
Abstract
Patients with systemic sclerosis are at high risk of developing systemic sclerosis–associated interstitial lung disease. Symptoms and outcomes of systemic sclerosis–associated interstitial lung disease range from subclinical lung involvement to respiratory failure and death. Early and accurate diagnosis of systemic sclerosis–associated interstitial lung disease is therefore important to enable appropriate intervention. The most sensitive and specific way to diagnose systemic sclerosis–associated interstitial lung disease is by high-resolution computed tomography, and experts recommend that high-resolution computed tomography should be performed in all patients with systemic sclerosis at the time of initial diagnosis. In addition to being an important screening and diagnostic tool, high-resolution computed tomography can be used to evaluate disease extent in systemic sclerosis–associated interstitial lung disease and may be helpful in assessing prognosis in some patients. Currently, there is no consensus with regards to frequency and scanning intervals in patients at risk of interstitial lung disease development and/or progression. However, expert guidance does suggest that frequency of screening using high-resolution computed tomography should be guided by risk of developing interstitial lung disease. Most experienced clinicians would not repeat high-resolution computed tomography more than once a year or every other year for the first few years unless symptoms arose. Several computed tomography techniques have been developed in recent years that are suitable for regular monitoring, including low-radiation protocols, which, together with other technologies, such as lung ultrasound and magnetic resonance imaging, may further assist in the evaluation and monitoring of patients with systemic sclerosis–associated interstitial lung disease. A video abstract to accompany this article is available at: https://www.globalmedcomms.com/respiratory/Khanna/HRCTinSScILD
Keywords
Introduction
Among patients with systemic sclerosis (SSc), there is a high risk of developing interstitial lung disease (ILD), which when present is associated with respiratory impairment, reduced quality of life and increased risk of death. 1 Early and accurate diagnosis of systemic sclerosis–associated interstitial lung disease (SSc-ILD) facilitates clinical management, and the most sensitive and specific diagnostic modality is high-resolution computed tomography (HRCT) of the chest.2–4 The utility of HRCT in SSc-ILD is not limited to screening and diagnosis, as it is also useful in disease monitoring5–8 and determining prognosis. 9 However, HRCT may be underused in patients with SSc-ILD. 10
This review will highlight the importance of early diagnosis in SSc-ILD, focusing on the use of HRCT of the chest as a screening, diagnostic, prognostic, and monitoring tool, as well as the evolution of chest imaging techniques.
SSc-ILD
SSc is a heterogeneous autoimmune connective tissue disease characterized by skin thickening and progressive fibrosis of the skin and internal organs. 11 Patients with SSc are at high risk of developing ILD, which causes significant morbidity and mortality: symptoms and outcomes range from subclinical lung involvement to major pulmonary disease, respiratory failure, and death. 12 Pulmonary fibrosis resulting from ILD is one of the leading causes of mortality in patients with SSc, responsible for up to 17% of SSc-related deaths. 13
Many patients with SSc-ILD experience clinically significant progression, and clinical outcome is worse in patients with more extensive disease. 14 While some patients may remain stable indefinitely, others decline and then become stable, whereas others will progress inexorably with a variety of trajectories. For example, in the European Scleroderma Trials and Research Group database, almost one-third of patients had stable lung function during 5 years of follow-up; 15 however, among those with initial progression at 1 year, almost half showed further progression over 5 years. 16
Potential risk factors for any ILD in patients with SSc and for progression of ILD in SSc-ILD are shown in Table 1. However, it should be noted that some of these risk factors are yet to be confirmed or come from single-center cohorts. Risk factors for progression may also depend on the phase of the disease.
Potential risk factors for ILD and progression of ILD in SSc.
