
Abstract
For the first time, we assess episodic simulation in a patient with visual memory deficit amnesia, following damage to visual association cortices. Compared to control participants, the patient with visual memory deficit amnesia shows severely restricted responses when asked to simulate different types of future episodic scenarios. Surprisingly, the patient’s responses are more limited in cases where the scenarios require less reliance on visual information. We explain this counterintuitive finding through discussing how the severe retrograde amnesia in visual memory deficit amnesia limits the patient’s access to episodic memories in which vision has not been a focus of their life. As a result, we argue that the deficits in visual memory deficit amnesia continue to distinguish it from amnesia after direct damage to the hippocampus.
Introduction
Recollecting one’s personal past (episodic memory) and constructing imagined or future personal events (episodic simulation) share similar cognitive and neuronal underpinnings (Hassabis, et al., 2007b; Schacter and Addis, 2007). In particular, both episodic memory and simulation are disrupted by bilateral damage to the hippocampus (Hassabis et al., 2007a, 2007b; Mullally et al., 2012). Such findings have underpinned the development of the scene construction hypothesis (Hassabis and Maguire, 2009), in which intact hippocampal function is required to construct spatially coherent, navigable scenes which form the basis of episodic processes.
However, episodic simulation requires a larger network of structures, for example, the core network (Benoit and Schacter, 2015) and ventromedial prefrontal cortex (McCormick et al., 2018) working in tandem with the hippocampus (Williams et al., 2020). In addition, some patients with hippocampal damage and severe episodic memory impairments do not show parallel impairments in episodic simulation (Hassabis et al., 2007b; Hurley et al., 2011; Maguire et al., 2010), although for these patients, remnant hippocampal activation and semantic processes were sufficient to support performance on the episodic simulation task (Mullally et al., 2012, 2014). Therefore, these patients do not provide strong evidence against the importance of the hippocampus in scene construction hypothesis. However, alongside the evidence for involvement of regions beyond the hippocampus, they highlight the need to consider episodic simulation in patients with amnesia but without hippocampal damage.
Rubin and Greenberg (1998) proposed that patients with associative visual agnosia following damage to the visual association cortices may present with a unique form of amnesia termed visual memory deficit amnesia (VMDA). VMDA is characterised by severe retrograde episodic deficits (i.e. loss of memories that were formed before injury) alongside significantly less severe deficits in anterograde memory (i.e. memories formed following the injury). It was hypothesised that this reflects the reliance of episodic memory on visual and spatial imagery. Episodic memories formed before damage to the visual cortices suffer from the loss of their central visual elements and, moreover, this loss disrupts the cascade of activation required to activate non-visual elements of the memory. This results in a severe and temporally ungraded amnesia for memories formed before the injury. Those memories formed post-injury are less reliant on the visual elements and are therefore less disrupted. One example of a patient possessing VMDA is patient MS, reported by Greenberg et al. (2005).
Because VMDA patients do not show episodic memory loss as a direct result of damage to the hippocampus, it remains unclear whether such patients will present with deficits in episodic simulation. For instance, patient MS possesses remnant hippocampal tissue in the right hippocampus (Heywood et al., 1991), similar to P01 (Mullally et al., 2012). Consequently, he might possess preserved episodic simulation abilities. However, given the loss of visual imagery in patient MS, a known component of episodic simulation (Greenberg and Rubin, 2003), it is possible that even with such remnant tissue, deficits in episodic simulation might nonetheless occur. Consequently, examining episodic simulation in patient MS offers insight into the importance of visual imagery in episodic simulation.
Therefore, this study aimed to establish whether patient MS could perform episodic simulation. To account for the visual deficits of patient MS, both visual and non-visual scenarios were used along with adaptions to self-report measures. As an older patient than many tested in such episodic simulation tasks to date, we compared patient MS’s performance with a healthy ageing control group and a young adult group to ensure that any impairment in patient MS was beyond that expected through healthy ageing.
