
Abstract
Background and objective:
Patients with systemic sclerosis (SSc) and pulmonary arterial hypertension (PAH) have a poor prognosis, accounting for 30% of all SSc-related deaths. Guidelines recommend annual screening for PAH regardless of symptoms, as early treatment improves outcomes. Current protocols include combinations of clinical features, biomarkers, pulmonary function tests, and echocardiography. None include exercise testing, although early-stage PAH may only be evident during exercise. This systematic review assessed the performance of exercise tests in predicting the presence of PAH in patients with SSc, where PAH was confirmed through right heart catheterisation (RHC).
Methods:
Comprehensive literature searches were performed using MEDLINE, EMBASE, Cochrane Database of Systematic Reviews and Cochrane Central Register of Controlled Trails, CINAHL, Scopus and Web of Science from inception to May 2023. Articles were screened for eligibility by two independent reviewers. Eligibility criteria included the use of a non-invasive exercise test to screen adult patients to detect PAH in a population without a previous diagnosis of PAH, with diagnosis confirmed by RHC.
Results:
Eight studies met the inclusion criteria, describing at least one of three different non-invasive exercise tests: cardiopulmonary exercise test, six-minute walk test and stress Doppler echocardiography. All studies found that exercise tests had some ability to predict the presence of PAH, with sensitivity between 50% and 100% and specificity from 73% to 91%.
Conclusion:
Exercise tests are infrequently used for screening for PAH in SSc but can predict the presence of PAH. More data are required to establish which tests are most effective.
Keywords
Introduction
Systemic sclerosis (scleroderma, SSc) is an autoimmune multisystem connective tissue disease characterised by vasculopathy and fibrosis. SSc causes significant morbidity, poor health-related quality of life and increased mortality, 4 and there is no cure. Pulmonary arterial hypertension (PAH) occurs in up to 12% of SSc patients1,2 and is a common cause of SSc-related death, with 50% 1-year survival if untreated.2–5 Symptoms are nonspecific, leading to delayed diagnosis and poorer outcomes. 6 Early detection of PAH enables institution of PAH-specific therapies while patients are in a better functional class. This can favourably alter disease management, 5 delay clinical deterioration, 4 improve health-related quality of life 6 and improve survival. 7 To confirm the presence of PAH, patients undergo right heart catheterisation (RHC), an invasive procedure with some morbidity and mortality, which should be reserved for patients at high risk of PAH. 8
Annual transthoracic echocardiogram screening for PAH is recommended, 9 but some cases can be missed despite exertional dyspnoea, 10 due to inability to estimate the pulmonary artery systolic pressure (PASP), as the required tricuspid regurgitant jet may be absent in up to 39% of patients. 11
Published screening algorithms for PAH in SSc patients include the DETECT 12 and Australian Scleroderma Interest Group algorithm. 13 These comprise combinations of clinical and serological variables, echocardiography and pulmonary function tests. Although their sensitivity approaches 100%, specificity is low, with relatively high rates of positive screens, potentially leading to RHC. 14 The cost-effectiveness of these composite indices is yet to be confirmed. Because no screening tool distinguishes between PAH and other types of pulmonary hypertension, RHC remains a necessary investigation, but more specific screening may reduce the number required. ‘Exercise tests’ are used once a diagnosis of PAH is established, to assess mortality risk, monitor progression and treatment efficacy. 9 None of the existing algorithms include exercise testing, even though the features of early PAH may only be evident during exercise. This systematic literature review aimed to investigate which exercise modalities have been used to screen for PAH in SSc and to assess how well they predict risk of PAH.
Methods
Search strategy
A librarian-assisted literature search was performed using MEDLINE (via Ovid), EMBASE, Cochrane Database of Systematic Reviews and Cochrane Central Register of Controlled Trials (CENTRAL), CINAHL (Ebsco), Scopus and Web of Science from inception to May 2021. The protocol was registered on PROSPERO (CRD42021245791). The search syntax consisted of three categories of keywords and/or subject headings intersected by the Boolean terms ‘AND’ or ‘OR’: (1) terms related to SSc; (2) terms related to pulmonary hypertension and (3) terms related to exercise test (Supplemental Table 1). All citations were uploaded to Endnote X9 for duplicate removal. Titles and abstracts were reviewed against the eligibility criteria by two independent reviewers (SM and DS) using the online tool Covidence®. The search was rerun in February 2023 to ensure the review was current.
Eligibility criteria
Eligibility criteria included the use of a non-invasive exercise test to screen for PAH in patients with SSc. The research had to be original, in adults without a prior diagnosis of PAH and the diagnosis of PAH confirmed by RHC. Articles had to be written in English, with no restrictions on setting or timeframe. A study was excluded at the title and abstract screening stage only if both reviewers considered it ineligible. Studies considered potentially eligible for inclusion by either reviewer then underwent full-text screening. Discrepancies between reviewers were resolved by discussion or, if required, by a third reviewer (R.A.). Where there were insufficient data, authors were contacted to determine study eligibility.
