
Abstract
Being a developing country with a large population with high density, India was on high alert for the COVID-19 pandemic. India overcame much difficulty from the first wave, but was soon after smacked by the second wave of the COVID-19 pandemic. Due to its contiguous nature, people were advised to stay in their home, but some people have to continue their work to maintain public health, law and order and provide necessary services. Sanitary workers are one of them; they maintain cleanliness and sanitise public places, communities, towns and cities to control the COVID-19 spread. It is essential to know and understand their situation in such a problematic condition of the COVID-19 pandemic. This paper will elaborate on their social, occupational, and living conditions and possible relation with COVID-19. The author collected quantitative data through a cross-sectional study in four towns (Ladwa, Indri, Thanesar and Radaur) of Haryana in 2017. Quantitative and qualitative data had collected from sanitary workers through structured interview and observation. During fieldwork, the researcher lived with the community and observed closely. Results show that their working conditions are risky, working timings and duration also risky, alcohol and tobacco use is high, protective gears are not available to them, job status primarily contractual, no or low educational standard, health conditions are down and the standard of living is low & living situation are congested. The results indicate that they are at high risk of COVID-19 infection, to develop severe acute illness from COVID-19 and community spread. While their sanitary workers come into contact with different kinds of waste and surfaces, so their chance of infection is high because COVID-19 can survive on any surface. Their occupational, educational, social, health, living standards and living conditions make them vulnerable to developing a severe acute illness, leading to a high death rate and community spread. Therefore we need to take some essential steps in this regard.
Background
COVID-19 is well known in the present scenario, this ghost is hunting all around the world. Coronaviruses are a large family of viruses, and it can affect both animals and human beings (WHO, 2020). They develop severe acute respiratory syndrome (SARS), which is fatalistic (Jiang et al., 2020). Presently the world is suffering from COVID-19 pandemic, which is due to newly discovered coronavirus first encountered in Wuhan (China). COVID-19 is an infectious disease, can spread from person to person through droplets (Guo et al., 2020). COVID-19 spread from an infected person through droplets while coughing and exhaling, whenever other people come into contact with those droplets, they can get infected (Guo et al., 2020). The virus cannot hang in the air for much time, but can survive for a long time in an open environment (WHO, 2020). Therefore, whenever anybody comes into contact with the virus through body parts, and touches their eyes, nose and mouth, that person can get infected. The virus can show its effect from 1 to 14 days after entering into the human body, generally symptoms come in the first five days (Wang et al., 2020). People can get infected, but those at the most risk of developing serious illness are senior citizens and persons with medical conditions such as high blood pressure, heart disease, lung disease, TB, cancer and debates (Li et al., 2020). As per experts, human body immunity plays a very important role in fighting with infection or developing severe acute illness from COVID-19 infection. Lower the immunity level, higher the chance of developing severe acute illness from COVID-19, and the latter leads to death (Wang et al., 2020).
COVID-19 is declared a pandemic by word (Sohrabi et al., 2020), and advised to take precautions to stop the spread of the virus. Being a developing country, with a huge population and high-density, India is on high alert for COVID-19. Due to that India announced lockdown and later changed it into curfew. Still some people are serving to maintain public health; sanitary workers are one of them. They are serving to maintain cleanliness and sanitize public places, communities, towns and cities to control the COVID-19 spread. For public health concerns their work is very important, therefore sanitary workers are one of the strong pillars to maintain public health and stop COVID-19 infection spread. But when we talk about sanitary workers in India, it always different from other parts of the world? Because in India they, if not all but most, belong to the same social group (caste), and historically engaged in manual scavenging and sweeping (Kumar, 2017; Shahid, 2015; Singh, 2014). They are considered untouchables, and incapable to perform other duties and work (Kumar, 2014), so forced to engage in work of scavenging and sweeping. Because of their caste status and occupational status, they face exclusion in getting an education, in economic activities, residential area, political participation, and so on (Kumar, 2017; Shahid, 2015; Vivek, 2000). These condition further leads them to social stigma (Kumar, 2017). The study was conducted to understand the occupational, social, political, financial and health conditions of sanitary workers. Based on that data, the present article will elaborate on their high risk of COVID-19 infection, further developing severe acute illness from COVID-19 and further risk of community spread.