Method
Participants
Patient MS was a 66-year-old male with visual object agnosia and amnesia. His case history has been reported in depth elsewhere (e.g. Greenberg et al., 2005; Kentridge et al., 2012). Briefly, at 23 years of age, patient MS suffered idiopathic herpes encephalitis causing left homonymous hemianopia, achromatopsia, visual object agnosia and a severe anterograde episodic memory loss. Magnetic resonance imaging (MRI) scans identified that the left occipital lobe was spared, but with some atypical signalling among white matter for infra-and-supracalcarine regions. In contrast, the right occipital lobe was extensively damaged, including the occipitotemporal junction. For the left temporal lobe, there was complete loss of the temporal pole, parahippocampal gyrus, hippocampus, amygdala and fourth temporal gyrus. However, the first to third temporal gyri were relatively spared. The right temporal lobe showed destruction of the temporal pole along with the second to fourth temporal gyri. There was also damage to the right anterior parahippocampal gyrus, but the hippocampus, posterior amygdala and first temporal gyrus appeared intact (Heywood et al., 1991). An account of his amnesia as a result of his visual memory deficit was outlined in Greenberg et al. (2005).
Fourteen participants were recruited as control participants for patient MS. These consisted of two groups: 10 younger adults (two male and eight female) and four older adults (one male and three female) matched in age to MS. Younger adults were aged between 19 and 31 years (mean (M) = 22.80, standard deviation (SD) = 3.79), with 14–21 years of education (M = 16.80, SD = 2.10) and were recruited through a participant pool, for which they gained course credit. The older adults were aged between 59 and 63 years (M = 61.00, SD = 1.83), with 9–17 years of education (M = 11.75, SD = 3.59, cf. approx. 9–10 years of education for patient MS) and were recruited through opportunity sampling and were not offered incentives to take part. All participants were native English speakers, not presenting with a history of neurological disease, mental health problems or any drug or alcohol dependency. All participants provided informed consent.
Older adults possessed significantly fewer years of education compared to younger adults, U = 6.00, z = −1.99, and p = 0.047 (two-tailed). These older adults were matched with MS based on age, t(3) = 2.44 and p = 0.092 (two-tailed).
Episodic simulation task
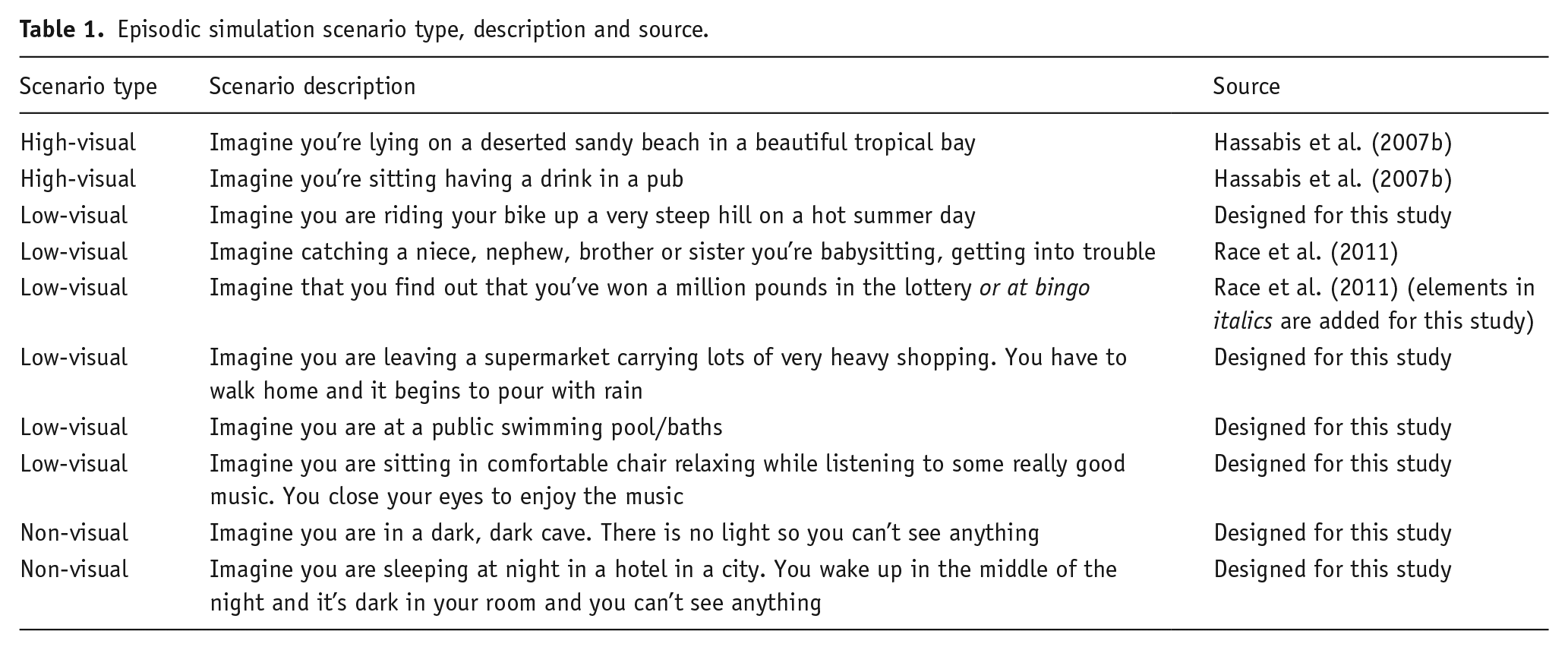
This task was adapted from Hassabis et al. (2007b). A total of 10 scenarios were presented to participants who were asked to imagine and describe their experiences. Of those 10 scenarios, four were taken from previous experiments (Hassabis et al., 2007b; Race et al., 2011) and the other six were designed for this study. Scenarios were split into three groups: high-visual (two scenarios), low-visual (six scenarios) and non-visual (two scenarios). Instructions for all scenarios were the same and participants were guided to include a range of sensory information (visual, auditory, etc.) as well as emotional and spatial information. Nonetheless, the scenarios differed in the