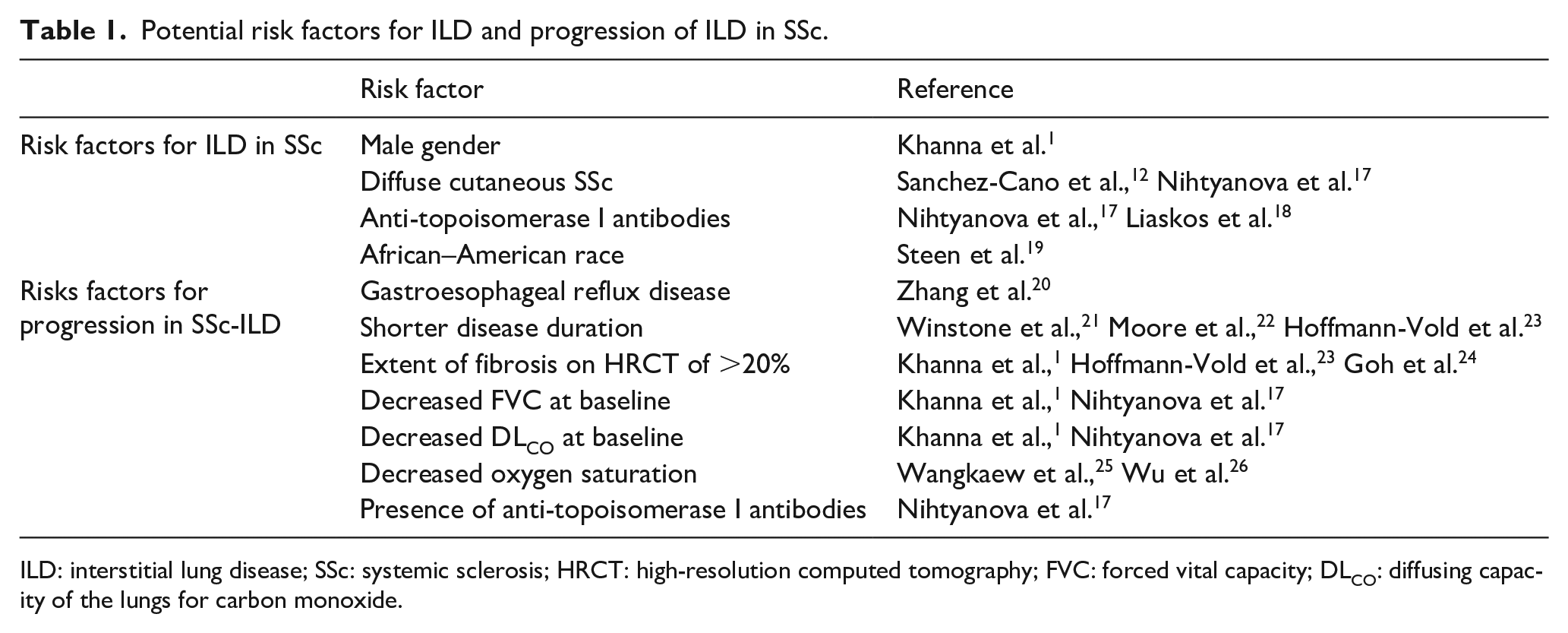
ILD: interstitial lung disease; SSc: systemic sclerosis; HRCT: high-resolution computed tomography; FVC: forced vital capacity; DLCO: diffusing capacity of the lungs for carbon monoxide.
As the risk of developing ILD is greatest in the first few years after SSc diagnosis,27,28 screening patients with SSc for ILD may help with prognosis and management. Patients with clinically significant disease at baseline and those at high risk for clinically significant progression should be identified as early as possible. 4 As the disease course is variable 23 and difficult to predict, it is appropriate to monitor patients with SSc-ILD regularly for signs of progression. 29
Emphysema is independently associated with SSc, and like SSc-ILD, is best seen on HRCT. Combined pulmonary fibrosis and emphysema (CPFE) is also present in approximately 7%–18% of patients with SSc-ILD.30,31 Patients with CPFE-SSc have worse survival than with SSc-ILD and SSc-emphysema,30,31 and early diagnosis by HRCT is important for disease management.
For this review, the PubMed database was searched for all publications up to 1 July 2019 (date of the search) using the following search terms: (high-resolution computed tomography and systemic sclerosis) and (diagnosis or treatment); high-resolution computed tomography and (safety or interstitial lung disease). Publications relating to idiopathic pulmonary fibrosis or ILD not including SSc were excluded. Publications were additionally included based on the expert knowledge of the authors.
HRCT in SSc-ILD
Screening and diagnosis
Early detection of ILD in patients with SSc is important for baseline evaluation and for consideration of treatment interventions. Expert consensus recommendations endorse screening all patients using HRCT and lung function testing2–4 (Table 2).
Expert consensus regarding use of HRCT and PFTs in patients with SSc-ILD.
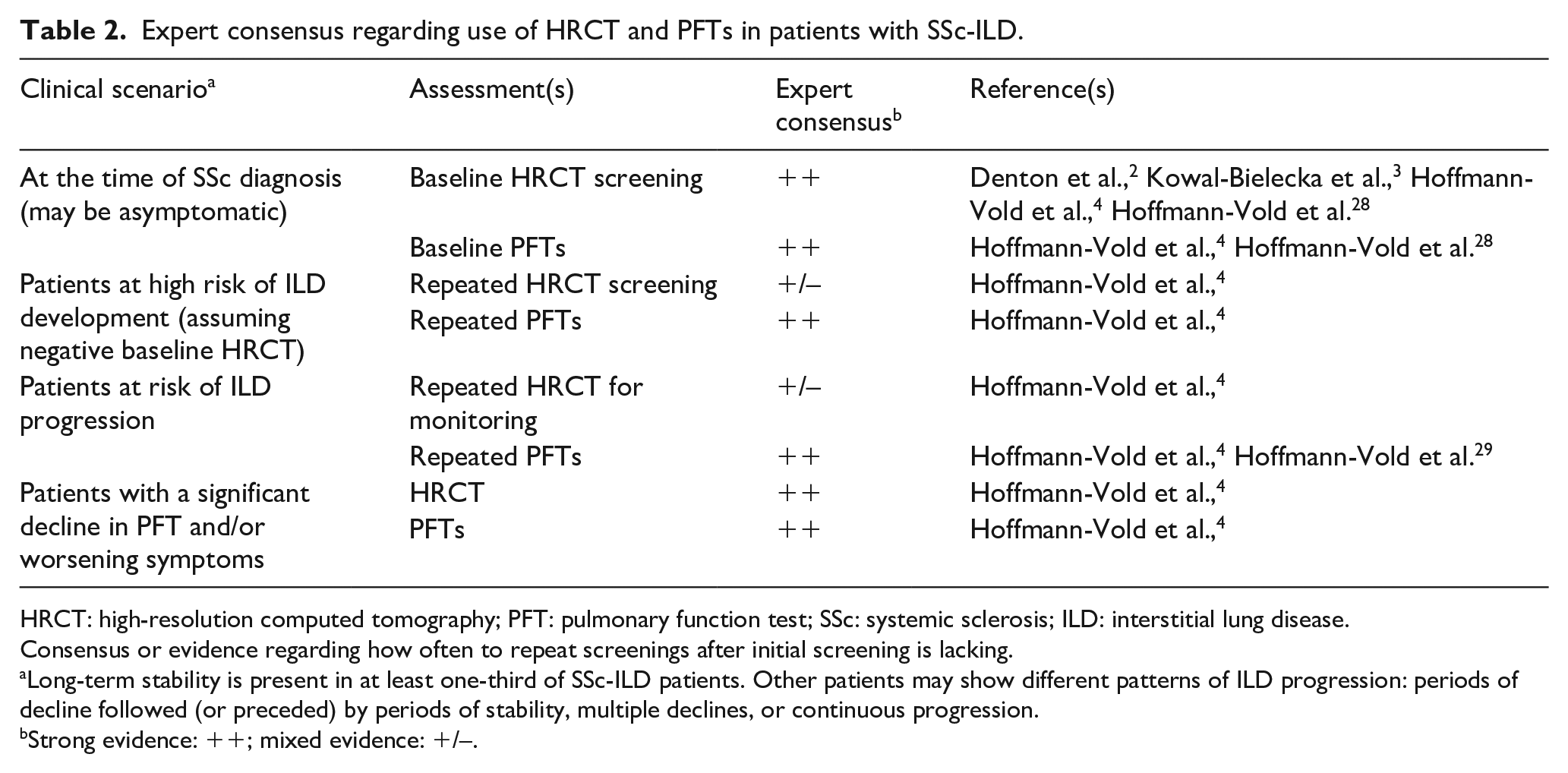
HRCT: high-resolution computed tomography; PFT: pulmonary function test; SSc: systemic sclerosis; ILD: interstitial lung disease.
Consensus or evidence regarding how often to repeat screenings after initial screening is lacking.
