ovarian syndrome are at high risk of developing NAFLD. The increasing incidence of female NAFLD after menopause appears to be related to reduced estrogen and increased testosterone levels, as well as changes in the distribution of fatty tissue. Finally, the role of gender-specific nutrition patterns in the pathogenesis of NAFLD will be discussed. Fructose consumption from industrialized products is a promoter of NAFLD, depending on the total daily calorie intake of macronutrients. A higher level of health literacy and conscious food behavior have been noted among women of all age groups compared to males, which could play a role in the pathogenesis of NAFLD. Health professionals are confronted with the challenges of early diagnosis by the use of sensitive, reliable, and noninvasive diagnostic tools, including screening algorithms for high-risk persons and providing gender-specific nutritional support as a crucial element of treatment and disease prevention.
Keywords
Introduction
Nonalcoholic fatty liver disease (NAFLD) is the cause of 75% of all chronic liver diseases and is strongly linked to obesity and type 2 diabetes mellitus (T2DM). 1 Nonalcoholic fatty liver disease is defined as a hepatic manifestation of the metabolic syndrome and is correlated with high overall mortality and cardiovascular mortality rates. 2,3 In epidemiological studies, the prevalence of NAFLD is reported to range between 2% and 44% in the European population, while the prevalence rates of 70% have been noted in persons with T2DM. 2 The term NAFLD encompasses a wide spectrum of diseases of various severities, ranging from hepatic steatosis to steatohepatitis and subsequent fibrosis and cirrhosis with end-stage liver damage. Nonalcoholic fatty liver disease is defined as a condition in which macroscopic steatosis is noted in more than 5% of hepatocytes by light microscopy, in the absence of other etiologies of liver disease. 3 The appearance of the disease is very heterogeneous. Guidelines recommend ultrasound investigation and the measurement of transaminases as the preliminary steps of noninvasive diagnostic examination. 3
Early diagnosis is essential because NAFLD with or without steatohepatitis was found to create a predisposition for hepatocellular carcinoma in the absence of cirrhosis and advanced fibrosis. 4 Proton magnetic resonance spectroscopy or diagnostic procedures such as liver biopsy are expensive or invasive and cannot be recommended in routine clinical practice. 3 However, ultrasonography and serum biomarkers have their diagnostic limitations. Ultrasound is able to identify steatosis when the fat content of the liver exceeds 33%, depending on the quality of the examination. 5,6 Seventy percent of persons with NAFLD were reported to have normal levels of alanine aminotransferase (ALT) and aspartate aminotransferase (AST). 5,6
Fifty percent of persons with T2DM have NAFLD despite normal ALT levels. 7 These facts may explain the diversity of prevalence figures in epidemiological studies. The aim of this review is to delineate sex- and gender-specific differences in NAFLD while focusing on its prevalence and pathogenesis and establish whether female dietary patterns play a key role in the development of the disease.
Methods
We performed an electronic research with the keywords “epidemiology and pathogenesis of NAFLD,” “NAFLD and women,” “fructose and NAFLD,” “female dietary patterns,” AND “gender aspects of nutrition” in the PubMed, Google Scholar, and Cochrane library databases. The results were selected and identified by their title, relevance, and abstracts. Other sources cited in the articles were manually selected from the reference lists. The literature research was based on full texts in the English or German language. A small number of prospective trials have been focused on the pathogenesis of female NAFLD and nutrition. A follow-up period of 16 years was noted in some surveys and cohort studies identified by manual search. The majority of the 84 selected sources are reviews and meta-analyses.