Method
The present article is written based on data collected for MPhil thesis in 2017. This was a cross-sectional study, conducted in four towns (Ladwa, Indri, Thanesar and Radaur) of Haryana at one point of time. The study followed structured interviews, observation and in-depth interviews for collecting data from study participants. The study followed both qualitative as well as quantitative methods to gather objective and subjective experience of scavenger/sweeper community, therefore the study followed a mixed-method research design.
Four towns Ladwa, Kurukshetra, Indri and Radwar of Haryana were selected for conducting the study. Towns were selected through simple random sampling (chit method). The safai karamchari (sanitary workers) of municipalities from these four towns were selected as study participants. All Safai Karamchari of each town were approached, whoever was ready to participate in the study were involved as participants. A total of 300 participants had participated in the study.
Prior permission was taken to conduct the study—a permission letter was given to all municipality office. All participants were explained about the study and its objectives before conducting the interview. Before the interview, written or verbal consent was taken from all participants. They were not given any false hope and promises for providing information.
Results and Discussion
It is very important to understand the background characteristic of sanitary workers to understand other related factors. Result shows that 74.70% of participants were male, which indicate that either male worker are more or female workers avoided participating in the study. In light of literature and cultural practices, we can accept that male workers were working more as sanitary workers compare to females.
A large number of the 128 (42.7%) participants were from 49–58 years age group, that indicates two things: first, the new recruitments were less or people are choosing this work after trying different work options (Table 1). Here both can be true because as per information, now new regular sanitary worker’s appointment is not done; work is going on through outsourcing. Contractual workers are appointed as sanitary workers, so for more benefits contractors try to complete work with minimum workforce and minimum wages. Second, attached stigma with sweeping and scavenging, this work is associated with a specific caste group, which is considered untouchable in society. Through this work they can be identified easily, so they avoid joining this work, so they try other occupations. They come back to this work when they fail to get other work or may not be accepted in other occupations due to their untouchability status.
