
Abstract
Objectives:
To explore the within-person fluctuations of fatigue in systemic sclerosis and its association with negative affect, positive affect, pain, perceived exertion of physical activity and quality of sleep.
Methods:
We performed an ecological momentary assessment study in adult patients with a clinical diagnosis of systemic sclerosis. During 14 days, patients completed daily assessments of fatigue severity, negative affect, positive affect, pain, quality of sleep and perceived exertion of physical activity at four fixed time points. The day-to-day fluctuations in fatigue were quantified by the intra-individual variance and probability of acute change, capturing the magnitude and frequency of clinical relevant within-person day-to-day fluctuations, respectively. Using multilevel models, the within-person association between fatigue and the daily assessments were analysed.
Results:
Fifty-seven patients with systemic sclerosis participated. The mean (standard deviation) intra-individual variance was 1.08 (0.42) and the probability of acute change was mean (standard deviation) 0.40 (0.14), ranging from 0.08 to 0.77. For fatigue, a within-person variation of 51% was observed. Multilevel analyses showed that higher average levels and daily increases in negative affect, pain and perceived exertion of physical activity were associated with more fatigue, while the opposite was observed for positive affect and quality of sleep. Positive affect demonstrated the strongest association with fatigue fluctuations.
Conclusion:
This is the first quantitative study showing that fatigue in systemic sclerosis is characterized by a dynamic course and that approximately half of the day-to-day fluctuations within persons are clinically meaningful. Furthermore, our results indicate that integrating activities with positive impact on mood into fatigue treatment strategies might reduce the frequency of fatigue fluctuations.
Significance and innovations
* This is the first quantitative study confirming the existence of within-person fatigue fluctuations in systemic sclerosis.
* Large intra-individual differences exist in the magnitude and frequency of fluctuations in fatigue.
Background
Systemic sclerosis (SSc) is characterized by a triad of inflammation, vascular damage and fibrosis. The disease course in SSc is unpredictable and could affect the skin and multiple internal organs. 1 To date, the treatment con-sists of modifying the disease course as there is no cure available. 2 The large impact on physical health and unpredictable prognosis has repercussions on emotional and social well-being 3 with fatigue being the largest burden experienced by patients.4,5 Fatigue significantly impacts various domains of daily life, including working ability,6,7 social functioning 8 and parenting. 9 Approximately half of the patients with SSc experience severe fatigue. 10
The management of fatigue is a great unmet need for patients. Clinically fatigue is a challenge to treat as it is a multi-factorial problem involving different biological, physiological, psychosocial and behavioural mechanisms, whereby little is known about the interplay between these determinants. 11 Different cross-sectional and longitudinal studies have been initiated to gain more insight into the determinants of fatigue in SSc. Cross-sectional studies have reported that patients with more pain, higher levels of negative affect, poorer sleep quality, less physical activity, smaller social network, higher disease severity, and lower quality of life experience more fatigue.3,8,12–16 So far, two longitudinal studies have evaluated the course of fatigue in SSc and observed that fatigue remained stable over 3–11 years.17,18 In qualitative studies, in contrast, it has been reported that patients experience fatigue as a fluctuating, unpredictable symptom that negatively influences multiple domains of life.7,9,19–21
Given the impact of fatigue, more insight into the dy-namic nature of fatigue is warranted to understand how disease symptoms and psychosocial factors are associated with individual levels of fatigue. This knowledge will not only enhance our understanding of the dynamic nature of fatigue but will also guide the development of more tailored and adaptive intervention strategies. To elucidate its fluctuating behaviour, it will be advantageous to study the course of fatigue within a person, since the course of fatigue might vary between individuals, which might be obscured on a cohort level.11,17,18 The aim of this study was to examine the within-person fluctuations of fatigue in SSc as well as its association with negative affect, positive affect, pain, perceived exertion of physical activity and quality of sleep. We hypothesized that fluctuations in negative affect, pain and perceived exertion of physical activity are positively associated with within-person fluctuations of fatigue, while positive affect and quality of sleep will be negatively associated. Furthermore, we wanted to explore if we could characterize subgroups of patients with different frequencies of fluctuations in fatigue.
Patients and methods
Study design
Patient population and characteristics
A prospective, ecological momentary assessment study was performed at the Department of Rheumatology in the University Medical Centre Nijmegen. 22 Patients meeting the following inclusion criteria were asked to participate: a clinical diagnosis of SSc, having a pulmonary function test within 3 months of inclusion with a vital capacity and diffusing capacity of the lung for carbon monoxide (DLCO) >50%, age ⩾18 years, and a life-expectancy >1 year based on the judgement of experienced physician. Patients who were diagnosed with pulmonary hypertension or a malignancy in the past 5 years (except basal cell carcinoma) and patients without a smartphone device or Internet access were excluded. Based on prior sample size calculation, we aimed to include 60 patients in our study (see Supplementary Data S1). The study was conducted in accordance with the Declaration of Helsinki, and the Institutional Review Board of the Radboud University Medical Centre, Nijmegen, determined that the study was not subject to the Dutch Medical Research Involving Human Subjects Act (dossier number 2021-13157). All participants gave written informed consent.