Long-term stability is present in at least one-third of SSc-ILD patients. Other patients may show different patterns of ILD progression: periods of decline followed (or preceded) by periods of stability, multiple declines, or continuous progression.
Strong evidence: ++; mixed evidence: +/–.
HRCT of the chest is the most sensitive means of detecting SSc-ILD 32 and is regarded as the gold standard for diagnosis. 4 On initial HRCT, ILD is present in more than 50% of patients, 28 including in some patients without symptoms. 33 Signs of interstitial lung abnormalities and ILD (including ground-glass opacity, septal lines, and honeycombing in the patterns of non-specific interstitial pneumonia and usual interstitial pneumonia (UIP)) can be seen even when pulmonary function test (PFT) results are in the normal range. 34 While PFTs alone may be insufficient for early diagnosis,23,28,33,34 PFTs should be performed at the time of SSc diagnosis and at regular follow-up intervals.4,29
Despite expert recommendations, HRCT is currently underused in the screening and diagnosis of SSc-ILD. In a recent study, only 51% of general rheumatologists and 66% of SSc experts reported routinely ordering HRCT in all newly diagnosed patients with SSc. 10 In addition to clinician specialty, factors affecting HRCT use may include clinician experience, lack of knowledge of guidelines, lack of routine progression of ILD, concerns about radiation exposure, as well as imaging cost and accessibility. 4
More research is needed before recommendations can be made about the benefits of routine follow-up HRCT imaging in asymptomatic patients who have a normal HRCT at baseline. Expert consensus suggests that frequency of screening using HRCT should be guided by risk of developing ILD (such as autoantibodies, cutaneous involvement, race, etc.), in combination with clinical symptoms and lung function. 4 However, there is currently no consensus regarding HRCT screening intervals. 4 Most experienced clinicians would not repeat HRCT more than once a year or every other year for the first few years unless symptoms arose. Likewise, the specifics of HRCT image acquisition (volumetric, inspiratory/expiratory images, and prone images) vary by institution. In all cases, the patient’s radiation exposure should be weighed against the anticipated benefits of the exam.