Demographic Details of Safai Karamchari (Sanitary Worker) of Ladwa, Indri, Thanesar and Radaur of Haryana, India (N = 300).
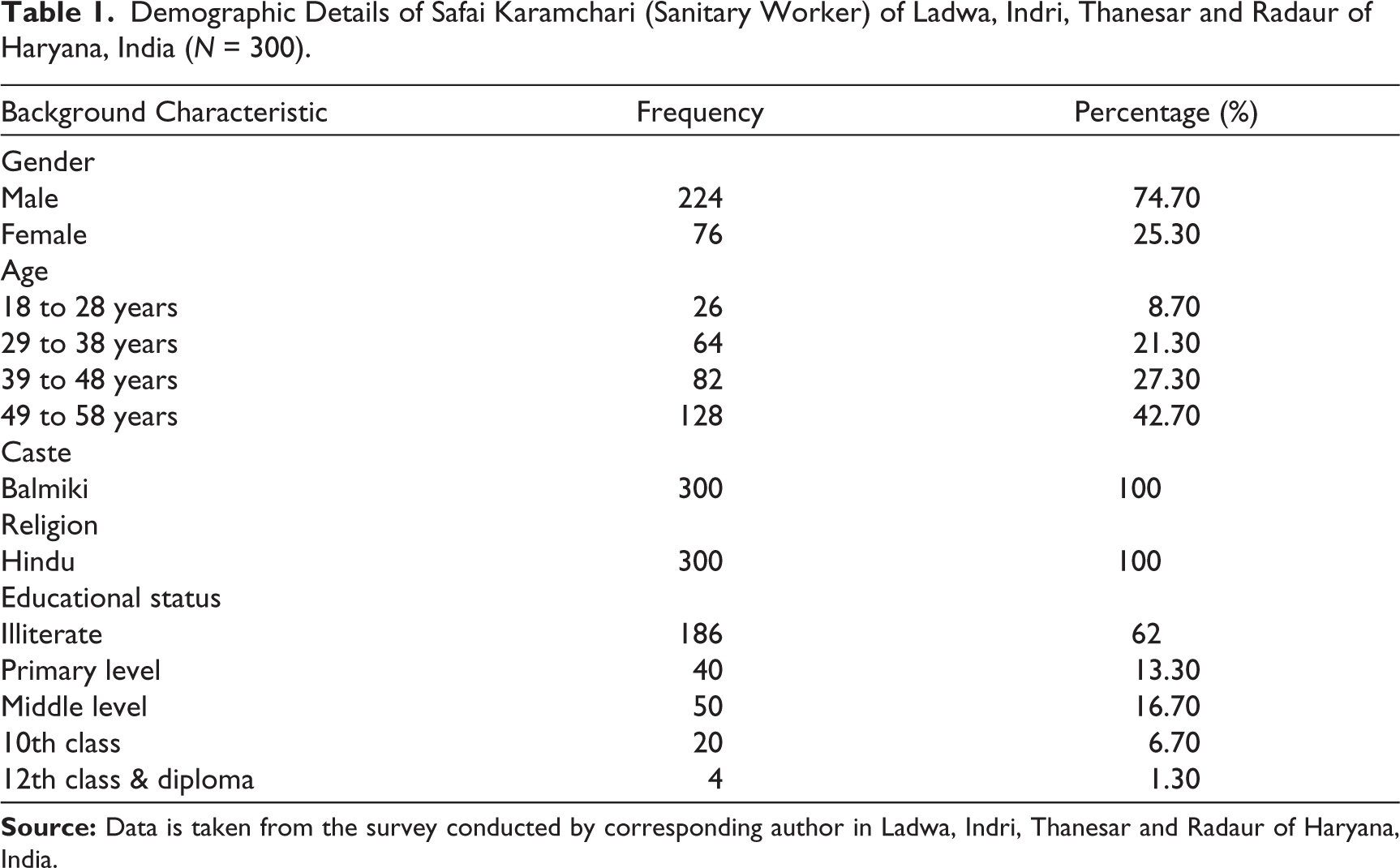
All participants belong to the Balmiki caste and Hindu religion. Again there are two possibilities, either all sanitary workers belong to the same caste or the sanitary workers from other caste groups avoided participating in the study. Both possibilities can be accepted, because historically sweeping and scavenging was associated with specific caste groups (known as Balmiki or Chuhara in Haryana), so the same system may be followed. Sanitary worker does not come forward, because of the attached stigma with this work.
The majority, 62% of participants were illiterate, and the rest also not highly educated. Having a such group of participants indicates either person with low education choose this work or community belonging to this work are excluded from getting the education. Both are highly possible because a person with high education will not choose this work due to the attached stigma and low wages. And the community associated with sweeping and scavenging is excluded from the education system, because of their untouchable status and community view that they do not need education, because they have to do menial work.
According to the aim of this article, only some occupational characteristics are included from available data. The main highlight of their occupational characteristic is their working status, use of protective gear and reason for choosing this work.
Result shows that 59.3% of participants were permanent regular worker and remaining were contractual worker (Table 2). As per them, contractual workers are more because of no new regular recruitment, but their participation in this study was less. The reason for that was, they were not allowed to leave their work and participate in the study.
Occupational Characteristic of Safai Karamchari (Sanitary Worker) of Ladwa, Indri, Thanesar and Radaur of Haryana, India (N = 300).