Procedure
Patients fulfilling the inclusion criteria scheduled to visit the outpatient department were approached via phone to provide information about the study. Patients interested in participating were included subsequently between 8 March 2022 and 31 August 2022 after obtaining informed consent. During the baseline visit, participants were instructed to install a smartphone application to complete the daily assessments (Improve app, NEN7510 and ISO 27001 certified) and were provided an opportunity to use the app as intended for the study. 23 At this visit, patients chose the start date of the daily diary assessments. Using a fixed-interval measurement schedule with evenly spaced time points carefully selected together with patient partners, participants received notifications at 9 am, 1 pm, 5 pm and 9 pm to complete combinations of single-item questions about fatigue, negative affect, positive affect, pain, perceived exertion of physical activity, and quality of sleep for 14 days. A 14-day study duration was chosen after consulting with our patient partners to minimize the burden on patients, while still capturing the fatigue fluctuations. Patients were asked to rate fatigue, affect, pain and quality of sleep (only at 9 am) using a numeric rating scale (NRS) ranging from 0 to 10; while the perceived exertion of physical activity was assessed on a Borg scale ranging from 0 to 10 (0: no exertion at all, 10: maximal effort). The occurrence of overwhelming fatigue (yes/no) was assessed at 9 pm with a single-item question (see Supplementary 2). Participants had half an hour to respond to each notification initiated at the fixed time points.
At baseline, participants completed questionnaires regarding health-related quality of life (Scleroderma Health Assessment Questionnaire (SHAQ)), anxiety and depressive symptoms (Hospital Anxiety and Depression Scale (HADS)), quality of sleep (PROMIS SF 6a for sleep), fatigue severity and impact of fatigue in daily life (Functional Assessment of Chronic Illness Therapy – Fatigue Subscale (FACIT-FS)) and the types of intensity of physical activity (International physical activity Questi-onnaire SF7 (IPAQ-SF 7))24–28 (see Supplementary S2 for details on questionnaires).
At baseline, highest educational level (according to UNESCO International Standard Classification of Edu-cation 2011), living status and occupational status were assessed. 29 Other demographic characteristics, disease characteristics and comorbidities (including previous COVID-19 infections) at baseline were collected from medical records.
Statistical analyses
Within-person day-to-day fluctuations of fatigue
The prevalence of overwhelming fatigue was calculated by the mean number of times overwhelming fatigue occurred during the 14-day period. The day-to-day fluctuations of fatigue were assessed using the intra-individual variance (iSD) and the probability of acute change (PAC). 30 The iSD captures the variability in fatigue that can occur within a single individual over time, whereas the PAC captures the occurrence of significant changes across observations. The minimal clinical important difference (MCID) for fatigue in rheumatoid arthritis was used as cut-off to identify a clinically meaningful fluctuations in fatigue, −1.12 for improvement and of 1.26 for worsening, as no MCID for fatigue in SSc is known. 31 In addition, the correlation between the iSD and PAC was assessed with the Pearson correlation coefficient.
We assessed differences in patient-related features between patients with a low frequency of clinically meaningful fluctuations (<mean PAC) and patients with a high frequency (⩾mean PAC) of clinical meaningful changes using the t-test, Mann–Whitney U test, and Fishers’s exact test as appropriate. To account for multiple testing, a Bonferroni correction was applied.
Association between within-person fluctuations of fatigue and daily determinants within days and across days
Likelihood ratio tests demonstrated that fatigue and the determinants from the ecological momentary assessment, except quality of sleep, were clustered at 3-levels (i.e. observation, day, and patient). Using multilevel mixed models with residual maximum likelihood, we analysed the association between within-person fluctuations of fatigue and the following determinants: negative affect, positive affect, pain, perceived exertion of physical activity and quality of sleep. The significance of fixed effects and confounders was evaluated with Wald tests using Satterthwaite denominator degrees of freedom, whereas the significance of random effects was evaluated with likelihood ratio tests.
First, the association between time and fatigue was established by assessing the need for fixed and random effects for time (linear and quadratic). After establishing the best model for the association between fatigue and time, a separate multilevel model was constructed for each daily diary assessment. Before entering the determinants from the ecological momentary assessment into the model, they were disaggregated into a level 1 variable representing the within-person within-day fluctuation (i.e. observation minus mean of observations of specific day of that patient), level 2 variable representing the within person between day fluctuation (i.e. mean of observations of specific day minus mean of observations of that patient over 14 days) and level 3 variable (i.e. mean of patient over 14 days). The level 3 variable was centred using the grand mean. Each level of the determinant from the daily diary assessment was added as a fixed effect. Next, the need for a random effect was evaluated for the level 1 determinant first over days and then over patients. Subsequently, the need for a random effect for the level 2 determinant over patients was assessed. Thereafter, sex, age, body mass index (BMI), and the presence of COVID-19 history were assessed for confounding with the change-in-estimation approach using a cut-off point of 10%.32,33
All statistical tests were performed two-sided (α = 0.05), and all analyses were carried out using Stata statistical software version 17.