Prognosis and monitoring
HRCT may be helpful in assessing prognosis in some patients. HRCT data have been included in staging models to gauge ILD progression risk and predict prognosis. 24 Further study is needed in this area, particularly with regards to whether HRCT findings can be used to predict response to treatment.21,35–39
The extent of ILD involvement on HRCT has been shown to correlate with degree of functional impairment (New York Heart Association class) and lung function 40 in patients with SSc-ILD. More extensive ILD on HRCT has been associated with a lower forced vital capacity (FVC) at initial assessment, 41 a greater decline in FVC during follow-up, 42 and early mortality. 23 In a retrospective study of HRCTs from patients in the Australian Scleroderma Cohort Study, extensive disease involving more than 20% of the lung parenchyma on HRCT at baseline was associated with a three-fold increased risk of deterioration or death compared with limited disease, although this study did not account for time from first non-Raynaud symptom and could suffer from lead-time bias. 14 The presence of fibrosis at baseline on HRCT was associated with mortality in multivariable modeling in patients with SSc-ILD in Norway. 28 Although HRCT parameters were not shown to be predictive of survival in patients in one study of early SSc, 26 a number of other published studies support the use of HRCT in determining the prognosis of patients with SSc-ILD.21,24,43,44
Changes in extent or pattern on HRCT might be used to monitor disease progression in treated or untreated patients.8,25,29,45–47 Due to the heterogeneous longitudinal behavior, the risks of radiation exposure and imaging costs, there is currently no consensus on how often HRCT needs to be repeated (Table 2). The use of HRCT for monitoring disease progression is therefore guided by the clinician 4 and is generally performed in response to worsening of symptoms, as this can be multifactorial in SSc (ILD, pulmonary hypertension, pulmonary embolism, emphysema, deconditioning, anemia, cardiac involvement, etc.). Clinicians may also order a follow-up HRCT scan when there are conflicting data between symptoms and PFTs, or suspicion of pulmonary embolism.
In summary, quantifying the degree of ILD on HRCT is potentially useful to evaluate prognosis and disease progression in SSc-ILD.
Performing HRCT
History
HRCT was first introduced in the 1980s,48,49 when it transformed the diagnosis of diffuse lung disease, particularly fibrosing lung diseases, by providing detailed cross-sectional images of the lungs. Since that time, there have been tremendous developments in computed tomography (CT) technology that are relevant to the diagnosis and monitoring of SSc-ILD. Modern scanners use multidetector helical CT techniques to undertake volumetric scans of the entire thorax that can be reconstructed into thin (less than 1.25 mm) slices, enabling detection of the pattern and extent of subtle abnormalities. Scanner speed enables volumetric whole lung imaging at different states, each in a single breath-hold, such as inspiration and expiration. In addition, radiation dose-reduction techniques, such as automatic exposure control methods and tube current modulation, allow the radiation dose to be adapted to the size of the patient, and more efficient detector systems allow for lower radiation dose exposures to be performed while preserving image quality. Recently, advanced image reconstruction techniques, such as iterative reconstruction, allow even lower radiation dose techniques to be used while still preserving image quality. 50 Thus, the clinician can now choose to use reduced-dose CT protocols for follow-up scans. These approaches are discussed in more detail below.
Practical recommendations
Detailed practical recommendations for performing HRCT scans and interpreting the results for patients with predicted SSc-ILD have recently been described. 32 Volumetric acquisition with thin slices using a supine inspiratory scan acquisition is recommended to allow reconstruction in the coronal and sagittal planes with sufficient image fidelity; reconstructions should be performed with less than 1.25-mm thick slices. Supine expiratory scans allow better detection of air trapping; if dependent density is observed, then a prone inspiratory scan should be conducted to allow differential diagnosis of early ILD from atelectasis. Moderate edge-enhancing reconstruction algorithms should be employed, as areas of pseudo-honeycombing may result from an algorithm that is too sharp. Specific breathing instructions should be provided to patients to ensure repeatability between scans. Scans should be reviewed immediately following acquisition. 32 Whole-lung contiguous acquisition allows the application of advanced processing techniques, including whole-lung segmentation, volume measurements, and quantification of normal and abnormal lung tissue.
Minimum (MinIP) and maximum intensity projection (MaxIP) are post-processing techniques that convert the voxel with the lowest or highest density, respectively, on every view throughout the volume into a two-dimensional image. 51 MinIP allows for improved detection of air trapping, can obviate the need for an expiratory scan, and is useful in the identification and quantification of ground-glass opacities. MaxIP can help improve the detection of nodules and micronodules associated with comorbidities.
Minimizing radiation exposure in HRCT and the associated trade-offs
CT scans use ionizing radiation, which does carry some risks. These risks are stochastic in nature at the levels of radiation exposure associated with CT scans for SSc-ILD, and are primarily related to radiation-induced carcinogenesis. These are considered to be small, though non-zero, risks. The risks of ionizing radiation are higher in women and decrease with age. 52 Therefore, balancing the radiation exposure to the patient, while maintaining sufficient image quality to obtain the desired diagnostic information, should always be considered. As mentioned above, there have been tremendous advances in CT scanner hardware and software that have allowed the generation of high-quality images of the entire lungs in a single breath-hold while requiring lower levels of radiation exposure. Measures to reduce HRCT-associated radiation exposure include the use of more efficient detector systems, automatic exposure control (such as tube current modulation), and advanced image reconstruction methods, such as iterative reconstruction techniques. In addition, further radiation dose reductions can be achieved by using limited axial scans (rather than helical scans), in which thin slices are acquired with large intervals (such as a 1-mm width acquisition spaced every 10 or 20 mm). While this reduces the radiation dose to the patient, it also substantially limits the amount of anatomy that is available for determining presence or severity of SSc-ILD.
