
Abstract
Introduction:
Telemedicine tools offer multiple advantages to achieve an epidemiological screening of communities in rural settings countrywide. However, evidence on the cardiological pathology surveillance in these communities is limited. The feasibility of telemedicine as an electrocardiographic (EKG) mapping tool for the diagnosis and prevention of cardiological pathologies in Paraguay was investigated.
Methods:
A descriptive study was conducted in 60 telediagnostic centers countrywide in Paraguay to evaluate the feasibility of telemedicine as an EKG mapping tool for the diagnosis and prevention of cardiological pathologies over a period of 5 years from 2014 to 2018. The adherence rate was determined comparing yearly scheduled visits versus fulfilled visits at the telemedicine platform.
Results:
During the study, 246,217 remote EKG diagnoses were performed in 60 hospitals using telemedicine. The patients were 19.4% children/adolescents and 80.6% adults. The results of EKG tests in the children/adolescent group were 79.4% normal and 20.6% abnormal. The most frequent abnormal heart rhythms observed were sinusal bradicardia (10.6%), sinusal tachycardia (3.2%), and unspecified arrhythmia (2.8%). In the adult group, the results were 66.3% normal and 33.7% abnormal. The most frequent abnormal heart rhythms in this group were sinusal bradicardia (11.2%), blockade of the right branch (4.8%), and left ventricular hypertrophy (4.7%). The most frequent cardiovascular risk factors observed were the association of hypertension and obesity (40%), hypertension and diabetes (20%), and hypertension and dyslipidemia (19%). During the test period (2014–2018), the average rate of patient adherence to the prevention program was 2.26 for each 1000 diagnosis.
Conclusion:
These results demonstrate the feasibility of telemedicine as an EKG mapping tool for the diagnosis and prevention of cardiological pathologies in low-resource countries, thus enhancing cardiovascular disease surveillance and optimizing human and financial resources.
Keywords
Introduction
Ischemic cardiopathy is one of the principal causes of morbidity and mortality in the world. It was accountable for 12.7% of deaths in 2016. 1 In addition, according to the World Health Organization (WHO), 2 cardiac pathologies were responsible for 15.7% of all deaths in Paraguay during 2017 representing one of the principal causes of death in this country. This shows the existence of a clear similar trend in the rates of death by cardiac disorders in developing countries compared to developed countries.
Innovations in information and communication technologies (ICTs) and biomedical technologies have improved health care in many countries of the world. 3 , 4 Technological innovations and health initiatives have made possible that many medical procedures today can be carried out without the “physical presence” of a physician or health worker. One of these innovations is, undoubtedly, telemedicine, which reduces the gap in the effectivity, accessibility, availability, and coverage of health services. 5 Telemedicine is a strong tool for diagnostic assistance and follow-up tests in remote populations. Thus, a big challange for developing countries 6 is to develop a cardiovascular prevention program using telemedicine and implement programs of health harmonization at a national level.
An improvement in the quality of health care is essential. Developing an affordable and equitable access to health services with independence of the social context, economic situation, or the home-place situation of each citizen is extremely important. In addition, to achieve these goals, telemedicine apps showed considerable usability and proved to be a powerful promising tool.7–9 In general terms, the populations living in remote areas of a country usually have no access to specialized medical care and treatment, as well as good support and counseling, often relying on local first aid medical services. These services have scarce resources and low ability to solve and make decisions. 7 The people in these remote locations have access only to an asymmetrical health system. In the end, the government cannot offer equity and universal coverage to the population. Accordingly, the health policies should be focused on a broader health service plan for remote populations, which have no access to specialized medical care.5–7 For this purpose, the telemedicine department of the Ministry of Public Health and Social Welfare of Paraguay, in collaboration with the Department of Biomedical Engineering and the Health Sciences Research Institute (IICS) of the National University of Asuncion of Paraguay and the Basque Country University (UPV/EHU) of Spain, undertook this study in order to evaluate the feasibility of telemedicine as an electrocardiographic (EKG) mapping tool for diagnosis and prevention plans of cardiological pathologies in Paraguay.
