
Abstract
Decentralisation was one of the more visible changes in Western welfare states from the 1970s to the 2000s and was viewed by some as an unstoppable trend. However, during the Great Recession, governmental responses to certain policy problems have called into question the decentralisation process through a series of recentralising changes in territorial governance in several multilevel systems. This article seeks to understand whether and how the territorial governance of the Welfare State has experienced a process of recentralisation by identifying and measuring three of its dimensions in the Spanish case. This is done by constructing an index of Social Policy Recentralisation (SPREI) and applying it to the healthcare and long-term care policies in Spain between 2010 and 2016. We observe a recentralisation process in the policies analysed with a differentiated scope and intensity in the different dimensions reflected in the proposed index.
Introduction
In the last 30 years of the twentieth century, subnational governments (SNGs) gained ground in the various dimensions of welfare state policymaking, even in unitary systems. This shift pursued the aims of improving the quality of public services and enabling them to become more agile, efficient, innovative and responsive to diverse citizens and territorial demands (see Kazepov, 2010; Obinger et al., 2005). In the early twenty-first century, the World Bank (2000) stated that decentralisation continued to appear to be unstoppable. Some subsequent analyses of the expansive policies implemented during the early years of the Great Recession initiated in 2008 pointed in the same direction (OECD/KIPF, 2016; Hooghe et al., 2016).
However, the impact of the latter phase of the Great Recession, between 2011 and 2015, on the territorial governance of social protection systems is far from clear. On the one hand, concerns for new policy problems, both related to economic efficiency and social justice, seem to have encouraged Central Government’s (CG) actions affecting the very tenets of decentralised welfare. First, to balance national accounts, especially in governments that received supranational bail-out funds, economic responses were accompanied in many cases by an increase in the conditionality of intergovernmental transfers, and the implementation of stricter fiscal rules reflecting a reduction in subnational social policymaking and fiscal financial management autonomy (Canavire-Bacarreza et al., 2021). In addition, in this context the increase in social demands caused by the crisis surpassed the response capacity of several SNGs, with large differences with regard to their availability of financial, human and technical resources. To guarantee equal access by all citizens to basic services, some CGs introduced new national programmes to standardise the implementation by subnational governments, thus also reducing their autonomy (Andreotti and Mingione, 2016).
In this light, the territorial dimension of the Welfare States social policy has become increasingly important in comparative research (Greer et al., 2023; Kazepov, 2010; López-Santana, 2015). How has territorial welfare governance really evolved during the Great Recession? Why? Has it slowed down or reversed the decentralisation process which characterised the development of the Welfare State since the 1970s? What public policy instruments have been used and what dimensions of territorial governance have changed, with what intensity/scope?
This article seeks to contribute to the literature on the scope and measurement of changes in social policy multilevel governance, and to explain how and why multilevel welfare systems have recentralised in response to the crisis. We examine whether the attempt to respond to new public policy problems (such as fiscal consolidation) can affect the territorial governance of social policies. We are looking for signs of recentralisation in the Welfare State, which occur when we find the erosion of subnational responsibilities or fiscal autonomy and/or of the influence that SNG can exert on the CG in this sector, that is, self-rule and shared-rule (Elazar, 1987). Self-government and the influence of SNGs depends on changes to the degree of control over a range of resources, such as financial, political, or administrative (Elander, 1990; Eckersley, 2017). To capture recentralisation, we have developed the Social Policy Recentralisation Index (SPREI), an original composite index adaptable to the particular field of social policies and made up of several indicators both qualitative and quantitative, which operationalises three empirical dimensions of analysis. Additionally, to validate our indicators for a specific case, we have conducted 19 semi-structured interviews with national and regional policymakers and officials. 1
Regarding our case selection, Spain provides a persuasive crucial case for studying the dynamics of welfare governance under crisis. Coming from a tradition of strong centralisation, decentralisation was one of the most significant trends in the institutional development of Spain since the early 1980s. The case of Spain illustrates a multilevel country in which the welfare state is fully devolved. In a short period of time, it has witnessed several dynamics of centralisation/decentralisation/recentralisation in the social policy area driven by external factors. Those factors, such as the Great Recession and the pandemics, have also affected other similar multilevel countries. Although several studies have sought to pinpoint the effects of those crises and the austerity policies pursued in the Spanish decentralisation model (Muro, 2015; Colino & del Pino, 2017), few of them have sought to systematically measure the extent and type of recentralisation occurred. That means it is also a good test case or plausibility probe for the applicability of our index, which was developed for comparative purposes. Drawing upon previous in-depth qualitative research of our own on the Spanish case, we were able adjust and test the design and indicators of the index. That makes it more applicable to other cases and useful for cross-sector and cross-country comparisons.
In order to validate our index and identify different dynamics regarding the territorial governance of social policies, we analyse two policies. We have selected healthcare and long-term care2 policies because both involve the provision of public services and are classical welfare state policies which are usually constitutionally devolved and represent the bulk of regional social spending. They are also the policy areas in which central government are likely to, formally or informally, regain powers in contexts of crises and external shocks implying fiscal consolidation paths and spending cutbacks. Both of them have undergone significant changes in their territorial and institutional organisation in most multilevel countries. As a result, the analysed territorial dynamics are more complex than in social policies that consist only of the payment of cash benefits, such as pensions or unemployment benefits, which remain centralised in most countries of the world. This makes our cases more complex and relevant if we want to understand dynamics of authority migration and power shifts. In Spain, we have witnessed moves from centralization to decentralisation of healthcare since 2002. In long-term care, which was initiated as a shared competence, it has experienced different phases of recentralisation in decisional and financial terms. Finally, the fact that healthcare is a highly valued and long-established policy area within the remit of most welfare states, while long-term care is a relatively new and still weak policy area in terms of professionalisation (Hernández-Moreno et al., 2023) and popularity, provides also some scope for variance and to observe possible variation across sectors of public activity (Arlotti and Aguilar-Hendrickson, 2018; Costa-Font and Greer, 2013; Greer, 2004).
To preview our results, after a qualitative process tracing analysis of our cases, and the application of our index, we find that the crisis put the Spanish decentralisation model under serious stress due to national fiscal consolidation requirements. During the Great Recession, several recentralisation initiatives were pursued affecting the arrangements governing decision-making, financing and the implementation of social policies, which are aptly reflected in our proposed index scores. However, our index also shows some specific differences by sector or dimensions of recentralisation that reflect the fact that Spanish regions have been able to safeguard some of their space of autonomy.
The article is structured into five sections. Section 2 presents a literature review on approaches to change in the governance of social policies, outlining how these changes have been conceptualised and measured within three main bodies of research. Section 3 proposes a recentralisation index made up of several indicators to measure and compare territorial welfare governance. In the fourth section, we apply this composite index to healthcare and long-term care policies in Spain during the Great Recession. Finally, we present our conclusions and their implications for further research.