Figure 1 shows HRCT images of a patient with SSc-ILD reconstructed with simulated dose reduction, keeping all other acquisition parameters the same. Some increased noise with loss of discrimination between the different manifestations of SSc-ILD can be seen.
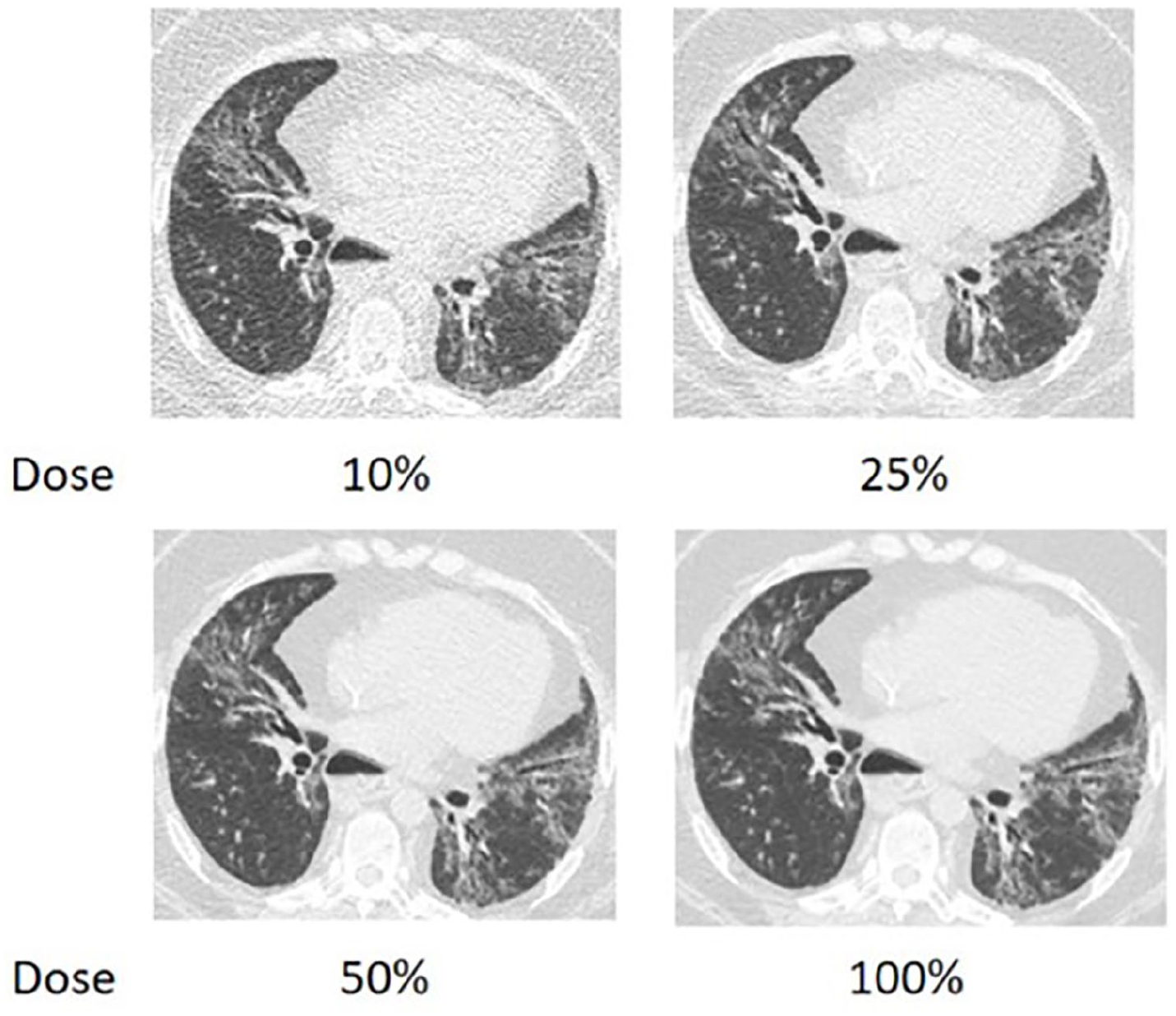
HRCT images comparing conventional versus reduced dose protocol in a patient with diffuse SSc-ILD. Axial thin section CT slice through the lower lobes of the lungs in a 35-year-old female patient with SSc with images reconstructed at simulated 10%, 25%, and 50% of acquired dose (100%). At all doses, the classic features of SSc-ILD can be identified; an NSIP pattern with peribronchovascular ground-glass and reticular opacities plus architectural distortion consistent with fibrosis. With decreasing dose, there is increased image noise resulting in loss of clarity of the different abnormalities due to loss of clarity of the ground-glass opacities as distinct from the reticular abnormalities.
