
Abstract
Therapeutic options for Renal Cell Carcinoma (RCC) are rapidly advancing. Systemic immune-oncology (IO) treatments, including immune checkpoint inhibitor (ICI) combination therapy and ICI with vascular endothelial growth factor tyrosine kinase inhibitors (VEGF TKIs), have shown substantial overall survival advantages. Data comparing first-line treatments for advanced RCC is limited, and second- and third-line therapies are frequently determined by approvals prior to current therapies. Pragmatic clinical trials (PCTs) are designed to inform a clinical decision by implementing evidence in a real-world setting. PCTs have increasing relevancy in oncology and offer advantages including generalizability, ease of trial execution, and can assist in evaluating whether therapies exhibit equivalent efficacy in clinical practice. Several PCTs have provided insight into metastatic RCC (mRCC) management. COMPARZ and PICSES trials compared pazopanib to sunitinib for mRCC patients and offered new insights into tolerability and patient preference. The MaRCC Registry yielded real-world data on treatment patterns and physician decision-making. The CARMENA trial demonstrated non-inferiority of sunitinib alone versus nephrectomy followed by sunitinib, while the STAR trial explored standard continuous versus intermittent VEGF-TKI therapy. Ongoing PCTs include the PROBE trial, ODYSSEY RCC, and CARE1 trials. Future opportunities for PCTs include comparing second-line treatment regimens for mRCC, examining differences in clinical responses by gender or age, the use of consolidative tumor-directed therapy in oligometastatic disease or for debulking metastases, and the impact of lifestyle variances on management. PCTs are needed to fill knowledge gaps and address patient-centered priorities that can inform our practices and improve quality care for patients with mRCC.
Introduction
Renal cell carcinoma (RCC) is among the most common cancers in the United States, with an estimated 81,610 diagnoses reported in 2024.1,2 The treatment landscape for RCC is rapidly evolving, with various targeted therapies emerging in the last decade as promising treatment options.1,3 Notably, systemic immune-oncology (IO) treatments such as immune checkpoint inhibitor (ICI) combination therapy and ICI combined with vascular endothelial growth factor tyrosine kinase inhibitors (VEGF TKIs) have demonstrated significant overall survival benefits.4–6 However, data comparing contemporary first-line RCC treatment options remain limited. 4 To date, no head-to-head randomized control trials (RCTs) have compared approved ICI-based combination treatments. 4 Efforts have been made to compare first-line interventions, such as ICI-ICI and ICI-TKI combinations, through network meta-analyses, but these studies have had their limitations, including inconsistent treatment durations and limited follow-up, making it difficult to infer differences in overall survival benefits.4,7
Despite advances in first-line treatment outcomes, many patients will require second-line therapy. 6 Evidence to inform second-line therapies in the IO era is also an underexplored aspect of RCC management. Guidelines for second-line therapy are based on approvals before current frontline therapies were being used, and in the second and third lines, control arms are based on antiquated historical standards, typically sunitinib or everolimus.6,8,9 As therapies evolve, there is a growing need for real-world evidence and comparative analysis to inform practice and guidelines for RCC treatment. 7 Pragmatic clinical trials (PCTs) can aid in determining if therapies perform as well in the clinical realm as they do in registrational randomized controlled trials (RCTs).10,11 The following review discusses how pragmatic trials can be practice informing, complementing RCTs by providing increased generalizability and real-world evidence surrounding current RCC treatment options.
What is a pragmatic trial?