Data collection
The study data extracted were author, country, exercise test(s) performed, year of publication, study type, sample size, demographics and use of RHC to confirm PAH. Bias was assessed using the Risk of Bias in Non-randomised Studies–of Interventions (ROBINS-I) tool. 15
Results
The original search yielded 1536 results for review, with 739 duplicates. The second search yielded 220 results, with 89 duplicates. A total of 797 titles were screened from the first search, and 131 from the second. Of the 928 titles screened, 183 articles from the first search and 9 articles from the second were read in full text after others were excluded based on title and abstract. Of these, 173 were excluded on full-text review in the first search, and 8 in the second. Eight articles, seven from the original search and one from the update were selected for inclusion (Figure 1).
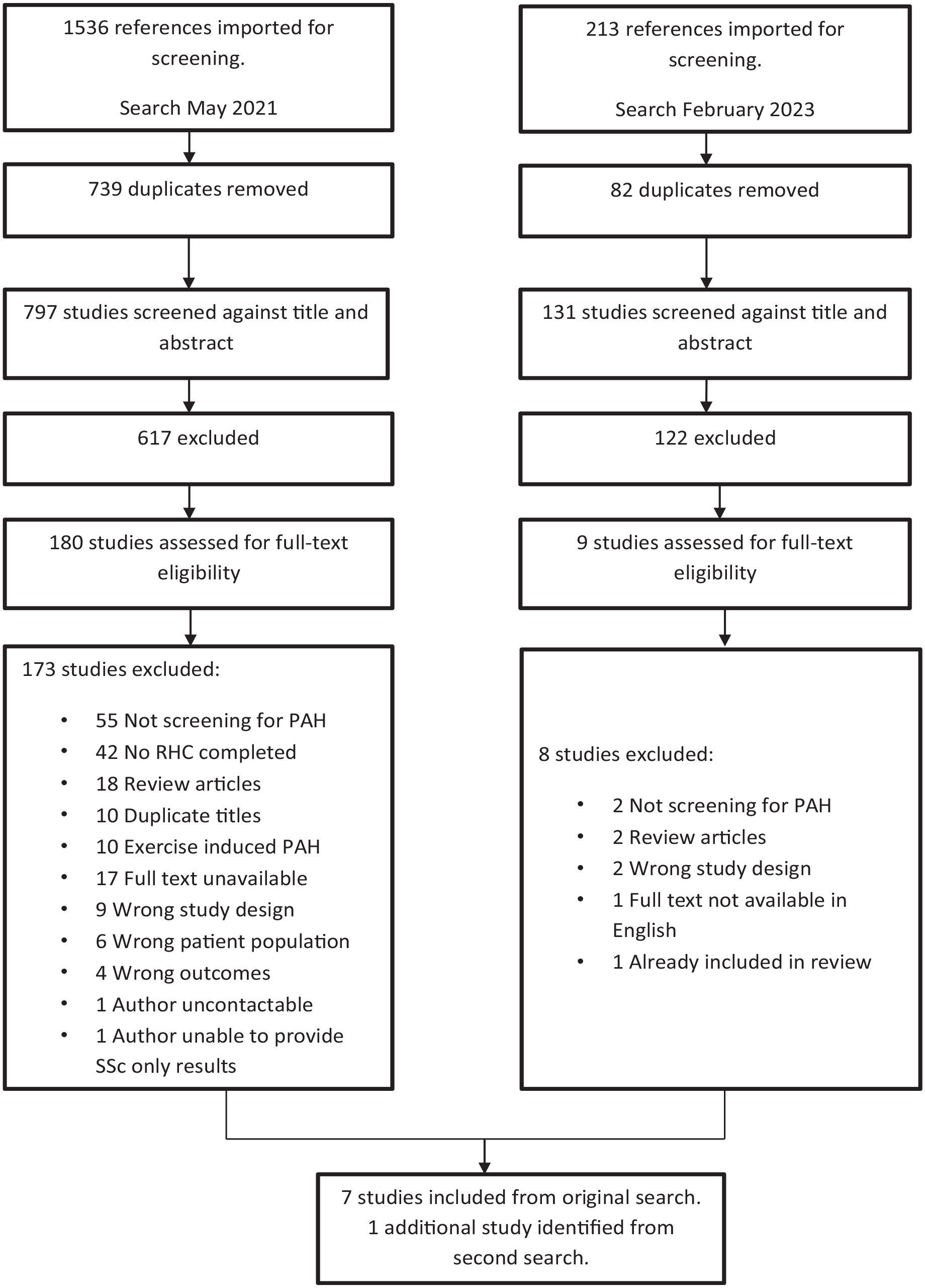
PRISMA flow diagram depicting the process by which articles were screened.
Three types of exercise test were reported: cardiopulmonary exercise test (CPET) (n = 2), six-minute walk test (6MWT) (n = 2), stress Doppler echocardiography (SDE) (n = 3). One reported the use of both the 6MWT and SDE (n = 1) (Supplemental Table 2).
All studies except that of Nagel et al. 16 required patients to have results suggestive of PAH or be symptomatic at the time of enrolment; leading to possible confounding bias. It was not possible to determine with certainty that there was no selection bias in the reported results (Figure 2).