Capturing recentralising trends in territorial welfare governance: A state of the art
The effects of the crisis on the governance of social policies are not always clear. One of the reasons why conclusions on changes in the governance of the Welfare State are limited is measurement problems. Until the 1970s, large central bureaucracies controlled the provision of social policies, and their decentralisation was easily identifiable through any rough indicator of devolution of powers (e.g. the development of regional legislation) or through variations in the social spending managed by SNGs (Kazepov, 2010:41). But these indicators do not reflect the complexity of the territorial governance of the Welfare State after decades of evolution. In addition, in most countries the governance of each social policy area implies a wide variety of resources in the decision-making, funding or implementation of social policies which in many territorially complex systems are distributed among different levels of government (Ferrera 2005; Greer, 2010). Several strands of research are relevant to better understand the evolution of decentralisation and recentralisation trends and its measurement:
On the one hand, since the late 1970s, some indices have attempted to track decentralisation or autonomy shifts through analysis on the distribution of authority (e.g. comparative federalism), as well as from studies on governance and new public management (for an overview, see Harguindéguy et al., 2021). Among them, the Regional Authority Index (RA), developed by Hooghe et al. (2010, 2016) and Shair-Rosenfield et al. (2014, 2021) track changes of regional powers in 81 countries from 1950 to 2010, using 10 dimensions around the political, administrative and fiscal powers of governments. Niedzwiecki et al. (2021), applying the RAI to 27 countries in Latin America and the Caribbean, also detected trends towards decentralisation in most cases. Based on a critical review of the RAI, Dardanelli (2019) has proposed a new scheme to measure (de)centralisation and autonomy. His index has identified the strengthening of some regional and local governments and the existence of processes of weakening regional autonomy, or cases where no change has occurred.
Some indices measure and compare changes in local governance (Wolman and Goldsmith, 1990; Lidström, 1998; Fleurke and Willemse, 2006). The Local Autonomy Index (LAI) measures local autonomy in 39 countries between 1990 and 2014 using 11 variables. It shows an overall increase in local autonomy and a growing consolidation of local governments, albeit with a disparate extent across countries (Ladner et al., 2023: 347–348; Ladner and Keuffer, 2021). According to a more recent LAI 2.0., the overall results indicate that, over the last 30 years, local autonomy continued to rise – especially in Central and Eastern European countries – although with a much more moderate pace in the most recent period of 2015–2020 (Ladner et al., 2023).
Most measurement proposals resort to the three classical dimensions, namely, fiscal, administrative and political (although differently labelled), with the use of quantitative methods and techniques becoming increasingly widespread (Dardanelli, 2019). In some cases, the indices are based on a single dimension, usually political or fiscal (International Monetary Fund (IMF), 2013; Rodden, 2004; World Bank, 2013), and increasingly on the combination of several of these dimensions (Dardanelli, 2019; Hooghe et al., 2010, 2016; Ladner and Keuffer, 2021).
These contributions are very useful in the field of comparative politics to understand the extent of changes in territorial governance dynamically over the years. However, they are not entirely well suited to the field of social policy, mainly because of over-reliance on fiscal data and indicators. While these indicators have proved valuable, they are overly abstract for measuring the complexity of (de)centralization processes on the ground (Dardanelli, 2019: 209–211). The share of subnational spending and tax revenue in relation to the overall amount of spending and revenues can provide us with useful information, but ‘they are silent about which level of government sets the policy framework that determines citizen entitlement to benefits and services’ (Banting, 2006: 48). For example, in the Nordic countries, subnational governments spend most of the public funds allocated to social policies. However, they have very limited decision-making capacity on the type of benefits and little room for manoeuvre on how to spend (Hooghe et al., 2010:28). Moreover, most indexes of decentralisation tend to neglect aspects linked to the coordination of public policies in intergovernmental forums (Do Vale, 2015: 751–754).
Regarding a second strand in the literature in the field of social policies, there have been some analyses around the dynamics of decentralisation and recentralisation which have also considered different types and paths of decentralisation using the three classical dimensions of decentralisation mentioned above (Greer et al., 2023; Minas et al., 2012). But others have also tried to operationalise these dimensions utilising a set of indicators (Saltman and Bankauskite, 2006; Sellers and Lidström, 2007; Barberis et al., 2010). Here, we should especially mention the work by Bossert (1998) and Bossert and Beauvais (2002), who drawing on health services research, develop the ‘decision space approach’. This approach focuses on identifying the scope in which a given government can make and implement its decisions. Decision space refers to various functions and activities (e.g. service delivery, financing, and planning) over which lower levels of government enjoy a certain degree of autonomy. Following the work of Bossert and colleagues, Terlizzi (2019) analyses the dynamics of decentralisation and recentralisation in the case of health systems in several countries. Drawing on discursive and historical institutionalism, the author also dwells on classical institutional dimensions, acknowledging the complexity and multidimensionality of the object of study ‘rather than considering decentralization as the transfer of a fixed and unique block of authority and responsibility’ (Terlizzi, 2019: 975). Terlizzi’s proposal for operationalising and measuring change is based on qualitative composite descriptions and evaluations, rather than one-dimensional quantitative measures (see also Terlizzi and Esposito 2023).
However, most of these proposals identify aggregated patterns and general trends, thus foregoing a detailed analysis of each of the policy areas and dimensions. In the case of the approach proposed by Bossert and colleagues, its main limitation is that ‘the comparative analysis of decision spaces rapidly points to a few recurrent patterns known to students of comparative politics. Working out what constitutes decision space depends on comparative politics insight’ (Greer & da Fonseca, 2015: 411). Thus, the methodological design of most proposals from the welfare field might give a very different picture of the reality on the ground, greatly altering the scope of the results obtained by these studies (Barberis et al., 2010: 388). For example, Italian regions and municipalities have an important financial and administrative role in elderly care (Ranci and Pavolini, 2013), while in labour market policies and social assistance subnational institutions still overwhelmingly rely on resources directly allocated by the central government (Vampa, 2017). On the other hand, some analyses in the crisis context show that different governance change dynamics depend on the policy dimension in question. Although most of the existing research does not base their indicators on the power of governments explicitly, or remain very broad, in general, it is the decisional and fiscal dimensions the ones that seem to be more affected by recentralisation (León et al., 2015). However, these territorial welfare governance reform processes do not show a clear direction or homogeneous scope in countries with traditionally decentralised power structures, even in unitary states such as the Nordic countries (Minas et al., 2018).