Methodology
Population
A descriptive study was conducted in 60 telediagnostic centers countrywide to evaluate the feasibility of telemedicine as an EKG mapping tool for the diagnosis and prevention of cardiological pathologies in Paraguay over a period of 5 years from 2014 to 2018. This study was approved by the Health Sciences Research Institute Scientific and Ethics Committee (approval no. P5/03 – C22/08) and has included 246,217 patients with medical request for an EKG test, who were referred to one of the 60 widespread countryside hospitals during the study period. All patients provided a written informed consent prior to enrollment in the study. Patient data were consigned in a complete electronic fact sheet. The EKG studies used the RJ45 and USB connection of the EKG device, which via a COM port interacted with the computer via an applicative software. This facilitated the capture of the information and the subsequent generation of pictures in Joint Photographic Experts Group (JPG) format. Each EKG device used (Nihon Kohden, model Cardiofax S SG-1250K) generated the EKG test curves through a conversion software in a scaled (intervals and voltages) JPG format. The asynchronous mode was used to forward the clinical information provided by the local physician and pictures from the rural health center to the remote cardiologist. The cardiologist analyzed the clinical data of the patient and the attached images for diagnosis after entering the data into the telemedicine platform. The telemedicine platform is web-based and allocated in the cloud. Immediately after this, the cardiologist made the diagnosis. The report was available for printing and delivery to the patient and/or for referral by mail to the treating physician. A coordination department of five cardiologists was responsible for reviewing the diagnosis results (mapping of countrywide cardiologic disease prevalence, productivity, and quality control) and patient adherence to the prevention of cardiological pathologies of the 60 connected countryside hospitals. The coordination department analyzed the results and developed a treatment protocol for patients according to the type and severity of the heart disease (national mapping). Thereafter, a patient treatment adherence monitoring protocol was activated for the purpose of follow-up visit to the patient by the corresponding cardiologist. The adherence rate was determined comparing yearly scheduled versus fulfilled follow-up visits to the registered cardiologist at the telemedicine platform. This determined the average visit rate of the patient in 1 year. The scheduled visits represent the preventive plan for the affected patients, and through the telemedicine platform, a monitoring of compliance with this plan was conducted.
Results
This study performed and analyzed 246,217 electrocardiograms and monitored the treatment compliance with the heart disease prevention plan. The EKG tests were conducted in the 60 community health centers of the national telemedicine network of the Ministry of Public Health and Social Welfare (MSPBS). Of the analyzed tests, 80.6% corresponded to adults and 19.4 to children/adolescents. The average age of the patients was 43 years.
With respect to the children/adolescents tests, 51% corresponded to girls and 49% to boys. Concerning the age group of the patients, 62% corresponded to 12–18 years and 28% to the range of 6–11 years. According to the analyzed results, 79.4% of the tests performed were normal and 20.6 abnormal. The most prevalent abnormal heart rhythms were sinusal bradicardia (10.6%), sinusal tachycardia (3.2%), and unspecified arrhythmia (2.8%). Other less frequently detected pathologies included right branch blockade (1.9%), left ventricular hypertrophy (1.0%), left branch blockade (0.4%), disorder in the ventricular repolarization (DVR) (0.3%), and atrial fibrillation (0.2%). The distribution of the type and number of EKG diagnostics performed in children/adolescents can be observed in Figure 1.