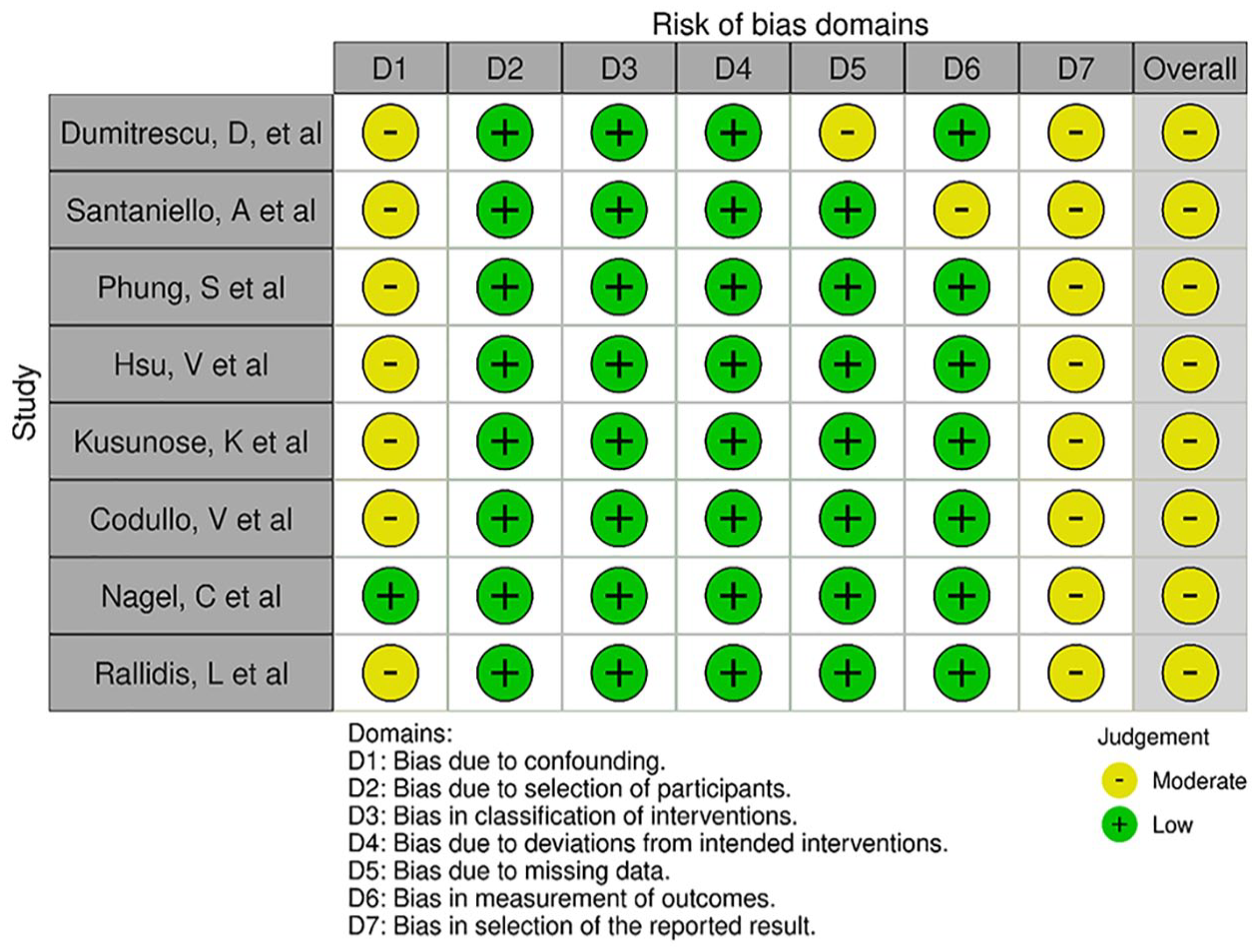
Risk-of-bias assessment.
