
Abstract
Background:
Therapeutic plasma exchange has been tried as a treatment approach for systemic sclerosis since 1978 based on the rationale that some circulating factor is involved in disease pathogenesis, for example, autoantibodies or immune complexes, and that removing the potential pathogenic factors could lead to symptom improvement. Based on our impression that clinicians and researchers are largely unaware that a large volume of research has been published about the use of therapeutic plasma exchange as a treatment for systemic sclerosis, we conducted a comprehensive review and analysis of all published research on this topic.
Results:
We identified 46 relevant articles that met our search criteria, involving a total of 572 patients. Of these, 19 were case studies; the rest ranged from small observational studies to prospective randomized clinical trials. In all but two studies, most patients receiving therapeutic plasma exchange showed improvements in both clinical symptoms and laboratory markers, including significant improvement in Raynaud’s symptoms and healing of digital ulceration after three to four weekly treatments. The beneficial effects from even a short course of therapeutic plasma exchange treatments were long-lasting, typically 6 months or longer. Therapeutic plasma exchange was very well tolerated. Adverse events were rare and, in almost all cases, mild and transitory.
Conclusion:
These results suggest that long-term therapeutic plasma exchange may offer a low-risk way to control and in some cases reverse systemic sclerosis symptoms. The mechanism for the clinical improvements seen from therapeutic plasma exchange in systemic sclerosis patients is unclear. Therefore, additional studies of therapeutic plasma exchange effects in systemic sclerosis appear to be highly desirable.
Keywords
Introduction
Systemic sclerosis (SSc) is an umbrella term for a family of rare autoimmune diseases with the common factor being abnormal skin fibrosis and thickening in association with Raynaud’s. While the degree of skin fibrosis varies depending on the specific disease variant, all forms of SSc include dysregulation of the immune system and extensive microvascular injury leading to fibrotic damage to internal organ systems, including the lungs, gastrointestinal (GI) system, kidneys, and heart.
There are two recognized subsets of SSc: diffuse cutaneous systemic sclerosis (dcSSc) and limited cutaneous systemic sclerosis (lcSSc). Patients with dcSSc generally have rapid onset of symptoms and significantly reduced survival, mostly due to lung, heart, and kidney involvement. In contrast, patients with lcSSc typically have a much slower progression rate with near normal lifespans but with increasing disability and disfigurement over time.
Conventional treatment approaches
Management of SSc is usually done through a combination of systemic and symptom-specific interventions. Standard systemic treatments focus on immunoregulation (hydroxychloroquine or intravenous immunoglobulin (IVIG)) or immunosuppression (methotrexate, mycophenolate mofetil, cyclophosphamide, and rituximab). Raynaud’s phenomenon (RP) and digital ulcers (DUs) are almost universal in SSc and are treated with a variety of approaches, including vasodilators (calcium channel blockers, phosphodiesterase type 5 (PDE5) inhibitors, and prostaglandins), vasoconstrictor antagonists (endothelin-1 and angiotensin II receptor antagonists), or, in more severe cases, surgical or chemical sympathectomy. GI symptoms, such as gastroesophageal reflux disease (GERD), gastroparesis, malabsorption, and small intestinal bacterial overgrowth (SIBO), are managed through a variety of mostly pharmaceutical treatments although surgical interventions are sometimes employed in severe cases. Scleroderma renal crisis (SRC) is generally treated with ACE inhibitors. To date, no medications have proven to be very effective in treating either pulmonary arterial hypertension (PAH) or interstitial lung disease (ILD), and as a result, lung-related complications from both PAH and pulmonary fibrosis (PF) are the leading causes of SSc-related mortality. 1 According to a recent study, 2 it is not clear that any standard treatment for SSc has led to improved SSc survival rates over the past 40 years, beyond what would be expected by overall improvements in survival rates in the general population during this same time period.
Therapeutic plasma exchange
Therapeutic plasma exchange (TPE), also called therapeutic apheresis, is a procedure in which a large volume of plasma (typically 1–1.5 blood volumes) is replaced by a substitute fluid (most commonly 4%–5% sterilized albumin) in a continuous flow process. Cellular components (RBC, WBC, and platelets) are separated from the plasma by either centrifugal separation or filtration, combined with the replacement fluid and returned in a process that typically takes 1.5–2 h. In the United States, almost all TPE is done using centrifugal separation. A related procedure—plasmapheresis—removes a smaller amount of plasma (typically less than 15% of blood volume) that is inadequate to cause significant hypovolemia, so no replacement fluid is required. Unfortunately, the terms “therapeutic plasma exchange” and “plasmapheresis” are often used interchangeably in the published literature, creating potential confusion when researching the effects of TPE.