Results
Sex- and Gender-Specific Differences in Prevalence and Pathogenesis
Nonalcoholic fatty liver disease is primarily a male disease. Men below the age of 60 years are more frequently affected with NAFLD than women of the same age, but a rising incidence has been noted among postmenopausal women and women with polycystic ovarian syndrome (PCOS). 8
Polycystic ovarian syndrome is linked with hyperandrogenism and a higher risk of T2DM due to insulin resistance. 5,8,9 The prevalence of NAFLD among women with PCOS has been reported to range between 15% and 55%. 5 The alteration in sex hormone levels, specifically reduced estrogens and increased androgens during and after menopause, is an important factor in the emergence of NAFLD. Data show a prevalence of 23% among postmenopausal women compared to 7% among premenopausal women. In men between the ages of 30 and 60 years, NAFLD occurs at a rate of 27%, with no age-related changes. 8 Regarding the prevalence of nonalcoholic steatohepatitis (NASH), men are younger but more women than men older than 50 years develop NASH. 8
Ethnic Differences in NAFLD
Ethnicity plays an important role in the worldwide prevalence of NAFLD. The risk of NAFLD is especially high among Hispanics and Asians (odds ratio [OR]: 1.72; 95% confidence interval [CI]: 1.28-2.33), compared to African Americans; a significantly lower risk has been noted in the latter group (OR: 0.52; 95%CI: 0.34-0.78). 10,11 However, obese African American individuals have a lower rate of NAFLD, NASH, and liver fibrosis than non-Hispanics and Hispanics. 12 According to US population-based studies, the highest prevalence of NAFLD has been observed in Hispanics and the lowest prevalence in non-Hispanic blacks. 12 These racial and ethnic differences may be based on environmental, behavioral, and genetic factors. However, the genetic variation of Patatin-like phospholipase domain-containing protein 3 (PNPLA3) is regarded as a trigger for liver fat accumulation and susceptibility to disease progression. 12 Furthermore, ethnic differences have also been noted in the distribution of obesity, especially among women. The quantity of abdominal fat is greater among Hispanic women than white women; this may explain the different prevalence rates in the various ethnic groups. 12
Lipid Metabolism
The pathogenesis of NAFLD is associated with a disorder of hepatokines and hormones controlling glucose metabolism, which increases gluconeogenesis and inhibits the effects of insulin. 13 Insulin resistance causes an increased lipolysis in the adipose tissue. Fatty acid fluxes from the adipose tissues lead to an accumulation of fatty acyl coenzyme A in the liver. The increased concentrations of fatty acids are used in intrahepatic de novo lipogenesis. Acyl coenzyme A is metabolized through different enzymatic steps to diacylglycerol, which plays a crucial role in insulin resistance and increases the production of inflammatory hepatokines. 13 Diacylglycerol can be hydrolyzed to glycerol by releasing fatty acids; glycerol serves as a substrate for gluconeogenesis. 13
In addition to insulin resistance, a variety of adipokines are involved in lipid metabolism and the pathogenesis of NAFLD. 5 Data suggest that NASH and the severity of fibrosis are correlated with elevated leptin levels, whereas low adiponectin levels are found in the presence of NAFLD, dyslipidemia, and T2DM. 5
Endocrine Aspects of Disease—Differences Between Male and Female NAFLD
The male form of NAFLD is associated with higher levels of ALT, lower adiponectin, and lower leptin levels, as well as thicker visceral fatty tissue compared to that in women. 14 -17
Moreover, Feitosa et al suggested that elevated ALT levels may serve as a surrogate parameter of coronary heart disease among males. 18,19 Testosterone plays a key role in insulin sensitivity and lipid metabolism. Low levels of testosterone and sex hormone–binding globulin are predictors of metabolic syndrome among men and are linked with a greater accumulation of visceral fatty tissue. 5
Changes in the distribution of fat with increasing visceral adiposity are correlated with postmenopausal status and are triggered by estrogen deficiency and a relative excess of androgens. 14 Polycystic ovarian syndrome is characterized by hyperandrogenism, lower adiponectin levels, estrogen deficiency, insulin resistance, dyslipidemia, and higher cardiovascular risk.