Iterative reconstruction techniques can allow the use of reduced radiation dose without compromising diagnostic accuracy (despite a possible loss of spatial resolution and differences in noise texture).53–55 A study of HRCT images from 55 patients with SSc-ILD found little difference between images generated using scans performed with a conventional (filtered back projection) reconstruction algorithm at 120 kV and 110 effective mAs (corresponding to a volume CT dose index (CTDIvol) of approximately 7.2 mGy) and those generated using 40% of that scanner output (120 kV, 44 effective mAs, corresponding to a CTDIvol of approximately 2.9 mGy), using an iterative reconstruction algorithm. Patients received either an estimated mean effective dose of 3.67 (range: 2.01–5.83) mSv when the full dose was used, or 1.8 (1.01–4.35) mSv with the dose reduction. 54 However, an increase in image noise may be problematic for detecting subtle changes in SSc-ILD, for scanning larger patients at lower doses, and for applying computer-aided diagnosis and machine-learning techniques to CT data sets. Therefore, although promising, these findings should be replicated in other institutions using scanners from other manufacturers.
Several other studies have shown even greater dose reductions when applying iterative reconstruction methods without substantial loss of image quality, although their assessments of image quality were not always specific to SSc-ILD and included subjective assessments. Some simple quantitative assessments have been performed, and measures that primarily involve assessment of Hounsfield units (HU; for example, mean HU or mean HU in a region) are usually well preserved at very low doses. 55 More complicated measures used in quantitative assessments (such as texture and others described below) have not been shown to be robust at these levels of dose reduction, and this is an area of further investigation.
CT scan protocols that do not use volumetric acquisition, but rather use a limited set of axial scans with large intervals between scans (for example, 1 mm scans every 10 or 20 mm), have also been used successfully to detect ILD in patients with SSc.56–58 This approach offers further radiation dose reduction, as a limited sample of lung anatomy is scanned instead of the entire lung, although these non-volumetric techniques may have limited assessment of regional variations or heterogeneity. By maintaining HRCT accuracy and sensitivity, these protocols enable detection of mild SSc-ILD while substantially reducing the estimated effective radiation dose.
Through automatic exposure control techniques and other technology developments, modern scanners use lower doses of radiation to achieve high-quality scans. The estimated effective dose of a standard HRCT scan is 2–4 mSv (Table 3). 56 This is slightly higher than the estimated effective dose of a low-dose lung cancer screening CT exam (1–2 mSv)59,60 or chest X-ray (0.02–0.1 mSv) 61 but is lower than the estimated effective dose of a routine diagnostic thoracic CT exam (estimated 5–7 mSv). The estimated effective dose from a standard HRCT scan is thus similar to the estimated naturally occurring background annual radiation in the United States (3.1 mSv) 62 and the annual exposure for airline crew operating on long-haul flights (2–3 mSv). 63 The estimated effective doses from HRCT scans can also be compared to the annual allowed exposure for radiation workers (including radiologists, radiologic technologists, and medical physicists) of 50 mSv per year. 64 The International Commission on Radiological Protection has also recommended an annual average of not more than 20 mSv per year over a 5-year period for occupational exposure. 65
Effective radiation dose for environmental exposure and different chest imaging protocols a .
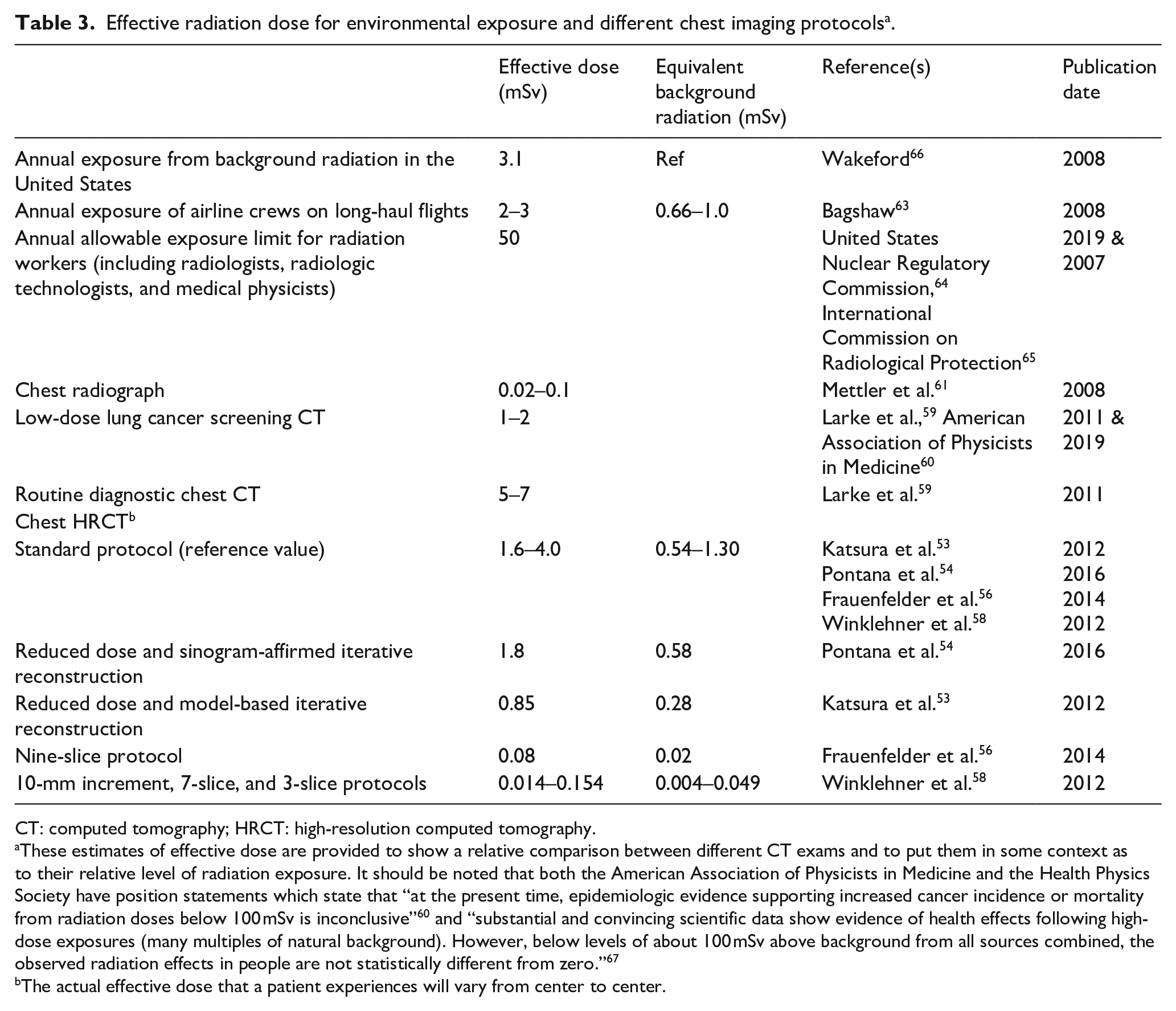
CT: computed tomography; HRCT: high-resolution computed tomography.
