
Abstract
This article makes a case for introducing actionable policy alternatives to address the human health hazards posed by agricultural use of pesticides in India. Pesticides, which include insecticides, rodenticides, herbicides, and fungicides, are widely used in global agricultural practices to protect crops from pest attacks. While pesticides are considered important for their role in boosting agricultural productivity and meeting global food security targets, the article argues that pesticides have a detrimental impact on human health both via occupational and non-occupational routes of exposure. It discusses the human health effects of prolonged pesticide exposure both in the international and national contexts. The article shows that despite a lower aggregate and per capita pesticide consumption vis-à-vis other countries at the national level, the use of agricultural pesticides in India has led to a disproportionate burden of premature deaths due to chronic diseases. By categorising the registered Indian pesticides as per the World Health Organization’s toxicity criterion, the paper argues that unregulated sale of both registered and unregistered pesticides must be addressed to counter the broader health hazards associated with pesticides in general, and the looming burden of chronic diseases that India is faced with in particular.
Keywords
Introduction
Pesticides, a term that encompasses insecticides, rodenticides, herbicides, and fungicides, are chemical compounds that are widely used in global agricultural practices to protect crops from pest attacks, augment agricultural productivity and meet the global targets of food security. The use of synthetic pesticides in agriculture and the realisation that they could harm human applicators and inflict damage on agricultural produce originally transpired around the same time in the nineteenth century (National Research Council, 2000). However, indiscriminate use of pesticides has continued in global agricultural practices. It is also worthwhile to highlight that the percentage increase in agricultural pesticide use has been more than twice as much as the increase in agricultural output. For instance, compared to the 35.3% increase in world cereal production, global pesticide use in agriculture proliferated by 76.3% between 1992 and 2018 (Food and Agriculture Organization (FAO), n.d.; 2020). 1 Although epidemiological evidence has increasingly highlighted the health hazards posed by rampant pesticide use in agriculture, the existing understanding on such implications has remained fragmented (Lam et al., 2017). Nevertheless, agricultural use of pesticides is regarded as a major environmental threat and is often associated with detrimental repercussions especially for soil and water ecosystems (Silva et al., 2019).
Agricultural use of pesticides is associated with a number of environmental hazards, which in turn generate negative consequences for human health. Certain agricultural pesticides are composed of persistent organic pollutants that inhibit the process of pesticide degradability and facilitate their environmental persistence for several years (Yadav et al., 2015). Due to their tendency to bioaccumulate and biomagnify, some pesticides have the potential to bioconcentrate by almost 70,000 times as compared to their initial concentration (Kim et al., 2017). Further, since a majority of pesticides used in agriculture belong to the broad-spectrum category of pesticides, a number of non-target organisms get adversely affected by indiscriminate pesticide use. It has also been argued that excessive pesticide use can make pests resistant to the impact of pesticides and cause substantial damage to biodiversity (Damalas & Eleftherohorinos, 2011).
Given that agriculture is often the principal economic activity in developing countries where a significant proportion of working-age population is engaged in agriculture, pesticide-induced health risks are considered to be more adverse for such contexts. For instance, according to Census 2011, the number of cultivators and agricultural labourers in India stood at 263.1 million and constituted 54.6% of the aggregate workforce (Ministry of Agriculture and Farmers’ Welfare, 2020a). In addition to cultivators and agricultural labourers who are occupationally and also directly exposed to the hazards of pesticide use, consumers of food crops are indirectly or non-occupationally predisposed to the harmful effects of pesticide residues.
While the issue of pesticide residues has been at the forefront of deliberations concerning international trade, concerns pertaining to excessive pesticide residues in food crops have increasingly garnered widespread recognition in the realm of environmental health (Gill et al., 2020). The impact of short-term or acute pesticide-induced toxicity typically manifests in the form of poisonings, irritation in the eyes, nausea and so forth. Such effects are easily identifiable and are usually prevalent among agricultural workers. On the other hand, hazards posed by prolonged or chronic exposure to pesticide residues are difficult to measure (Gill et al., 2020). Notwithstanding such challenges related to attribution and quantification, prolonged exposure to pesticides has been increasingly associated with deleterious human health effects such as cancers, immune suppression, endocrinal malfunctioning and neurological disorders (Gupta, 2004; Kim et al., 2017). Needless to emphasise, unabated pesticide use in agriculture may reverse the gains achieved in agricultural productivity and may increasingly render human beings and ecological systems vulnerable to toxic pesticides.
In 2018, agricultural use of pesticides for India was estimated at 58,160 tonnes. It is important to highlight that India’s annual pesticide consumption was considerably lower than China, the United States, Brazil and other major pesticide-consuming economies (FAOSTAT, 2021). In fact, India’s per hectare consumption of pesticides for the year 2014–2015 was estimated at 0.29 kg per hectare (kg/ha), which was insignificant compared to several other economies, such as China (13.06 kg/ha), Japan (11.85 kg/ha) and Brazil (4.57 kg/ha) (Subash et al., 2017). However, a recent study carried out by the Ministry of Agriculture and Farmers’ Welfare which entailed the analysis of 23,660 samples of food commodities concluded that 19.1% of the tested food samples contained pesticide residues and 2.2% of such samples contained pesticides above the prescribed threshold of maximum residues (Food Safety and Standards Authority of India (FSSAI), 2019). In addition to food crops, a substantial degree of evidence indicating the presence of chemical pesticides in groundwater exists for the Indian context (Sackaria & Elango, 2020; Somashekar et al., 2015). Thus, although the aggregate and per hectare use of agricultural pesticides is apparently trivial for India vis-à-vis other countries, challenges associated with direct pesticide exposure and indirect exposure via pesticide residues call for immediate corrective measures.
It is worthwhile to bring to the fore that concerns regarding the injudicious use of pesticides in agriculture have been expressed by various government committees in India. For instance, in August 2018, the Department-related Parliamentary Standing Committee on Health and Family Welfare took cognisance of the unrestricted use of agricultural pesticides and the health risks that agricultural intensification practices entail. The Committee urged the Ministry of Health and Family Welfare to formulate guidelines, and the Ministry of Agriculture to implement curbs for curtailing the use of pesticides in Indian agriculture (Rajya Sabha Secretariat, 2018). Similarly, the fifty-fourth report of the Standing Committee on Agriculture (2017–2018) noted that disproportionate use of pesticides is linked with the rising incidence of cancer and other diseases among agricultural workers in Punjab and other states. It asserted that by virtue of being biodegradable, pesticides present in the food chain have the potential to enter human blood stream, and thus emphasised on the need for promoting rational use of pesticides in agriculture (Lok Sabha Secretariat, 2018). Moreover, even though Indian regulatory bodies have restrained the use of certain agricultural pesticides over the last two decades, use of products derived from the banned chemical pesticides has persistently remained high (Sharma et al., 2014).