More recently, a third group of studies has developed around specific trends towards recentralisation in Latin America, Africa, Asia, and Europe. Countries as diverse as Brazil, Mexico, South Africa, Bolivia, Israel, China, Colombia, and Russia have experienced changes in the balance of power between levels of government in the wake of the financial crisis but also before and independently of it (Béland et al., 2018; Eaton and Dickovick, 2004; Eshel and Hananel, 2019; Kennedy, 2017). Dickovick (2011) studied how CGs have reinforced its control over SNGs through tight control of spending and borrowing, have trimmed borrowing powers, managed expenditures with increasing technocratic efficiency, and passed increasingly strict statutes that criminalise subnational fiscal irresponsibility. A common trend in decentralised countries, and reinforced during the Great Recession, was that CGs assumed a more prominent role in controlling the social expenditure of some SNGs, justified by the need to address urgent problems of fiscal discipline and to prevent opportunist behaviours (Bolgherini, 2014). These studies detect changes brought about by various types of instruments including regulatory, financial, and organisational elements (Eaton, 2014; Mendoza Ruiz et al., 2020; Olmeda and Armesto, 2017). However, as in other multilevel systems, financial instruments in the form of conditional grants, spending regulations, borrowing decisions, and conditionality have been the most recurrent (Braun and Trein, 2014; Schlegel, 2022).
One of the main premises of these work is that recentralisation is the result of interactions between strategic actors located at different levels of government, pursuing their policy preferences. They have sought to establish under what conditions national authorities are willing to recentralise and to identify the diversity of factors that contribute to their success. They have emphasised factors such as economic crises or neoliberal reforms, political parties’ strategies or electoral calculations of national and regional presidents, or the difficulties of SNGs to deliver those services previously decentralised. Despite their merits, these studies have not been very explicit on how to measure the dependent variable, that is, the degree of recentralisation and its different dimensions.
In sum, although all these three strands of research have represented a breakthrough, we still lack a systematic framework for capturing changes in the territorial governance of welfare, nor do existing work offer us a comprehensive, accurate, and transparent measurement tool, replicable by other researchers in other countries or public policy sectors.
Developing the Social Policy Recentralisation Index (SPREI)
As stated above, factors which help to measure the scope and the direction of territorial change in the specific field of social policies are still insufficiently understood. The literature on comparative federalism offers us some clear foundations for studying the territorial dynamics of continuity and change using different drivers, including the need to solve policy problems (Benz and Broschek, 2013; Braun and Trein, 2014). Solutions to public policy problems can involve questioning the existing institutional balance and the role of different governments in policymaking, leading to changes in governance (Braun and Schnabel, 2019). But others can act by conditioning the direction of governance change. The different territorial actors seek to maximise their power over policymaking by controlling a series of resources, such as political or fiscal ones, in order to guarantee their autonomy (Rhodes, 1981). This can lead to different types of reforms which combine centralisation in certain resources and decentralisation in others, even in the same policy sector. Changes in the territorial governance do not necessarily imply the transfer of authority in its entirety between levels of government but rather refers to the relative expansion of central control in one or several governance dimensions (Treisman, 2007).
To analyse the scope and direction of the territorial social policy governance change in multilevel systems, we propose some indicators inspired in a combination of (1) the two components of the federal principle by Elazar (1987) and (2) the resource dependence approach to the study of intergovernmental relations (IGRs) by Rhodes (1981), among others. We start from a basic definition of the recentralisation of social policies according to which it consists of an increase in the power of the central government at the expense of SNGs in one specific policy sector. Perhaps the CG is trying to get the SNGs to do what they would not do of its own volition, or it wants to prevent the SNGs from doing something they would do if they were allowed to.
Applying Elazar’s (1987) distinction between ‘self-rule’ and ‘shared-rule’, we understand that recentralisation occurs when we find an erosion (1) in the capacity for subnational self-government and/or (2) in the influence that SNGs can exert on the central level in the area of social policy. The self-government and influence of SNGs depends on their degree of control over a range of resources, not solely financial but also constitutional-legal, regulatory, political, and administrative, to obtain their own policy priorities (Elander and Montin, 1990). Without these resources or with limited resources, the ability of SNGs to act and influence the different phases of policymaking would be limited (Eckersley, 2017).
Based on these definitions and on previous work on the literature on territorial welfare governance (Barberis et al., 2010; Del Pino et al., 2022; López-Santana, 2015; Sellers and Lidström, 2007), on political science work on dynamic decentralisation (Dardanelli, 2019; Hooghe et al., 2016; Ladner and Keuffer, 2021), and on recent studies on recentralisation in the wake of economic crises (Armesto and Olmeda, 2017; Dickovick, 2011; Eaton, 2017; Eaton and Dickovick, 2004; López-Santana, 2015), we propose the three following analytical dimensions, including several empirical indicators each, that make up our composite index. We have called it the Social Policy Recentralisation Index (SPREI), around which we try to assess the extent to which the central government gained power vis-à-vis SNGs throughout a specific time period.
Decision-making
The ability to establish the basic design of social policies can be altered in various ways: formal changes in the distribution of powers or the rules of the political process (in the Constitution, national or regional sectoral legislation or special statutes) affecting the role of the CG (Indicator D1) 5 ; increase of the power of horizontal departments in the CG (typically the Ministries of Finance or Public Administration) leading to decisions that significantly reduce SNG leeway in their sectoral welfare policies (Indicator D2); legislative mechanisms in the national parliament (territorial second chamber, IG parliamentary committees) through which SNGs participate in the elaboration of state-level legislation are suppressed or reformed in such a way that the ability of SNGs to influence the legislative process is reduced (Indicator D3); the operation of those IG mechanisms in the national parliament (territorial second chamber, IG parliamentary committees) through which SNGs participate in the elaboration of state-level legislation changes in such a way that the ability of SNGs to influence the legislative process is reduced (Indicator D4); multilateral IG social policy coordination and cooperation bodies are suppressed or reformed in such a way that the ability of SNGs to influence decision-making is reduced (Indicator D5); the operation of multilateral IG cooperation bodies in social policies changes in such a way that the ability of SNGs to influence decision-making is reduced 4 (Indicator D6).
Finance
The capacity of SNGs to finance their policies may also be constrained in different ways: the percentage of CG revenue over total public revenue increases (Indicator F1); the CG reduces the power of SNGs to establish their own taxes, regulate allocated taxes or reliance on credit markets to obtain financial resources (Indicator F2); IG financing mechanisms and intergovernmental transfers dependent on the CG (devolved taxes, fund transfers and liquidity funds) increase their conditionality (Indicator F3); the CG sets spending caps for SNGs (if it did not previously) (Indicator F4); and the CG sets spending targets for SNG welfare programmes or services (if it did not previously) (Indicator F5).
Implementation
This dimension refers to the organisational and administrative elements linked to social benefits or services delivery. Thus, (re)centralisation is observed if: the CG replaces the SNGs in the management of welfare programmes (Indicator I1); the degree of detailedness in the content of the central welfare legislation increases (Indicator I2); the CG promotes, directs (or, if they exist, perfects) the development of monitoring and evaluation systems related to SNGs programmes, services or organisational performance (this includes quality standards) (Indicator I3); the CG (on its own or in collaboration with others) creates (or strengthens) an agency to supervise the implementation of welfare programmes and services delivered by SNGs (Indicator I4); the CG increases its ability to influence the day-to-day management of decentralised welfare programmes through the recruitment, selection, training, or assignment of SNGs personnel (Indicator I5).