extent to which each might innately cue visual information. High-visual scenarios were taken from Hassabis et al. (2007b) and would allow participants to describe visual stimuli easily (i.e. they allowed for a wide variety of visual information to be described). Low-visual scenarios implicitly directed participants towards non-visual elements of a scene (e.g. emotion, sounds, and touch), yet the event occurred in the light and visual elements could, therefore, easily form part of a coherent experience, even though that visual experience might be somewhat limited. For example, in a swimming pool, the types of visual information are somewhat restricted – the experience is inside a room, sightlines are restricted and there are fewer visual features, while there are obvious tactile and auditory stimuli which feature strongly in most constructions of this scenario. Two low-visual scenarios came from Race et al. (2011) and three were developed for this experiment. The two non-visual scenarios were developed for this experiment to accommodate the visual deficits of MS. Both scenarios occurred in the dark and therefore explicitly steered participants to using non-visual elements of a scene to produce a coherent experience (i.e. while visual elements were possible, the darkness meant that other sensory elements of the scene were likely to be the dominant feature of such constructions). Each scenario is outlined in Table 1.
Episodic simulation scenario type, description and source.
Procedure
Participants were asked to complete 11 scenarios (10 unique scenarios and the first scenario repeated at the end of the experiment to explore any performance change). To allow direct comparison with patient MS, all older participants and half the younger participants were given the same scenarios in the same order as patient MS. The remaining five younger participants were given the scenarios in a different order to ensure testing order had no role in the results obtained. To control for fatigue, patient MS was tested across 3 days, while controls were tested on all scenarios on the same day, but with two 10-min breaks after the fifth and tenth scenarios, respectively. Although this led to a difference in the timescale for testing in patient MS and the control participants, we believe that it reduced the chances of control participants planning their responses to future sessions in light of previous testing; an option not likely in patient MS because of his amnesia.
All participants were tested individually with sessions recorded for later transcription and scoring. To begin, participants were provided with explicit instructions regarding the task requirements. The experimenter gave an apparently spontaneous example of what an episodic simulation might be like, using the example from Hassabis et al. (2007b) which deliberately highlights different types of content (e.g. auditory or tactile). As patient MS was tested over three sessions and has a memory deficit, this example was repeated at the start of each session. Participants were asked whether they understood the instructions and what was expected. Once it was verified that participants had understood, the test phase began.