The central argument of the present article is that even though the use of pesticides in India is insignificant compared to the top-ten countries with highest pesticide use, health risks associated with prolonged pesticide exposure are substantial in India. This is because mortality due to chronic diseases caused by pesticides is on the rise in Indian states with the highest per capita consumption of agricultural pesticides. The article is divided into eight sections. Second Section describes the data and methods used in the article. Third Section reviews the existing literature to identify the health risks associated with agricultural use of pesticides. Fourth Section reviews the international and national evidence on the human health impact of prolonged exposure to pesticides. Fifth Section provides the empirical basis for this issue. Sixth Section discusses the regulatory structure for pesticides in the country. Seventh Section undertakes an assessment in terms of classifying the registered Indian pesticides as per the World Health Organization’s (WHO) toxicity criterion for pesticide classification. Moreover, it reiterates the need for government intervention. Eight Section provides policy alternatives and highlights potential challenges that may arise during their implementation. The last section is the conclusion.
Data and Methods
The present article uses secondary data for analysing the human health impact of pesticides in India. Data from the following sources has been used:
Directorate of Plant Protection, Quarantine and Storage, Government of India FAO database India State-level Disease Burden Initiative Population Division, United Nations Reserve Bank of India (RBI) Sample Registration System (SRS)
In addition to the above data sources, peer-reviewed literature from Google Scholar and PubMed was reviewed. Government reports, legislations, media articles and WHO’s toxicity criterion for pesticide classification (2020) were referred to for the current analysis.
Health Risks from Agricultural Pesticides
Human health risks associated with pesticide use emanate from both direct or occupational exposure, and indirect exposure linked with the presence of pesticide residues in food crops. Pesticides can typically affect human heath by entering human bodies through dermal, oral, ocular, and respiratory routes (Kim et al., 2017; Sharma et al., 2020). Although the routes of exposure play an important role in ascertaining the health risks from pesticide exposure, pesticide-induced health risks are also directly correlated with the amount of pesticide dosage, duration, frequency and intensity of exposure, and toxicity and persistence of pesticides (Damalas & Eleftherohorinos, 2011; Damalas & Koutroubas, 2016; Kim et al., 2017). In addition to these factors, environmental factors such as wind speed and humidity, determine the human health risks related to agricultural use of pesticides (Sharma et al., 2020). It is also argued that behavioural factors such as smoking and diet preferences could also explain the health effects associated with pesticide exposure. Since assessment of health risks attributable to pesticide exposure must take into account all such intervening variables, it is often difficult to accurately identify the human health impact of pesticide use in agriculture (Damalas & Koutroubas, 2016).
Compared to non-occupational exposure, the health risks associated with occupational exposure to pesticides are assumed to be much more substantial (Damalas & Koutroubas, 2016; Deziel et al., 2015). This is because pesticides have a higher potential to enter the bodies of agricultural workers and pesticide applicators through all the aforementioned routes of exposure. First, dermal exposure to pesticides is common among these workers as they routinely handle chemical pesticides which may enter the body through skin and exposed body tissues. Second, since chemical pesticides are composed of highly volatile substances, the risk of respiratory exposure and inhalation is higher among those engaged in agriculture. Third, pesticide applicators occasionally suffer from ocular ailments as chemicals constituents in pesticides often tend to rebound from food crops and cause severe ocular damage to applicators. Fourth, agricultural workers often become victims of pesticide poisonings that occur due to accidental ingestion of pesticides or their residues, which may remain on their hands post application (Kim et al., 2017; Sharma et al., 2020). In fact, poisoning resulting from ingestion of pesticides could be the most severe risk. According to data published by the National Crime Records Bureau on Accidental Deaths and Suicides in India, 6,962 deaths were caused by the accidental intake of pesticides in 2019 and accounted for the second-highest poisoning-induced deaths after snake bites (National Crime Records Bureau, 2020). While it may be easier to determine the routes of pesticide exposure in episodes of acute toxicity, ascertaining the exposure routes after prolonged periods of pesticide exposure could be challenging.
In contrast to workers employed in agriculture, consumers of food crops are exposed to pesticides mainly via the oral route, that is, through the ingestion of pesticide residues in food crops or drinking water. Further, when residential areas are in close proximity to agricultural farms, air pollution as an outcome of pesticide drift may cause residents to inhale volatile chemical substances present in pesticides (Damalas & Koutroubas, 2016). Even though health hazards accruing from occupational exposure to pesticides are more significant compared to non-occupational exposure, accurate understanding of routes of exposure and comprehensive analysis of modes of transmission could facilitate epidemiological analyses among non-agricultural populations, especially those in agrarian regions where pesticide consumption is high (Deziel et al., 2015).
Human Health Impact of Prolonged Exposure to Pesticides
Several studies have epidemiologically and statistically assessed the health effects of prolonged pesticide use in agriculture. In a majority of such studies, a common pathogenic mechanism through which pesticides affect human bodies is by increasing the level of oxidative stress. Simply put, oxidative stress refers to the imbalance between oxidant and antioxidant levels in the human body. An antioxidant response is triggered by the excessive production of oxidants, which subsequently leads to cell, tissue and organ damage (Moylan & Reid, 2007; Sharifi-Rad et al., 2020). The following diseases and health conditions resulting from prolonged pesticide exposure were identified in these studies:
Cancers
It is widely argued that the presence of carcinogenic substances in pesticides may be attributed to the limited understanding with respect to human carcinogenicity. This has in turn led to the massive production and easy availability of carcinogenic pesticides and elevated the risk of cancers among agricultural workers and the wider population (Alavanja et al., 2013). A number of studies have established the correlation between pesticide exposure and cancers. For instance, a study conducted in two American states—North Carolina and Iowa—which involved female spouses of pesticide applicators revealed that organophosphate insecticides distort endocrinal functioning in women, making them vulnerable to a number of hormonal cancers such as breast, thyroid and ovary (Lerro et al., 2015). Results from a case-control study from several hospitals in Pakistan showed that pesticide exposure is positively linked with the incidence of lung cancer (Luqman et al., 2014). In a population-based case control study conducted in southwestern France, occupational exposure to pesticides was found to be significantly associated with the risk of developing brain tumours (Provost et al., 2007). A study carried out in the Yucatán state of Mexico reported the presence of organochlorine pesticides in the blood samples of Mayan women suffering from uterine cervix cancer. The study ascribed the disease to the contamination of groundwater by pesticides (Rodríguez et al., 2017). It has also been contended that pesticides have the potential to stimulate malignant alteration of genes linked with cancer (Vakonaki et al., 2013).