In a prospective trial, Cerda et al reported NAFLD in 41.5% of postmenopausal women with PCOS compared to 19.4% in the control group matched by age and body mass index (BMI). 9 Elevated ALT levels were noted in 50% of women with PCOS. 9 Obese women with PCOS have a higher risk of NAFLD than normal-weight women with PCOS. Feitosa et al mention that female NAFLD is frequently associated with normal ALT levels. 19 The potential protective effect of hormone replacement therapy (HRT) is controversially discussed; the existing body of data in this regard is weak. In a cross-sectional study, Yang et al noted a lower risk of NAFLD in postmenopausal women taking HRT compared to those without HRT. 20
Cardiovascular Risk
Recently, Liu et al reported the occurrence of cardiovascular disease among individuals with NAFLD. 18 Nonalcoholic fatty liver disease is strongly correlated with elements of the metabolic syndrome, especially T2DM and dyslipidemia. 18
Nonalcoholic fatty liver disease is associated with the early onset of endothelial dysfunction in patients without overt atherosclerosis. Besides, atrial fibrillation is more common among persons with NAFLD, regardless of other cardiovascular risk factors. 18,21
Fan et al included 11 studies in a meta-analysis to evaluate the extent of endothelial dysfunction in persons with NAFLD. Endothelial function was measured by brachial artery flow–mediated dilation and nitrate-induced dilatation techniques. The results showed a reduction in brachial artery flow-mediated dilatation, with a mean difference of −4.82% (95% CI: −5.63 to −4) among those with NAFLD. 22
Endothelial dysfunction was correlated with the degree of liver disease. It was more severe among persons with NASH compared to persons with simple steatosis. 22 No data have been provided about sex-related differences in endothelial dysfunction among females and males with NAFLD.
Oxidative stress and inflammation are major triggers for the development of NAFLD, combined with the production of pro-inflammatory cytokines such as tumor necrosis factor α (TNF-α), interleukin (IL) 6, C-reactive protein (CRP), and IL-8. 18 This implies the presence of atherogenic factors and may be the crucial link between NAFLD and cardiovascular morbidity. 18
The correlation between NAFLD and subclinical atherosclerosis was investigated in the Multi-Ethnic Study of Atherosclerosis cohort study. The study population consisted of 3976 men and women between the ages of 45 and 84 years. Cardiac computed tomography was used to measure coronary artery calcium; subclinical atherosclerosis was defined as a coronary artery calcium score >0. 23
Individuals with NAFLD more frequently had CRP levels >2 mg/L (OR: 2.22; 95% CI: 1.85-2.67), and the prevalence of subclinical atherosclerosis was higher in the NAFLD group than in controls (54% vs 50%). 23
Independent of other aspects of the metabolic syndrome, a significant association was noted between NAFLD and subclinical atherosclerosis (OR: 1.37, 95% CI: 1.11-1.68). With regard to sex-specific differences, the authors noted a stronger correlation and elevated markers of inflammation in women with NAFLD compared with men. 23
Current data show that NAFLD is associated with a higher risk of congestive heart failure due to a disruption of myocardial metabolism. Higher levels of intrahepatic fat are correlated with higher myocardial fat content and cardiac steatosis, which is a strong predictor of left ventricular diastolic dysfunction. 24 Recently, it was reported that patients with NAFLD have early changes in myocardial substrate metabolism, especially impaired high-energy phosphate metabolism and increased insulin resistance, leading to left ventricular dysfunction and hypertrophy. Both are strongly linked with a high risk of congestive heart failure. 24
Pro-inflammatory cytokines from adipose tissue may be the crucial link between NAFLD and extrahepatic comorbidity. Chronic kidney disease (CKD) has been noted among 20% to 55% of persons with NAFLD, compared to 5% to 35% among those without NAFLD. 24,25
Nonalcoholic fatty liver disease and CKD share a number of important cardiometabolic risk factors and common pathophysiological mechanisms and both are correlated with a higher risk of cardiovascular events. The possible molecular mediators linking NAFLD and CKD may rely on the release of pro-inflammatory cytokines, as well as CRP, TNF-α, and plasminogen activator inhibitor 1 from the steatotic liver. 24
Recent studies mention reduced levels of adiponectin as the main connection between the pathophysiological pathways of the liver and the kidney. 24 Lower adiponectin levels reduce the activation of the energy sensor 5′-Adenosine monophosphate (AMP)-activated protein kinase which enhances inflammatory and profibrotic processes, leading to end-organ damage. 24
Hepatic and peripheral insulin resistance play a key role in the pathogenesis of metabolic syndrome and NAFLD. Nonalcoholic fatty liver disease may be defined as the precursor of the metabolic syndrome. 26
Sex and Gender Aspects of Nutrition
Nutrition obviously plays a key role in the worldwide epidemic of obesity and obesity-related morbidities such as T2DM and NAFLD. The excessive intake of calories combined with poor physical activity may be responsible for the accumulation of intrahepatic fat and hepatotoxicity. 27 Persons with NAFLD were reported to have typical dietary patterns marked by a greater consumption of saturated fat and cholesterol and low intake of dietary fiber. 28 The consumption of fructose is associated with the rising prevalence of NAFLD, obesity, and T2DM. 29 A diet rich in fructose reduces sensitivity to hepatic insulin, may influence the central nervous system, and is correlated with increased energy consumption and weight gain. 29 -32 However, the role of fructose consumption and its metabolic effects on the pathogenesis of NAFLD are controversially discussed. Vos and Lavine concluded in their review that persons with NAFLD had higher levels of triglycerides after the intake of fructose than healthy individuals without NAFLD. 33 Furthermore, the influence of fructose consumption on lipid metabolism differs between men and women. Data suggest that premenopausal women have lower triglyceride levels after fructose intake compared with men. 34 Eight nutrition trials were included in this review, which was conducted to determine whether female dietary patterns play a role in the pathogenesis of female NAFLD (Table 1).