The concept of pragmatism in clinical trials emerged in response to concerns that traditional registrational RCTs are at risk of not adequately representing clinical practice. 10 PCTs aim to inform a clinical decision by implementing evidence in a real-world setting with fewer limitations and common constraints that more definitive RCTs face.10,12 While RCTs are an ideal study for establishing causal relationships, their findings may not always apply to the patient population that ultimately uses the studied intervention.11,12 PCTs have broader inclusion criteria, endpoints relevant to clinical practice, and often fewer exclusion criteria, which can increase their generalizability.12,13 One example of an RCT with limited external validity improved by a PCT can be seen when comparing the METEOR trial to Outcomes Database to Prospectively Assess the Changing Therapy Landscape in Renal Cell Carcinoma (ODYSSEY RCC) trial.8,14 The METEOR trial specifically assessed cabozantinib (Cabometyx, Exelixis) versus everolimus, an mTOR inhibitor, in patients that had progressive RCC following VEGF TKI therapy. 8 In METEOR, the trial had strict inclusion criteria including Karnofsky performance status score of at least 70% and restrictions on comorbidities and organ function. Additionally, METEOR was not indicative of the large percentage of patients that are now post- IO treatment, limiting its relevance today. 8 ODYSSEY, as discussed further below, is an ongoing prospective observational study to evaluate real world treatment patterns across academic and community settings. 14 The registry includes patients with varying performance statuses and those who have been on previous IO combination therapy, more representative of today's population of RCC patients. ODYSSEY also incorporates assessments of quality of life and treatment tolerability, which impact patient adherence and provide more representative real-world conditions. 14
PCTs aim to answer more basic, practice-informing questions. PCTs are often more cost-effective, patient-friendly, and easier to carry out than traditional RCTs.10,12,15 The primary goal of pragmatic trials is not to gain regulatory approval from organizations such as the Food and Drug Administration (FDA) but rather to inform practice in the real world. PCTs have increasing relevance in oncology, particularly in RCC, where head-to-head comparisons of treatment options are rare. Pragmatic trials can serve as a link between controlled clinical research in RCTs and daily clinical practice to ensure results remain applicable to direct patient care. 16 Some drawbacks of PCTs include the requirement of often larger sample sizes than RCTs, extended follow-up periods, and the potential for increased variability in responses given the heterogeneity of patient characteristics. 17 The pros and cons of pragmatic trials are listed in Figure 1.
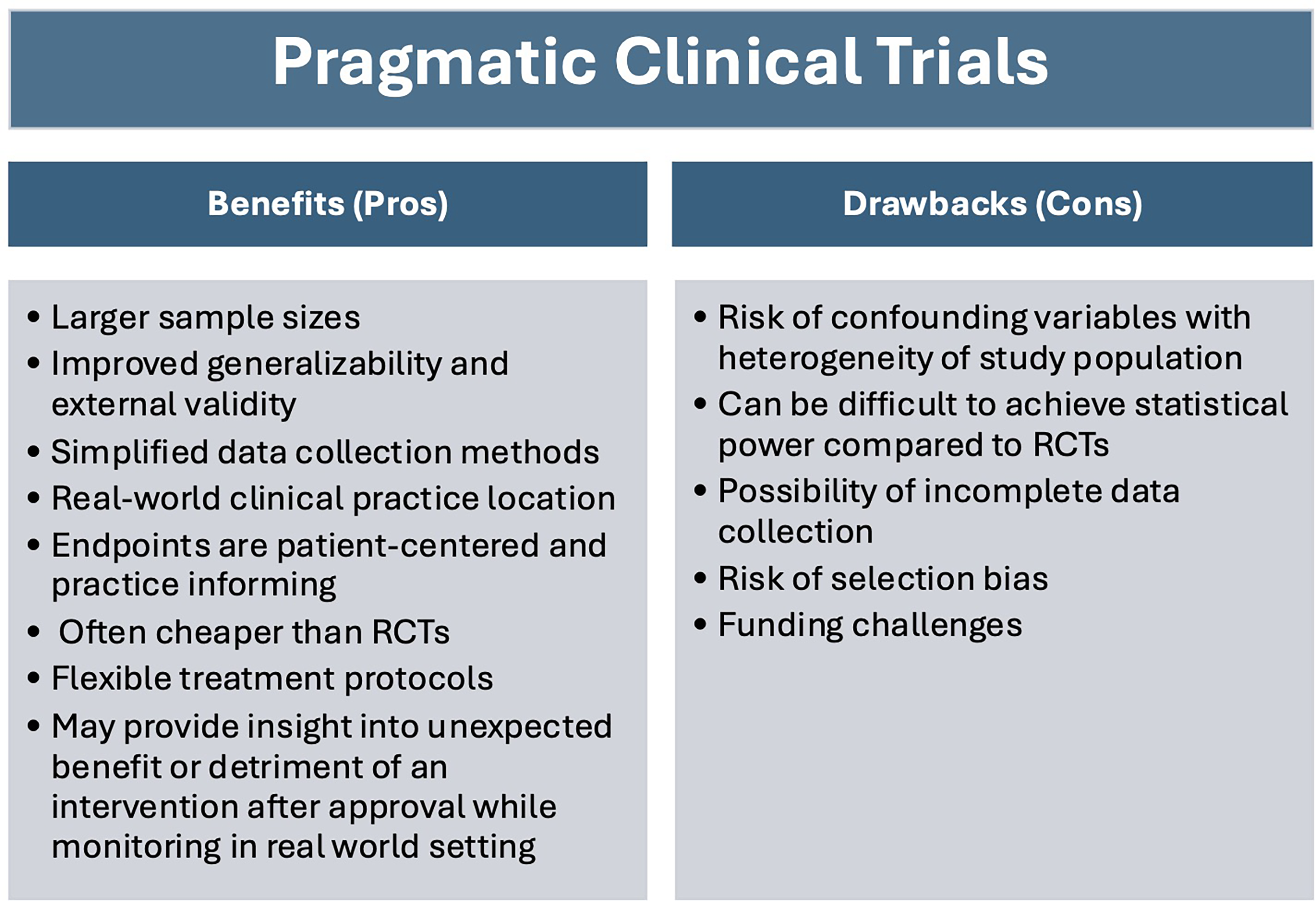
Pros (left side) and cons (right side) of pragmatic clinical trials.