Results
In total, 57 of the 60 included patients completed the ecological momentary assessment study (Figure 1). De-mographic and clinical characteristics of the study sample are shown in Table 1. The mean (SD) age of the study sample was 54.3 (14.6) years with a male: female ratio of 1:2. A total of 29.8% had diffuse subtype of SSc, and the mean (SD) disease duration was 6.9 (4.8) years.
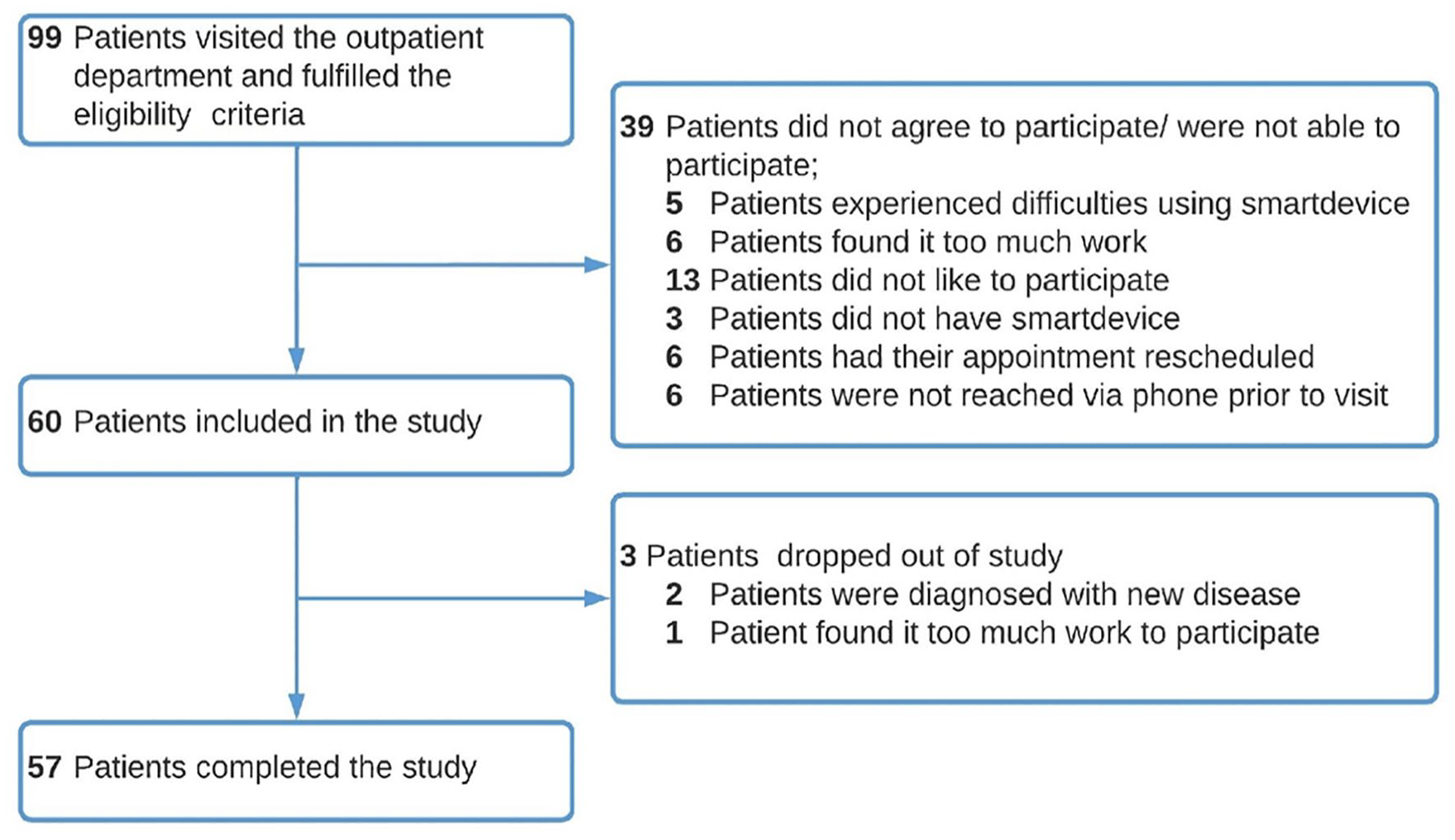
Flowchart.
Demographic and disease characteristics at baseline in study population.