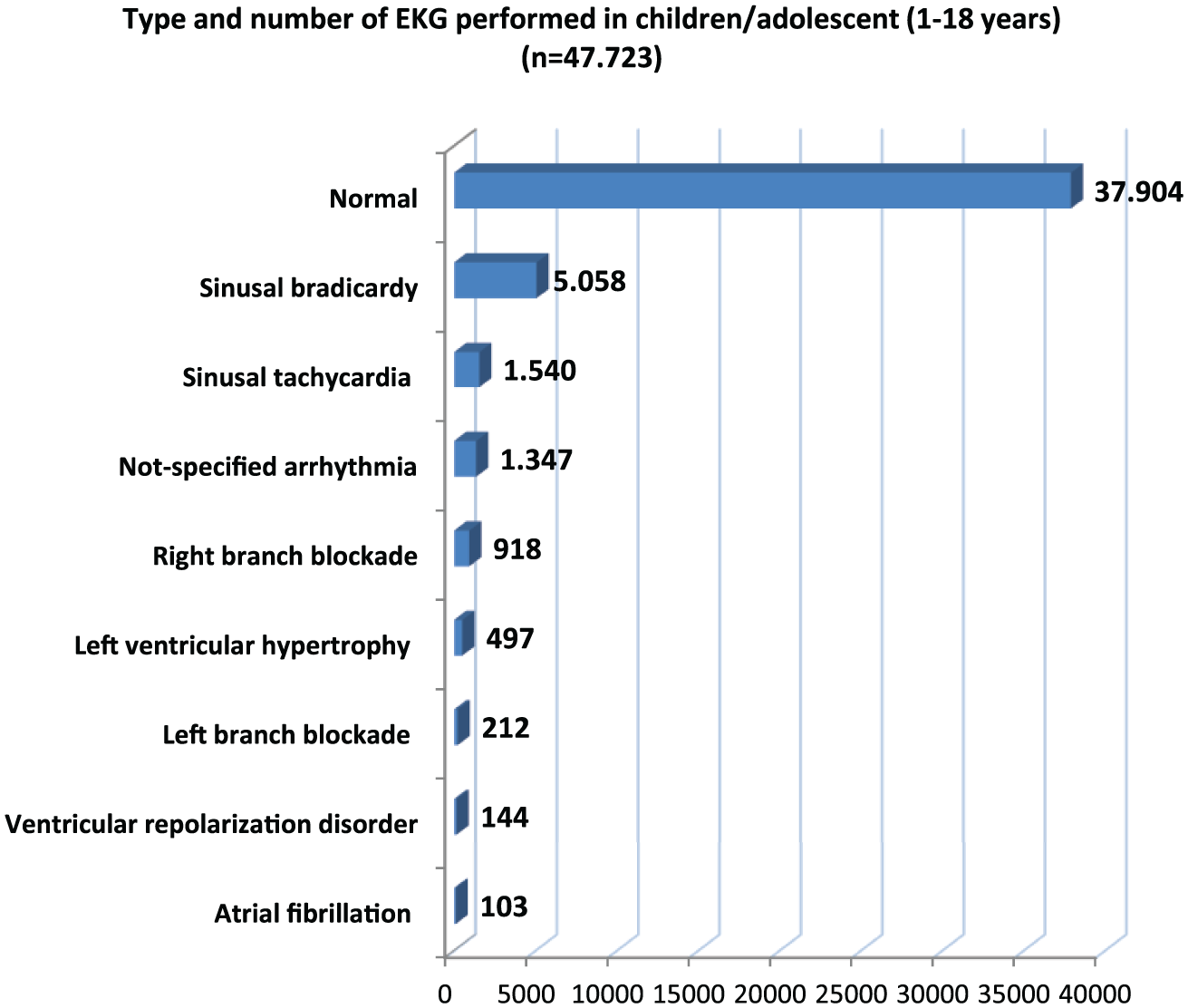
Type and number of tele-electrocardiographic studies performed in children/adolescents from January 2014 to August 2018 (n = 47,723; data from 31 January 2014 to 30 August 2018).
The analysis of the adult tests corresponded to 67% women and 33% men. The main age groups of the patients were over 60 years (31%) and between 50 and 59 years (20%). According to the analyzed results, 66.3% were normal and 33.7% abnormal.
The most prevalent abnormal heart rhythms were sinusal bradicardia (11.2%), blockade of the right branch (4.8%), and left ventricular hypertrophy (4.7%). Other less frequently detected pathologies included DVR (4.4%), sinusal tachycardia (4.4%), ischemia (1.7%), atrial fibrillation (1.1%), blockade of the left branch (0.7%), and unspecified arrhythmias (0.6%). Regarding the cardiovascular risk factors observed, arterial hypertension presented as unique factor in 25% of all the cases, association of hypertension and obesity in 40%, hypertension and diabetes in 20%, and hypertension and dyslipidemia in 19%. The distribution of type and number of EKG diagnostics performed in adults can be observed in Figure 2.

Type and number of tele-electrocardiographic studies performed in adults from January 2014 to August 2018 (n = 198,494; data from 31 January 2014 to 30 August 2018).