Comparison of the Nutrition Study Trials.
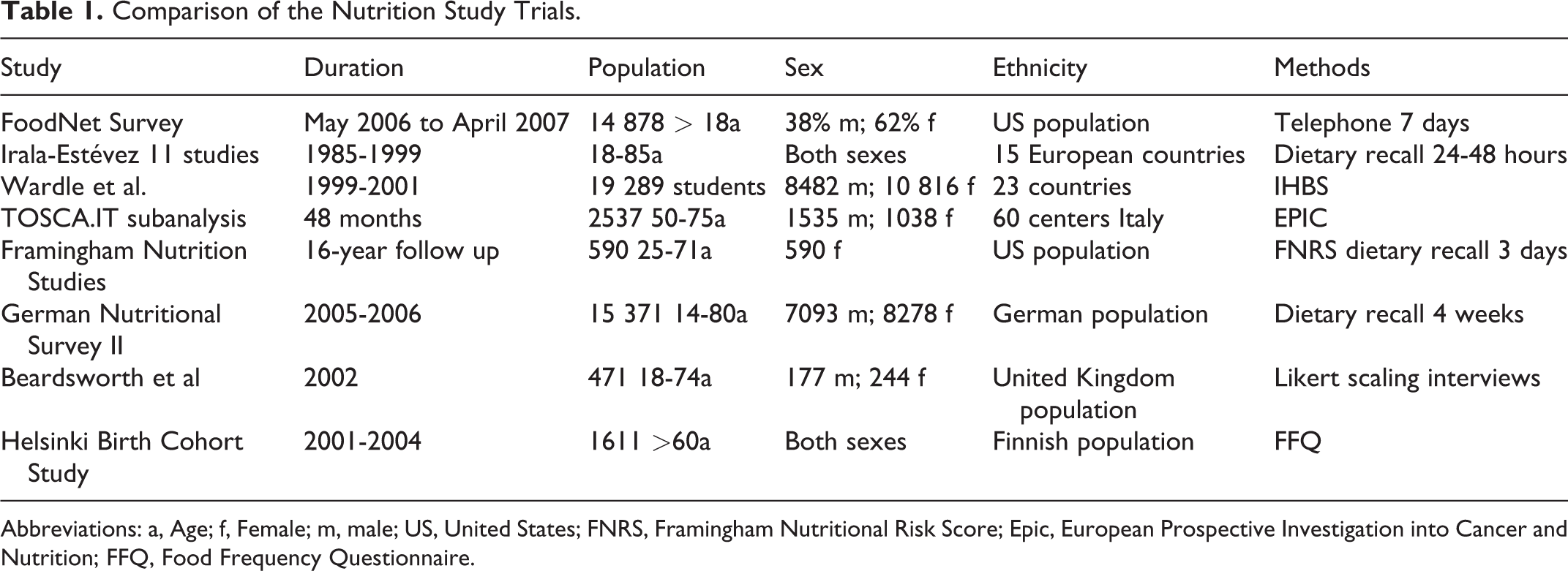
Abbreviations: a, Age; f, Female; m, male; US, United States; FNRS, Framingham Nutritional Risk Score; Epic, European Prospective Investigation into Cancer and Nutrition; FFQ, Food Frequency Questionnaire.