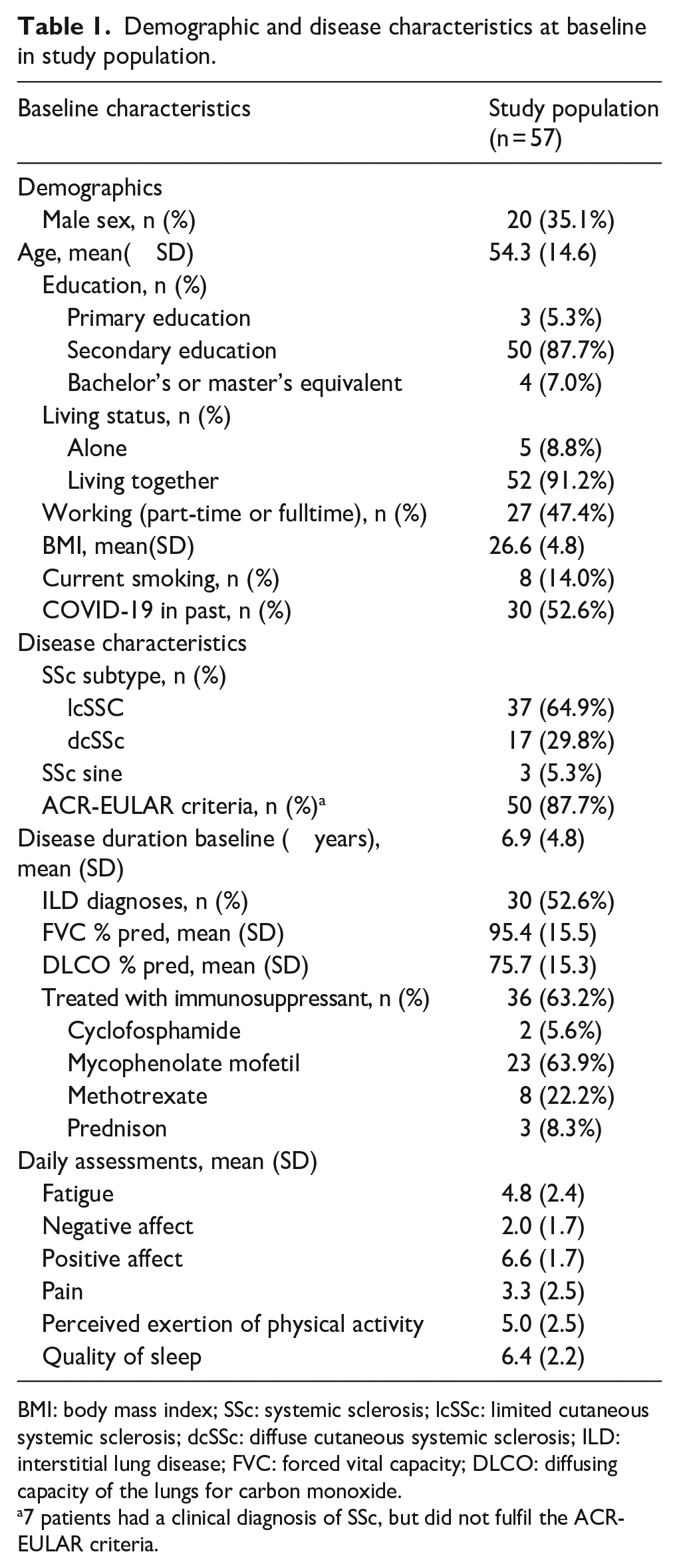
BMI: body mass index; SSc: systemic sclerosis; lcSSc: limited cutaneous systemic sclerosis; dcSSc: diffuse cutaneous systemic sclerosis; ILD: interstitial lung disease; FVC: forced vital capacity; DLCO: diffusing capacity of the lungs for carbon monoxide.
7 patients had a clinical diagnosis of SSc, but did not fulfil the ACR-EULAR criteria.
Day-to-day fluctuations of fatigue
In total, 81% of all observations were completed. The prevalence of overwhelming fatigue on an individual level was 23.7% during the study period of 14 days, with a range between 0.0% and 84.6%. The iSD mean (SD) was 1.08 (0.42) and the PAC was mean (SD) 0.40 (0.23), meaning respectively, that on average a fluctuation in fatigue between days deviated 1.08 SD from the person’s mean and that on average 40% of the fluctuations (i.e. 5 out of observed day-to-day fluctuations) were clinically meaningful. A high correlation between the iSD and PAC (r = 0.75, p < 0.001) was found. As shown in Figure 2, the iSD captures the amplitude of the fluctuations, whereas the PAC captures the frequency of clinically meaningful fluctuations.