With respect to the Indian context, a number of studies have identified pesticide exposure as the leading risk factor for the rising incidence of cancer cases, particularly for the state of Punjab. For instance, in a study that compared oxidative stress levels between occupationally-exposed and unexposed population groups in the Bathinda district of Malwa region, commonly referred to as the ‘cancer belt of Punjab’, higher oxidative stress level and accumulation of pesticide residues were observed in the exposed population segment (Kaur et al., 2018). Moreover, in a separate study conducted in the Talwandi Sabo Block in Bathinda district, residues of a banned pesticide (endosulfan) were detected in the blood samples of healthy women employed in agricultural activities (Sharma et al., 2019). In Kerala, cancer cases in the vicinity of cardamom plantations of the state and paddy fields of Kuttanad have often being associated with excessive pesticide use (Indira Devi, 2007). In a Varanasi-based hospital, abnormal levels of pesticide concentrations were found in hospitalised patients suffering from gallbladder carcinoma, and the disease was attributed to the contamination of drinking water with agricultural pesticides (Shukla et al., 2001).
Chronic Respiratory Diseases
A sufficient degree of evidence has assessed the link between pesticide exposure and chronic respiratory diseases such as asthma, impaired lung function, chronic bronchitis and chronic obstructive pulmonary disease (COPD). For instance, a cross-sectional study that encompassed 1,379 agricultural workers in Brazil found that pesticide exposure was positively linked with a higher prevalence of asthma among people employed in agriculture (Faria et al., 2005). Similarly, a cross-sectional study conducted among 1,939 male farmers in the Saskatchewan province in Canada revealed that self-reported asthma was related with the use of a particular type of insecticide (Senthilselvan et al., 1992). A cross-sectional study carried out among female indigenous plantation workers in Costa Rica found that exposed plantain plantation workers had a higher prevalence of wheezing and shortness of breath compared to non-exposed female workers who worked at organic banana plantations and or other places which did not expose them to pesticides (Fieten et al., 2009). Moreover, a study conducted in California established that the use of elemental sulfur, which is one of the oldest pesticides used in the world, has unfavourable consequences on the respiratory health of children living in proximity to agricultural fields (Raanan et al., 2017).
Similar evidence exists for certain Indian states. For instance, a cross-sectional study conducted with a sample of 166 pesticide applicators in Lucknow observed that unprotected pesticide exposure is associated with adverse respiratory outcomes and reduced functioning of the lungs (Fareed et al., 2013). Likewise, a study carried out among 376 non-smoking agricultural workers in rural areas of West Bengal showed that prolonged exposure to pesticides is linked with impaired functioning of the lungs, COPD and other symptoms indicating the presence of respiratory diseases (Chakraborty et al., 2009).
Cardiovascular Diseases
A significant body of evidence has established that the risk of developing cardiovascular diseases increases with pesticide exposure. For instance, a retrospective cohort study that used data from National Health Insurance Research Database in Taiwan demonstrated how chronic exposure to organophosphorus pesticides is associated with higher susceptibility to arrhythmias, coronary artery disease and congestive heart failure. The study attributed the adverse health consequences to the malfunctioning of cardiac muscles, which results in oxidative stress (Hung et al., 2015). A study conducted among farming communities in Tunisia concluded that pesticides augment the risk of cardiovascular diseases in exposed populations by disrupting the activity of a particular gene, known as paraoxonase, which checks the level of oxidative stress and manages the production of high-density lipoproteins or good cholesterol (Wafa et al., 2013). A cohort assessment that included 7,557 Japanese-American men corroborated the findings of similar studies by concluding that long-term exposure to pesticides is linked with a higher incidence of cardiovascular diseases (Berg et al., 2019).
In the Indian context, a study conducted among 60 visibly healthy male agricultural workers in Karnataka observed abnormalities in electrocardiogram indicators of these workers. It confirmed that despite remaining asymptomatic for prolonged durations, pesticide exposure of farm workers could lead to deaths attributable to cardiovascular diseases (Sunitha et al., 2020). A self-reported health assessment of 248 male agricultural workers in Sagar District of Madhya Pradesh concluded that approximately 17% of workers experienced symptoms linked with cardiac issues (Kori et al., 2018).
Endocrine Diseases
A significant amount of evidence on the endocrine-disrupting properties of pesticides has emerged in the recent past. For instance, a large-scale population-based case control study that involved 45,050 cases including pregnant women and male children from ten districts of Andalusia in Spain established that gestational exposure of women to certain pesticides may cause disorders such as low birth weight and miscarriage, inhibit foetal growth and lead to male congenital genitourinary/urogenital deformities (García et al., 2017). A population-based case control study undertaken among 866 farmers who suffered from diabetes mellitus in the Bang Rakam district of central Thailand showed that diabetes prevalence had positive linkages with exposure to various agricultural pesticides (Juntarawijit & Juntarawijit, 2018). Similar observations were made in a small-scale exploratory study conducted among 40 diabetic patients in Korea with low-dose organochlorine pesticide exposure (Son et al., 2010). Moreover, presence of organophosphorus pesticides in the form of residues in food commodities has been increasingly known for exerting adverse effects on the neuroendocrine system, which is vital for maintaining a healthy metabolism and regulating the level of growth and reproductive hormones in human beings (Yang et al., 2019).