The usual rationale and the primary post hoc explanation for any benefits seen from TPE is that TPE treatments temporarily reduce the levels of circulating factor(s) (e.g. autoantibodies or immune complexes, cytokines, or adhesion molecules) that are presumed to be involved in SSc disease pathogenesis. A single TPE treatment of 1–1.5 blood volumes removes approximately 65% of any potential circulating pathogenic factors. 3 It is important to note that certain plasma components are also present in the extravascular space, so post-TPE plasma concentrations may be different than expected due to tissue–plasma equilibration. 4
TPE has been tried as a possible treatment for SSc since 1978. While TPE is rarely used as a treatment modality for SSc in the United States, it is more commonly used in Europe and is a mainline, government-approved treatment option in Italy. 5 Medicare and some US healthcare companies cover TPE as an available treatment option for SSc patients who are unresponsive to conventional therapy. 6 The American Society for Apheresis (ASFA) currently classifies TPE for treating SSc treatment as a Category III treatment: “Optimum role of apheresis therapy is not established. Decision making should be individualized.” 7 Our impression is that clinicians and researchers who work with SSc patients are largely unaware that a large volume of research has been published about the use of TPE as a treatment for SSc.
Method
A minimal Boolean search phrase was constructed that encompasses all common current and historical terms for both SSc and TPE:
(plasmapheresis OR “plasma exchange” OR apheresis OR “plasma filtration”) AND (“systemic sclerosis” OR SSc OR scleroderma OR Raynaud’s OR PSS OR CREST OR (“mixed connective tissue” AND (disorder OR disease) or MCTD)
Mixed connective tissue disorder (MCTD) was included for completeness since it features symptoms of SSc along with symptoms of systemic lupus erythematosus (SLE) and polymyositis.
Initial searching (using the above search phrase) was done using Google Scholar during November and December 2015 in preparation for an abstract that was presented as a poster at the ASFA meeting in May 2016. 8 For all articles that met our inclusion criteria (original research, English abstract), we reviewed all of the references and included any additional articles that had been missed in the original search. An updated search that also included PubMed/MEDLINE, Scopus, and the Cochrane Library was conducted in September and October 2017.