These estimates of effective dose are provided to show a relative comparison between different CT exams and to put them in some context as to their relative level of radiation exposure. It should be noted that both the American Association of Physicists in Medicine and the Health Physics Society have position statements which state that “at the present time, epidemiologic evidence supporting increased cancer incidence or mortality from radiation doses below 100 mSv is inconclusive” 60 and “substantial and convincing scientific data show evidence of health effects following high-dose exposures (many multiples of natural background). However, below levels of about 100 mSv above background from all sources combined, the observed radiation effects in people are not statistically different from zero.” 67
The actual effective dose that a patient experiences will vary from center to center.
Computer-based quantification of fibrosis in patients with SSc-ILD
Computer-aided diagnosis algorithms for classifying HRCT patterns in diffuse lung disease for SSc-ILD were first reported in 2010. 68 This algorithm was developed using a machine-learnt texture feature classification to detect and quantitate the amount of ground glass (QGG), lung fibrosis (QLF), and honeycomb cysts in patients with SSc-ILD. QGG and QLF have been used in several settings to determine the measurement variation and cut points for meaningful change. 47 The extent of QLF is a predictor of decline in FVC over a 1-year period and is independent of the staging system used to classify extent of disease. 42 Other algorithms, including the automated lung parenchymal characterization by computer-aided lung informatics for pathology evaluation and rating (CALIPER), were also developed using a computer-vision-based technique that includes volumetric local histogram and morphologic analysis to provide quantitative assessment of pulmonary parenchymal disease on HRCT data. 69 These algorithms can objectively quantify specific patterns of ILD changes during treatment in patients with SSc-ILD.45,47 Results have been found to be equivalent to or better than those of a radiologist,9,70,71 although these algorithms are patented and not widely available.
More recently, artificial intelligence and deep learning have been applied to the classification of fibrotic lung disease on HRCT, using criteria specified by two international diagnostic guideline statements. The algorithm developed therein was able to differentiate between UIP, possible UIP and patterns inconsistent with UIP with 73.3% accuracy, and the authors note that this could be applicable in centers lacking in radiologic expertise. 72
Emerging imaging techniques
Lung ultrasound
Lung ultrasound is sensitive for the detection of lung disease but not as specific as HRCT.73–75 Lung ultrasound abnormalities correlate with increases in the score and digital vascular damage when assessing progression of ILD. 76 B-lines on lung ultrasound show mild-to-moderate correlation with fibrosis on HRCT 77 and detection of multiple B-lines, pleural irregularity, and pleural line thickening on lung ultrasound is highly predictive of the presence of significant SSc-ILD on HRCT.78,79 However, there is not yet a consensus on whether lung ultrasound can be used routinely to screen for ILD in SSc.
Other imaging techniques
Magnetic resonance imaging (MRI) techniques show promise in the detection of pulmonary fibrosis.80,81 While HRCT has superior image quality, MRI may be useful to detect inflammatory changes and is free of any radiation exposure. As a molecular imaging modality, positron emission tomography (PET)-CT is being studied as a potential monitoring tool. 18 F-fluorodeoxyglucose (FDG) is a commonly used PET radiotracer in oncology. In lung fibrosis, FDG uptake has been observed in macrophages, neutrophils, and eosinophils and may detect cellular inflammation through the glycolysis of immune cells, as an indirect means to monitor fibrosis. 82 Single-photon emission CT (SPECT) has potential utility in the early detection of ILD, by using radiolabeled, target-specific probes to visualize inflammatory stages of ILD. Preclinical studies in animal models and resections from human lungs have shown that SPECT could potentially identify ILD before significant tissue remodeling has occurred.83,84 These promising tools need further evaluation in the screening and management of SSc-ILD.