Like global evidence, epidemiological studies showing the impact of pesticides on endocrinal diseases is gradually evolving in India. A study conducted in Lucknow showed that occupational exposure to pesticides led to distorted blood, liver and kidney biomarkers among 60 pesticide applicators who worked in mango plantations (Jamal et al., 2016). Results of a separate study undertaken in a tertiary health care research institute in Lucknow with 70 women who had suffered from two or more miscarriages in the past highlighted that pesticide exposure was related to elevated risk of repeated pregnancy loss, which may be regarded as a manifestation of endocrinal malfunctioning (Pandey et al., 2020). The impact of pesticides on endocrine system may also be verified by studies that have detected the presence of pesticide residues in human breast milk samples in agrarian states of Punjab (Bedi et al., 2013) and Haryana (Mehta et al., 2020). Furthermore, a recent case-control study conducted among non-glucose intolerant, pre-diabetic and diabetic participants concluded that presence of pesticides in groundwater could enhance the population’s susceptibility to type 2 diabetes mellitus (Tyagi et al., 2021).
Empirical Basis
The issue of injudicious use of agricultural pesticides and the health hazards that originate from such use merit stringent and effective government interventions. Even though the Indian government has taken several measures to curb pesticide use in agriculture, including the ban of certain lethal pesticides, stepping up of government measures is the need of the hour. The rationale for augmented government intervention is established in this section using data from various sources.
Figure 1 shows the gross cropped area (GCA, in ’000 hectares) and pesticide consumption (MT technical grade) from 1999–2000 to 2015–2016 for Punjab, Haryana, Maharashtra, West Bengal and Kerala—states which had the highest per capita consumption of agricultural pesticides in 2015–2016. 2 While GCA increased for all five states with the exception of Kerala, pesticide consumption rose dramatically for Maharashtra in 2015–2016, although a significant decline was reported in 2008–2009 as compared to 1999–2000 and 2003–2004. In Uttar Pradesh, pesticide consumption recorded a steady increase in 2008–2009 and 2015–2016. In 2003–2004 and 2008–2009, pesticide consumption in Kerala decreased substantially as compared to 1999–2000 but increased close to the 1999–2000 level in 2015–2016. While pesticide consumption reduced systematically for Punjab and Haryana between 1999–2000 and 2015–2016, West Bengal registered a substantial decline in pesticide consumption in 2015–2016, especially with respect to the 1999–2000 level.
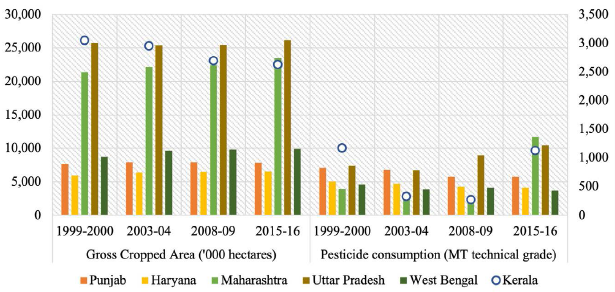
Figure 2 shows the per hectare pesticide consumption in agriculture (in kg) for these states from 1999–2000 to 2015–2016. Since, per hectare consumption measures the intensity of pesticide use in a given geography, it is a more precise measure of pesticide use compared to the aggregate consumption data. At the national level, India’s per hectare pesticide consumption in 2015–2016 was equivalent to the level recorded in 1999–2000, albeit the declines recorded in 2003–2004 and 2008–2009. Similar to the observations made in Figure 1, per capita pesticide consumption in agriculture for Punjab and Haryana fell notably in 2015–2016 and was substantially lower for both the states as compared to 1999–2000. The per capita pesticide use showed a major increase for Maharashtra and Kerala in 2015–2016, particularly in comparison with the levels registered in 2008–2009. The per capita agricultural use of pesticides rose gradually with respect to the 1999–2000 level for Uttar Pradesh, whereas West Bengal showed a significant reduction.
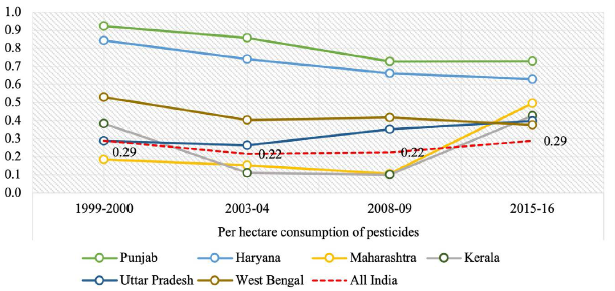
Figure 3 shows the percentage distribution of deaths by broad age groups for the selected Indian states in 2016. The underlying notion behind such a representation is to evaluate the status of health for Indian states with respect to the level of premature mortality, that is, deaths that occur before the age of 60 years. Although the threshold for premature mortality is often assumed to be up to the age of 65 or 70 years in the international context, data available from the SRS in India does not report the percentage of deaths that occur after the age of 70 years. Therefore, from the perspective of present analysis, deaths that occur before the age of 60 years are regarded as premature. A higher percentage of deaths in 0–14 and 15–59 age groups denotes that a lower percentage of people are able to survive up to ages 60 and above. Although a majority of Indian states have made significant strides in terms of reducing mortality between 0 and 14 years, particularly due to nationwide efforts aimed at controlling under-5 morbidity and mortality, deaths in the 15–59 age group are particularly higher for Punjab, followed by Uttar Pradesh, Haryana and Maharashtra. It is also important to highlight that although deaths in the 0–14 years age group may be attributed to more preventable factors such as inadequate sanitation, contaminated drinking water, malnutrition and injuries, deaths in the 15–59 years age group in developing countries are mostly caused by chronic diseases such as cardiovascular diseases, cancers, and respiratory diseases. A disproportionately high proportion of deaths in the 15–59 years age bracket signifies a looming burden of chronic diseases that may not be easily addressable by health systems of developing countries. While Kerala seems to have considerably curtailed its burden of premature mortality, which may be attributable to its progressive health care system and advanced stages of demographic transition, a higher percentage of deaths in the 15–59 years age group for Punjab, Uttar Pradesh, Haryana, Maharashtra and West Bengal is representative of the threat posed by chronic diseases that must be addressed. Given the relatively higher fraction of deaths in the 0–14 years age group for Uttar Pradesh and Haryana, it may be convincingly deduced that the impending burden of chronic diseases coexists with preventable primordial health conditions in these states.