The US The Foodborne Diseases Active Surveillance Network (FoodNet) survey comprised 14 878 persons aged older than 18 years and reported a higher consumption of fruit and vegetables among women but a lower consumption of meat and high-risk food. 35
Irala-Estévez et al addressed the consumption of fruit and vegetables in European countries and suggested a positive correlation between the level of education and the intake of fruit and vegetables. Similar to the US survey, women tended to consume more fruit and vegetables than men. 36
Wardle et al mention that boys and men consume more soft drinks and less fruit and vegetables than women. Health protective behavior is regarded as a female phenomenon, whereas health risk behavior is attributed to a masculine attitude. 37 Women were reported to consume high-fat foods and salt in lesser quantities. 37
The TOSCA.IT study examined food behavior among persons with T2DM and their effect on lipid metabolism; the authors reported that fewer women than men achieved the therapy target for low-density lipoprotein (LDL), but female HbA1C values were slightly lower than those of males. 38 Females reported a higher consumption of added sugar; 2.8% of women and 2.75% of men exceeded the recommended daily added sugar intake, while men had a preference for starchy foods. 38
The British survey included in the review comprised 477 individuals. In conformity with other surveys, it was found that women consumed more fruit and vegetables whereas men had a preference for fried foods and processed meat. No gender differences were noted in the consumption of chocolate and starchy foods. 39 The Framingham Nutrition Study was an investigation conducted after the so-called Framingham Offspring and Spouse Study comprising 560 women, and it suggests that poor food quality is associated with obesity. 40
The German National Nutrition Survey II comprising 15 371 participants between the ages of 14 and 80 years reports a higher consumption of meat and meat products among men of all age groups as well as a higher intake of sweets, ice cream, sweeteners, soft drinks, and alcoholic beverages among men. 41 Women between the ages of 14 and 50 years reported a lower intake of milk, dairy products, and cheese. 41
Summarizing the abovementioned trials and nutrition surveys, it may be concluded that women of all age groups tend to opt for more healthy food. Gender differences in eating behavior emerge during adolescence: girls aged 12 to 17 years give more attention to food choices than boys of the same age (62.5% vs 55.9%). 42
The association of dietary patterns and NAFLD was examined in the Israeli National Health and Nutrition Survey, which comprised 375 persons of both sexes. Individuals with NAFLD had a 2-fold higher consumption of high-carbohydrate and sweet foods than those without NAFLD. The NAFLD group consumed 27% more meat protein from all types of meat, but there was no difference between other categories of protein intake. 31 The results suggest that a higher intake of soft drinks and meat was associated with a higher risk of NAFLD, whereas the consumption of fish with omega-3 reduces the risk, independent of age, BMI, and sex. Female participants with NAFLD even had a higher calorie intake than male participants with NAFLD. 31 This could be explained by the fact that women have greater awareness to serving sizes and energy density than men, a recall bias of the dietary self-reports must be taken into consideration.
Fructose Consumption
Ouyang et al investigated the correlation between fructose consumption and NAFLD and noted that individuals with NAFLD consumed greater quantities of fructose: 365 kcal/d versus 170 kcal/d among healthy individuals. 43 In a Finnish nutrition trial comprising 663 participants, the authors also noted a higher consumption of fructose among women than among men. Individuals with the highest quartile of fructose intake had a higher level of education and physical activity, a higher intake of dietary fiber, and a lower intake of fat, and they were less likely to be smokers than individuals with the lowest ingestion of fructose. 44
Surprisingly, the prevalence of NAFLD was 28% to 44% lower among those with the highest consumption of fructose than those with the lowest fructose intake. The average fructose intake was 20 g/d; only 60 persons reported a fructose intake in excess of 60 g/d. The cohort study provides no data about the sources of fructose. 44
Discussion
Nonalcoholic fatty liver disease is one of the leading causes of end-stage liver disease; its rising prevalence is associated with T2DM and obesity. Seventy percent of persons with T2DM are affected with NAFLD. 2 Ethnicity plays an important role in the prevalence of NAFLD; the risk is especially high among Hispanics and Asians. 10,11
Environmental, behavioral, and genetic factors influence the accumulation of intrahepatic fat and progression of the disease. There is a lack of epidemiological studies about ethnic differences in prevalence rates of NAFLD in European countries.