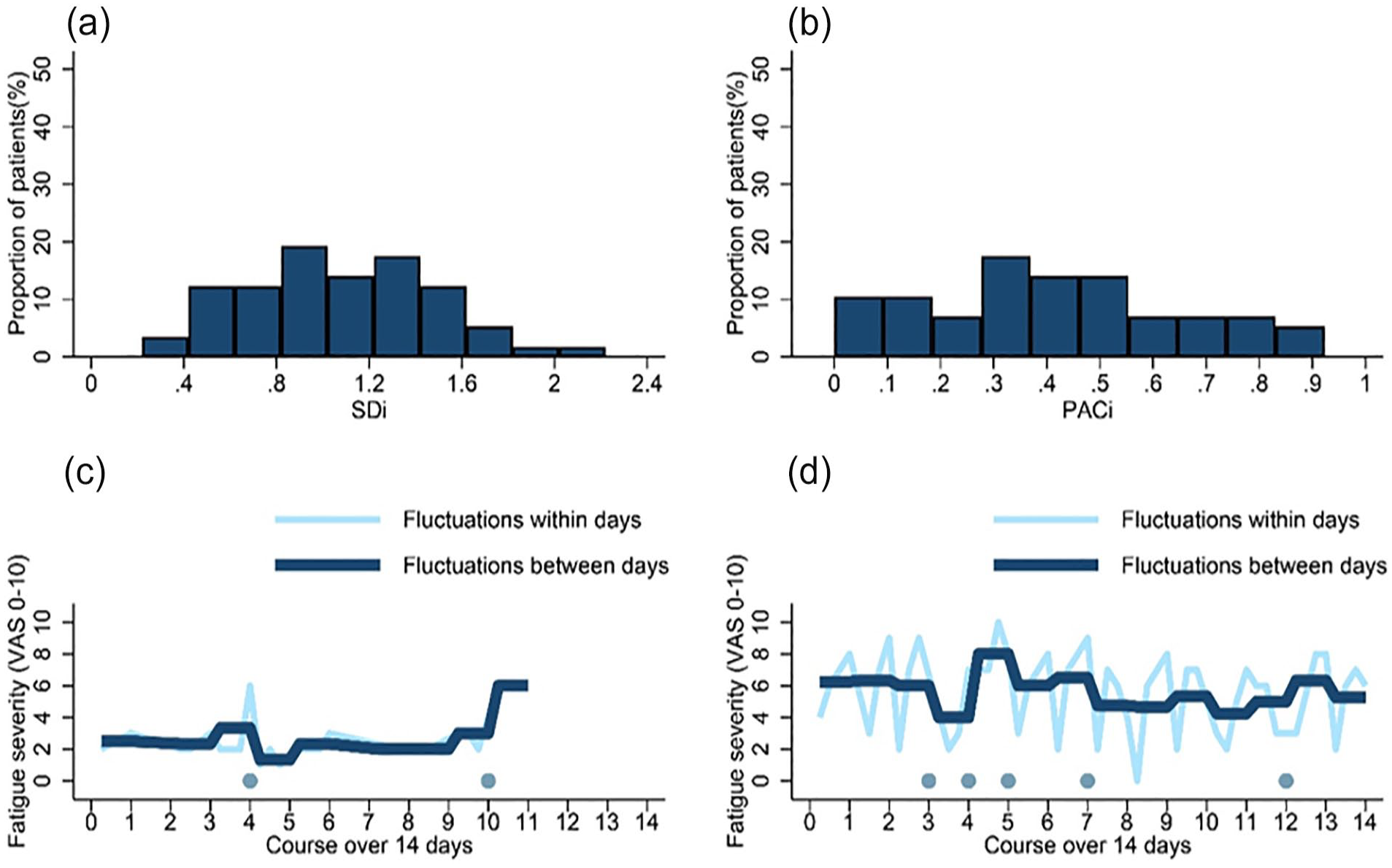
Overview of iSD and PAC in study sample (N = 57) with two examples. (a) Range of iSD in sample. (b) Range of clinical meaningful fatigue fluctuations captured by PAC in sample. (c and d) Illustration of fluctuations of fatigue within (light blue line) and between days (dark blue line) of two patients with similar iSD of 1.07, but different degrees of clinically meaningful fluctuations across 14 days (panel c, PAC 15%; panel d, PAC 38%). Dark blue dot on bottom represents clinical meaningful fluctuation in fatigue between days.
Next, based on the sample mean PAC, patients were divided into patients with low (n = 26) and high (n = 31) frequency of clinical meaningful fluctuations in fatigue across 14 days. No significant differences were observed between these two groups (Table 2, see Supplementary Table 1 for all baseline characteristics between groups).
Overview of relevant baseline characteristics in patients with low degree of fluctuations and patients with high degree of fluctuations in fatigue.