Evaluation of the EKG tests and development of the cardiovascular prevention program
During the analysis of the EKG tests, it was not possible to detect abnormalities like low-quality optical aberrations and low fidelity of the tracing. However, the vulnerability of the connectivity is high and dependent on the used communication technology (in our case mainly wireless). A discrepancy in the diagnostic evaluation by each center (technicians) and reviewer (cardiologist) was not determined separately, but the rate of concordance between the “gold standard” (original picture of the EKG-Device) and the Internet-transmitted picture (telemedicine platform) was determined. The average prevalence of diagnoses adjusted by centers was 92.9% (n = 246,217; 95% confidence intervals).
The average patient adherence to treatment was 2.26 per 1000 tests performed. The rate (number/thousand diagnosis) of compliance with the treatment and developed cardiovascular disease prevention plan (cessation of smoking, increase in the consumption of fruit and vegetables, and increase in the number of doctor visits in the community hospitals) was 1.47 in 2014, 2.00 in 2015, 2.71 in 2016, 2.43 in 2017, and 2.68 in 2018. Consequently, a constant increasing adherence rate was observed between 2014 and 2018. The adherence in the urban and rural communities was markedly different: 70% in the urban areas and 30% in the rural areas.
Discussion
Our results show that the telediagnostic network of the Ministry of Public Health of Paraguay can be considered a feasible tool for the diagnosis of heart disease and monitoring adherence to prevention program, with a positive cost-effectiveness for a wide territorial coverage.
The improvement in the national coverage and equal access to diagnostic technology reached through the implemented tele-EKG is in accordance with that referenced by other authors in other countries. 7 , 8 Furthermore, the telediagnostic tool provided monetary and political benefits for the population because it reduced the costs of medical assistance and transportation of patients and trained specialized staff. Moreover, the telemedicine network may be useful in implementing a contingency plan in order to provide special medical assistance in case of cardiological emergencies or to monitor the adherence to the prevention plan for cardiovascular disease patients. 7
The network model of the telediagnostic concept (web-based) allows a centralized application from any computer and in any place with access to Internet. To facilitate the technological innovation through the tele-EKG, it was necessary to develop a new diagnostic assistance protocol where a revision and improvement of the classic routine procedure was an important issue. The new improved procedure implied an innovation in the form to catch, record, transmit, and process the patient’s biological and clinical information from a scientific, legal, and ethical point of view. 8 , 9 Moreover, key factors were determined, which influenced the efficiency, reliability, transmission speed, network security, and cost-effectiveness of the telediagnosis. These factors were the representation algorithm, transmission protocol, and compaction of the pictures, as well as the information provided by the diagnostic device transmitted through the Internet to the telemedicine platform in the cloud.
According to the systematic literature review and despite the promising results obtained using telemedicine in low-income countries, 10 there is no significant evidence that telediagnosis is more cost-effective and sustainable than face-to-face diagnosis. 4 , 6 , 8 ,10,11 Most of the analyzed papers indicated the need to develop more appropriate methodologies that include the overall costs for the telemedicine implementation versus the social costs of traditional medicine (cost of transferring a patient to a place with adequate technology to make “face-to-face” diagnosis or the cost of multiplying the health teams and the technical equipments).12–39
Considering the results, it can be assumed that the used telemedicine tools offer significant advantages to draw a quick map of the prevalent cardiovascular diseases countrywide. Such advances contribute to more efficient and cost-effective care, increased patient engagement, and an influx of patient-based data to help manage better individual and population care in all regions of the country. Hopefully, universal coverage will be guaranteed to all citizens, and the elaboration of national policies for diagnosis and prevention of cardiological pathologies will be facilitated. However, before recommending its implementation, its technical and economic sustainability should be contextualized according to the epidemiological profile of each region of the country.
Conclusion
The results of this research suggest the feasibility of telemedicine as an EKG mapping tool for the diagnosis and prevention of cardiological pathologies in low-resource countries, thus enhancing cardiovascular disease surveillance and optimizing human and financial resources. Nevertheless, it is necessary to conduct a randomized controlled trial to verify the results obtained regarding better adherence to medication and the change to healthy eating habits and physical exercise in patients affected by cardiovascular diseases.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.