For each scenario, the description was read aloud to the participant upon which they were instructed to imagine the cued situation and describe this in as much detail as possible. Participants were instructed to not rely on a previous experience, instead creating a new imagined experience. They were also provided with a printed card placed upon the desk in front of them containing the scenario, acting as a reminder should that be required. There was no time limit on the length of descriptions, with participants being able to finish their description whenever they felt nothing else could be added. The interviewer was able to probe further into the experiences using a set of clearly defined questions for specific situations and which had been previously implemented in other experiments (Hassabis et al., 2007b; Race et al., 2011) with some modifications, again to account for patient MS’s visual deficits. The aim of the probes was to encourage further description. For instance, to garner further information when poor detail was provided (e.g. ‘Can you imagine anything else?’), more specific information on elements of their experience (e.g. ‘Can you tell me anymore about X?’) or even to encourage spatial coherence (e.g. ‘Imagine the whole situation, what else is going on?’).
Scoring
The scoring paradigm was the same as that used by Hassabis et al. (2007b) except the spatial coherence index was excluded. The spatial coherence index requires participants to respond about the nature of visualisation on the basis of scenes or objects, and it was decided that patient MS’s visual object agnosia would interfere with reliable measurement on this scale. Without this scale, we were unable to complete the overall experiential index, as reported by Hassabis et al. (2007b), but all other components of the scale were completed and we therefore report a modified experiential index (herein referred to as experiential index) which comprises all measures and scoring from Hassabis et al. but without the addition of the spatial coherence index.
Transcripts were scored by the experimenter based on the criteria set out in Hassabis et al. (2007b). For each scenario, content analysis was performed on four types of description: sensory details; entities present; spatial references; and thoughts, emotions and actions (TEA). Each of these sub-components was capped at a maximum score of 7, meaning a total score of 28 could be achieved. This capped score allowed comparability across participants irrespective of the length of their individual contributions. Although no verbal fluency measure was taken, individuals varied in the length of their responses. However, most control participants met or approached the capped score for these elements, meaning that differences in response lengths did not add variability to the data. Patient MS found the task extremely demanding and needed frequent prompting to continue his descriptions. In order that excessive prompting did not impact results, for all participants, only the information provided after the scenario was set and after the first three probes counted towards the content score. In addition, unexpectedly patient MS failed to be able to provide responses to the non-visual scenarios. He was unable to generate even limited description of the scenarios and became apparently anxious in attempting to do so. Therefore, although both non-visual scenarios were presented to patient MS, they were ended quickly and no response recorded.
The scorer provided a score from 0 (devoid of details with no sense of experiencing) to 10 (richly detailed and likely emerged from a vividly imagined experience). This score was then multiplied by 1.8 so that the scale ranged from 0 to 18. As such, the maximum quality score value was 18. Finally, participants completed a questionnaire on their self-reported experiences of vividness, detail, sense of presence, similarity to other memories and difficulty of generating the scene for each descriptor. All of these were scored on a Likert-type scale from 1 to 5 (e.g. 1 being no sense of presence and 5 being a strong feeling of presence). However, only vividness and sense of presence were included for the experiential index and rescaled from 1–5 to 0–4, meaning an additional 8 points could be obtained from these self-report measures. Therefore, the experiential index score equation is calculated by summation of content score (out of 28), richness score (out of 18) and self-report (out of 8), leading to a maximum value of 54.
Results
Transcriptions of the recordings of all participants were scored for content by a single experimenter. All of patient MS’s responses and a random sample of four participants’ responses (two from the older and two from the younger control groups) were also scored by a second experimenter. In line with previous studies (e.g. Hassabis et al., 2007a, 2007b), a 2 × 4 analysis of variance (ANOVA) (scorer × content measure) showed no main effect of scorer (F(1,4) = 1.084, p = 0.36) and no interaction of scorer and content type (F(3,12) = 1.790, p = 0.20).