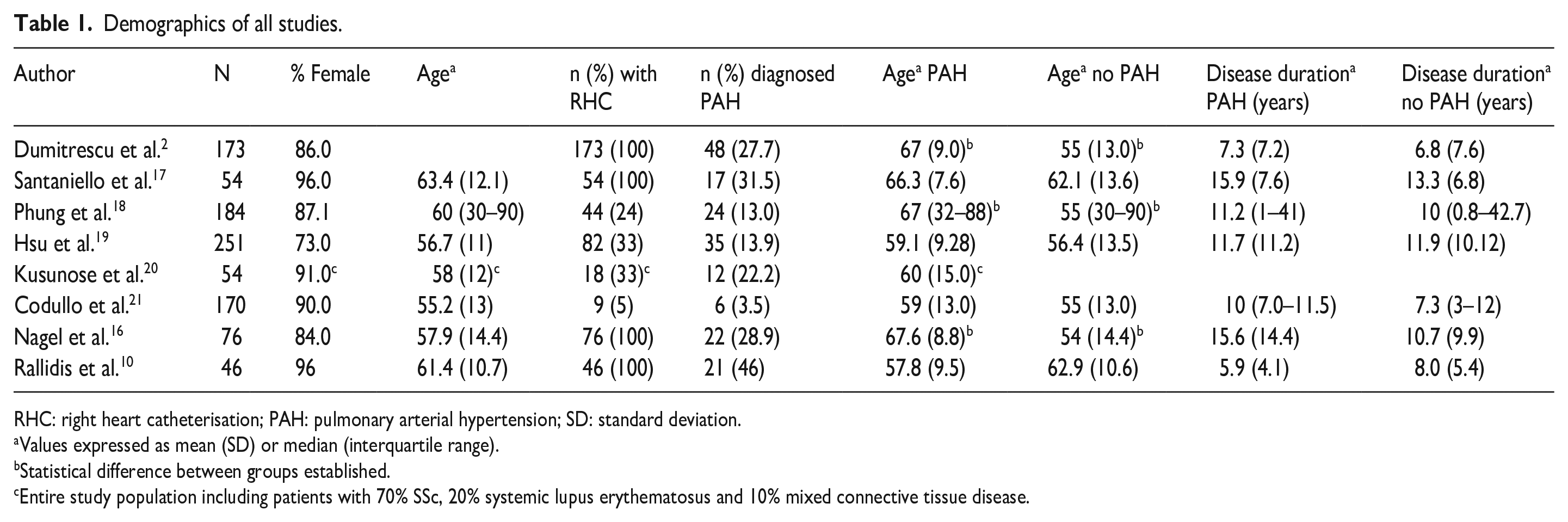
Due to the limited number of studies meeting the inclusion criteria, meta-analysis could not be undertaken; therefore, a narrative review of all studies is presented. Patient demographics are shown in Table 1.
Demographics of all studies.
RHC: right heart catheterisation; PAH: pulmonary arterial hypertension; SD: standard deviation.
Values expressed as mean (SD) or median (interquartile range).
Statistical difference between groups established.
Entire study population including patients with 70% SSc, 20% systemic lupus erythematosus and 10% mixed connective tissue disease.
Studies recruited patients who were being screened for PAH due to symptoms (n = 1), other test results suggesting the presence of PAH (n = 6) or as normal practice to screen all patients regardless of symptoms (n = 1), with study inclusion and exclusion criteria shown in Supplemental Table 3. All patients in all studies had SSc except the study of Kusunose et al. 20 wherein 16 of 78 (20%) patients had systemic lupus erythematosus (SLE) and 9 of 78 (10%) had mixed connective tissue disease (MCTD). The sample size ranged from 46 to 251 participants, with the majority being female in all studies. Participant age and SSc disease duration were similar in patients with and without PAH in all studies. RHC was performed in all patients in three studies, with all other studies requiring a clinical decision of increased risk before referral for RHC. All RHCs were performed after the exercise test was completed. The reported incidence of PAH ranged from 3.5% to 45.6%, with all but one study reporting incidences higher than the 10%–12% reported in an unselected SSc population. 2 All studies were conducted in countries with access to comparable treatment options. No studies reported any adverse events occurring during exercise.
Cardiopulmonary exercise test
Two studies used CPET to predict PAH in patients diagnosed with SSc.2,17 Both recruited patients with clinical features of PAH, such as symptoms or on other non-invasive test results.2,17 All patients underwent RHC regardless of CPET results. CPET was performed on a cycle ergometer using incremental work protocols until patients reached their maximum exercise capacity. Both studies used the v-slope method to determine first ventilatory threshold (fVT) or anerobic threshold (AT). The term AT may infer different ventilatory thresholds depending upon the context. In these studies, fVT is the same as AT and determined using the same methodology.2,17
Dumitrescu et al. 2 evaluated CPET in consecutive patients displaying potential clinical signs of PAH. Receiver operating charateristic curve (ROC) analyses were performed on CPET results to compare gas exchange parameters by area under the curve (AUC) between study patients with and without PAH and reported that the AUCs of peak oxygen uptake (VO2, mls/min/kg), partial pressure of end-tidal carbon dioxide, nadir ventilatory equivalent for CO2 (EQCO2) and fVT (mLVO2/min/kg) were 0.891, 0.851, 0.850 and 0.842, respectively. Based on these analyses, thresholds to optimise both the sensitivity and specificity were determined by using the Youden Index (Table 2). 2
Performance of CPET in predicting PAH confirmed by right heart catheterisation in patients with systemic sclerosis.