Real-World evidence in RCC
Real world evidence encompasses data that is routinely collected from medical records, product and disease registries, and other sources that can inform on health status and generate evidence on practice patterns. 18 Real world evidence can serve as a compliment to RCTs and aid in increasing the generalizability of a study intervention. 18 Within real world evidence falls pragmatic trials, which include prospective PCTs and registries, and retrospective real-world data analysis, all of which are pragmatic in nature. The FDA recently issued guidance on real-world data collection to ensure reliability and relevance of data for generating real world evidence.18–20 Data reliability is further classified into accuracy of data, completeness, and traceability to ensure quality of data collection is upheld. 20 Real-world evidence collected from health record reviews, similar to traditional PCTs, can reflect the clinical environment and highlight relevant information on comorbidities, adherence, and additional treatments used. 18 Traditional prospective PCTs, however, retain advantages compared to retrospective real world data analyses, including participant randomization and prospective data collection, but both approaches generate valuable information to inform clinical practice.
The distinction between explanatory, randomized controlled trials compared to pragmatic trials is often not completely distinct, but rather on a continuum. There are working groups that have developed tools to aid in study design and assessment of pragmatism in trials such as the Pragmatic- Explanatory Continuum Indicator Summary (PRECIS) tool. 21 PRECIS has undergone further revisions to the now more widely used PRECIS-2 tool. The PRECIS-2 tool has nine domains: eligibility criteria, recruitment, setting, organization, flexibility in delivery intervention, flexibility in monitoring adherence relative to usual care, follow up, primary outcomes, and primary analysis. 22 Each domain is then scored from 1–5 on the degree of pragmatism, with 5 being the highest in pragmatism. 22 In this manuscript, we discuss examples of current and ongoing pragmatic trials to demonstrate their value and highlight opportunities for future pragmatic trials.
Pragmatic RCC trials and registries
The following section includes examples of completed and ongoing trials and registries regarding RCC management that are pragmatic in nature. Table 1 summarizes the trials included in this review.
Examples of completed or ongoing pragmatic RCC trials.

Pragmatic trials
Pazopanib versus sunitinib in metastatic renal-cell carcinoma (COMPARZ)
The COMPARZ trial is a multinational, phase III, randomized, non-inferiority study aimed at comparing the efficacy and tolerability of pazopanib with sunitinib for the treatment of metastatic renal cell carcinoma (mRCC). 23 These treatments were both first-line therapy for mRCC during study enrollment and completion. 23 The primary endpoint was progression-free survival (PFS), while secondary endpoints included overall survival, health-related quality of life, safety, and medical resource utilization. The trial enrolled a total of 1110 patients who were randomized to either receive pazopanib 800 mg once daily on a continuous regimen or sunitinib 50 mg once daily, administered in a 6-week cycle consisting of 4 weeks of treatment followed by 2 weeks without therapy. 23 Results demonstrated that disease progression was comparable in both groups. Median PFS was 8.4 months in the pazopanib cohort compared to 9.5 months in the sunitinib arm, with a hazard ratio for progression or death of 1.05 [95% CI, 0.90–1.22], 23 meeting the predetermined criteria for noninferiority. Median overall survival (OS) was also similar between groups, with a hazard ratio for death of 0.91 [95% CI, 0.76–1.08]. 23
The study highlighted non-inferiority in PFS, but there were notable differences in secondary endpoints, including adverse events and tolerability of the therapies. 23 Fatigue was reported in 55% of patients receiving pazopanib versus 63% in the sunitinib group. Hand-foot syndrome occurred in 29% of pazopanib-treated patients compared to 50% of patients in the sunitinib group. 23 Hematological abnormalities such as leukopenia, thrombocytopenia, anemia, and neutropenia were more prevalent in the sunitinib group. Thrombocytopenia was observed in 78% of sunitinib-treated patients compared with 41% for those treated with pazopanib. 23 In contrast, elevations in alanine aminotransferase were more frequent in the pazopanib cohort (60% vs. 43% in sunitinib) and were one of the primary reasons for pazopanib discontinuation. 23 Health-related quality-of-life evaluations significantly favored pazopanib across 11 of 14 of the variables measured in the initial six months of therapy. 23 The pazopanib group had fewer emergency department visits and telephone consultations. These findings indicated improved tolerability, lower medical resource utilization, and a better side effect profile for pazopanib compared to sunitinib. 23 COMPARZ is pragmatic in nature according to the PRECIS-2 tool given the study included patients that were eligible for first line-therapy across a broad geographical area reflecting routine care, and allowed for flexibility in intervention delivery and adherence given dose reductions were made for patients with adverse effects. COMPARZ provided insights into how clinicians may prioritize lower adverse effect burden and improved patient-reported outcomes when selecting treatments with comparable efficacy for mRCC.