The Index of Social Policy Recentralisation.
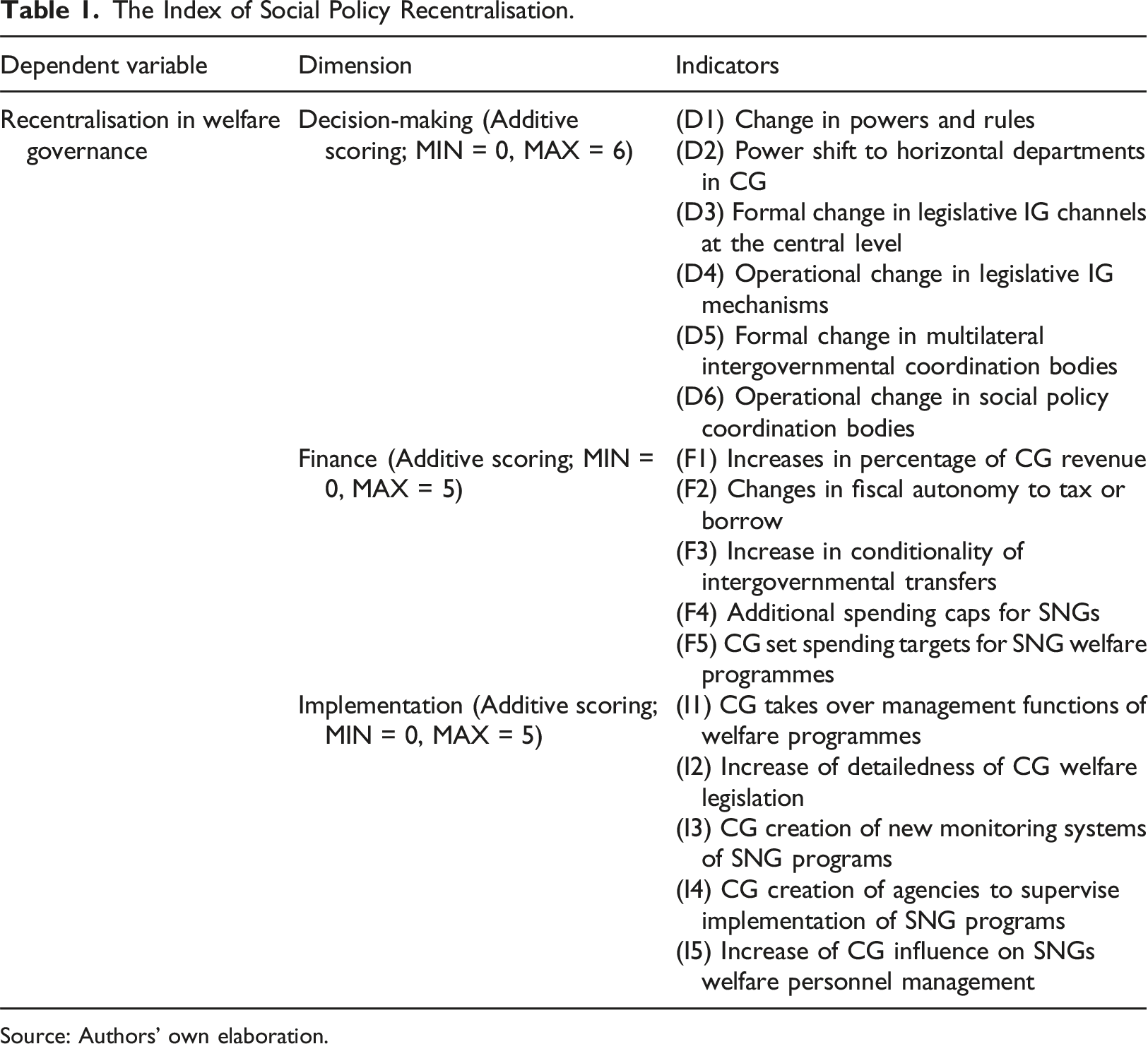
Source: Authors’ own elaboration.
This composite index draws on the commonalities of different cases and institutional designs and may thus work as a comparative device to study territorial welfare governance. The definition of most dimensions and indicators of our index are comprehensive and abstract enough to be able to include the common traits of all multilevel systems and at the same time to reflect the specificities of most countries with devolved social policies. In any case, our assumption of reliability and general applicability of our index can only be validated through its future practical application to other cases. Moreover, we also believe that it may be applicable to other public policy fields, for example, in education, migration, or active labour market policies. In many welfare states, decision-making activities are driven by the central government, through general or framework laws about healthcare, housing, education or labour activation policies, whilst implementation and funding have been decentralised (Minas et al., 2018). Our point is that this index enables us to measure changes in the governance of social policies using a set of indicators easily measurable for policy experts familiar with intergovernmental relations in those sectors.
Besides that, the index may also be utilised to develop testable empirical expectations about change in specific cases. For example, in our case, based on the literature, the scope of the crisis, and the specificities of Spanish territorial governance, we could develop several expectations about change in the behaviour of the index in its different dimensions. First, in the context of severe economic crisis and strong EU pressures and given the fact that social policies account for some 75% of regional budgets, we would expect the index score to increase reflecting the CG’s decisions or regulations that affect the social policy governance in the hands of regional governments. As a second expectation, we predict that the index score will increase in both selected policies. Thirdly, given the anti-crisis policy instruments used by the CG, we expect the different dimensions of the index (decision, finance, and implementation), to vary in the extent of their increase. Since the CG and the SNGs play diverse roles and control different types of resources to different degrees, we assume that the CG will prefer to act in the decisional and fiscal dimensions, where it is stronger. The deeply decentralised model of territorial organisation and the social support for both policies limit the CG’s scope for action. For instance, we could expect the index to reflect the change in the use by the CG of framework regulations and tighter conditionality in funding. 2
Recentralisation trends in health and long-term care in Spain
The Spanish devolved model, the so-called Autonomic State, has enabled the 17 regional governments to attain high degrees of legislative and executive capabilities in key social protection system policies. Healthcare and long-term care represent together around 8.6% of the Spanish GDP (Gallego and Subirats, 2012). From 2010 to 2016, 3 Spain suffered a big impact from the Great Recession and a clear tension emerged between safeguarding the autonomy of SNGs and the need to keep national public finances under control. In a period of just 2 years, the legislative process saw the enactment of 48 regulations by the central parliament, which was controlled by a left-wing party in 2011 and by a right-wing party from 2012 on. These regulations were enacted by emergency procedure and had a significant impact on the role of the SNGs in the governance of their social protection systems, particularly in the areas of healthcare and long-term care. Let’s consider them in turn.