Articles selected for inclusion in this review were categorized as follows:
Case reports (CR);
Single-group pre-post studies with no control group (PP);
Observational studies (OS);
Controlled trials (CT; quasi-experimental studies);
Randomized controlled trials (RCT).
Each article was independently graded by authors E.S.H. and M.M. using standard checklists for the appropriate article category, as is shown in Table 1. Any differences in grading were resolved by discussion. We also reviewed each article to determine whether any observed treatment effects could reasonably be attributed to TPE alone. A number of studies listed additional simultaneous interventions along with TPE, making it impossible to determine whether any observed effects were from TPE, alternative treatments, or synergistic effects from multiple simultaneous treatments.
Grading checklists and criteria.
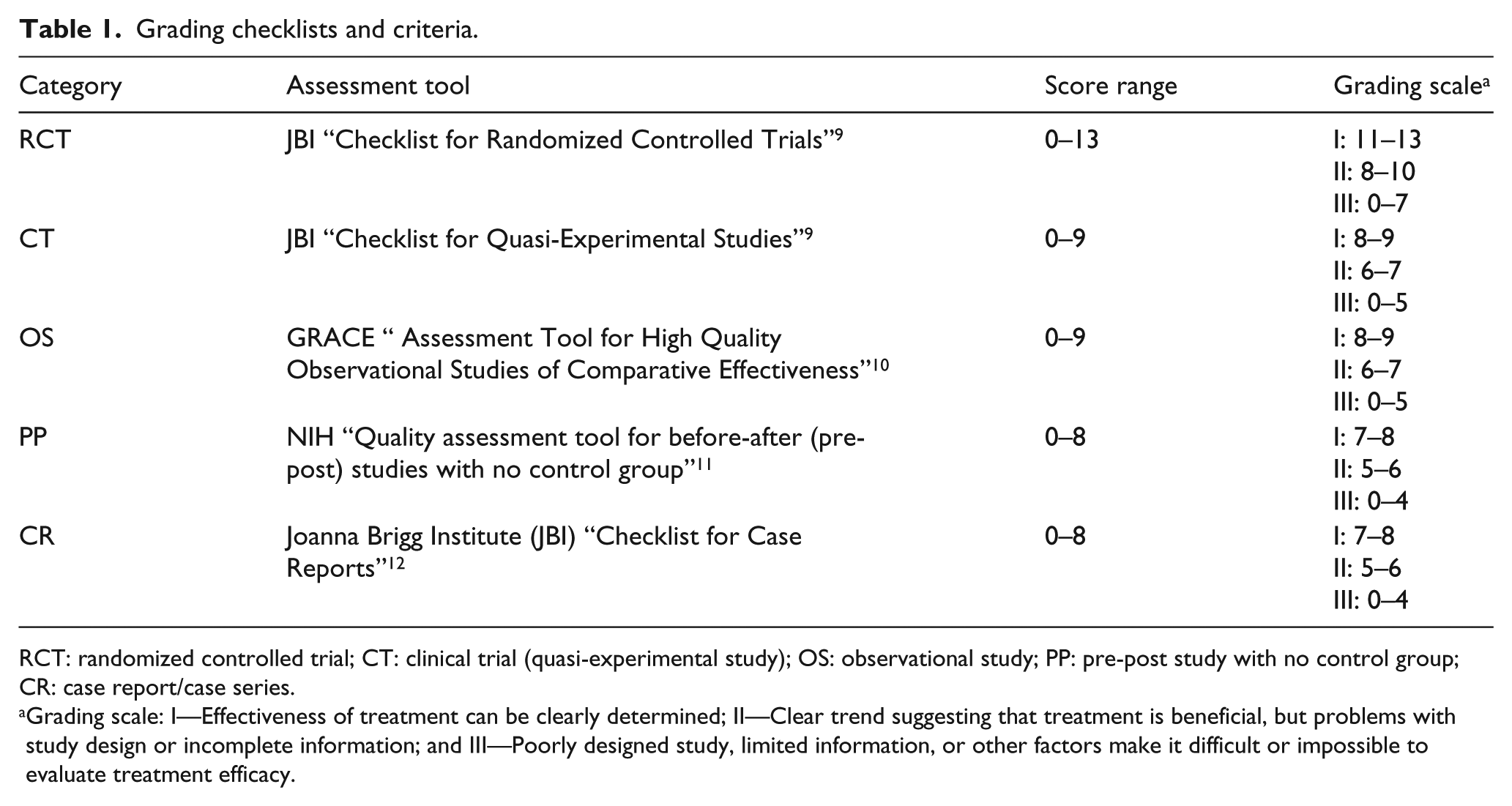
RCT: randomized controlled trial; CT: clinical trial (quasi-experimental study); OS: observational study; PP: pre-post study with no control group; CR: case report/case series.
Grading scale: I—Effectiveness of treatment can be clearly determined; II—Clear trend suggesting that treatment is beneficial, but problems with study design or incomplete information; and III—Poorly designed study, limited information, or other factors make it difficult or impossible to evaluate treatment efficacy.
Results
Overview
We identified 46 articles that met our search criteria, involving a total of 572 patients. Of the articles, 19 were CRs, involving a total of 26 patients. The remaining 27 articles (546 patients) ranged from letters to the editor describing a small group of patients treated with TPE to a large-scale review of 102 patients treated over a 15-year period at a single clinic in Italy. Out of the 572 patients, 455 received TPE. The rest were in control groups.
The diagnostic breakdown of the patients involved in these studies is as follows:
dcSSc: 294;
lcSSc: 90;
MCTD: 6.
Unclear/pre-dated the adoption of the 1980 ACR Systemic Sclerosis (Scleroderma) Classification Criteria: 182
Detailed summaries of randomized clinical trials, clinical trials (quasi-experimental studies), OS, single-group pre-post studies, and CRs are shown in Tables 2–6 and are discussed in the following. Tables are sorted by (1) TPE Only (yes/no), (2) Grade (I, II, and III), and (3) reverse chronological order (most recent first). In 25 out of the 46 studies, TPE was the only treatment intervention.
Randomized clinical trials.