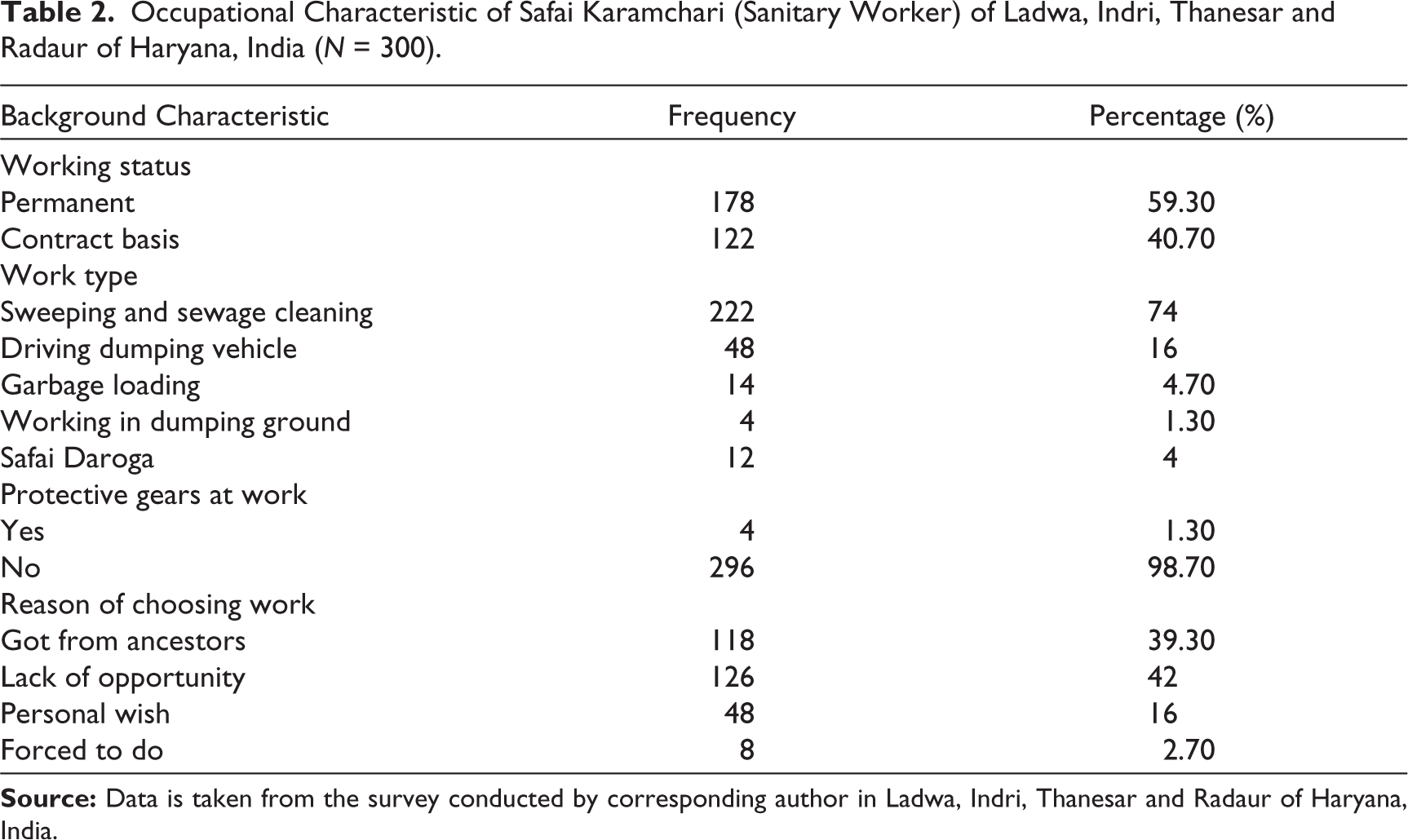
The study found that 98.7% of participants reported that they do not get any protective gear while working, the same was observed during data collection. Some of them reported that authority person take their signature or thumb impression on receiving of gloves and shoes but does not provide the same.