Randomized, Controlled, Double-Blind, Cross-Over Trial Assessing Treatment Preference for Pazopanib Versus Sunitinib in Patients With Metastatic Renal Cell Carcinoma: PISCES Study (PISCES)
The PISCES study is a randomized, multicenter, double-blind, phase III crossover trial that assigned patients with mRCC in a 1:1 ratio to receive either pazopanib or sunitinib followed by the alternative therapy. 24 Pazopanib was administered at a dosage of 800 mg once daily for ten weeks, while sunitinib was dosed at 50 mg once daily for four weeks, followed by a two-week placebo period, then resumed at 50 mg once daily for the remaining four weeks resulting in a total duration of ten weeks. 24 The primary endpoint of the study was to assess patient preference for treatment with pazopanib versus sunitinib, which was assessed at the end of treatment periods using a questionnaire. 24 Patients were queried regarding their preference for therapy administered in period one versus period two. The study also allowed patients to indicate no preference. A total of 114 patients were included in the analysis of the study.
Results indicated that 70% of patients preferred pazopanib [95% CI, 60.9% to 78.4%] compared to 22% favoring sunitinib [95% CI, 14.7% to 30.6%]. 24 Eight percent of patients expressed no preference between therapies. There was a higher proportion of patients that preferred the treatment in period one, but after correcting for response differences between treatment periods, patient preference for pazopanib over sunitinib remained statistically significant [49.3% (95% CI, 34.7% to 63.8%)]. 24 According to the administered questionnaires, factors that primarily influenced patients to select pazopanib as their preferred treatment included increased quality of life (QoL) and less fatigue. 24 Patients who preferred sunitinib (22% compared to 70% who preferred pazopanib) cited less diarrhea and overall QoL as primary reasons. Physician preferences were in line with patient preferences, with 61% of physicians preferring pazopanib, with the remaining physicians selecting sunitinib or no preference. Although pazopanib and sunitinib are now rarely utilized in clinical practice, the PISCES trial complements the efficacy and safety data of the COMPARZ trial, and meets pragmatic criteria according to PRECIS-2 in the primary outcome domain, given patient preference was the primary outcome and highly relevant to participants, and offers additional insight into how patient-reported outcomes (PROs) and treatment data can influence mRCC treatment decisions.
Sunitinib alone or after nephrectomy in metastatic renal- cell carcinoma (CARMENA)
Another pivotal pragmatic trial is the CARMENA trial. 25 Multiple studies prior to the advancement of immunotherapy and targeted therapies indicated that cytoreductive nephrectomy was a cornerstone of treatment. 26 The CARMENA trial was a prospective, multi-center, open-label, randomized, phase III non-inferiority study aimed at assessing the role of nephrectomy in mRCC patients who were also receiving targeted systemic therapy. The trial included a total of 450 patients from September 2009 to September 2017 from 79 healthcare centers in France among a small subset of other centers in Europe. 25 The primary endpoint of the study was OS. Some of the secondary endpoints included PFS, objective response rate, treatment adherence, mortality, and safety, among others.