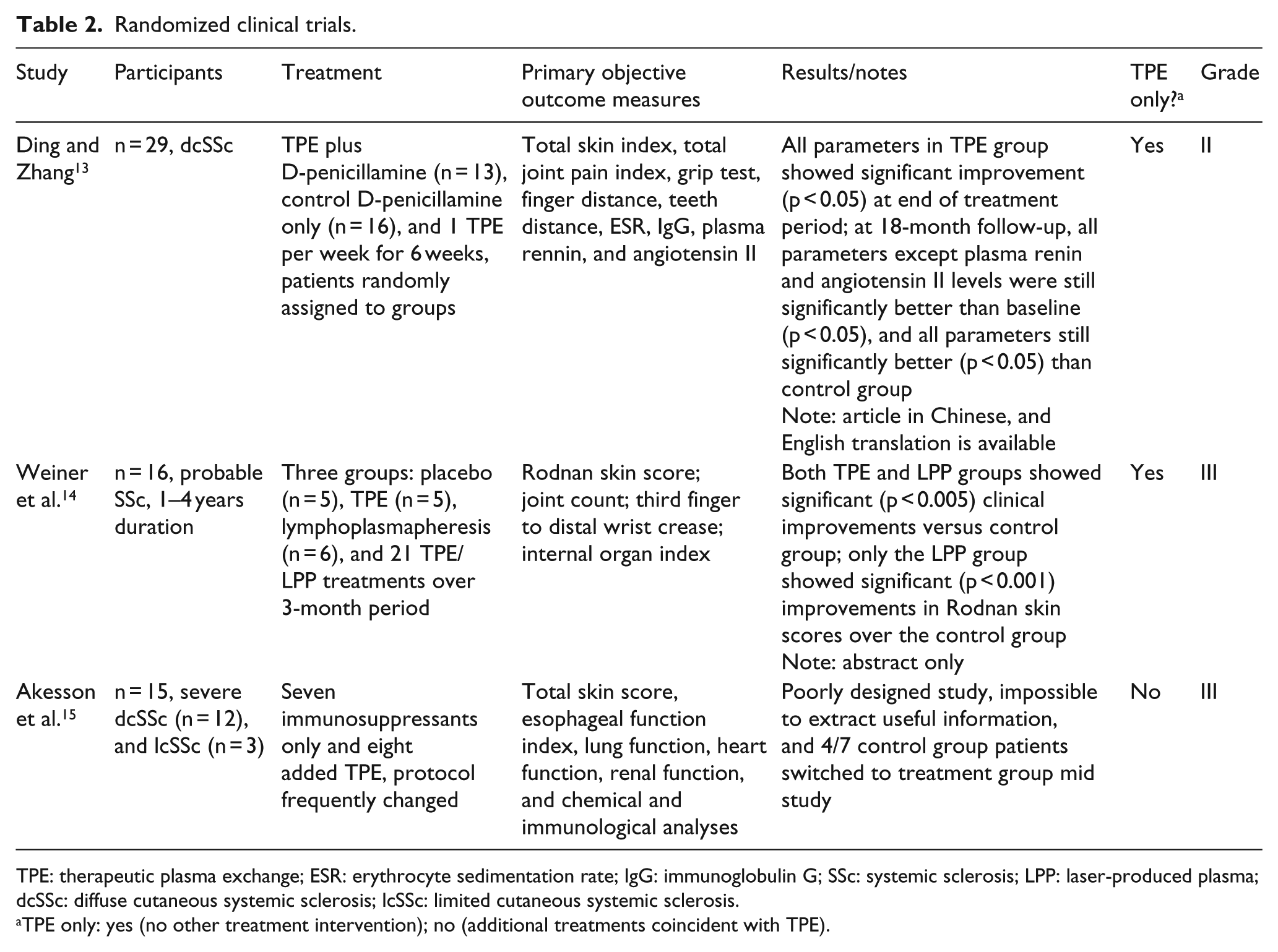
TPE: therapeutic plasma exchange; ESR: erythrocyte sedimentation rate; IgG: immunoglobulin G; SSc: systemic sclerosis; LPP: laser-produced plasma; dcSSc: diffuse cutaneous systemic sclerosis; lcSSc: limited cutaneous systemic sclerosis.
TPE only: yes (no other treatment intervention); no (additional treatments coincident with TPE).
Clinical trials (quasi-experimental studies).
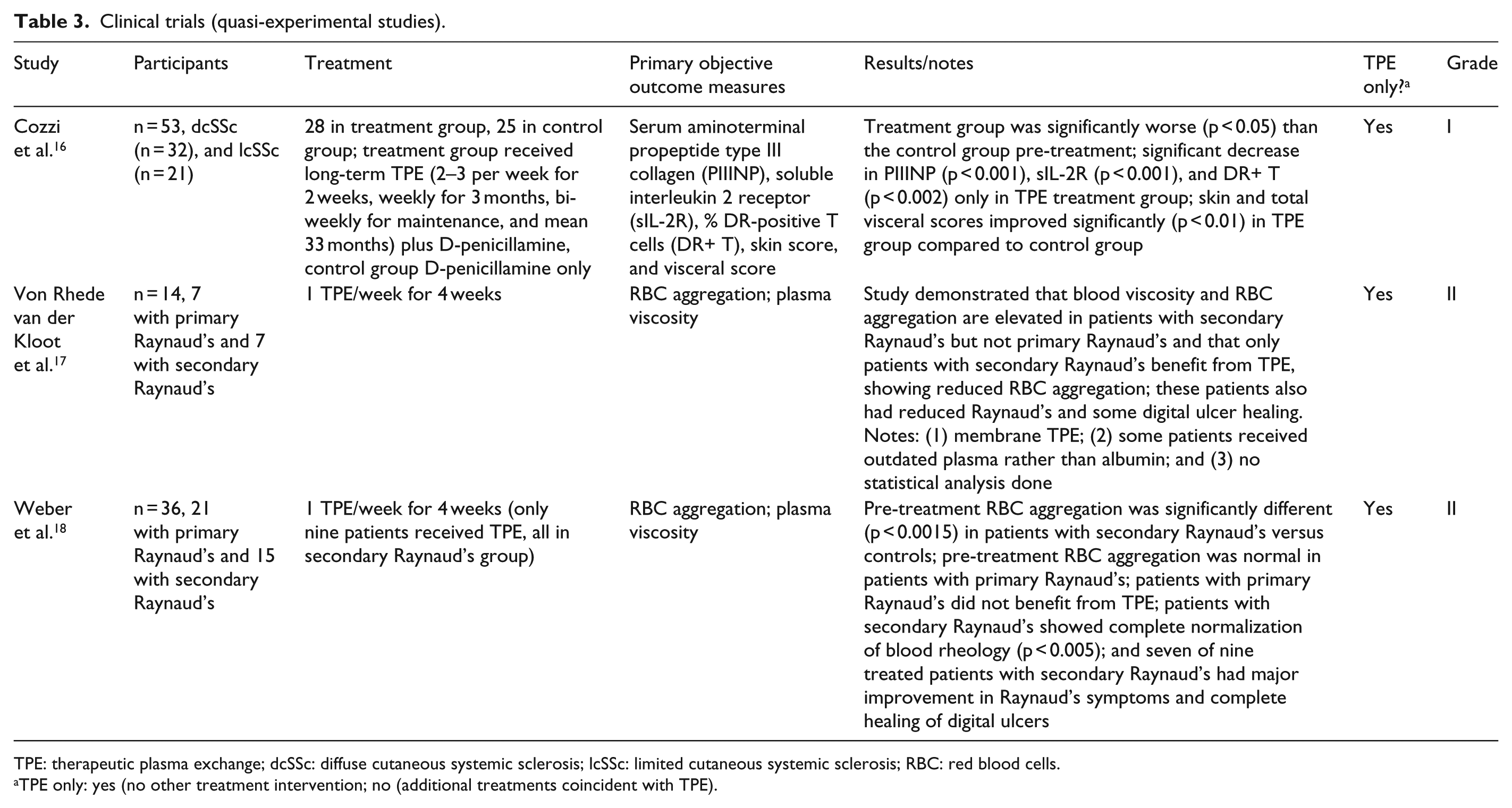