Comparison of control participants
Analyses were undertaken through JASP 0.12.0 (2020). Any null results are reported with Bayes Factors (BF10) and computed using default priors. For ANOVA, the shape parameter (r) of the prior distribution was 0.50, with an r scale covariate of 0.35. For t-tests, the Cauchy prior of 0.707 centred at 0 was used. Finally, Kendall’s tau-b analysis used the stretched beta prior width of 1. For all analyses, some caution should be taken, given the unbalanced design and small sample size (Shaw and Mitchell-Olds, 1993).
A 2 (age group: younger versus older) × 3 (scenario type: non-visual, low-visual and high-visual) mixed ANOVA was computed to assess differences in experiential index scores in the control groups. Due to concerns about sample size causing difficulties with assessing model assumptions, Greenhouse–Geisser correction was applied. Omega-squared effect sizes are reported with mixed ANOVA to account for the small sample (Albers and Lakens, 2018). Post hoc analyses applied Bonferroni–Holm correction to control for familywise error.
There was a main effect of scenario type, F(1.86,22.31) = 9.11, p = 0.002, ω2 = 0.14 with post hoc tests revealing that experiential index scores were significantly better in the high-visual (M = 43.34, SE = 1.51) compared to the non-visual scenarios (M = 36.08, SE = 1.60; p < 0.001). However, there was neither significant difference between low-visual (M = 39.64, SE = 1.52) and non-visual (p = 0.073, BF10 = 1.06) scenarios nor between high-visual and low-visual scenarios, although this was very close to significance (p = 0.051, BF10 = 2.15).
No main effect of age was found (F(1,12) = 0.11, p = 0.745, ω2 = 0.00, BF10 = 0.49) and there was no interaction between scenario type and age (F(1.86,22.31) = 0.52, p = 0.589, ω2 = 0.00, BF10 = 0.43). As age did not show a significant influence on performance, the control data were collapsed into a single group to increase statistical power for the remaining analyses.
To assess whether the order in which scenarios were presented impacted results, younger control participants were tested with either the same or a different testing order to patient MS. A Welch’s t-test was computed, with Hedges g reported as an effect size estimate. Collapsed across all scenario types, it was found that there was no significant difference in experiential scores between testing the same (M = 41.99, SE = 1.53) or different (M = 39.06, SE = 2.02) orders, t(7.46) = 1.16, p = 0.284, g = 0.66, BF10 = 0.73. Therefore, all control data were considered together irrespective of testing order.
Kendall’s tau-b analyses were computed to assess how performance on each scenario type was influenced by perceived task difficulty. For all tests, there was no significant correlation between perceived difficulty and scenario type performance (p ⩾ 0.182, BF10 ⩽ 0.81). There was also no evidence of practise effects, with the first (M = 41.50, SE = 1.89) and final (M = 43.96, SE = 1.51) scenarios showing no significant difference in their experiential index scores, t(13) = 1.39, p = 0.187, d = 0.37, BF10 = 0.60.
Comparison of patient MS and control participants
When comparing MS and controls, a modified t-test was used (Crawford and Garthwaite, 2002, 2005; Crawford and Howell, 1998); this treats an individual patient’s score as a sample, allowing for comparisons with a control group. Furthermore, a point estimate of the average difference, based on classical z-score reports, represented as zcc (Crawford et al., 2010) is also reported along with 95% confidence intervals (CIs).
Figure 1 shows the performance of controls and patient MS across all scenario types. Patient MS showed a clear deficit in comparison to controls for both the high (p = 0.001, zcc = −4.31, 95% CI (−6.01, −2.58)) and low (p = 0.004, zcc = −3.56, 95% CI (−5.01, −2.10)) visual scenarios. However, patient MS did not fulfil the criteria for a dissociation between high- and low-visual scenarios, t(13) = 0.68, p = 0.508, zcc = −0.76, 95% CI (−2.73, 1.14), suggesting an equivalent level of deficit on both scenario types. Patient MS did not complete any non-visual scenarios, meaning statistical comparison of these scenarios was not possible.

Mean experiential index score for each scenario type for control participants and patient MS. Patient MS was unable to complete the non-visual scenarios and so no data are present. Blue dots represent younger age controls and yellow dots represent older age controls. Error bars represent 95% CI of mean.