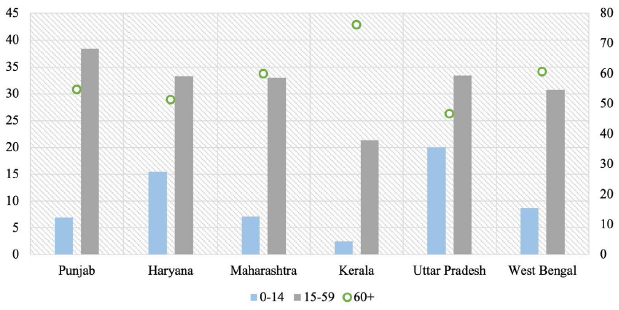
Figure 4 shows the causes of death in the 40–69 years age group for the selected Indian states in 2016. While cardiovascular diseases accounted for the maximum proportion of deaths, cancers were the second leading cause of death in this age group, particularly for Kerala and Haryana. Chronic respiratory diseases accounted for a significant share of deaths in Uttar Pradesh and Haryana while diabetes/urogenital/blood/endocrine diseases were identified as major killers in Punjab and Kerala. Figure 5 represents the causes of death in the 15–39 years age group in 2016. Although injuries, accidents and self-harm constituted a substantial percentage of deaths in this age bracket and are indicative of pesticide-related deaths caused by accidental or deliberate poisonings, cardiovascular diseases, cancers and diabetes/urogenital/blood/endocrine diseases caused a significant fraction of deaths in the 15–39 years age group. Cardiovascular diseases were responsible for a major share of deaths in Punjab, Haryana, and West Bengal while cancers emerged as the leading cause of death in Kerala and Haryana among people in the 15–39 years age group. Proportion of deaths attributable to diabetes/urogenital/blood/endocrine diseases among people aged 15–39 years were the highest in Punjab and Kerala.
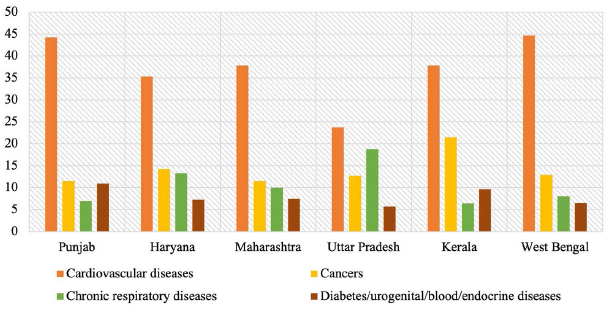
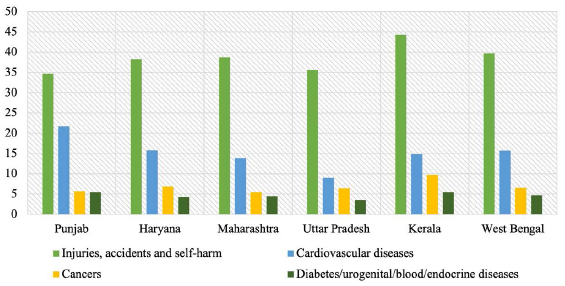
Figure 6 shows the average amount (in tonnes of active ingredient) and percentage of pesticide consumption in agriculture by India along with top-ten pesticide consuming countries in 2015–2016. China (mainland), the United States and Brazil accounted for 62% of the global agricultural pesticide use, whereas India’s pesticide consumption was much lower even with respect to the aggregate amount of pesticide used in agriculture by Spain, which accounted for the lowest share of pesticide consumption in agriculture among the top-ten countries.
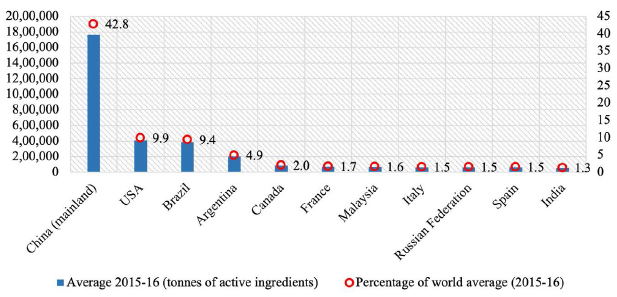
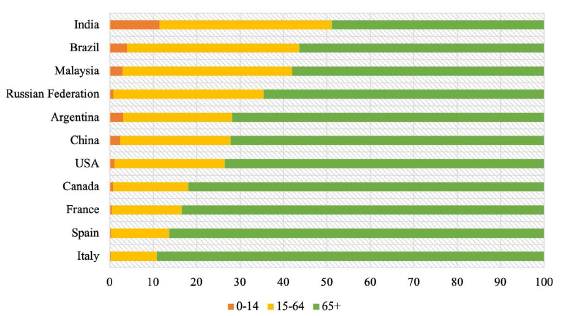
Figure 7 presents the estimates for percentage distribution of deaths by age groups for 2015–2020. As mentioned before, a higher share of deaths in the under-60/65/70-year age groups represents an increase in the burden of premature mortality and reduced potential in terms of surviving up to older age groups. As represented in Figure 7, India’s proportion of deaths in the 65 plus age group is the lowest vis-à-vis the top-ten pesticide consuming countries, indicating a higher burden of mortality in earlier age groups. Given that a considerable proportion of deaths in the selected Indian states (with the exception of Kerala) occurred in the 15–59 years age group (Figure 3) and a significant percentage of deaths in the 40–69 years and 15–39 years age groups was attributed to chronic diseases in 2016 (Figures 4 and 5), morbidity and mortality accruing from these diseases must be addressed from the perspective of reducing premature mortality among Indians. Furthermore, unlike other countries, India’s share of deaths in the 0–14 years age group is the highest for India as compared to other countries (Figure 7), thereby implying that in addition to tackling the burden of chronic diseases among higher age groups, India has to intensify efforts to address the causes of child and adolescent mortality. Therefore, despite a lower aggregate and per capita pesticide consumption vis-à-vis other countries, the burden of premature mortality attributable to chronic diseases is higher in India vis-à-vis other countries. The status quo calls for urgent government interventions to address the risk factors of excess morbidity and mortality, especially in the 15–59 years age group. It is also worthwhile to reiterate that in 2015–2016, per hectare pesticide use was substantially above the national average (Figure 2) for all the selected states. Even though there have been intermittent declines in per hectare pesticide use in agriculture at the national level, the 2015–2016 level was exactly equivalent to the level reported in 1999–2000.