The impact of the Great Recession on territorial healthcare governance
Background
Since 2002, the Spanish National Health System (NHS) has been decentralised to the 17 Autonomous Communities (ACs). Currently, the CG is responsible for the regulation of the right to healthcare and the basic elements of the organisation, coordination and financing of the NHS. The ACs legislate within the framework of the basic national regulation, decide on the configuration and management of their own Regional Health Services, and were in charge of 92.5% of healthcare spending in 2016 (OECD, 2020). The Inter-territorial Council of the NHS (CISNS) is the intergovernmental cooperation body which brings together the regional and national healthcare ministries. Healthcare is funded mainly through the resources provided by a mix of taxes assigned, totally or partially, by the CG. Before the arrival of the crisis, the CG had lost most of its influence over subnational spending decisions in this area.
Decision-making
During the Great Recession, the CG promoted numerous reforms in the sectoral legislation which reinforced its role to the detriment of the legislative and executive capacities of the ACs (Indicator D1) 5 . In 2012, the CG enacted by Royal Decree Law 16/2012 on urgent measures to guarantee the sustainability of the NHS. This regulation, justified by the CG for equity, efficiency, and viability reasons, amended the scope of the right to free healthcare under the public system, which ceased to be universal, excluding some groups previously entitled (immigrants). It increased the contribution insured persons must make for the purchase of medicine (co-payment). It also included a provision which had a recentralising effect in that it established a common portfolio of available services, while recognising the possibility for ACs to include additional ones, as long as they ensure the resources to fund them.
Other CG initiatives included provisions to control the ACs’ pharmaceutical and healthcare expenditure, and a set of sanctions for non-compliance in the submission of information to the CG. Nevertheless, ACs continue to seek to defend their priorities (interviews 7, 9, 11, 14, 15, 18). For example, three of them (Andalusia, Asturias, and Catalonia) developed different strategies to circumvent the restrictions imposed on certain population groups to access the public health system. The first (left-wing) AC continued serving them without adopting any specific legislation, the second (left-wing) established an alternative procedure to care for irregular immigrants; in the third (Catalan nationalist-right), all patients continued to receive medical care, justified on efficiency reasons.
The Ministry of Finance strengthened its role in the policy formulation process (interviews 10, 16, 17) (Indicator D2). At the same time, a process of strengthening the CG coordination mechanisms is taking place through the Cabinet subcommittee for Economic Affairs, an executive structure linked to the Prime Minister. In 2010, an austerity framework agreement was implemented which, while formally respecting the autonomy of the ACs, actually affected many decentralised management areas. ACs were obliged to send information on payment proposals and amounts paid to private companies, non-profit institutions and families. Other subsequent regulations established a requirement of a Ministry of Finance authorisation for exemptions from framework agreements and centralised systems for drugs purchasing.
There were no formal changes which modified the role of ACs in parliamentary policymaking at the national level through the Senate (the territorial representation chamber) (Indicator D3). However, a decrease can be observed in the activity levels of the General Committee of the Autonomous Communities, the Senate committee in charge of enhancing the upper chamber’s territorial function through the inclusion of the ACs into the State legislative procedures (Senate, 2020). Likewise, in the Health and Social Affairs Committee (which leads the healthcare debate in the Senate), the parliamentary majority (Popular Party, -PP- and the Socialist Party, -PSOE-) excluded certain regional nationalist parties from its governing body, thus reducing their capacity to influence legislative decision-making processes (Indicator D4).
There was also a decline in the activity of the main intergovernmental cooperation body in this policy area, the CISNS, whose average number of annual meetings fell from 5.3 in the period 2009–2011 to 2.2 in the period 2012–2016 (Ministry of Territorial, 2020). This implied a decrease in the opportunities for the ACs to assert their interests (Indicator D6). There were also changes in the functioning of these bodies. Between 2011 and 2016, there was a devaluation of the role of the CISNS second level IG committees and working groups (interview 15). The congruence of the ‘political colour’ of the CG (PP) with the governments of most of the ACs contributed to reinforce the trend of the CISNS to operate according to a logic based on partisan alignment. This, in turn, contributed to broadening the CG’s room for manoeuvre, as it has less need to negotiate the content of its proposals. 4
Finance
In Spain ACs are structurally financially dependent on the CG to an important degree. From 2009 onwards, and at least temporarily, the ACs have seen the share of public resources allocated to them reduced (CERRFM, 2017:26) (Indicator F1). There is also a vertical fiscal imbalance, understood as the mismatch between the capacity to obtain own resources by the SNGs and their spending needs (IMF, 2020). Several of the regional ministers of finance referred to this situation (e.g. interview 16). More than 400 taxing regulations reforms were enacted in Spain during the crisis at both levels of government (Rubio and Álvarez, 2019) and numerous taxes were increased, but most of the additional resources obtained were left in the hands of the CG. Moreover, certain fiscal initiatives undertaken by some ACs led to conflicts with the CG. This was the case with a new tax (the ‘Euro per prescription’) established by Catalonia and Madrid and declared unconstitutional in May 2014. In addition, through new Organic Laws, the CG was empowered to limit the regulatory competences and the revenue raising powers of the ACs in relation to the taxes allocated ‘when it is necessary to comply with the commitments of fiscal consolidation’ (Art 25.1.a). Finally, Organic Law 2/2012 reinforced the control powers of the CG regarding the debt operations of the ACs, as an AC required the explicit authorisation of the CG in order to borrow in the credit markets (interview 16). In short, during the Great Recession the CG conducted reforms aimed at reducing the powers and fiscal opportunities available to regional governments (Indicator F2). 5
To provide funding to ACs, the CG implemented several initiatives on an extraordinary basis. The CG created the Supplier Payment Mechanism, the Regional Liquidity Fund (FLA), and the Social Fund. The first one provides resources so that the ACs can settle pending invoices from external providers. The second one is aimed at financing, under advantageous conditions, the debt of ACs. The third one is intended to finance transfers in the field of social policies, as well as payment obligations linked to agreements signed between the ACs and local governments in this area. These instruments mobilised €175,021 million in the period 2012–2016 for the SNGs (Ministry of Finances, 2020). In exchange for this money, the ACs had to accept certain conditions, such as the development of complementary retrenchment plans evaluated by the Ministry of Finance, the reimbursement of the amounts contributed by the liquidity support instruments, and to accept the system of penalties provided for in them. This undoubtedly strengthened the CG’s position in its relations with the ACs (Indicator F3). 68.2% of the total amount provided by the extraordinary financing mechanisms to the ACs was devoted to healthcare. In the specific case of the FLA, this percentage was 78.6% (Ministry of Finances, 2020). Although it provided financing at very favourable rates, it also included conditions such as the mandatory adherence to an ‘Instrument to Support the Sustainability of Health and Pharmaceutical Expenditure’, as well as the submission of detailed information, both on pharmaceutical and healthcare expenditure, and on the contracts and agreements signed with authorities, third-sector organisations and private companies. All regional policymakers acknowledged that the FLA reduced their room for manoeuvre.