Health-Related Factors
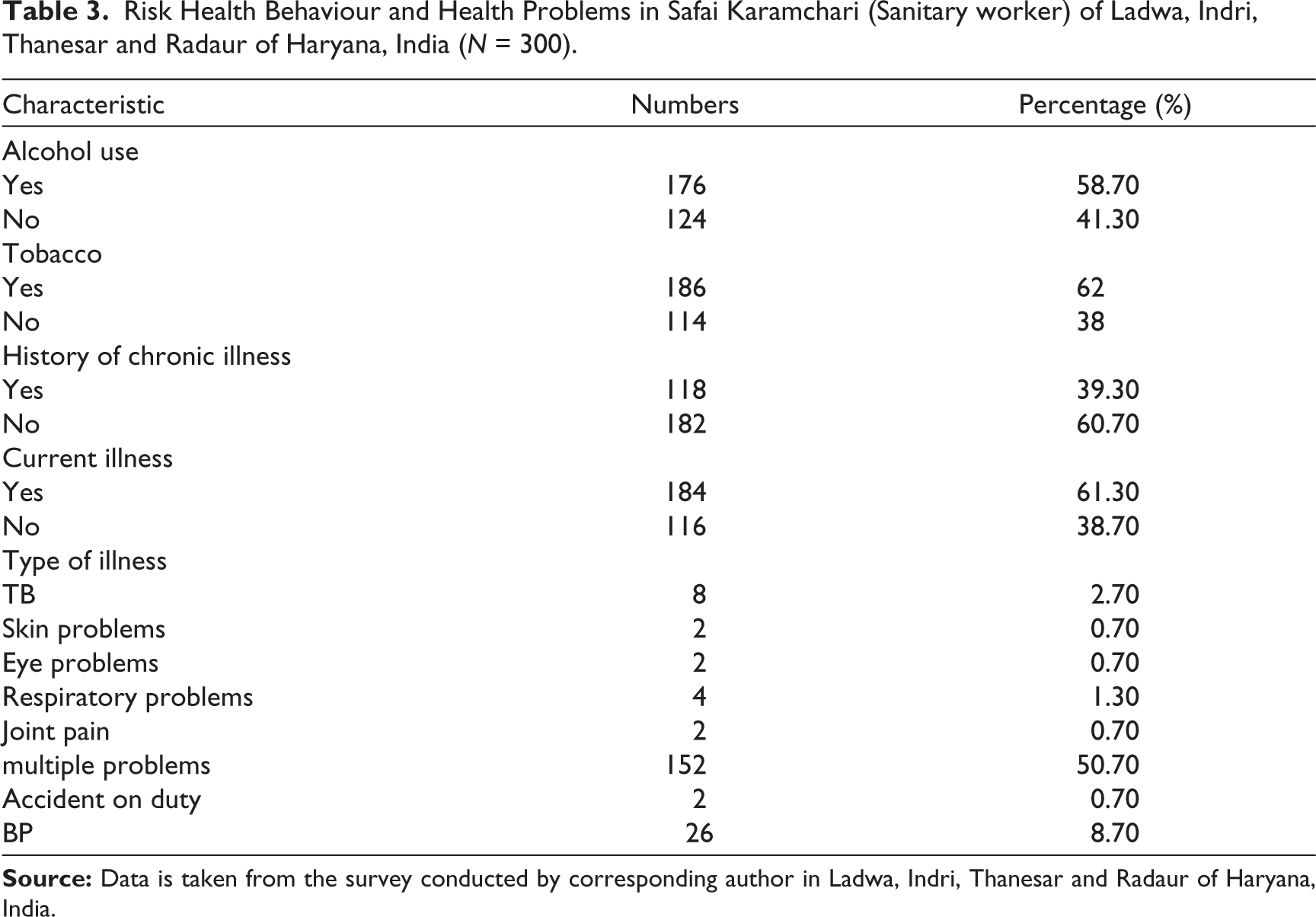
Results show that 58.7% of participants were taking alcohol daily and all were males. They also have justification for their alcohol intake, as per them they take alcohol because it is very difficult to work in dirt, fumes and bad smells without drinking. Some of the participants told bed smell and pictures of dirt keep on coming even after work, so having food also becomes difficult, that is why they drink to have food and sleep.