The study results indicated that patients who received sunitinib alone had a longer median OS [95% CI] than those who underwent nephrectomy and sunitinib (18.4 months [14.7 to 23.0] vs. 13.9 months [11.8 to 18.3]) in the intention-to-treat (ITT) analysis population. 25 Following the OS analysis, the hazard ratio (HR) for death showed that sunitinib alone was noninferior to nephrectomy followed by sunitinib therapy in mRCC patients (HR 0.89 [0.71 to 1.10]) with intermediate or poor-risk disease based on the study's functional scoring system. Among patients with poor-risk and intermediate-risk disease, the median OS was longer in the sunitinib group compared to the nephrectomy–sunitinib group (23.4 versus 19.0 months in the intermediate-risk subgroup and 13.3 vs. 10.2 months in the poor-risk group). 25 In 67.1% of the patients included in the study, sunitinib therapy was discontinued due to disease progression, in 13% due to adverse effects, and in 6.2% due to patient death. 25 If either group was unable to tolerate sunitinib, everolimus followed by axitinib (INLYTA, Pfizer) was used as subsequent therapies.
CARMENA is an example of a pragmatic trial, as aspects of the trial's design and setting align with pragmatic domains of the PRECIS-2 tool. The trial recruitment spanned across multiple countries in Europe and captured a large patient population across approximately 8 years. The sunitinib intervention was implemented in accordance with standard of care protocols, permitting dose modifications or subsequent treatment with agents like everolimus, reflecting actual clinical practice. However, a limitation of the trial is that candidates included in the study were all deemed appropriate for nephrectomy by a referring urologist, which places the patient population at a higher performance status than patients not a candidate for nephrectomy with mRCC. The trial highlights that prior to the IO era, avoiding surgery might provide benefits such as minimizing surgical complications and avoiding blood transfusions, among others without compromising outcomes.25,27 Further pragmatic trials, such as the PROBE trial, will investigate the utility of nephrectomy now that ICI combination therapies are used in the front line. 28
Temporary treatment cessation versus continuation of first-line tyrosine kinase inhibitor in patients with advanced clear cell renal cell carcinoma (STAR)
The STAR trial aimed to assess if a drug-free interval strategy for TKIs would be non-inferior to conventional continuation therapy for treatment of advanced RCC. 29 The trial was conducted from January 2012 to September 2017 and included 920 participants across 60 United Kingdom hospital sites. 29 The average follow-up period was 58 months. The sites included in the study ranged from comprehensive cancer centers to local cancer units. Co-primary endpoints included OS and quality-adjusted life years (QALYs). Patients in this open-label, non-inferiority trial were randomly assigned to either a continuous TKI strategy or intervals without drug therapy. TKIs included as part of the study were oral sunitinib (50 mg per day; 4 weeks on treatment followed by 2 weeks off) or oral pazopanib (800 mg per day) for at least 24 weeks (four cycles) according to the standard drug dosing guidelines at the time of the study. The treating physician selected each TKI used. Upon assessment at 24 weeks, participants of the study who had a complete response, partial response, or stable disease on therapy began randomized allocation to either continuous therapy or temporary cessation. Following the 24-week time mark, 488 trial participants were included in the study. 47% of total participants discontinued the treatment prior to reaching allocation due to various reasons, with the most common being radiological disease progression and toxicity. There was comparable drop-out in the continuation strategy and drug-free interval strategy. The study results were analyzed using both ITT and per-protocol analysis. In the ITT protocol population only, it was found that the drug-free interval strategy was noninferior to continuation therapy (HR .97 [.83 to 1.12]). The study also demonstrated non-inferiority with QALYs in both the ITT and protocol groups. The most common adverse effects noted in the study included hypertension (26% in the conventional continuation strategy vs. 29% in the drug-free interval group), hepatotoxicity (11% in both arms), and fatigue (8% in the continuous vs. 15% in the drug-free interval strategy).