Therefore, it is reasonable to conclude that prolonged pesticide exposure leads to detrimental health outcomes. Such impact typically manifests in the form of chronic diseases discussed in third Section. Moreover, as mortality and morbidity reporting systems in the country suffer from a host of challenges, the estimates of mortality due to chronic diseases, represented in Figures 4 and 5, may not depict the enormity of the actual disease burden. Even though several sources of data have been used to arrive at estimates shown in Figures 4 and 5, the collaborators of the study (ICMR, PHFI and IHME, 2017) have acknowledged the deficiencies that exist in Indian data reporting systems (Dhillon et al., 2018).
First, since only an insignificant proportion of registered deaths are medically certified, Medical Certification of Cause of Death (MCCD) data does not provide an accurate impression of the disease burden in the country. For instance, only 21.1% of total registered deaths were medically certified in India in 2018 (Office of the Registrar General of India, 2020). Second, even in cases where the death is medically certified, the underlying cause of death remains unknown and only the immediate cause is reported (Rukmini, 2020). Third, the present coverage of verbal-autopsy based reporting under SRS, which is regarded as a reliable method of determining actual cause of deaths, is currently inadequate (Krishnan et al., 2020). Fourth, incorrect data coding due to limited training of human resources is a major impediment to generating accurate mortality and morbidity statistics in India (Dhillon et al., 2018). Fifth, diseases such as cancers for which disease registries have been established to capture the actual disease burden are primarily confined to urban areas and hence have limited coverage (Behera & Patro, 2018). Further, inaccuracies in urban cancer registries have raised concerns over the quality and reliability of morbidity data (Smith & Mallath, 2019).
Finally, dearth of advanced diagnostics contributes substantially to data under-reporting and misclassification for complex diseases such as cancers (Dhillon et al., 2018; Singh et al., 2018). For instance, Mahal et al. (2006) note that in addition to the inadequacy of medical diagnostics, the geographic distribution of advanced diagnostic facilities in India is skewed. Shortage of diagnostic facilities combined with inefficient utilisation of diagnostics in public health care facilities have led patients to seek diagnostic services from private health care facilities (Barik & Thorat, 2015; Mahal et al., 2006). Rajpal et al. (2018) highlight that cancer prevalence in India is suggestive of an underlying income gradient in that richer households report a higher incidence of cancer. One possible explanation for this phenomenon is that since urban areas have a higher concentration of diagnostic and screening facilities, richer households report higher prevalence of cancer. Although data for medical diagnostics in India are only sparsely available, Statista data from April 2019 to March 2020 indicates that the Indian diagnostic industry is dominated by the private sector. During this period, around 200 million tests were performed for over 64 million patients by four private sector diagnostic companies (Statista, 2021). Since there is limited provision of data sharing by privately-owned diagnostic companies, it is difficult to accurately measure the burden of complex diseases and ascertain their causes and risk factors.
Regulatory Situation of Pesticides in India
The Insecticides Act, 1968 and Insecticides Rules, 1971 provide the regulatory framework for the use of pesticides in India. While Pesticide Management Bills of 2008, 2017 and 2020 were proposed with the intention of repealing the Act, these have not yet been passed by the Indian Parliament (Bonvoisin et al., 2020; Pesticide Management Bill, 2020). Instituted under Section 4 of the Insecticides Act, Central Insecticides Board and Registration Committee (CIBRC) of the Department of Agriculture, Cooperation and Farmers’ Welfare, Government of India, plays an important role in various aspects including administering the Act, governing manufacture, sale and distribution of pesticides and providing guidance to both the Central and state governments on human and animal health risks posed by pesticide use and measures that may pre-empt such risks (Department of Agriculture, Cooperation and Farmers’ Welfare, 2020). Furthermore, the onus of registration of pesticides manufactured domestically or imported by India, after evaluating the efficacy and efficiency of pesticide compounds, rests with the CIBRC (Devi et al., 2017). As of 1 March 2021, 293 pesticides are registered for use in the country (Department of Agriculture, Cooperation and Farmers’ Welfare, 2021). Although the Insecticides Act, 1968 does not contain provisions for periodic assessment of pesticides, safety of specific pesticides may be evaluated by expert committees, which may subsequently prescribe curbs or bans (Bonvoisin et al., 2020). The FSSAI, a statutory body under the Ministry of Health and Family Welfare, Government of India, is responsible for determining and monitoring the maximum residue limits (MRLs) of pesticides in food products (Devi et al., 2017).
A crucial aspect of the Indian pesticide regulations is that the Insecticides Act provides inadequate authority to states to regulate pesticide use (Bonvoisin et al., 2020). In addition to the Act, the Pesticide Management Bill, 2020 lacks an emphasis on decentralised authority and recommends giving complete regulatory authority of the Indian pesticide industry to the Central government. In fact, the Bill’s clause on ‘Declaration of expediency of Union Government’ reinforces the authority of the Central government of India over regulation of pesticide use in the country. As per the clause,
‘…it is expedient in the public interest that Union should take under its control the regulation of pesticide industry to the extent hereinafter provided (The Pesticide Management Bill, 2020, p. 2)’.
It is also important to note that under the Insecticides Act, state governments are capacitated to impose only temporary bans to curtail the use of pesticides in states and these bans may range from 60 to 90 days (Bonvoisin et al., 2020). However, state governments have the power to curb the use of unsafe pesticides by rejecting applications for license renewal of such pesticides. For instance, Punjab banned the use of 20 pesticides through this route in 2018. Similarly, the state government of Kerala denied renewal of licenses for sale and distribution of glyphosate in 2019 (Chakraborty, 2018; Rajwi, 2020). Although the government of Sikkim has set an example for other states and countries in terms of successfully banning the import, sale and use of chemical pesticides in agriculture, this could be distinctly attributed to the ecological fragility of the state. Efforts to transform Sikkim into an organic state commenced in 2003 by introducing subsidy cutbacks on chemical pesticides. Subsequently, the Sikkim Agricultural, Horticultural Input and Livestock Feed Regulatory Act was passed in 2014 to implement legal sanctions against unauthorised use of inorganic inputs for agricultural and horticulture use, and as livestock feed. However, it is often argued that pesticide ban in Sikkim could be effectively enforced because the state is not a major agrarian state and largely relies on West Bengal for meeting its demand for food commodities (Taneja, 2017).