Tobacco is more prevalent among sanitary workers, 62% of participants reported the use of tobacco, most of which was smoking bidi. Smoking bidi is very common in Haryana, so no surprise if they are using. Even while work they are not allowed to take rest, then this bidi helps them. While smoking bidi they can have bit chat and slight rest during their work time.
Result shows that 39.3% of participants reported a history of chronic illness and injury and 61.3% respondents reported currently living with health problems (Table 3). The data is surprising but it was expected, because they deal with several chemicals, poisons gases, indisposed animal and human waste, and so on, without protective gear and without any knowledge about the danger from what they deal with.
Risk Health Behaviour and Health Problems in Safai Karamchari (Sanitary worker) of Ladwa, Indri, Thanesar and Radaur of Haryana, India (N = 300).
Working Condition: They work to clean roads, sewage lines, toilet cleaning, door to door garbage collection, garbage loading and unloading, working in dumping yards, and so on (Singh, 2009). Daily they deal with waste food items, tissue papers, used masks (in current scenario), baby diapers, dog shit, cow dung, dead animals, sewage fume and dangerous gases, dust, and several other waste products (Kumar, 2017). So while sweeping, dust collecting, loading and unloading they come in direct contact with waste products which contains so many dangerous viruses and infection.
Working Time and Duration: Their morning duty timing is 6:00 am to 1:00 pm and evening timing is 3:00
Living Conditions: Historically they were excluded from the main settlement, so they were living in the outskirts of the village, town and cities (Jammanna & Sudhakar, 2015). In the present time, they live in maholas, slums and government rehabilitation settlements, usually at the corner of the town, but due to continuous construction they came in cities. They mostly live in one to two-room houses, very close to each other’s houses (Shahid, 2015). Several places they share common community toilets, a commonplace for filling water (Vivek, 2000). They live in congested settlements, with small streets attaching each other and other places.
Belief System: As per the observation and available literature, the scavenger/sweeper community (Balmiki caste) prays to multiple godling divine.
Each family in the sweeper group worships at least one of the five special caste godlings, as well as several widely worshiped disease goddesses, village tutelary deities, and malevolent ghosts. The offerings are intended to satisfy the appetites of the deity, and thus to avert the vindictive visitation of illness and disease upon members of the worshiping household. Traditionally, each family further hoped that through extraordinary service and devotion, at least one male member of the household might become a powerful shaman. (Mahar, 1960, p. 282)
Even if someone gets fever or some minor body ache, dizziness, fatigue, and so on, for that family Bhagat goes through the possession and tells the cause of the problem and its solution. It is believed that godling speak through family Bhagat and provide a solution.
COVID-19 and Sanitary Workers
The relation between COVID-19 and conditions of sanitary workers can be divided into three levels. These three levels can be—the relation between COVID-19 infection and their conditions; second, development of acute chronic illness due to COVID-19 and their conditions; and third, is COVID-19 spread and their conditions.
COVID-19 Infection and Sanitary Workers: As explained, while they work, they come into contact with different surfaces and waste products, which is highly risky. As per the nature of the COVID-19, it can stay few to several hours on different surfaces (Sohrabi et al., 2020), so when sanitary workers come into contact with such surfaces, the virus can enter their body. Waste products and used tissues and masks have a high possibility of carrying the virus, and when they deal with such waste, they come into contact, and through that it can enter their body. Through their hand it can go to their nose, eyes, or mouth and through that can enter inside the body and get infected.
They have two hours lunch break and again three hours duty. During the two hours break the worker from nearby goes to their home for lunch and remaining take their lunch at the workplace and take rest under the tree shade. Whoever goes home may take a bath or may not take a bath before having food. Taking bath reduced the risk of contamination, but not taking bath increase the risk of infection to the person as well as family members. Whoever does not go home, take their lunch without changing clothes, and without bathing, which increases the risk of COVID-19 infection for them. While taking rest with the same clothes, they touch multiple times their nose and eyes, which also increases their risk.