Given that targeted RCC treatments are often continued for months to years, the survival benefits of therapy are often obtained at the expense of quality of life.29,30 The STAR trial was one of the first studies to assess co-primary endpoints of QALYs and OS. The study did reveal non-inferiority when assessing temporary treatment cessation vs. continuous therapy for QALY in both ITT and per-protocol analysis. However, the study did not result in a conclusive non-inferiority result for OS in the per-protocol analysis, which makes it difficult to infer non-inferiority for temporary treatment cessation. The authors note, however, that there was not a clinically meaningful reduction in life expectancy identified between treatment groups. As a secondary reported measure, economic benefits and cost analyses were performed. The study uncovered cost benefits associated with the treatment break approach. While non-inferiority was not clearly indicated in the OS endpoint, there are potential lifestyle, quality of life, and health economic advantages to treatment breaks in TKI therapy that, per STAR, are unlikely to be detrimental to patient outcomes. According to PRECIS-2, this study demonstrated pragmatic features by being conducted at numerous sites including district hospitals and cancer centers, where patients would routinely receive care. The primary and secondary outcomes were all also highly relevant to participants in the study. STAR provides valuable information if there is a direct patient need to pause therapy, such as a drug shortage, toxicity concerns, or alternative health care need that requires disruption of treatment, as often happens in clinical practice.
Comparing the outcome of immunotherapy-based drug combination therapy With or without surgery to remove the kidney in metastatic kidney cancer, the PROBE trial (PROBE)
Since the publication of the CARMENA trial, which demonstrated noninferiority in survival outcomes with nephrectomy and TKI therapy vs. sunitinib alone, there have been further advancements in the treatment for RCC. 25 ICI combination therapy in particular has quickly become the standard of care for mRCC. 31 Led by the SWOG cooperative group, the PROBE trial is an ongoing phase III trial that assesses differences in OS in participants with mRCC who receive ICI-based combination therapy with cytoreductive nephrectomy versus solely ICI therapy. 28 Secondary objectives include comparing survival rates between immunotherapy treatment arms, evaluating post-nephrectomy complications and drug toxicities, and assessing for change in primary tumor at week 12 during disease assessment for those that received pre-randomization treatment. The trial is expected to be complete by 2033. The study has 387 participating locations. The patients meeting eligibility for the study are treated with one of the IO combination therapies: ipilimumab and nivolumab, axitinib and pembrolizumab (Keytruda, Merck & Co), or axitinib and avelumab (Bavencio, Pfizer).
Since trial initiation, PROBE has also included amendments to expand additional therapy combinations, including lenvatinib (Lenvima, Eisai and Merck & Co) plus pembrolizumab and cabozantinib (Cabometyx, Exelixis) plus nivolumab, which represents an adjustment to real-world, first-line treatment options. Amendments such as these are possible in pragmatic trials, which allow for the data to remain relevant to a changing treatment landscape. Randomization of trial participants will occur between 10 and 14 weeks of therapy, with participants receiving nephrectomy followed by ICI combination therapy or continuing solely on systemic therapy. Approximately 300 participants are eligible for trial inclusion. The authors hypothesize that cytoreductive nephrectomy will improve OS in advanced RCC post-ICI-based therapy. PROBE is consistent with pragmatism in the eligibility, setting, flexibility of delivery and adherence, analysis and outcome domains of the PRECIS-2 tool. The study will produce key data that will allow for secondary analysis and comparison of response rates to treatments that mimic real-world practice with first-line therapies.
CARE1 pragmatic clinical trial: first line randomized study platform to optimize treatment in patients with metastatic renal cell carcinoma (CARE1)
CARE1 is a pragmatic randomized phase III study aimed at optimizing treatment in patients with mRCC. 32 The trial is an active international, multi-center study with a primary objective of delineating which ICI-based combination therapy most improves survival. In particular, the authors hypothesize that ICI-ICI improves survival compared to ICI-VEGFR TKI in PDL1-positive patients. 32 The study will also assess whether ICI-VEGFR TKI ultimately improves outcomes in patients that are PDL1 negative compared to ICI-ICI based treatment. By incorporating biomarker testing such as PDL-1, this pragmatic study aims to further refine focused treatment options and improve patient outcomes. The patients included will be randomized in equal ratios to receive either ICI-ICI or ICI-TKI therapy.
CARE1 will enroll a total of 1200 participants across a total of 8 European countries. Given the extensive breadth of recruitment and comparison between first-line therapies, the generalizability of this trial is expected to be high and invaluable to clinicians deciding between first-line therapies. The study is highly pragmatic in multiple PRECIS-2 domains, notably eligibility, setting, follow-up, and outcomes. While decisions regarding therapy are often based on various factors, such as prognostic indicators, side-effect profiles, physician preference, and performance status, biomarkers could provide additional insight into optimal management.6,33 Secondary outcomes to be assessed in the study include PFS, objective response rate, time to initiation of treatment, length of therapy, QoL, safety, economic viability, and additional PROs. 32 Additionally, this study attempts to gather time until subsequent systemic therapy, a very valuable end point that can aid in answering the expected response and duration of initial treatment in first-line therapies. These clinically relevant primary and secondary endpoints will likely yield invaluable insight into practice patterns and comparative analysis between therapeutic options in a real-world setting.