In September 2011, following an agreement between the Socialist CG and the main opposition party (the PP), the amendment of article 135 of the Constitution was passed. Public administrations, both at the central and subnational levels, must comply with the principle of budgetary stability, and may not exceed the deficit and public debt reference levels established by the EU, except in the case of natural catastrophes, economic recession or emergency situations beyond the control of the State. In April 2012, with the new CG of the right-wing PP, Organic Law 2/2012, which developed this constitutional precept, was enacted. In addition to setting the principle of budgetary stability (which implies achieving a budgetary balance or surplus), it established a spending rule according to which expenditures (including those of subnational governments) ‘cannot increase above the rate of growth with reference to GDP’ (Indicator F4). Later on, the 2015 reform of Organic Law 2/2012 strengthened the CG’s task of controlling public expenditure to ensure that budgetary stability objectives are met. The CG sought to establish spending limits for different elements of healthcare policy. However, regional policymakers also noted that the ACs did their best to maintain their room for manoeuvre and use it to develop their own priorities. Examples of this are the investments made in specialised primary care, prevention, health promotion and vaccines, or in the improvement of communication networks (interviews 13, 15, 18) (Indicator F5).
Implementation
The management of healthcare services, facilities and personnel remains a responsibility of ACs (Indicator I1). However, through national level welfare legislation, the CG places the ACs in charge of implementing a wide range of measures regarding health services, justified on grounds of pursuing administrative efficiency. This induced standardisation in the rules and procedures of healthcare services provided by the ACs, aimed at increasing the degree of homogeneity and ensuring a stricter control of the use of funds provided by the CG (Indicator I2). The CG also established a system for evaluating the costs of implementing the NHS common portfolio, as well as those related to new care procedures. The CG tried to establish common quality standards for hospitals through the Spanish Society for Healthcare Quality. Nevertheless, beyond the general recommendations, each AC establishes its own standards (interview 13) (Indicator I3). Human resource management remain in the hands of the ACs. Through Royal Decree Law 16/2012, the CG sought to standardise certain aspects of human resource management at regional level. The measures included the creation of a new centralised state registry for healthcare professionals, the approval of a homogeneous catalogue of professional categories and a mandate for regional services to establish procedures for training and evaluating personnel performance. The freezing of public recruitment at a 10% replacement rate for healthcare personnel was also implemented by the CG (Indicator I5).
The impact of the Great Recession on territorial long-term care governance
Background
The most important reform of the Spanish welfare state before the Great Recession was the creation through a national law of the Long-Term Care System (known as SAAD) in 2006, providing universal coverage for all persons in need of care. The CG reserves the right to regulate certain basic aspects of SAAD throughout the national territory. The ACs accepted that the CG would assume some new social assistance competences because this would simultaneously finance an important part of the system. The financing of the SAAD is structured in three levels. The CG assumed the full cost of the ‘minimum level’ benefits and services for dependent persons, transferring the corresponding funds to the ACs. The ‘agreed level’ was funded jointly by the CG and the ACs. Finally, an ‘additional level’ was financed by each region. The ACs are responsible for implementing and managing the SAAD. Implementation is uneven across regions, with different rules for co-payment, access procedures, coverage levels, and financing (Marbán, 2015:51). The role of municipalities depends on the regulations enacted by the ACs and varies significantly between regions. The law created the SAAD Territorial Council as a multilateral intergovernmental cooperation body in which the three levels of administration participate.
Decision-making
The CG amended the previous distribution of powers to its favour (Indicator D1). The CG, through Royal Decree Law 20/2012 and 1051/2013 changed the deadline for recognising the right to enter SAAD, modified the criteria for assessing benefits, reduced the generosity and amount of certain services, and delayed the full deployment of SAAD. As in the case of healthcare, the Ministry of Finance strengthened its role in the policy formulation process during the crisis (Indicator D2). In 2010, the first framework austerity agreement was reached with the ACs, which actually represented an imposition affecting many areas of regional management, including long-term care, with measures which are detailed in the previous case. As we have seen, during the crisis, the Health and Social Affairs Committee in national parliament reduced its activity and with it the ability of regional authorities to influence decision-making in this area (same data as for health) (Indicator D4).
The intergovernmental cooperation bodies were also reorganised in this period. Through Royal Decree Law 20/2012, the CG merged the intergovernmental Council of Ministers for Social Affairs with the SAAD Council, giving rise to the Territorial Council of Social Services and SAAD. From the perspective of the regional policymakers, by restructuring these intergovernmental bodies, the CG developed a workspace which favours the achievement of its priorities over those of the ACs. For example, the CG moved to determine certain formal aspects of this body, such as its agenda setting powers (interviews 3, 5, 6, 19) (Indicator D5).
The number of Council meetings decreased during the crisis (from 2.2 per year in the period 2009–2011 to 1.6 annually in the period 2012–2016; Ministry of Territorial, 2020). Moreover, between 2007 and 2011, a climate of collaboration prevailed (interview 1). Decisions tended to be made unanimously. Several interviewees stressed the importance of the technical component (as opposed to the political one) in the functioning of the SAAD (interviews 4 and 5). Then, coinciding with the worsening of the crisis and the change of party controlling the CG, things changed: with a large majority of the ACs governed by the conservative PP, the logic of party alignment tended to prevail (interview 1) (Indicator D6). From 2015 onwards, the political composition of the Council changed, as several ACs governed by the PP now came under the control of left-wing governments. Since then, most of the proposals presented by the CG have been blocked (interviews 4, 5, 6).
Finance
Before specifically considering long-term care policy, it should be remembered that the ACs have seen their share of public revenues reduced (CERRFM 2017:26) (Indicator F1). Likewise, the CG limited the access of the ACs to the financial markets, and some new regional taxes were challenged by the CG before the Constitutional Court (TC). However, unlike what happened in healthcare with the ‘health cent’, in the case of social services the CG does not prevent the development of financing mechanisms specifically linked to them (Indicator F2). Accordingly, ACs are active in the implementation of co-payments. Although the lack of transparency of the system prevents us from knowing exactly the impact of this increase, estimates point to an average of 20% of the cost of benefits, and may be even higher depending on the relative weight of the different benefits (Montserrat-Codorniu, 2015:197).
Regarding the degree of conditionality attached to the funding provided by the CG (Indicator F3), the situation in long-term care is different from healthcare. Although the funding of long-term care policy provided for in Law 39/2006 had already an earmarked character before the crisis (unlike healthcare), its degree of conditionality does not increase with it. Moreover, only a minimal share of the resources from the extraordinary financing mechanisms (strongly conditioned) were devoted to social services, specifically 7.4% of the total extraordinary funds and 7.6% of the FLA (Ministry of Finances, 2020).