Conclusion
HRCT is currently the gold standard for early detection and accurate diagnosis of ILD in patients with SSc and should be performed in all patients at the time of initial SSc diagnosis. Patients most at risk of developing ILD are those with a recent diagnosis of SSc, diffuse cutaneous SSc, smoking history or male gender, and these should be considered when determining whether a patient would benefit from regular screening. HRCT can also be used for prognosis and to monitor for disease progression in addition to serial lung function tests and other measures. Currently, follow-up HRCT is guided by symptoms and suspicion of progression, and more research is needed on the optimal frequency in patients at different levels of ILD risk.
As HRCT scan techniques are constantly evolving, low-radiation protocols that are suitable for the regular screening and monitoring of patients are now available. The introduction of other technologies, such as lung ultrasound or MRI, with or without HRCT, is a potential future direction that may further assist in the evaluation of patients with SSc-ILD.
Footnotes
Acknowledgements
Medical writing, editorial support, and formatting assistance for this manuscript was provided by Rebecca Sutch, PhD, of AMICULUM and Helen Keyworth, PhD, of Nucleus Global under the authors’ conceptual direction and based on feedback from the authors, and was contracted and funded by Boehringer Ingelheim International GmbH (B.I.). B.I. was given the opportunity to review the manuscript for medical and scientific accuracy as well as intellectual property considerations.
Author contributions
The authors meet criteria for authorship as recommended by the International Committee of Medical Journal Editors (ICMJE). The authors did not receive payment related to the development of the manuscript. All authors reviewed and revised the manuscript critically for important intellectual content; and approved the final version of the manuscript. The authors take full responsibility for the scope, direction, content of, and editorial decisions relating to the manuscript, were involved at all stages of development, and have approved the submitted manuscript.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: D.K. reports consultancies with Acceleron, Actelion, Bayer, BMS, Boehringer Ingelheim, Corbus, Galapagos, Genentech/Roche, GSK, Mitsubishi Tanabi, Sanofi-Aventis/Genzyme; and stock ownership or options with Eicos Sciences, Inc. O.D. has/had a consultancy relationship with and/or has received research funding from: Abbvie, Acceleron Pharma, Amgen, AnaMar, Bayer, Boehringer Ingelheim, Catenion, Drug Development International Ltd, CSL Behring, ChemomAb, GSK, Horizon (Curzion) Pharmaceuticals, Inventiva, Italfarmaco, IQVIA, Lilly, Medac, Medscape, Mitsubishi Tanabe Pharma, MSD, Novartis, Pfizer, Roche, Sanofi, Serodapharm, Target Bio Science and UCB in the area of potential treatments of scleroderma and its complications. In addition, O.D. has a patent issued for mir-29 for the treatment of systemic sclerosis (US8247389, EP2331143). V.C. reports personal fees and non-financial support from Actelion; grants, personal fees and non-financial support from Boehringer Ingelheim and Roche; and personal fees from Bayer, MSD, Novartis, Sanofi, Promedior, Celgene, Galapagos and Galecto outside the submitted work. K.K.B. reports personal fees from Bayer, MSD, Novartis, Sanofi, Promedior, Celgene, Galapagos, Galecto, Genoa, Lifemax, MedImmune, OSIC (Open Source Imaging Consortium), Pliant, ProMetic, Third Pole, Theravance, Three Lakes Partners, Veracyte; personal fees and non-financial support from Actelion and Boehringer Ingelheim; grants from NIH; consultancies with Biogen and Blade; and grants, personal fees and non-financial support from Roche outside the submitted work. L.C. has served on scientific advisory boards for Boehringer Ingelheim and Mitsubishi Tanabe; serves on a steering committee for Eicos and a data monitoring safety board for Reata; and receives grant funding from Boehringer Ingelheim and United Therapeutics. J.G.G. is the founder of MedQIA, LLC. E.L.M. has a consultancy relationship and/or has received research funding from Boehringer Ingelheim and Gilead. E.K. has no potential conflicts of interest to disclose. S.L.F.W. reports personal fees from Sanofi-Aventis, Roche, Galapagos, OSIC (Open Source Imaging Consortium) and Bracco; grants and personal fees from Boehringer Ingelheim; and grants from National Institute for Health and Research, outside the submitted work. M.M-.G. is a member of a scientific advisory board for Hura Imaging, Inc.; received research funding from Siemens Healthineers and UCLA Radiological Sciences and has a Master Research Agreement with Siemens Healthineers. T.M.M. received research funding and/or consulting fees or other remuneration from AstraZeneca, Bayer, Boehringer Ingelheim, Biogen, Cipla, GSK, Prometic, Roche, Samumed and UCB; and has stock options or bond holdings in the for-profit corporation Apellis.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Medical writing support was contracted and funded by Boehringer Ingelheim International GmbH.