Pragmatic registries
The metastatic renal cell carcinoma (MaRCC) registry
The MaRCC Registry is a United States-based prospective observational cohort study that collected data surrounding real-world clinical practice patterns and patient outcomes for mRCC across both academic and community settings. 34 The study enrolled a total of 505 patients with known mRCC from March 2014 to December 2016. 33 Of those, 376 patients included within the MaRCC registry initiated mRCC therapy and met inclusion criteria. 287 (76.3%) patients initiated first-line therapy as the initial treatment strategy rather than undergoing a period of active surveillance followed by delayed systemic therapy. 320 participants received the standard of care at that time in the first line with pazopanib (171, 45.5%) or sunitinib (75, 19.9%) or enrolled in a clinical trial. 33 Greater proportions of clinical trial participants had an Eastern Cooperative Oncology Group performance status of 0 (60.8%), and most clinical trial patients were identified to have clear cell histology (∼89%). 33 OS (95% CI) was longest in the clinical trial group (50.3 months on average) versus pazopanib (39.0 [29.7–50.9] months) and sunitinib (26.2 [19.9–61.5] months). Non-clear cell RCC was associated with worse median OS than clear cell RCC (18.0 vs. 47.3 months). 33
Physicians in the study provided survey data to reveal insight into critical treatment decisions and selections of first-line therapy. Likelihood of clinical response was the highest prioritized factor in terms of OS or PFS (35.9% of responses), followed by likelihood of tumor regression. 33 Individualized characteristics of the patient, including prognostic factors, co-morbidities, performance status, and age, collectively accounted for approximately 26% of the reasons physicians prioritized a particular treatment. Other factors, such as QoL, cost, side effect profiles, and patient preferences, were less commonly mentioned as primary reasons for physician drug selection.
Results from the study revealed that the majority of physicians adhered to prescribing guidelines, with 85.1% of patients receiving therapy supported by the National Comprehensive Cancer Network. The MaRCC Registry offered insights into first-line treatment choices and the rationale of physicians regarding therapy selection in a real-world trial context. While this period was prior to the IO-TKI combination therapy era, the study provides useful information surrounding how first-line therapies at the time were prescribed and utilized by patients as newer IO-based first-line treatment options became available. Including PROs will likely also assist in physician decision-making. Prior studies, such as the phase III Check-Mate 214 trial with ipilimumab (Yervoy, Bristol Myers Squibb) plus nivolumab (Opdivo, Bristol Myers Squibb) combination therapy, revealed that patients receiving this therapy compared to sunitinib had better QoL outcomes and fewer symptoms.33,35 Therefore, continuing to study treatment selection patterns and patient-specific factors will yield invaluable insight into RCC management.
The study also revealed outcomes of mRCC patients who did not receive any systemic therapy in the first line setting, so-called deferred treatment or active surveillance (AS) patients. 36 143 participants (32%) underwent AS and 305 started immediate systemic therapy (ST). With a median of 33 months of follow up, only 50% of patients (72/143) had initiated ST with 17% deaths (compared to 52% for the immediate ST cohort). Baseline characteristics differed between the AS and ST cohorts in that AS patients were more likely to have ECOG performance status 0 (53% vs 36%), to be clear cell histology (87% vs 76%), to have adrenal metastases (16% vs 8%) and to have a favorable IMDC risk score (60% vs 14%). AS patients were less likely to have an intermediate IMDC risk score (38% vs 65%) or to have bone metastases (18% vs 27%). 36 The MaRCC Registry meets PRECIS-2 pragmatic criteria in eligibility, recruitment, setting, flexibility of delivery and adherence, and follow up, making this registry highly pragmatic in nature.