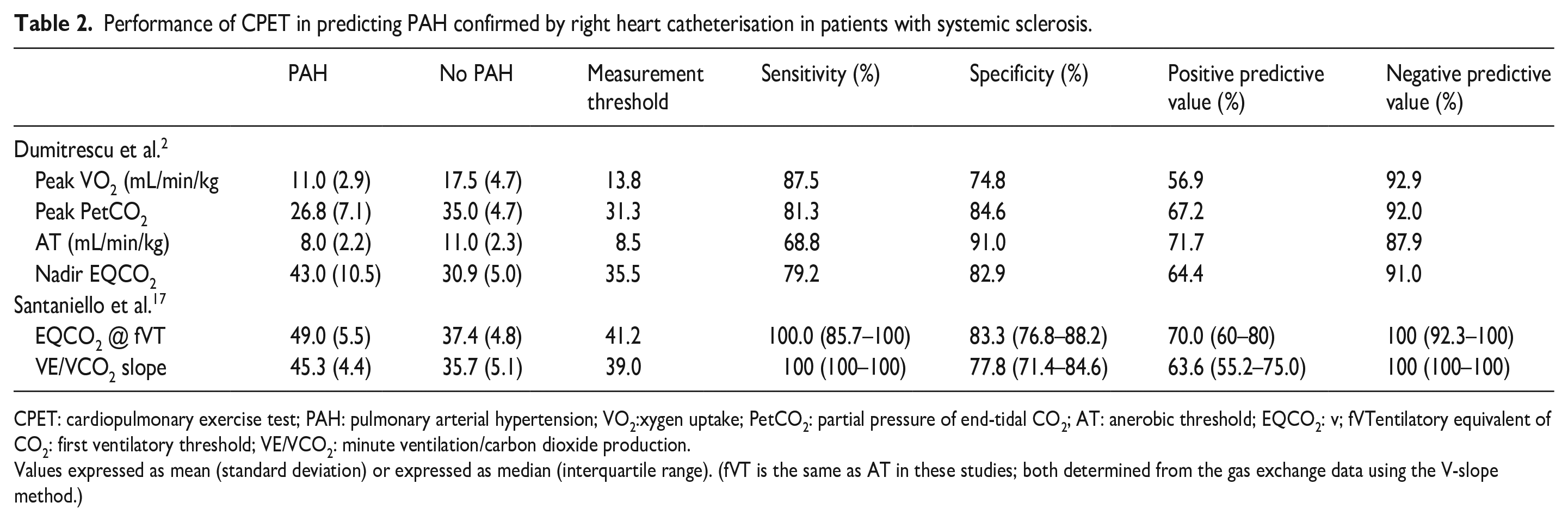
CPET: cardiopulmonary exercise test; PAH: pulmonary arterial hypertension; VO2:xygen uptake; PetCO2: partial pressure of end-tidal CO2; AT: anerobic threshold; EQCO2: v; fVTentilatory equivalent of CO2: first ventilatory threshold; VE/VCO2: minute ventilation/carbon dioxide production.
Values expressed as mean (standard deviation) or expressed as median (interquartile range). (fVT is the same as AT in these studies; both determined from the gas exchange data using the V-slope method.)
Santaniello et al. 17 evaluated CPET in SSc patients screening positive for PAH according to the DETECT algorithm. 14 The statistical method of bootstrap aggregating (bagging) was used to find statistically significant CPET parameters which identified patients with PAH. 17 EQCO2 at fVT with a bootstrapped threshold of 41.2 and minute ventilation/carbon dioxide production (VE/VCO2) slope of 39 were highly sensitive with specificities similar to those of the CPET parameters used by Dumitrescu et al. 2 (Table 2). None of the other CPET parameters investigated improved the performance of the DETECT algorithm.
Both studies found that EQCO2 predicted PAH, with Dumitrescu et al. 2 finding a sensitivity of 79.2% and a specificity of 82.9%, while Santaniello et al. 17 found a sensitivity of 100% and specificity of 83.3%. Dumitrescu et al. 2 found that 99% of patients with PAH had an EQCO2 nadir of >45.5 with the lowest false-positive rate (91%, positive predictive value 100%). Santaniello et al. 17 found both EQCO2 and VE/VCO2 slope could detect PAH with 100% sensitivity, but VE/VCO2 slope when used in conjunction with the DETECT screening algorithm led to a theoretical reduction in the number of RHCs required to identify PAH from 54 (100% of population) to 25 (46% of population), without missing any diagnosis of PAH.
Dumitrescu et al. 2 found that peak VO2 was the best discriminator between patients with and without PAH with the highest sensitivity (87.5%) and specificity (74.8%) and that a peak VO2 > 18.7 mL/min/kg excluded PAH in all cases. Santaniello et al. 17 assessed but could not confirm the role of peak VO2 in screening for PAH. They hypothesised this could be due to different enrolment strategies as Dumitrescu et al. 2 enrolled consecutive patients with clinical signs of possible PAH, while Santaniello et al. 17 used a PAH screening algorithm prior to enrolment, so patients in the Santaniello study were more likely to test positive for PAH.
Six-minute walk test
Three studies reported using 6MWT to screen SSc patients for PAH. However, none of the studies based the decision to refer for RHC on the 6MWT result.18–20 All studies based referral for RHC on either echocardiograph results or increased dyspnoea. There were methodological differences or lack of standardisation that may have influenced the assessment of 6MW distance in these studies. Two studies provided information on track length18,20 which varied between 20 and 50 metres, while only Phung et al. 18 used a standardised script as per American Thoracic Society /European Respiratory Society test guidelines. 22
All studies reported a shorter walk distance in patients with PAH than in patients without, with the results of Phung et al. 18 (345 m vs 445 m) and Hsu et al. 19 (352.89 m vs 422.15 m) reaching statistical significance (Table 3). In addition, Hsu et al. 19 found more patients diagnosed with PAH experienced exercise-induced desaturation to <92% when compared with those without PAH (p < 0.038). Decreasing walk distance combined with exercise desaturation were important risk factors for PAH that should be considered when assessing risk of PAH. 19 Hsu et al. 19 also found that the first walk test exercise-induced desaturation (O2 saturation < 92%) was an independent predictor of PAH development with a hazard ratio of 5.233.