Due to ceiling effects in some of the sub-components of high-visual scenarios, comparing a breakdown of the sub-components was not undertaken. Instead, both the controls and patient MS’s data were collapsed into an overall experiential index, ignoring scenario type to allow for sub-component analysis. Doing so found significant deficits in patient MS’s reporting of sensory details (p < 0.001, zcc = −8.27, 95% CI (−11.44, −5.08)), entities present (p < 0.001, zcc = −5.14) and TEA (p < 0.001, zcc = −8.51, 95% CI (−11.78, −5.24)). However, no significant difference was observed between patient MS and controls for spatial references, t(13) = 1.37, p = 0.194, zcc = −1.42, 95% CI (−2.16, −0.65). These comparisons are shown in Figure 2.

Mean sub-component scores across all scenarios for both control participants and patient MS. Blue dots represent younger age controls and yellow dots represent older age controls. Error bars represent 95% CI of mean.
For self-report measures, patient MS reported similar scores to control participants for perceived task difficulty (p = 0.477, zcc = −0.76, 95% CI (−1.35, −0.15)), salience (p = 0.212, zcc = −1.36), sense of presence (p = 0.758, zcc = −0.33, 95% CI (−0.22, 0.86)) and similarity to previous memories (p = 0.195, zcc = −1.42, 95% CI (0.65, 2.15)). However, patient MS did self-report significantly lower levels of detail in his simulated events (p = 0.018, zcc = −2.82, 95% CI (−4.00, −1.62)). In addition, patient MS’s quality judgement scores (from experimenter scoring) were significantly lower than that of controls (p = 0.003, zcc = −3.69, 95% CI (−5.18, −2.19)). Therefore, patient MS reports similar introspective experiences to control participants for most measures but shows a lack of detail in his imagined experiences and in the quality of his descriptions. Comparisons of patient MS’s responses to a scenario can be seen in Figure 3, alongside responses to the same scenario from two control participants.
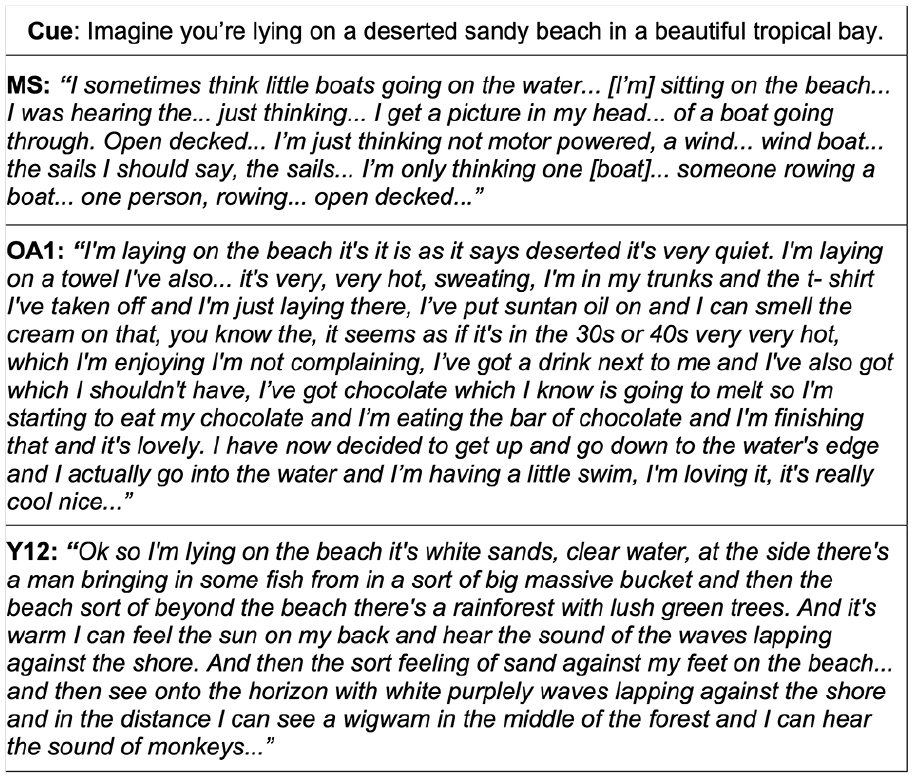
Example of descriptions provided by patient MS, an older adult (OA1) and a younger adult (Y12) in response to the same cue.