As we know protection is the only way to stop COVID-19 from spreading in a large community (Sohrabi et al., 2020). More than 98% of participants reported that they do not get any protective gear. In the present situation I could see, they are using masks, but after asking them I came to know some of interesting facts. They told me that they had been given only masks and not any other safety measures, which is single-use, after lunch break they have to use the same mask. That can increase the risk of COVID-19 infection. No soap or sanitizer made available to them, so while taking tea, snacks and lunch, they clean hands with plain water, which cannot clean the virus from hands.
Most sanitary workers smoke bidi, they feel frequent craving for smoking. While smoking, their hands touch their lips frequently. If their hand come into contact with COVID-19, viruses can easily enter their body. Someone might tell to ban their smoking, but practically it is not possible, even it can be more dangerous. If smoking is banned for them, they will still feel the craving to smoke and they might smoke hiding somewhere, which can compromise their hand washing and social distancing.
Result shows 62% of sanitary workers were illiterate, and only 8% studied up to 10th and above. They have high school dropouts, because of violence against them, social exclusion, discrimination and social stigma (Singh, 2014). This indicates that their awareness level is low, and their low education makes dissemination of information to them difficult. Their lack of awareness can lead to a lack of precautions and lead to COVID-19 infection.
Acute Chronic Illness due to COVID-19 and Sanitary Worker: Several conditions indicate that they are at high risk of developing acute chronic illness due to COVID-19 infection and further mortality. As per literature, human immunity has a very important role in controlling the acute chronic illness from COVID-19 infection (Li et al., 2020). Weakness of body immunity lead to chronic respiratory illness and high mortality.
Their work timings indicate that they do not take their breakfast or may take rarely, so for more than 18 hours—from dinner to lunch—they do not take meal except tea. That definitely affects their body immunity negatively and increases the risk of developing acute illness from virus infection. Therefore it indicates that if they get infected with COVID-19, most probably will develop acute chronic infection.
Their regular and dependent pattern of alcohol use increase extra pressure on their liver (Mandayam et al., 2004), and affect their food digestion system. Their body immunity gets weak due to a lack of digestion, which makes them vulnerable to developing severe acute illness due to COVID-19. Most of the workers who smoke also drink alcohol, which makes them a high-risk population. Because smoking during work increase the risk of getting an infection from COVID-19, and alcohol reduce their immunity, which can lead to severe acute infection and mortality. Another aspect is lockdown. Due to lockdown alcohol supply is not available, so sanitary workers with alcohol dependency are facing severe withdrawal symptoms. Because of withdrawal symptoms they get confusion, hand tremors, irritation, craving, and so on, which leads to poor hygiene and excessive use of tobacco smoking during their duty time.
Literature shows that sanitary workers suffer from several infections and diseases due to their working condition (Tiwari, 2008), the use of alcohol, and the use of tobacco (smoking and chewing) (Rangamani et al., 2015). More than 61% of the participants (scavenger/sweeper) reported one or more physical illness. So they are not only a high-risk population, but also have a high chance of developing severe acute illness due to already present physical illness.
Not only physical health, but they also have a high percentage of mental health problems due to long term social exclusion and social stigma. A study by Kumar (2017), reveals that more than 40% of scavenger/sweeper suffer from severe anxiety and depression. That can lead to poor hygiene and poor nutrition, which can lead to all three conditions—getting infected, spreading infection and getting severe acute illness from COVID-19 infection.
Community Level Spread of COVID-19 and Sanitary Worker: The biggest present fear of India is the community level spread of COVID-19. So it is important to understand the factors possibly responsible for community spread of COVID-19. In that case sanitary workers are very important because they are working day and night despite the country in complete lockdown. As it is a fact that sanitary workers are a high-risk group for getting the infection and developing acute chronic illness from infection. In that condition it becomes important to understand the factors associated with sanitary workers that possibly can lead to community spread.