TPE: therapeutic plasma exchange; dcSSc: diffuse cutaneous systemic sclerosis; lcSSc: limited cutaneous systemic sclerosis; RBC: red blood cells.
TPE only: yes (no other treatment intervention; no (additional treatments coincident with TPE).
Observational studies.
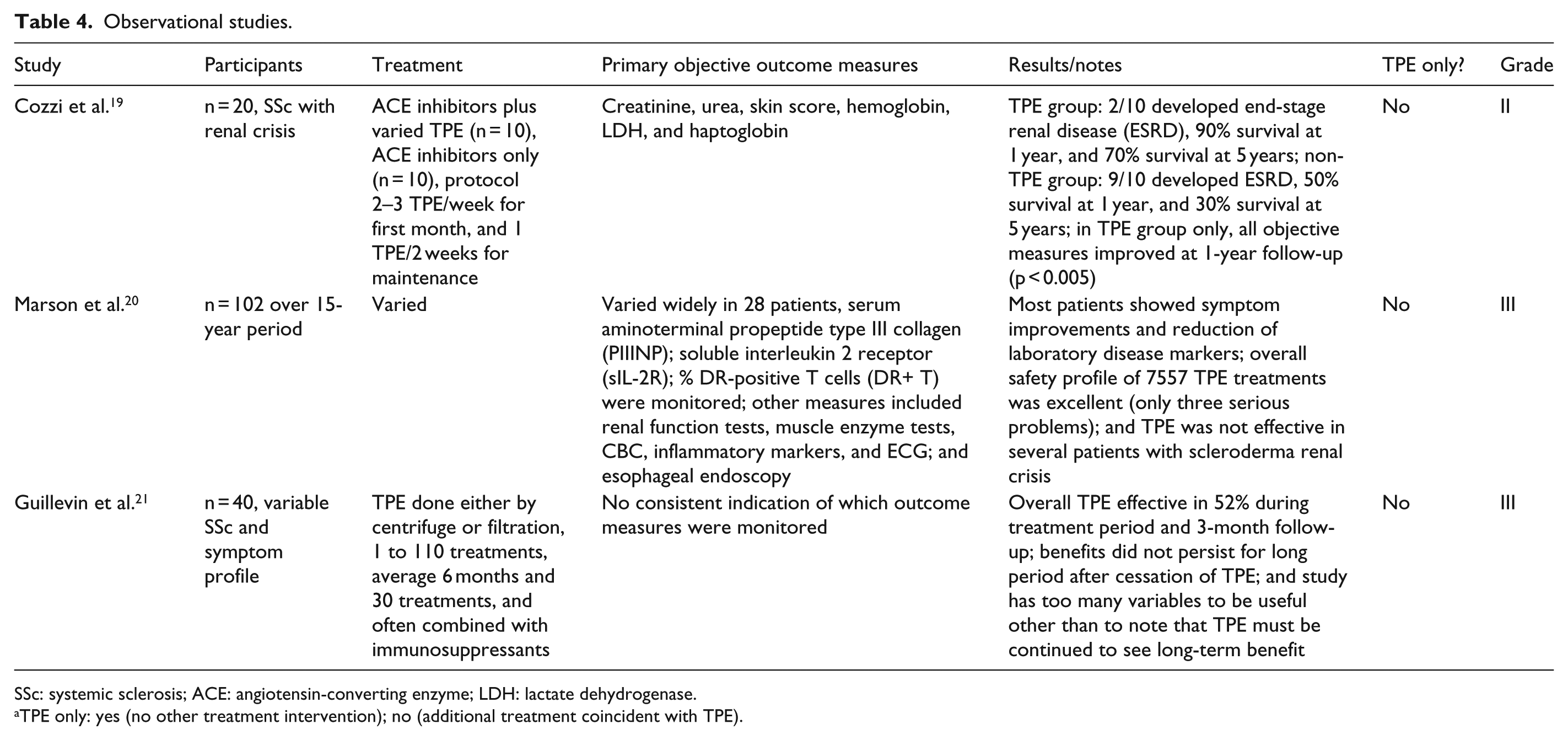
SSc: systemic sclerosis; ACE: angiotensin-converting enzyme; LDH: lactate dehydrogenase.
TPE only: yes (no other treatment intervention); no (additional treatment coincident with TPE).