Outcomes database to prospectively assess the changing therapy landscape in renal cell carcinoma (ODYSSEY RCC)
ODYSSEY RCC is a prospective, observational cohort Phase IV study that is aimed at understanding the cancer management and health-related QoL factors in patients diagnosed with mRCC. 14 The study aims to recruit approximately 800 participants receiving care in both academic and community centers. Inclusion criteria for the study are broad. Individuals are required to be greater than 19 years of age and could have had prior surgery and/or radiation therapy. Patients in active surveillance for RCC and patients who received prior neoadjuvant or adjuvant therapy for non-metastatic RCC are permitted to be included. 14 Patients treated for metastatic solid tumors apart from mRCC are excluded from the study. ODYSSEY RCC will primarily evaluate and gather data surrounding patient experiences through PROs via novel methods using PCORnet and Medicare data to minimize the burden on data collectors. Secondary objectives in the study are to collect decision-making factors that go into first-line treatment selection, duration of treatment, and factors that influence a physician's decision to cease therapy. Simultaneously, the study will attempt to address knowledge gaps for how real-world patients symptomatically change with IO treatment combinations. 14 This trial is pragmatic in nature given its primary focus on assessing clinically relevant endpoints, ease of collecting data, and broad inclusion criteria.
Opportunities for pragmatic RCC trials
Pragmatic trials present an opportunity to generate real-world practice evidence regarding the management of RCC. Despite the potential to refine clinical guidelines, pragmatic trials remain underutilized. 37 In the current treatment regimen era with IO and VEGF TKI therapies, there is a lack of head-to-head comparisons between frontline options. 4 Pragmatic trials can aid in patient selection for frontline therapies and help understand optimal second-line therapies after progression on IO combinations, using current standard of care as control arms.14,32 Traditional clinical trials focused on RCC targeted therapies lack the power to establish superiority, and non-inferiority trials often lack the ability to inform practice.38,39 Hence, pragmatic trials can help clinicians potentially understand when to choose one regimen over the other or if there is a difference in tolerance in the real world. For example, in an elderly population, perhaps a lower dose of drug could be efficacious or even allow for fewer treatment breaks. In contrast, in populations with favorable responses, pragmatic trials can attempt to determine if intermittent therapy will allow for decreased side effects and toxicity. 29 While trials indicate increased PFS and OS with IO therapy such as Lenvatinib/pembrolizumab compared to sunitinib, future PCTs could evaluate outcomes for lower doses of combination therapy, assess alternative dosing intervals, and expand on which population receives the most benefit in clinical practice. 40
A further opportunity for pragmatic RCC trials involves evaluating treatment for patients with refractory disease and those who have relapsed after initial therapy. Second-line therapies with VEGF TKIs such as cabozantinib (Cabometyx, Exelixis), tivozanib (Fotivda, Aveo Oncology), combination therapy with lenvatinib, a VEGF TKI, and everolimus (mTOR inhibitor), or anti-HIF2A therapies such as belzutifan (WELIREG, Merck & Co.) have shown benefit, but the majority of evidence for therapies following progression on ICI therapy is largely generated from retrospective data.6,8,41,42,43 Selection of second-line therapy relies heavily on patient-specific factors, such as toxicity profiles, response to previous treatment, and performance status, which pragmatic trials are well suited to further classify. 6 Answering the question of superiority in second-line regimens, when to transition to second-line therapy, and if subsequent therapy should differ depending on if the patient previously received IO/TKI therapy versus IO/IO therapy are still points of uncertainty.6,43,44
Pragmatic trials can attempt to answer some of these questions pertaining to RCC management. For example, mRCC can present or progress with oligometastatic disease. In settings such as these, there is an increasing use of tumor-directed therapy. Historically, surgery, commonly referred to as a metastatectomy, would be performed but with the increasing use of stereotactic radiotherapy, the use of tumor-directed treatment has expanded and is primed for a pragmatic trial design.
Finally, PCTs are also well positioned to study differences in clinical responses by gender or age, how lifestyle variances such as diet and exercise affect RCC management, and if less intensive treatment regimens can produce similar clinical outcomes in de-escalation studies.
Conclusion
Significant advancements in the management of RCC have emerged in recent years, leading to increased therapeutic options and improved patient outcomes. However, the absence of head-to-head data comparing first-line therapies underscores the need for pragmatic trials and real-world evidence to understand how to treat patients in a clinical setting. Pragmatic trials offer ample opportunities to continue investigating patient selection, treatment options, and de-escalation of therapy to improve outcomes for patients in clinical practice.
Footnotes
Ethical approval
This study did not involve human participants or animals and was therefore exempt from ethical review. All sources of data were publicly available, and no identifiable information was used.
Author contributions
Zachary Creech contributed to conceptualization, writing, and editing the manuscript. Matthew Labriola contributed to conceptualization, writing, and editing the manuscript. Daniel George contributed to conceptualization, review, and editing the manuscript. All sources of data were publicly available, thus all authors had access to the data discussed in this manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
N/A