Classification under WHO’s Toxicity Criterion for Pesticides
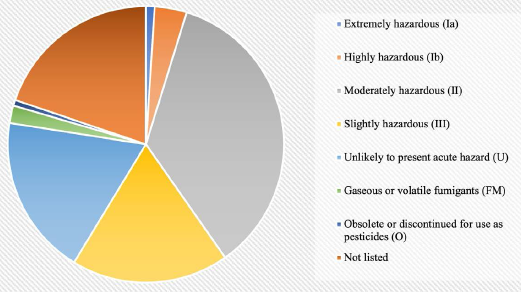
WHO’s Toxicity Criterion for Classification of Pesticides.
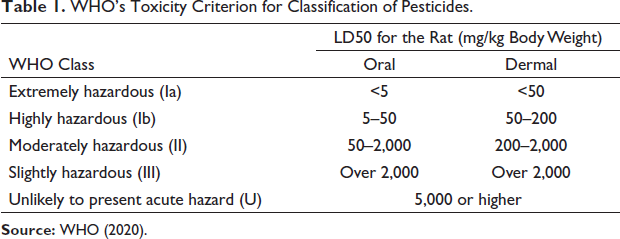
For the current analysis, the 293 pesticides registered for use in the industry were classified as per the WHO criterion. As shown in Figure 8, 104 pesticides, which constitute a significant share of pesticides registered in the country, fall in the ‘moderately hazardous (II)’ category. While 54 pesticides belong to the ‘slightly hazardous (III)’ category, 11 pesticides form a part of the ‘highly hazardous (Ib) category’ and 3 pesticides that are used in the country fall in the ‘extremely hazardous (Ia)’ category. Furthermore, 2 pesticides which continue to be used in the country have been designated as ‘obsolete or discontinued for use’ and 6 pesticides are a part of gaseous or volatile fumigants. It is also important to note that 58 pesticides registered in India do not currently exist in the WHO’s criterion for toxicity classification of pesticides. In fact, even the 55 pesticides that exist in the ‘Unlikely to present acute hazard in normal use’ category are seldom used in safe proportions. This is primarily due to inefficiencies associated with marketing of pesticides in the country, which has led to a disproportionate expansion of the role of private sector in the sale of pesticides. While pesticide manufacturers are not commonly engaged in the direct sale of pesticides to farmers, episodes of sales demonstrations to boost direct sales to farmers are often reported (Devi et al., 2017). Moreover, instances of sales of even unregistered pesticides in the country are frequently brought to the fore by the Indian media (Chari, 2018).
In addition to challenges associated with the direct sale of pesticides, the marketing landscape of pesticides in India is marred with problems concerning retail sale of pesticides. It is worthwhile to mention here that with the exception of certain North-eastern states where retail sale of pesticides is managed by the public sector, approximately 90% of such sale is dominated by the private sector (Devi et al., 2017). Since private sector monopolisation is typically driven by profits, such retailers often engage in unregulated sale of banned pesticides and misinformed sale of registered pesticides to farmers. By virtue of being the first point for pesticide procurement, private retail sellers can considerably influence decisions of farmers with respect to pesticide application. A number of studies have highlighted that farmers rely on private pesticide dealers for seeking information on patterns of pesticide use. For instance, a study conducted in 28 districts of 12 states showed that only 20% of farmers seek guidance on plant protection from authorised agricultural extension officers while 80% depend on suspicious sources for such information (Shetty et al., 2010). In an investigation conducted in four states, namely Karnataka, Maharashtra, Andhra Pradesh and Punjab, it was found that farmers in Karnataka and Andhra Pradesh relied extensively on pesticide company representatives and dealers for advice related to plant protection (Shetty, 2004). Therefore, overuse and irrational use of agricultural pesticides may be regarded as the outcome of inordinate involvement of private dealers in the retail sale of pesticides in the country. The issue must be duly addressed to tackle a myriad of health hazards associated with pesticides in general, and the looming burden of chronic diseases that the country is faced with in particular.
Policy Alternatives and Challenges Related to Their Implementation
A number of measures may be taken to curb the use of pesticides in the country and minimise their adverse impact on human health. For instance, the use of personal protective equipment (PPE) should be made legally binding for pesticide applicators and farmers. Directives for accurate labelling and packaging of pesticides may be issued to inform safe usage and storage. Similarly, with a view to limit direct sales to end users, pesticide regulations should aim at restraining promotion and advertisement of pesticides by pesticide manufacturers. All such efforts may be supplemented by frequent, small-scale surveys to determine how effectively they are being rolled out in different parts of the country. Moreover, pesticides that fall under the ‘extremely hazardous’ and ‘highly hazardous’ category of the WHO’s criterion should be gradually banned in the country. There should also be provisions to periodically assess the safety of pesticides being used in agriculture. While there is limited discussion in the existing pesticide regulatory structure with respect to the ‘polluter pays’ and ‘precautionary’ principles of environmental policy, these could provide important bases for registration and manufacture of pesticides from the perspective of protecting human health (Khurana & Kumar, 2020). For instance, in line with the ‘precautionary principle’ of environmental policy, pesticides with potentially harmful consequences for the health of farmers and consumers should not be registered by the CIBRC. Likewise, since ‘the polluter pays’ principle calls for levying heavy penalties on agents causing environment pollution, pesticides leading to deleterious human health effects should be banned and their manufacturers be made to compensate for the damage caused. Even though persistent attempts to repeal the Insecticides Act, 1968 are being made and the Pesticide Management Bill, 2020 does make occasional references to some of these proposals, due recognition of such measures is important from the perspective of limiting pesticide use and safeguarding human health against reckless pesticide use in agriculture.
While the aforementioned measures merit attention of public authorities, two actionable policy alternatives are discussed below along with some potential challenges that may exist while implementing them. Since state governments in India have limited authority, these alternatives are proposed for consideration of the Central government.
Overhauling Marketing Landscape for Pesticides: Stepping-up the Role of Government
In order to regulate retail sale of pesticides, the public sector must expand its presence in this domain. Since almost 90% of this sector is governed by the private sector which negatively influences the use of pesticides by farmers, the public sector could play an important role in regulating the retail sale of pesticides in Indian states. Unlike private dealers, the personnel employed in such outlets do not have an underlying objective to maximise sales and profits and thus, increase in the number of public sector retail outlets for pesticides could help in curtailing overuse of pesticides by Indian farmers. This could in turn generate a positive impact on health of farmers as well as consumers of food products. With greater involvement of the public sector, farmers could increasingly rely on authorised agricultural extension officers for seeking information on the use of pesticides. This could lead to a progressive decline in the influence of private dealers on farmer decisions.