Single-group pre–post studies with no control group.
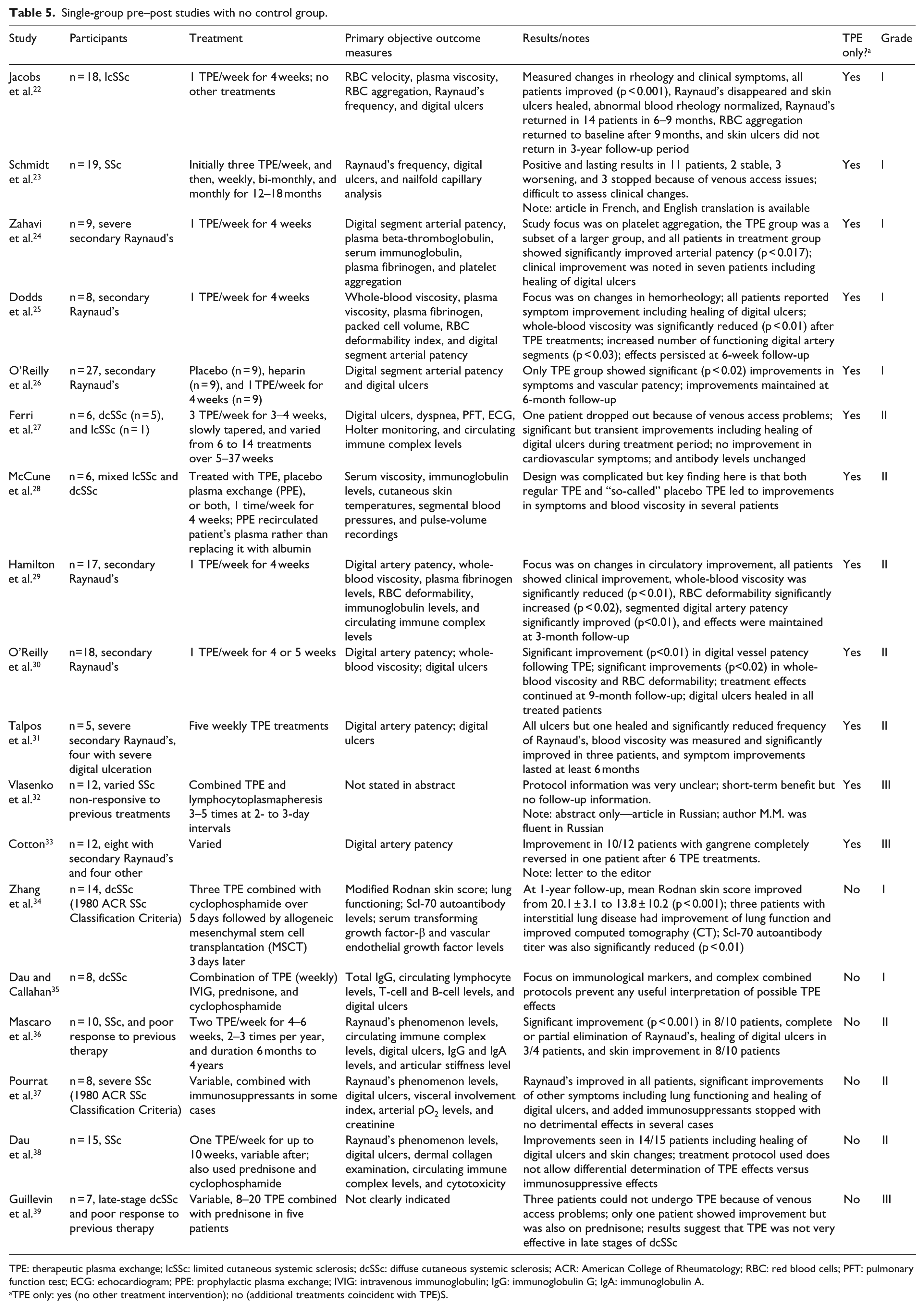
TPE: therapeutic plasma exchange; lcSSc: limited cutaneous systemic sclerosis; dcSSc: diffuse cutaneous systemic sclerosis; ACR: American College of Rheumatology; RBC: red blood cells; PFT: pulmonary function test; ECG: echocardiogram; PPE: prophylactic plasma exchange; IVIG: intravenous immunoglobulin; IgG: immunoglobulin G; IgA: immunoglobulin A.