Performance of 6MWT in predicting PAH confirmed by right heart catheterisation in patients with systemic sclerosis.
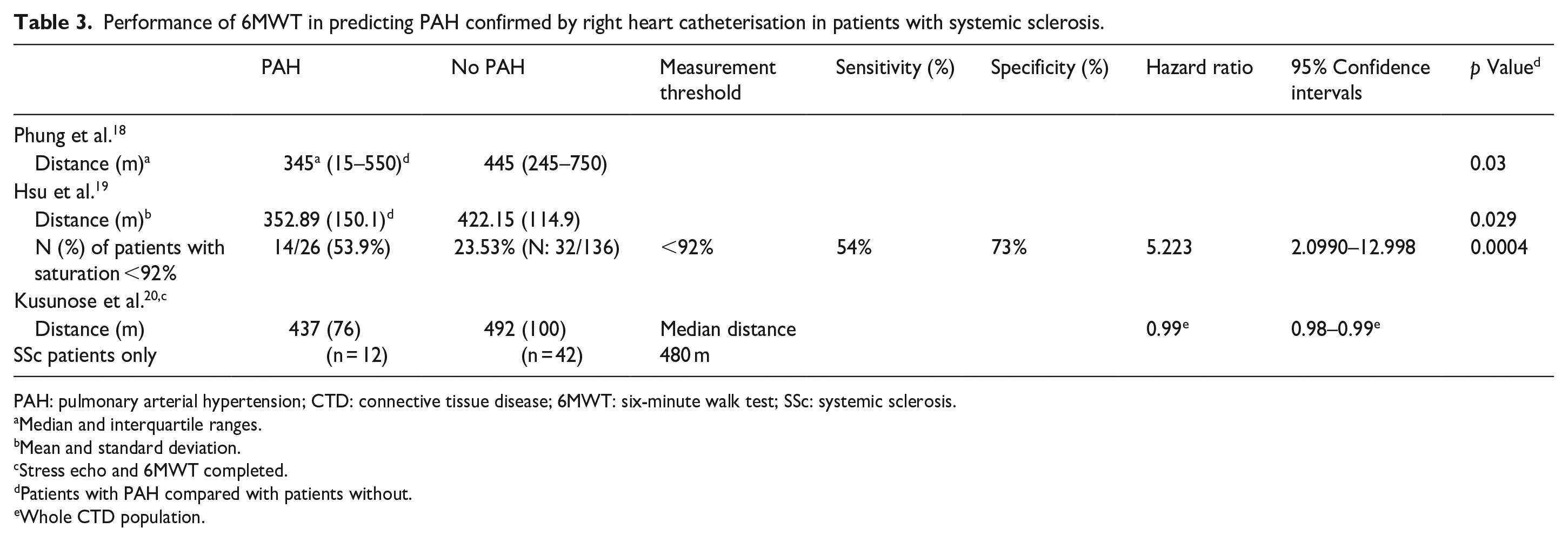
PAH: pulmonary arterial hypertension; CTD: connective tissue disease; 6MWT: six-minute walk test; SSc: systemic sclerosis.
Median and interquartile ranges.
Mean and standard deviation.
Stress echo and 6MWT completed.
Patients with PAH compared with patients without.
Whole CTD population.
Stress Doppler echocardiography
Four studies used SDE to screen for PAH in patients with SSc.10,16,20,21 Kusunose et al. 20 referred patients for RHC where there was an increase in mean pulmonary arterial pressure (PAP) on resting echocardiogram between annual visits with new or increased symptoms. Nagel et al. 16 and Rallidis et al. 10 performed RHC in all patients, and Codullo et al. 21 did so when resting electrocardiogram findings were suggestive of PAH or if PASP was ⩾40 mmHg on follow-up, diffusing capacity of lung for carbon monoxide was <55% and forced vital capacity was >70% of predicted values. Codullo et al. 21 and Nagel et al. 16 used similar testing protocols where cycle ergometer workload was increased by 25 Watts every 2 minutes until either a symptom-limited maximum (Nagel et al.) or 85% of the age-predicted maximum heart rate (Codullo et al. 21 ) was achieved. Kusunose et al. 20 completed echocardiography measurements after a 6MWT. Rallidis et al. 10 used the Bruce protocol on a treadmill with SDE undertaken within 1 minute of maximum exercise achieved. SDE results are summarised in Table 4.
Performance of stress Doppler echocardiography in predicting PAH confirmed by right heart catheterisation in patients with systemic sclerosis.