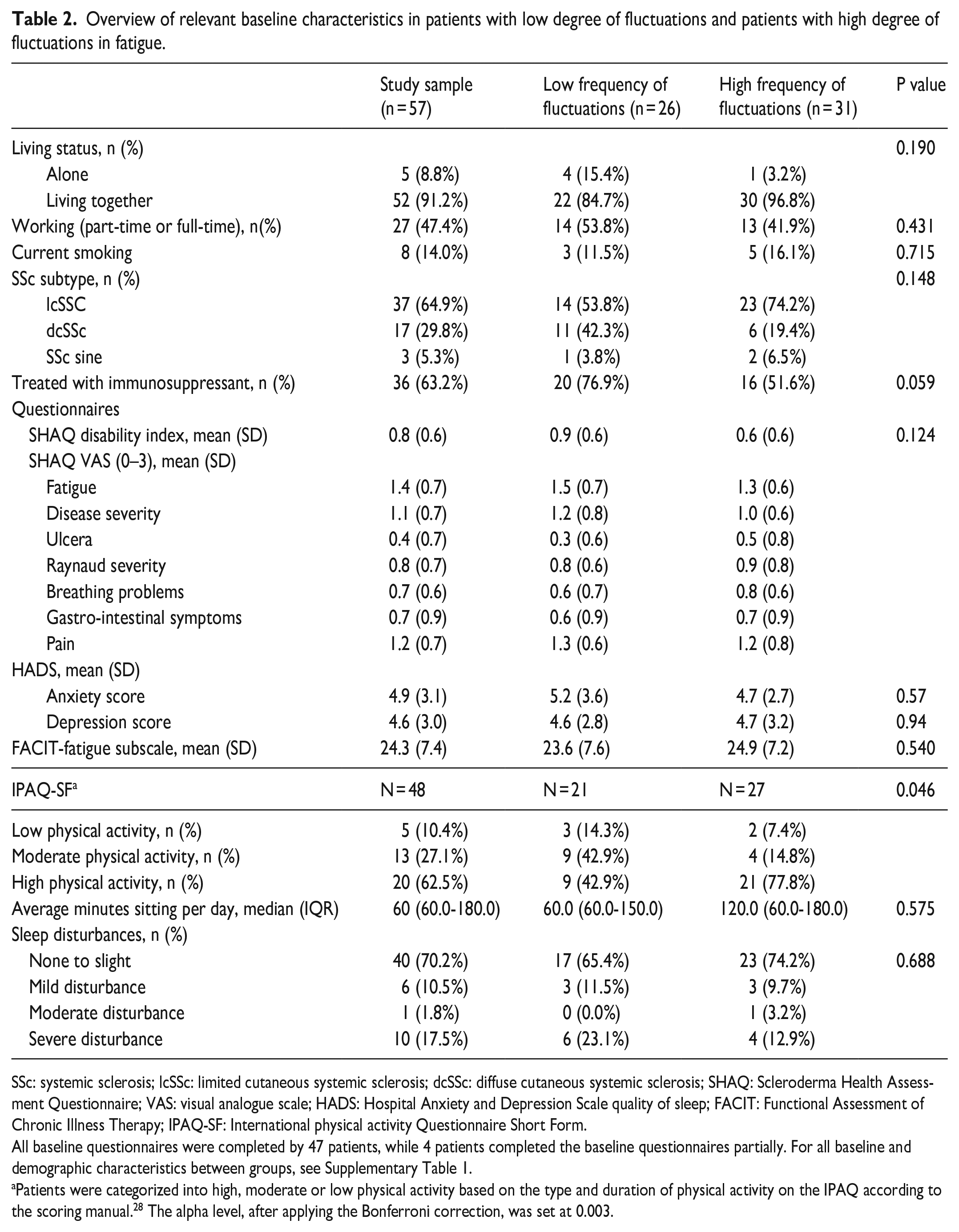
SSc: systemic sclerosis; lcSSc: limited cutaneous systemic sclerosis; dcSSc: diffuse cutaneous systemic sclerosis; SHAQ: Scleroderma Health Assessment Questionnaire; VAS: visual analogue scale; HADS: Hospital Anxiety and Depression Scale quality of sleep; FACIT: Functional Assessment of Chronic Illness Therapy; IPAQ-SF: International physical activity Questionnaire Short Form.
All baseline questionnaires were completed by 47 patients, while 4 patients completed the baseline questionnaires partially. For all baseline and demographic characteristics between groups, see Supplementary Table 1.
Patients were categorized into high, moderate or low physical activity based on the type and duration of physical activity on the IPAQ according to the scoring manual. 28 The alpha level, after applying the Bonferroni correction, was set at 0.003.
Association between within-person fluctuations of fatigue and daily determinants within days and across days
The within-person fluctuations of fatigue were modelled using hybrid mixed models, while controlling for the course over time. The best model for this association included fixed effects for time and quadratic time, random effects for time at both levels, and a random effect for quadratic time at level day. This model yielded an intraclass coefficient at the person level of 0.49 (95% CI: 0.39–0.59), indicating that 51% of fluctuations in fatigue severity were at a within-person level (i.e. within days and across days). Based on the course of fatigue, we concluded that no additional correction for specific weekday was needed (Supplementary Figure 1).
Next, the associations within a person between fatigue severity and negative affect, positive affect, pain, perceived physical exertion, and quality of sleep were modelled using a three-level mixed model (i.e. observation, day, patient). After disaggregating each determinant from the ecological momentary assessment into their corresponding levels, the needed fixed and random effects were added into the model of fatigue and time. With respect to confounders, only BMI was a significant confounder in the models for negative and positive affect (see Supplementary Table 2–6 for final models). The final models showed significant within-person association between fatigue severity and changes in the determinants from the daily diary assessments within a day, across days and across patients (Figure 3). A positive association was observed for negative affect, pain and perceived exertion of physical activity; indicating that an increase in negative affect, pain or perceived exertion of physical activity compared to either (1) the person’s usual state (within a day as well as across days) or to (b) the usual state for study population, was accompanied with more fatigue. The opposite was observed for quality of sleep and positive affect; indicating that a decrease in quality of sleep or positive affect, compared to either (1) the person’s usual state or to (2) the usual state for study population was accompanied with more fatigue.