Even though several benefits may accrue from changing the marketing landscape for pesticides by augmenting the role of public sector in retail sale of pesticides, two foreseeable challenges exist in its implementation:
Breaking the hegemony of the private sector: Stepping-up the role of government in retail sale of pesticides would imply breaking the hegemony of the private sector. While this issue could be addressed by recognising concerns related to the existing marketing structure by amending the Insecticides Act, 1968 or by introducing similar provisions in the Pesticide Management Bill, 2020, an expected outcome of such a policy alternative is that it would meet with strong resistance from the private sector, which governs bulk of the retail sale of pesticides in India.
Cost-intensive: Expansion of public sector retail outlets in Indian states is a cost-intensive process and would have important implications for both Central and state agricultural budgets. This is because substantial investments in terms of setting-up infrastructure and employing the required number of personnel would be needed to accomplish this process in all states. This could act as a major deterrent to increasing the presence of public sector in the realm of pesticide sales.
Increasing the Uptake of Biopesticides in Indian Agriculture
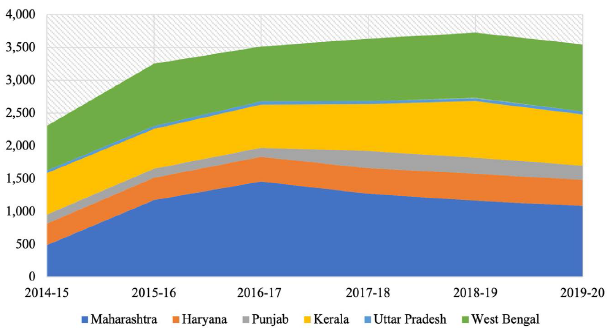
Biopesticides offer a promising alternative to synthetic pesticides. Since biopesticides are made from organic substances such as plants and microorganisms, their agricultural use is considered safe for environment and human health. While the market for biopesticides has considerably expanded in India and other parts of the world particularly since the last one decade, biopesticides have not been able to serve as effective substitutes to synthetic pesticides. As represented in Figure 9, although the use of biopesticides in Maharashtra, West Bengal and Kerala from 2014–2015 to 2019–2020 presents an optimistic scenario, the limited uptake of biopesticides in Punjab, Haryana and Uttar Pradesh shows the Indian farmers’ excessive dependence on synthetic pesticides. The Government of India can assume an important role in terms of sensitising the farmers about the benefits of biopesticides and in addressing apprehensions and concerns over biopesticides’ use among farmers. Some of the challenges that Indian farmers face with respect to the use of biopesticides instead of chemical pesticides have been documented in recent scholarly research:
Lower efficacy: Quality issues associated with biopesticides such as insufficient microbial count lead to lower efficacy of such substances in comparison with chemical pesticides, which ultimately lead to undesirable agricultural outcomes (Kumar et al., 2019). This is often regarded as a major factor behind the sluggish growth of biopesticide industry.
Limited shelf life: Since biopesticides are derived from natural substances, they have a limited shelf life (Mishra et al., 2015). Active ingredients of biopesticides rapidly lose their potency in the natural environment. Availability of adequate refrigeration is hence a prerequisite to sustain the shelf life of biopesticides, which is virtually missing in rural areas of India.
Complex registration process: The process of registration of biopesticides is a time and cost-intensive process and is based on obsolete toxicological requirements. In fact, surge in fake or unregistered biopesticide products in the Indian market is often attributed to the cumbersome registration process that these products involve (Kumar et al., 2019).
Inadequate tenacity: Unlike chemical pesticides, biopesticides lack tenacity on agricultural fields, a challenge that is compounded due to exposure to high levels of ultraviolet rays (Aneja et al., 2016). More frequent application is hence an inevitable requirement for farmers who choose biopesticides over chemical pesticide formulations.
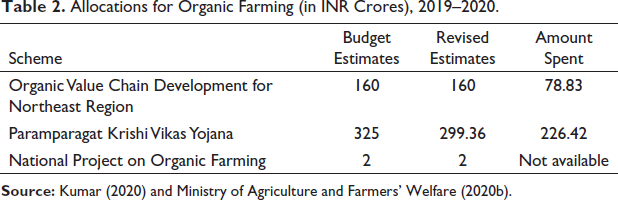
Allocations for Organic Farming (in INR Crores), 2019–2020.
Concluding Remarks
Pesticide use in agriculture is associated with negative effects, both for the environment and human health. The existing understanding on environmental health implications is fragmented and there are challenges related to establishing the impact of prolonged pesticide exposure on human health. However, compelling linkages may be drawn from the existing evidence on pesticide use in Indian states and mortality burden attributable to chronic diseases, particularly among premature age groups. It is also worthwhile to reiterate that despite India’s lower aggregate and per capita pesticide consumption vis-à-vis other countries, the burden of premature mortality attributable to chronic diseases is higher in India vis-à-vis other countries. Similar concerns related to rampant pesticide use in agriculture have also been expressed in recent political discourse in India, such as the Department-related Parliamentary Standing Committee on Health and Family Welfare (August 2018) and fifty-fourth report of the Standing Committee on Agriculture (2017–2018). Furthermore, it is important to highlight that due to deficiencies in mortality and morbidity reporting systems, the burden of chronic diseases reflected in the existing empirical evidence may be regarded as an under-representation of the actual disease burden.
Given that the regulatory structure for pesticides in India is governed by the Insecticides Act, 1968 which provides inadequate authority to states to regulate pesticide use, the Central government should adopt measures to curtail the unregulated, unauthorised and misinformed use of pesticides in Indian agriculture. Regulatory responses such as gradually phasing out the use of pesticides that fall under the ‘extremely hazardous’ and ‘highly hazardous’ category of the WHO’s toxicity criterion as well as incorporating the ‘polluter pays’ and ‘precautionary’ principles of environmental policy in the context of pesticide use must be given due recognition by the Government of India. The present article proposes two policy alternatives which are: overhauling the current marketing landscape for pesticides, which disproportionately empowers the private sector in retail sale of pesticides, and promoting the uptake of biopesticides among Indian farmers, which is far from sufficient given the current consumption estimates. By curbing the excessive use of chemical pesticides in agriculture, these measures have the potential to address the threat posed by chronic diseases among premature age groups in India.
Footnotes
Acknowledgements
The author would like to thank the editor and two anonymous reviewers for their useful comments.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.