During the Great Recession, the CG reduced its degree of financial commitment to the SAAD scheme. It thus suspended contributions to the ‘agreed level’ and decreased those for the ‘minimum level’: ‘if in 2010 the central funding of the minimum level reached 30.7% of the total cost, in 2015 it only covered 17.5%’ (Montserrat-Codorniu, 2015:188). The CG also conspicuously broke the principle of financial transparency (the ACs stopped controlling the global data of the long-term funding system) and those ACs with higher cash benefits were penalised. The combined effect of the reduction in CG contributions and the increase in co-payments represented a de facto transformation of this policy funding, which now largely depends on SNGs and the users themselves (Montserrat- Codorniu, 2015).
As with healthcare, SAAD was affected by the general spending caps derived from the application of the principle of budgetary stability (Indicator F4). In addition, in a context of resource scarcity combined with strict deficit controls, the partial decoupling of the CG in terms of financing gave rise to a scenario which pushed the ACs to align with the objectives of the former, focused on fiscal consolidation, preferably by cutting spending. However, the CG did not set a specific spending limit for long-term care policy (Indicator F5), which made it easier for the ACs to retain part of the leeway they had before the crisis. This is evident when we observe the percentage of spending reduction, much higher in the case of Castile-La Mancha during the PP (right-wing) government, than in the other ACs (left-wing or Catalan nationalist). This can also be observed when we consider the diversity of regional regulations regarding the co-payment of services.
Implementation
The ACs continued to be responsible for the daily operation of SAAD (Indicator I1). However, the CG reinforced its position in the management of the system (Indicator I2). Royal Decree Law 1051/2013 went on to establish the regulation of the conditions for accessing SAAD, the content and duration of benefits, as well as the regime for incompatibilities among them. It also tightened the criteria used to assess the degree of dependence, affecting the legal benefit entitlements. In 2014, the SAAD Information System (SISAAD) was established, which provides the CG with data on the protected population, human resources and facilities, the results obtained, and the quality of the services provided. This instrument reinforces the position of the CG by enabling it to obtain a global overview of SAAD and, as a result, to influence the decisions of the SNGs more effectively. Likewise, the Ministry, through the Institute of Social Services and the Elderly (IMSERSO), approved standards to homogenise different aspects of the system’s operation, promoted a good practice guide and established quality criteria for SAAD services (Indicator I3).
Index results
Applying the SPREI for Spain (2010–2016).
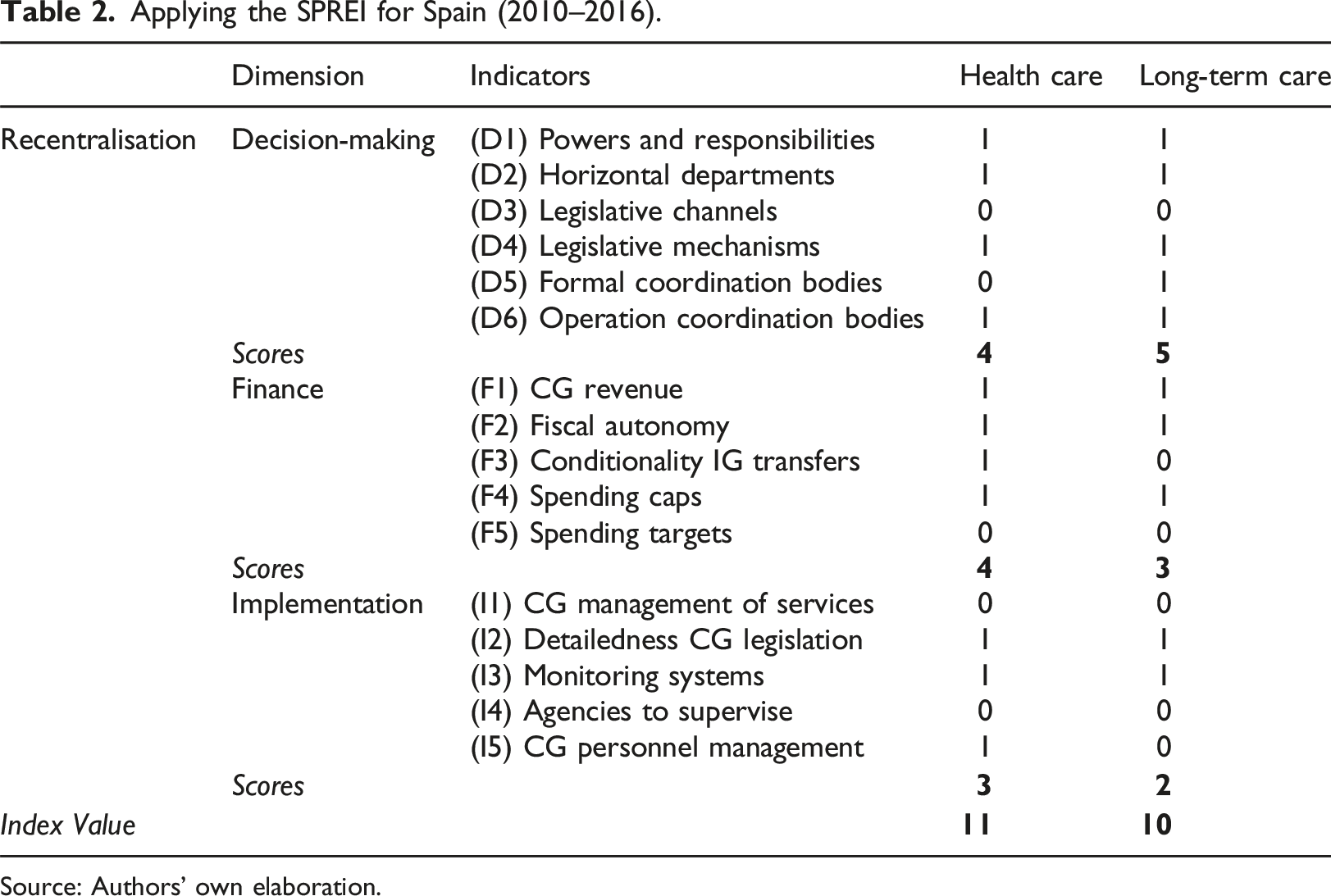
Source: Authors’ own elaboration.
The index scores show at first sight how the CG limited SNGs’ decision-making scope for both policies by developing both general and sectoral rules – sometimes using emergency regulatory procedures. The content of these rules aimed at reducing the scope of existing benefits to contain expenditure, as well as reducing inter-territorial differences in the supply of them. This affected the entitlements of individuals. In the case of long-term care, there was a de facto reduction in the content of the entitlements. In healthcare, there was a return to the principle of insurance to the detriment of the universal right to free public healthcare, which deprived part of the population of this type of coverage. Likewise, the reduction in the activity levels of intergovernmental cooperation bodies in the two policies and the strengthening of the tendency towards partisan alignment in their operation both contributed to reduce the ability of SNGs to influence decisions. The difference in score between the two policy sectors in the decision-making dimension (score of 4 vs 5 reflects the fact that in the case of long-term care policy the CG did also reinforce its position by introducing changes to the configuration of IGR cooperation/coordination bodies through amendments in their standing rules of procedure).