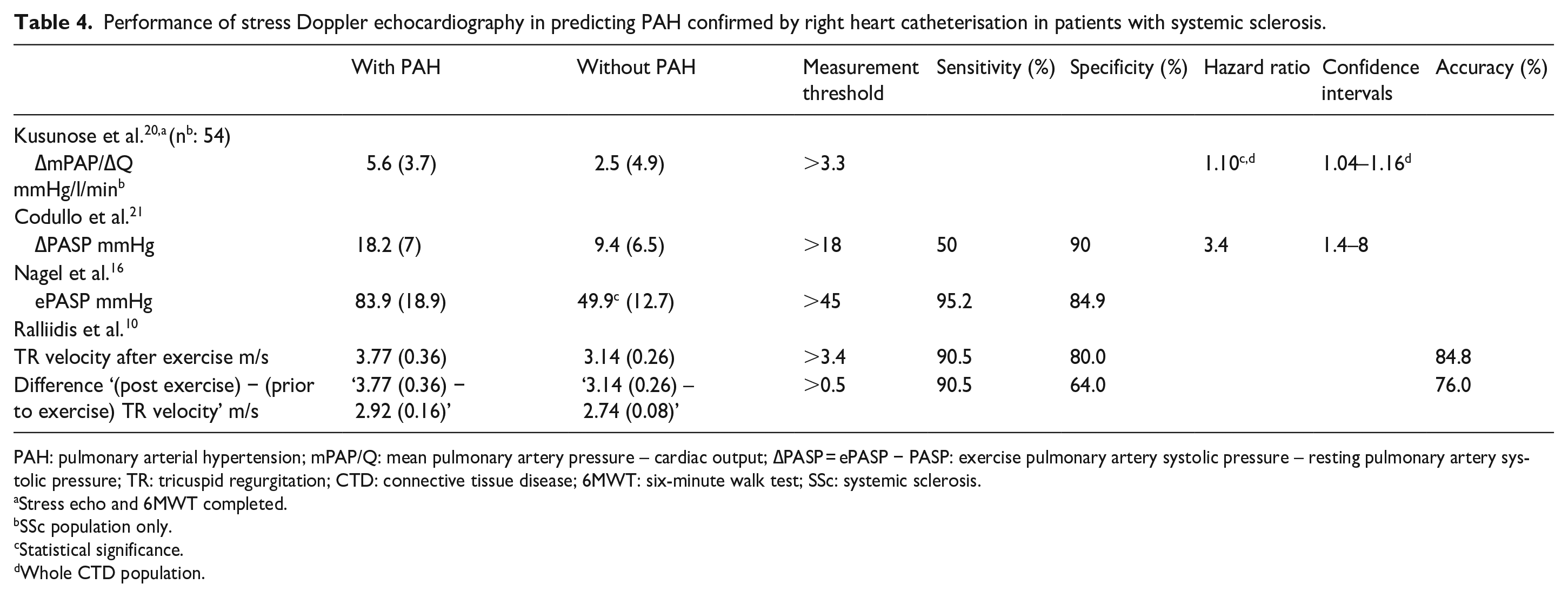
PAH: pulmonary arterial hypertension; mPAP/Q: mean pulmonary artery pressure – cardiac output; ∆PASP = ePASP − PASP: exercise pulmonary artery systolic pressure – resting pulmonary artery systolic pressure; TR: tricuspid regurgitation; CTD: connective tissue disease; 6MWT: six-minute walk test; SSc: systemic sclerosis.
Stress echo and 6MWT completed.
SSc population only.
Statistical significance.
Whole CTD population.
All studies found that SDE increased detection of PAH when compared to echocardiography performed at rest. Nagel et al. 16 found that the detection of PAH was 72.7% on resting echocardiography, increasing to 95.2% with SDE, using a PASP of 40 mmHg at rest and 45 mmHg during low exercise. Kusunose et al. 20 found that ∆mean pulmonary artery pressure/cardiac output (∆mPAP/∆Q) was a good predictor of PAH in the combined study population of patients with SSc, SLE and MCTD. Analysis of SSc patients only was not conducted. Codullo et al. 21 found that patients who had a PASP of ⩾48 mmHg with exercise more frequently developed PAH than those who did not (14% vs 2% of patients). Using ROC analysis, Codullo et al. 21 demonstrated that an increase in PASP by >18 mmHg during exercise was highly specific (90%) for PAH in this cohort but with low sensitivity (50%). Rallidis et al. 10 found that tricuspid regurgitation (TR) velocity >3.4 m/s after exercise had the greatest sensitivity and specificity for PAH with an accuracy of 76%. They also found that a difference of >0.5 m/s in TR velocity between exercise and rest had a sensitivity of 90.5%, specificity of 64% and accuracy of detecting PAH of 76%. 10
Kusunose et al. 20 performed SDE after the patient completed the 6MWT and found that PAH patients who had reduced walk distance and increased ∆mPAP/∆Q after the walk had significantly shorter event-free survival than those without impaired 6MWD or increased ∆mPAP/∆Q.
Discussion
This review demonstrates that exercise tests can contribute to the detection of PAH with high sensitivity but variable specificity. CPET and SDE show promise with EQCO2 nadir of >45.5 (CPET) and increased mPAP – cardiac output (>3.3) or PASP ⩾40 mmHg (SDE), demonstrating high sensitivity and specificity using defined cutoff values derived by ROC analysis. While 6MWD is reduced and exercise desaturation is increased in PAH patients, cutoff values with sensitivity and specificity for predicting PAH have not been defined.