Their living conditions show that social distancing is very difficult because staying and sleeping in one room will be close to each other, while filling water and going to the toilet at a commonplace they come in contact with each other. So on one side they are at high risk for contamination, on another side they are at very high risk of transmitting to each other making them high-risk groups. Their houses are adjacent to each other, and opening to a narrow street, increase the risk of community spread (The World Bank, 2019).
As most of sanitary worker smoke bidi, and frequently or maybe regularly have cough and throat infection. Therefore even if they get infected with the virus, differentiating symptoms will be difficult. So the chance of spreading in family and among co-workers is high because they do not come to know whether the symptoms are because of smoking or COVID-19.
As per the available literature, they are the least educated community (Kumar, 2014, 2017; Mohanty, 2014), which affects their awareness about COVID-19. Lack of education makes it difficult to get new knowledge about virus and other related factors. Because of that they do not practice all recommended advice and that increases the risk of infection and spread.
The community belief system also can be very risky for the community spread of COVID-19. As per their belief system, simple fever is caused by some uppriassar (spirit effect), and they seek solutions from their godlings. Therefore if they will not consider it as a medical illness caused by a virus, they will not go for medical check-up. Because of that other family members and community members will get infected.
Conclusion and Recommendation
COVID-19 can survive on any surface, while they work, sanitary worker comes into contact with different kinds of waste and surfaces. From there they can carry viruses and get infected. Their other occupational, educational, social, health, living standard and living conditions, make them vulnerable to develop severe acute illness, may lead to high mortality and community spread. Sanitary workers are one of the important pillars in maintaining public health, but if they become the risk for their health as well as public health, then what? The facts presented in this article show that, sanitary workers are playing a very important role in dealing with COVID-19 pandemic. But with that, this article also analysed the factors associated with sanitary workers which can take this pandemic to the community level. They are at high risk of getting infected and develop severe acute illness from COVID-19 infection. And their living conditions are highly risky for the spread of infection. Therefore it is very important to work on the factor presented in this article.
The author recommends providing some extra services and safety equipment to save their life and control the COVID-19 pandemic from spreading at the community level.
They should be given extra safety equipment, like providing 3 to 4 masks and gloves per day, restricting reuse of masks can reduce the risk of infection.
They should be clearly instructed about the dust containing a high chance of having the COVID-19 virus.
Personal soap or sanitizer should be given to the sanitary workers, so wherever they need to clean hands, they will be able to do.
They should be given some time duration for smoking or chewing tobacco if they are unable to control their craving. So they can be given sanitizing facilities before smoking or chewing tobacco and can reduce the risk of infection.
Whoever goes to their home for lunch, should be given clear instructions to keep their dresses separate from other clothes and other family members should not come into contact with that dress. After a proper bath only, they should have lunch, and avoid contact with family members. And who have food at the workplace, they should be given some facilities for taking a bath and changing clothes before lunch.
Another alternate can be shift duty, they will come and finish their work in a single shift, so the risk of middle break can be reduced.
Their morning duty timing should be started late so they can have breakfast and come to duty, or they should be given fruits and eatables at the workplace before starting their work.
They should be given complete knowledge about COVID-19 in their local language.
Their cultural beliefs are important, so that should be kept in mind while providing information to them.
Who already have some health problems, must be kept away from their risky workplace, without cutting their wages.
Their salary should be given on time so they can run their household and take proper nutrition to fight with COVID-19. Even they should be given extra payment because they are dealing with high-risk situations of life threat.
Regular screening of sanitary workers for COVID-19 symptoms should be done, and if found symptomatic should be cortile away from the home, and testing should be done. Because their houses mostly do not have enough space, so community spread is one of the risks.
Sanitary workers with alcohol dependency might face severe withdrawal syndrome, in such conditions they must be away from work and should be given emergency treatment.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.