Overall, the data suggest that age likely had little impact on performance on the task. Patient MS had severe deficits in imagining fictitious scenes in both high- and low-visual scenarios and was unable to complete non-visual scenarios. However, there was no dissociation between patient MS’s performance for high and low-visual scenarios. Patient MS also showed deficits in almost all of the four content elements of the experiential index, suggesting that patient MS (similar to other amnesic patients) can no longer produce coherent imagined scenes.
Discussion
This study provides the first evidence that a patient with VMDA shows significant problems in simulating episodic experiences. The mechanism of VMDA is distinctly different to medial temporal lobe (MTL) amnesia in which the hippocampus is at least partially intact, but the visual object agnosia leads to problems in integrating visual information into anterograde memories (Greenberg and Rubin, 2003). Here, in patient MS (a patient with visual object agnosia and VMDA; Greenberg et al., 2005), we show that there are significant problems in many components of episodic simulation.
The finding that age had little impact on performance on this task is in stark contrast to the findings of Rendell et al. (2012), who showed that older adults has poorer episodic simulation compared to younger adults. It is well documented that with age comes cognitive changes, including poorer episodic memory (e.g. Morcom and Friston, 2012; for review, see Salthouse, 2009), an ability closely tied to episodic simulation (e.g. Hassabis et al., 2007b; Schacter et al., 2008). However, in this study, the mean age of the sample was 61 years, and the evidence shows that below the age of 65 years, cognitive decline is not easily detected (Salthouse, 2009). Thus, these results do not necessarily contradict the findings of Rendell et al. (2012), but indicate that older adults in this research may not be of sufficient age to show detectable impairment in the task. As a result, we can also be confident that patient MS’s poor performance is not a result of his age alone.
As with his episodic memory (Greenberg et al., 2005), patient MS reported his episodic simulation to lack visual and contextual detail, making his overall profile highly similar to those of patients with MTL amnesia on similar tasks (Andelman et al., 2010; Hassabis et al., 2007b; Race et al., 2011; Rosenbaum et al., 2009). Due to his visual object agnosia, we could not assess patient MS on the spatial coherence of his episodic simulations. However, patient MS did not differ from control participants in self-reported measures of salience, sense of presence or similarity to previous memories, though he did report a reduced level of detail to his simulations.
Unlike MTL amnesia, MS and other VMDA patients present with greater retrograde than anterograde memory deficits (Greenberg et al., 2005; Rubin and Greenberg, 1998), with anterograde memories still being produced, though sparse and lacking a visual component. As such, the severe lack of retrograde memories and milder (though still severe) anterograde memory deficit may mean patient MS has only relatively recent memories available to support the simulation of novel episodic experiences. It has been argued (e.g. Addis and Schacter, 2012) that when simulating an experience we may rely on available episodic experiences. We might, therefore, expect patient MS to only have access to visually restricted episodic reserves because of his greater retrograde amnesia. In this case, patient MS would have better episodic simulation for events which have less reliance on visual information.
It was, therefore, surprising that patient MS showed significant anxiety at being asked to produce responses for the non-visual scenarios (e.g. imagining being in a dark cave), leading to him not being able to be tested on these scenarios. Although these non-visual scenarios produced lower modified experiential index scores for control participants, these scores were not related to perceived task difficulty. Therefore, difficulty alone cannot explain why patient MS found simulating non-visual scenarios so hard. Instead, patient MS’s reliance on his recent store of limited episodic experiences may paradoxically drive his simulations towards the visual domain. Despite (or perhaps because of) his visual object agnosia, patient MS is highly aware of his vision and the visual modality of his memories. For example, for the scenario of imagining waking in a dark hotel room in the middle of the night, he was unable to produce any response. When prompted beyond the task to imagine lying there with his eyes shut, he responded ‘when I’m awake I have my eyes open all the time’. This heightened focus on the visual elements of the world means that patient MS’s recent memories (which he is using to simulate these episodic events) are primarily visual in nature. Episodic memories with less focus on visual elements are likely to come from before his visual object agnosia, and therefore fall within his severe retrograde amnesia. These memories will therefore be unavailable to him for simulating new episodic experiences, leading to this surprising difficulty in simulating non-visual scenarios where vision plays little part.