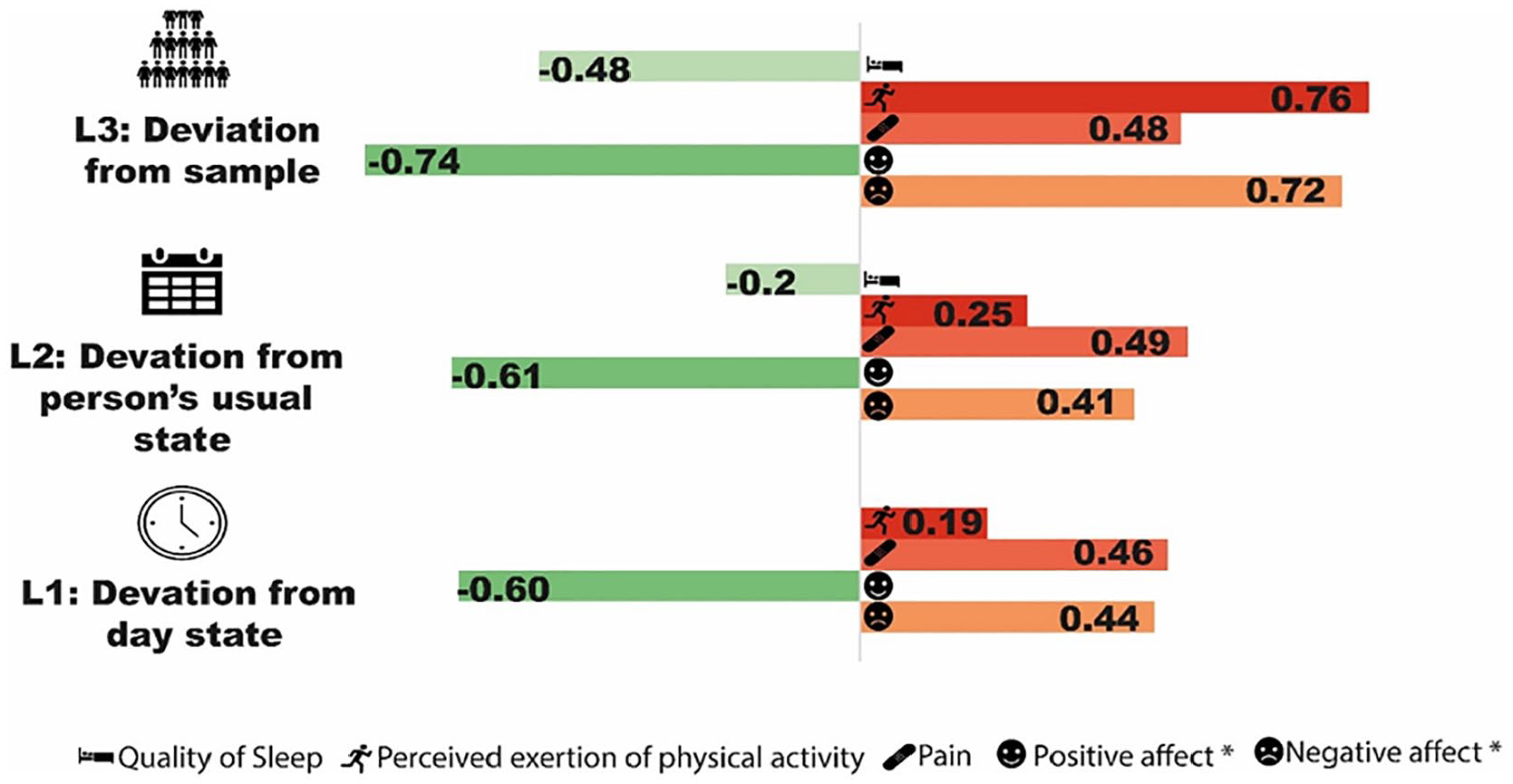
Overview of the association between daily diary assessments and fatigue at each level in the final models. For each determinant a separate multilevel model was constructed. The number in the bar represents the regression coefficient from the final model. All associations are significant (p value < 0.05).
Discussion
This is the first study using ecological momentary assessment that examined and quantified the variability of fatigue within individuals who have SSc. We showed that fatigue fluctuates significantly within persons across a period of 14 days; an individual experienced on average five times a clinical meaningful day-to-day fluctuation in fatigue on a total of 14 consecutive days. Furthermore, we found that increases in within-person levels of negative affect, pain or perceived exertion of physical activity compared to that individual’s usual state were associated with more fatigue, while the opposite was observed for positive affect and quality of sleep. Of note, the observed changes in negative affect, positive affect, pain, perceived exertion of physical activity, and quality of sleep do not provide information about the temporal relationship between these determinants and fatigue (i.e. lagged analyses).