TPE only: yes (no other treatment intervention); no (additional treatments coincident with TPE)S.
Case reports.
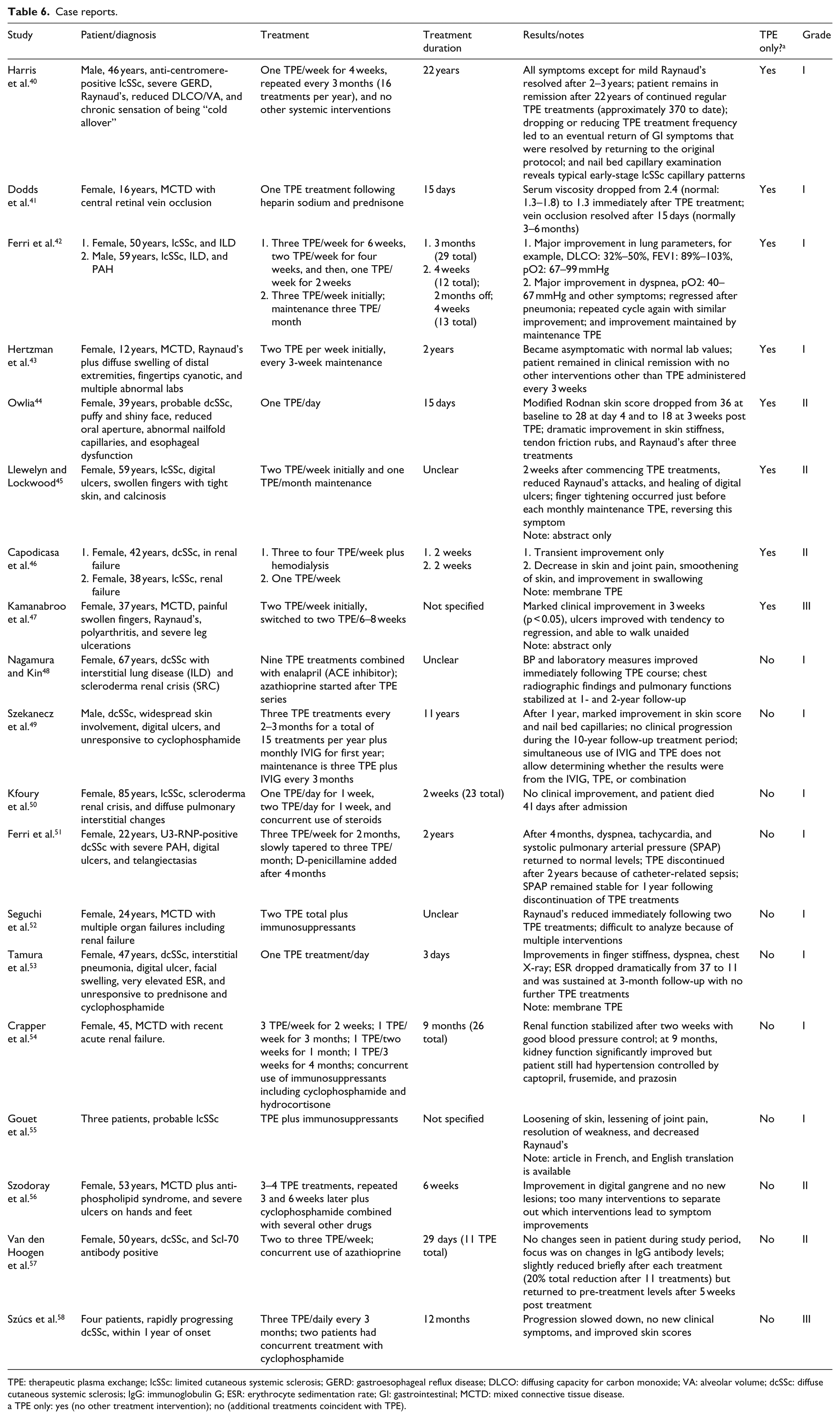
TPE: therapeutic plasma exchange; lcSSc: limited cutaneous systemic sclerosis; GERD: gastroesophageal reflux disease; DLCO: diffusing capacity for carbon monoxide; VA: alveolar volume; dcSSc: diffuse cutaneous systemic sclerosis; IgG: immunoglobulin G; ESR: erythrocyte sedimentation rate; GI: gastrointestinal; MCTD: mixed connective tissue disease.