Patient MS’s focus on the visual domain can also be seen in the low-visual scenarios. Unlike control participants, patient MS shows no difference in performance on these scenarios compared to the high-visual scenarios. There are two potential explanations for this finding. Patient MS has very impoverished responses to all scenarios meaning differences may not be observable because of floor effects in his modified experiential index. However, beyond this, we see that as for the non-visual scenarios, in these low-visual scenarios, patient MS has a tendency to focus on visual elements of the simulation. For example, by imagining cycling up a hill on a hot day (a scenario developed to allow focus on elements such as physical exertion, the feeling of sweat and the warm sun, etc.) patient MS focuses strongly on several visual elements of the scene such as ‘I’m just thinking [about the bike] with dropped handlebars’.
Therefore, patient MS has a poor ability to construct such episodic simulations. When he does construct such simulations, they are primarily reliant on a repository of episodic information based on relatively recent memories. The lack of visual and contextual information within these memories is not, however, sufficient to overcome the problems in generating these events as control participants do. The lack of episodic memories dating before his visual object agnosia also means all his episodic simulations are driven by episodic memories which lack visual information. Nonetheless, while these memories lack visual information, the visual information that remains is a point of focus for patient MS. Therefore, when patient MS does attempt episodic simulation the only episodic information available to him is lacking visual detail, but he primarily focuses on what visual detail remains. The result is that when patient MS is directed to construct an episodic simulation which is lacking visual information (i.e. the non-visual scenarios), he finds this extremely difficult.
It should be considered that the non-visual scenarios which patient MS showed so much difficulty do not only differ from other scenarios in the nature of the potential visual content. The scenarios with lower (or no) visual content were also potentially less plausible and less likely to be similar to previous experiences of the participant. However, we do not believe this can explain the pattern of data that we see. Low likelihood scenarios such as winning a million pounds were in the low-visual scenario condition and patient MS did not struggle to respond to these scenarios (even though his experiential index scores were poor). In contrast, patient MS did not manage to produce a response to non-visual scenarios even when they were relatively likely to be related to previous experiences (such as waking in a dark hotel room). For the same reasons, we believe it unlikely that any potential semantic memory impairment in patient MS as a result of damage to the anterior temporal poles can explain the pattern of impairment. It is also important to consider the possibility that some scenarios lend themselves to scene generation more than others and that this may be truer for the non-visual scenarios which patient MS struggled most with. However, there is little evidence that these scenarios generated poor simulations in any of the control participants; control participants were able to both report content of these scenes and a rich experience for them. Rather, it is most likely the visual elements of these scenes which differentiate them on the basis of patient MS’s performance.
One other finding of note is that patient MS showed no difference from control participants in spatial referencing within his episodic simulations. However, we offer a note of caution here. As can be seen in Figure 2, although patient MS is not significantly different from controls, his scores are lower, and the variability in performance of control participants is greater for this measure than other content components of the modified experiential index. Spatial references were also the only content component of the score to come off ceiling levels in the control participants. We therefore caution that this apparent performance within normal limits for patient MS may actually reflect surprisingly low performance on this score in control participants. This perhaps reflects spatial referencing difficulties in the low-visual and non-visual scenarios used in this task. With reduced visual referencing, we cannot be sure that spatial referencing is not also reduced. Therefore, we cannot be certain from these data whether patient MS shows impairments in spatial content of these episodic simulations.
These findings demonstrate that a VMDA patient with an amnesia arising from the loss of visual inputs to mnemonic shows poor performance on episodic simulation tasks. However, the presentation of deficits in VMDA remains distinct from the deficits of patients with amnesia as a direct result of damage to the hippocampus.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported in part through a Leverhulme Trust Research Fellowship to A.E.