Both studies using CPET2,17 found that EQCO2 was an important variable in detecting PAH. Although the EQCO2 nadir and EQCO2fVT numerical values should be very similar, there are small differences due to the different methodologies used to derive them. Dumitrescu et al. 2 showed that the EQCO2 correlated best with haemodynamic parameters, with higher sensitivity and specificity when analysing the nadir EQCO2 achieved as opposed to the value achieved at fVT. Santaniello et al. 17 were unable to confirm the role of peak VO2 in screening for PAH as found by Dumitrescu et al. 2 This could be due to the different study design and populations since Santaniello’s subjects were pre-screened using the DETECT algorithm. Both studies reported similar prevalence of PAH.
Studies using 6MWT reported that patients diagnosed with PAH had shorter walk distances. No study included 6MWD in the criteria for referral for RHC. Hsu et al. 19 found that exercise-induced desaturation was an independent predictor of PAH and was an important risk factor for identifying patients who should undergo RHC. Patients with desaturation <92% were five times more likely to develop PAH,10,13 indicating that desaturation on 6MWT could identify patients at risk of developing PAH. Rate of detection of PAH using 6MWT may be underestimated as none of the studies undertook RHC in all participants.
All studies reporting the use of SDE found different variables associated with PAH, ranging from mPAP-cardiac output, TR velocity, to exercise PASP – resting PASP, especially when the assessment was standardised. Nagel et al. 16 found that SDE improved the sensitivity from 72.7% on resting echocardiogram to 95.2% on exercise, with a specificity of 84.9%. The lower specificity was thought to be due to a concomitant cardiovascular disease. Nagel et al. 16 also found that SDE detected patients with only mild Pulmoary Hypertension/PAH-SSc at an early stage, which may have been overlooked by resting echocardiography. Rallidis et al. 10 also found that SDE was able to detect changes of PAH in patients with inconclusive resting echocardiographic studies by using TR velocity after exercise, with a high level of both sensitivity (90.5%) and specificity (80%).
Most studies reported a higher prevalence of PAH in patients with SSc (6%–46%) than that reported in the literature. 2 This was likely due to selection bias, as all but one study recruited patients in whom there was suspicion of PAH. As a result, these studies probably overestimate the detection rate for each modality compared with that in an unselected SSc population.
The design of the literature search and the review of the literature were comprehensive but had some limitations: The number of studies that met the eligibility criteria were small, preventing meta-analysis of results. Furthermore, the studies were heterogeneous in design and inherently had some limitations. All study populations other than that studied by Nagel et al. 16 were heavily screened prior to recruitment, and therefore, results may not represent results in an unselected clinical SSc population. In addition, studies had small sample sizes with relatively low numbers of events, limiting generalisability of results. Interpretation of all exercise tests is confounded by the difficulty in differentiating between abnormal results due to PAH or from other comorbidities such as left-heart disease. 17 The methodology of the 6MWT studies was poorly standardised, whereby different track lengths and lack of standardised scripts were employed, potentially affecting walk distance achieved. 22 Echocardiographic imaging after exercise is operator-dependent and needs to be performed promptly by experts. Hence, standardised testing procedures for SDE are essential to ensure optimal performance in predicting PAH. In addition, only one of the four studies completed RHC in all patients, so potential cases of PAH may have been missed in those studies. Rallidis et al. 10 used the new 2022 PAH guidelines for detecting PAH, dropping the mPAP to >20 mmHg and pulmonary vascular resistance (PVR) to >2 Wood units, 23 resulting in 21 (45.6%) patients being diagnosed with PAH compared with 10 (21.7%) using the previous cutoff values used in other studies. This may have skewed assessment of the test’s ability to predict PAH.
This review determined that CPET, 6MWT and SDE can all improve detection of PAH when screening SSc patients. Although a meta-analysis could not be undertaken, CPET was shown to improve the performance of the DETECT algorithm for screening SSc patients and reduced the number of RHC this patient population would have to undergo. It demonstrates the need to increase knowledge in the appropriate use of exercise tests for screening and early detection of PAH and to identify which parameters will improve sensitivity and specificity in an SSc population.
Supplemental Material
sj-pdf-1-jso-10.1177_23971983231199148 – Supplemental material for Use of exercise tests in screening for pulmonary arterial hypertension in systemic sclerosis: A systematic literature review
Supplemental material, sj-pdf-1-jso-10.1177_23971983231199148 for Use of exercise tests in screening for pulmonary arterial hypertension in systemic sclerosis: A systematic literature review by Sarah Madigan, Susanna Proudman, David Schembri, Huw Davies and Robert Adams in Journal of Scleroderma and Related Disorders
Footnotes
Acknowledgements
We acknowledge Nikki May from the SA Health Library Service for her assistance is designing and running the search strategies used in review.
Authors note
The Editor/Editorial Board Member of JSRD is an author of this article; therefore, the peer review process was managed by alternative members of the Board, and the submitting Editor/Board member had no involvement in the decision-making process.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.