In the economic and financial dimension, the 2011 constitutional amendment to introduce the principle of budgetary stability and the concrete way it was implemented in the context of adjustment policies strengthened the CG’s position in its relationships with the ACs. The fiscal reforms adopted in this period and the conditions attached to the liquidity support mechanisms operated in the same direction. This affected both policies, although not exactly in the same way. In the case of healthcare, more dependent on extraordinary financing mechanisms and with a more consolidated presence of the CG, recentralisation is more clearly manifested than in long-term care policy, with a score in this dimension of 4 points compared with 3 points.
Regarding the implementation dimension, recentralisation has, in both policies, gone hand-in-hand with an increase in the level of detail of national legislation and some development of centralised mechanisms for monitoring the implementation and evaluating subnational programmes and services. In the case of health, some additional measures related to human resource management have been implemented, too. These initiatives have sought to standardise activities, justified by the CG on the basis of the need to improve expenditure control and ensure equity. In spite of this, ACs have had some room for manoeuvre and have carried out actions on the ground that have not always been those advocated by the CG. In the case of healthcare, despite the restrictions on access to healthcare established in the CG’s Royal Decree Law 16/2012, some ACs have continued to attend immigrants in their regional health systems or have implemented new procedures in terms of organisation and management of services (such as telemedicine). As a result, the score obtained in the implementation dimension of the index is lower than the one observed in the decision-making and financial dimensions.
Conclusions
This article has sought to assess the dynamics of territorial governance of welfare states in a crisis context. Specifically, it asked to what extent the Great Recession reversed the process of decentralisation which characterised the development of the Spanish welfare state since the 1970s, what dimensions of territorial governance changed, and what policy instruments were used for this purpose.
We have defined recentralisation drawing on Elazar’s canonical distinction between self-rule and shared-rule, and the need to control a certain range of resources to perform these tasks. To capture a possible recentralisation in two analysed Spanish social policies (healthcare and long-term care) we have developed a composite index around three policy dimensions (decision-making, finance and implementation) consisting of several indicators, both qualitative and quantitative. In the absence of formal reforms in the territorial model, this dynamic index provides us with substantive information on the actual processes and outcomes of change in the territorial dimension of welfare and allows us to measure what is really happening in the de facto operation of the system and in relations between CG and SNGs.
The article also shows that changes in policy processes are driven by complex, interacting economic, political and social pressures, operating at different speeds in different sectoral and territorial contexts. For example, the congruence of the party in government at the central and regional levels facilitates the introduction of changes in the territorial governance of policies, as can be observed when we analyse the functioning of the existing intergovernmental coordination bodies. When there is no coincidence in the political orientation of the CG and the ACs governments, the latter use the resources at their disposal to resist recentralisation initiatives, exploiting the leeway they have in policy formulation and implementation, as well as through their actions in the intergovernmental coordination bodies.
We found that the Great Recession had a remarkable impact on the territorial governance of health and long-term care policies which could be summarised by saying that the CG, pursuing fiscal consolidation, diminished the SNG’s leeway in decision-making, finance and implementation by deploying a number of policy instruments. As the index scores clearly show, recentralisation is apparent in both policies, with no relevant differences between them despite the usual differences between these two sectors. The index scores also show that the intensity of recentralisation in the implementation dimension, although relevant, is lower than in the decision-making and the fiscal/financial dimensions. In any case, the recentralisation of health and long-term care policies during the Great Recession has not turned Spanish SNGs into mere agents of the CG. In both cases, the regional policy responsibilities recognised in the Constitution and regional charters (known as Statutes of Autonomy) have been preserved and regional governments have continued to be in charge of their regional systems of service provision. The index, however, also reflects a changing distribution of financial roles and resources between the two levels of government, with increasing dependence of SNGs on the CG compared to the pre-crisis situation.
Our study raises some issues relevant for future research. Firstly, our SPREI can be utilised to understand territorial governance reactions to different kind of crisis (e.g. the COVID-19 pandemic), since as with the Great Recession, a recentralising shock in territorial welfare governance may have occurred in some countries. The scope and intensity of recentralisation in the wake of the pandemic is not entirely clear yet, since some federal states have preferred the adaptation of health policies to territorial peculiarities, while others have prioritised coordination of common policies and general agreements. The SPREI makes it possible to measure complex social policies in which territorial dynamics are more difficult to capture than in those policies that only provide cash benefits. We believe this article is just a first step to understand and measure the dependent variable of recentralisation processes, we are aware that the next very important step is to establish what factors determine these changes in the territorial governance of the different social policies in Spain and in other federations and multilevel systems. Beyond short-term pressures (such as the economic and health crises), other political, institutional, and ideational factors may be behind the recentralisation of SNGs across the world. Regarding the feasibility of using our index for large-n analysis, we acknowledge that the index may be demanding in the sense that it requires detailed qualitative descriptions and process tracing about the institutions and dynamics in each of the sectors studied to soundly ground the scores. That can only happen, of course, within the framework of large international comparative research projects employing collaborative efforts and case specialists in different countries and/or sectors. However, we believe that its results show it can be worthwhile to apply it to advance comparative research in welfare governance and comparative federalism studies.
As for the policy implications of our study, we have seen that the need to solve public policy problems can become the main driver of territorial governance change. The global financial crisis caused intergovernmental coordination problems in relation to fiscal policy in a decentralised country. The search for a solution to this fiscal policy problem eventually led to a kind of spill-over effect, consisting of a change in the territorial governance of health and long-term care. Recently, in many decentralised countries, a public health crisis, COVID-19, has generated health coordination problems and this has led to questioning the existing institutional balance and the role of the different levels of government health and long-term care systems (Hernández-Moreno et al., 2025; Hernández-Moreno and Harguindéguy, 2024; Mattei and Del Pino, 2021). Similarly, the need to address population ageing is leading some countries to redefine the role of the different levels in the area of policies such as pensions or long-term care. The same is true of the need to address other policy problems or areas such as migration or labour market policies. The cases analysed have showed us that policy problems that have not originated in the social policy sector itself can also be an important driver leading to a reform of social policy territorial governance, and we need analytic instruments to be able to measure the extent of this change.
Supplemental Material
Supplemental Material - Recentralisation in welfare? Measuring and comparing territorial governance change in Spain
Supplemental Material for Recentralisation in welfare? Measuring and comparing territorial governance change in Spain by Jorge Hernandez, Eloísa Del Pino, Juan A. Ramo and César Colino in EPC: Politics and Space
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the ‘The Restructuring of the Governance of the Welfare State: political determinants and implications on the (de)commodification of risks (GoWPER)’ CSO2017-85598-R Spanish Ministry of Economy, Indu.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.