The results of the Austrian Diabetes Report 2013 report a prevalence of diabetes among 8% to 9% of the Austrian population. 45 Socioeconomic status and education level are negatively correlated with the presence of T2DM, especially for women. People with migration background have an overall higher risk of chronic diseases. Female migrants in Austria have 3- to 4-fold higher risk of developing T2DM, while male migrants have a 1- to 4-fold higher risk. 45,46 If we consider the prevalence of NAFLD among persons with T2DM with 70%, individuals with migration background are a susceptible risk group for the cluster of metabolic diseases.
Nonalcoholic fatty liver disease is a multisystem disease and an essential cardiovascular risk factor. 23,24 Pro-inflammatory cytokines from adipose tissue may be the link between NAFLD and extrahepatic comorbidity. 22 -25
The intense metabolic crosstalk between dysfunctional visceral adipose tissue and the liver causes a pro-inflammatory condition, with a greater release of free fatty acids and cytokines, hepatic and peripheral insulin resistance, and the reduction of anti-inflammatory cytokines such as adiponectin. The liver as such is a source of oxidative stress, hypercoagulability, hypofibrinolysis, and atherogenic dyslipidemia. 27
Especially postmenopausal women are at high risk of developing NAFLD due to their reduced estrogen and increased testosterone levels. Moreover, changes in the distribution of adipose tissue and greater visceral adiposity aggravate the disease in postmenopausal women. Men with NAFLD have higher ALT levels and lower leptin levels than women. 16,17 Reduced testosterone levels (aging men, hypogonadism, hormone therapy) serve as a promoter because of the effects of testosterone on adipose tissue distribution and insulin sensitivity.
Characteristically, women with NAFLD have lower ALT levels, but higher leptin levels. Estrogen deficiency during and after menopause as well as relative androgen excess and insulin resistance in the presence of PCOS have various effects on lipid metabolism and play a key role in the development of NAFLD. 8,14,22
The nutrition trials reveal similar data concerning the gender aspects of nutrition and indicate that there are “typical” female dietary patterns. Women of all age groups are healthier than men with regard to their food behavior. 35 -42 Nutrition plays a key role in the pathogenesis and progression of NAFLD. However, there is evidence that female dietary patterns are not causative for the increased incidence of NAFLD among postmenopausal women.
Kanerva et al noted that the quality of food, especially the quantity of fiber consumption, nutrient intake, physical activity, and abstinence from smoking, may reduce the risk of NAFLD. 44
Fructose consumption is frequently discussed as a factor in the pathogenesis of NAFLD. In view of the diverse findings with regard to fructose intake, it is important to distinguish between the various sources of fructose, especially sucrose and high corn fructose syrup in industrialized products and soft drinks and their correlation with the individual’s total daily calorie intake. 43,44 Further prospective trials will have to address the effects of various fructose sources on the accumulation of fat in the liver and liver toxicity.
Conclusion
Persons of all age groups may develop clinical or subclinical NAFLD, but postmenopausal women or women with endocrine disorders such as PCOS and men with a testosterone deficiency (primarily aging men) are at particularly high risk of developing the disease. In view of the endemic prevalence of obesity throughout the world, a rising incidence of NAFLD may be anticipated among children and adolescents in the coming decade. Sex- and gender-specific nutritional support and lifestyle intervention with focus on physical activity and weight reduction are basic tools of early treatment as well as primary prevention.
Furthermore, nutritional medicine and nutritional therapy should be given greater importance in rehabilitation therapy for cardiovascular disease, adapted to the sex- and gender-specific needs of men and women. It should be noted that nutrition trials report a lower level of health consciousness and less healthy food choices among men. Doctors, health professionals, insurance companies, and other stakeholders must be cautioned about the fact that NAFLD is a systemic disease with a high level of cardiovascular and overall mortality. Early screening procedures for high-risk individuals, especially premenopausal women with PCOS, should be established in clinical routine. In view of the rising prevalence of NAFLD over the past decade, the health-care system is confronted with the challenges of targeted prevention strategies, early diagnosis, and effective interdisciplinary treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.