In our study sample, around half of the observed variance in levels of fatigue can be attributed to fluctuations occurring within individuals, transpiring within a single day or spanning across multiple days. Our observation aligns with findings from other studies, as similar within-person variance rates, range between 35% and 50%, have been reported in conditions like rheumatoid arthritis, fibromyalgia and ankylosing spondylitis.34–37 Our findings demonstrated substantial variance among individuals in the magnitude of fatigue fluctuations. Also, we found a wide distribution in the frequency of clinically meaningful fluctuations of fatigue, ranging from individuals without any clinical meaningful fluctuations in fatigue between days to individuals experiencing clinically meaningful fluctuations on a daily basis during our observation period of 14 days. We did not find any distinctive patient-related features that could explain these heterogeneity. In summary, our results not only confirmed the findings of qualitative studies but also highlighted the presence of intra-individual differences in experienced fluctuations of fatigue.7,9,19–21
The associations observed between mood and fatigue at the group level were also identified at the individual level. 3 Similar associations between positive affect, negative affect and fatigue have been described previously at a within-person level in other rheumatic conditions. 38 Notably, we found the most robust association with changes in levels of fatigue at an individual level for positive affect. Our results suggest that incorporating strategies that positively influence mood, such as cognitive re-structuring, mindfulness stress reduction, into treatment may be beneficial. This hypothesis is further supported by a recent study demonstrating that focusing on positive events resulted in reduced disability due to fatigue in patients with inflammatory arthritis. 36 However, no studies have investigated the effect of mood-related interventions on fatigue or fluctuations in fatigue. 39 Further research and interventions targeting mood-related factors could potentially enhance fatigue management in SSc patients.
Our observation that an increase in perceived exertion of physical activity is associated with increased fatigue also deserves comment, as previous studies have reported that physical activity might alleviate fatigue.11,40 In our study, perceived exertion of physical activity was assessed with the Borg scale for perceived exertion of physical activity. 41 Given that this construct assesses the perceived intensity of physical activity experienced by patients, it is reasonable to expect a positive correlation with fatigue. In addition, it was observed that the relationship between perceived exertion of physical activity and fatigue is more pronounced at the group level compared to the within-person level. This finding suggests that patients who engage structurally in physical activities with perceived higher intensity, compared to other SSc patient, experience consistently higher levels of fatigue. On the contrary, transient increments in perceived exertion during physical activity have a minimal impact on experienced levels of fatigue. Given that this study focused on perceived exertion of physical activity, additional research with an objective measurement for physical activity is needed to determine the robustness of our findings.
A major strength of our study is the low missing rate in the daily assessments, allowing us to examine within-person fluctuations within days as well as between days. 42 Furthermore, we had a relatively large sample size for an ecological momentary assessment study. Nevertheless, there are also limitations with our study. 43 We did not include an objective measurement (e.g. activity tracker) for physical activity, which could have yielded more information about type and duration of physical activity that might contribute fatigue. Furthermore, our study sample consisted of individuals with a higher level of fatigue compared to previous studies, which might limit the generalizability of our results to all SSc patients.44–46 Although the sample size was sufficient for the primary outcome, it was too small to conduct multivariable statistical analyses, including positive affect, negative affect, pain and physical activity to analyse the independent associations of each determinant with fatigue. Future studies are needed to confirm our findings and evaluate the predictive value of the determinants on fatigue severity.
In conclusion, this is the first quantitative study showing within-person fluctuations of fatigue in SSc using real-time assessments, confirming the results of qualitative studies.7,9,19–21 The within-person analyses indicate that positive affect had the strongest association with fatigue fluctuations, compared to negative affect, pain, perceived exertion of physical activity and quality of sleep.
Supplemental Material
sj-pdf-1-jso-10.1177_23971983241242836 – Supplemental material for Within-person fluctuations of fatigue in patients with a clinical diagnosis of systemic sclerosis and its relationship with mood, pain, sleep and physical activity
Supplemental material, sj-pdf-1-jso-10.1177_23971983241242836 for Within-person fluctuations of fatigue in patients with a clinical diagnosis of systemic sclerosis and its relationship with mood, pain, sleep and physical activity by Arthiha Velauthapillai, Madelon C Vonk, Cornelia HM van den Ende and Johanna E Vriezekolk in Journal of Scleroderma and Related Disorders
Footnotes
Acknowledgements
The authors thank our patients and patient partners for their participation.
Availability of data and material
The datasets are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: M.C.V. received honorary as speaker from Boehringer Ingelheim, Bristol-Myers Squibb, GSK, Janssen, MSD, Novartis and Roche, as consultant from Boehringer Ingelheim and Janssen, Grant/research and received support from Research grants from Boehringer Ingelheim, Janssen, Ferrer and Galapagos, none on the subject of this study. J.E.V. received honorary as speaker from Eli Lilly, but this is not pertaining to this study. The remaining authors have declared no conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics
The study was conducted in accordance with the Declaration of Helsinki, and the Institutional Review Board of the Radboud University Medical Centre, Nijmegen, determined that the study was not subject to the Dutch Medical Research Involving Human Subjects Act. All participants provided written informed consent.
The statement
The Editor/Editorial Board Member of JSRD is an author of this paper; therefore, the peer-review process was managed by alternative members of the Board and the submitting Editor/Board member had no involvement in the decision-making process.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.