TPE only: yes (no other treatment intervention); no (additional treatments coincident with TPE).
RCTs
Only three RCTs have ever been published where TPE was evaluated against a randomly assigned control group. While RCTs are normally considered the “gold standard” for clinical treatment research, all three of these studies provided limited information that can guide a modern clinician. Only two of these studies used TPE as the sole treatment intervention, and none of these studies were rated Grade I on our rating scale.
A 1986 study, 14 only available as a short abstract, compared TPE with a related procedure—lymphoplasmapheresis—as well as a non-treatment control group on a very small group of patients. A study done in 1988 15 compared the effects of TPE plus immunosuppressants against immunosuppressants alone. Unfortunately, this study suffered from numerous design issues, including using different types of plasma exchange (PE) equipment and frequent alterations of the protocols on an individual basis. A third study, 13 while well designed, was performed in China using procedures and equipment than are different from those used in other studies done in Europe or the United States.
Clinical trials (quasi-experimental studies)
Two studies done in 198517,18 reported hemorheological characteristics of patients with primary versus secondary Raynaud’s and the effects of four weekly TPE treatments on hemorheology and symptoms. Both studies demonstrated that blood rheology is essentially normal in patients with primary Raynaud’s but highly abnormal (increased whole-blood viscosity (WBV) and RBC aggregation) in patients with secondary Raynaud’s. TPE led to long-lasting improvements in hemorheology and symptoms, including reduced Raynaud’s attacks and healing of DUs, only in the secondary Raynaud’s group.
Even though a large 2001 study 16 was not a RCT, it actually provides strong data suggesting positive effects from TPE. Patients admitted into the TPE treatment group had more severe and/or rapidly progressing disease and at baseline were significantly worse (p < 0.05) than patients in the control group. However, improvements in laboratory markers and clinical scores were only seen in the (worse) TPE treatment group.
All three of the quasi-experimental studies used only TPE as a treatment intervention. One of these studies 16 received a Grade I rating.
OS
Only three long-term OS on the use of TPE have been published.19–21 Unfortunately, in all of these studies, TPE was used in conjunction with other treatments including immunosuppressants and ACE inhibitors, making it impossible to determine to what (if any) degree TPE contributed to any observed improvements in laboratory markers and clinical symptoms. None of these papers were rated Grade I because of these issues.
Single-group pre-post studies with no control group
Of the studies, 18 are best categorized as single-group pretest–posttest studies with no control group. In this type of study, a number of laboratory markers and clinical symptoms are assessed before treatment; patients then receive TPE (and sometimes other) treatments for a period of time, and the laboratory markers and clinical symptoms are re-assessed immediately following cessation of TPE and at follow-up intervals that can be anywhere from a few days or weeks to several years. Of these studies, 12 used TPE as the sole treatment intervention. Seven studies were rated Grade I, although two of these studies combined TPE with another treatment intervention. Potential issues with interpretation of pre-post studies are discussed later in this article.
CRs
In 12 of the 19 CRs included in this study,41,42,44,46,48,50,52–57 TPE was used to treat an acute or, in some cases, critical medical situation such as SRC. Typically, these studies look at the effects of TPE over a short period of time (a few weeks or months); TPE was discontinued once the acute situation resolved or improved. Three of the CRs are notable in that they reported on the results of long-term, regular TPE as a systemic treatment approach.40,43,49 Eight of the CRs used TPE as the sole treatment intervention. Of the CRs, 12 received a Grade I rating; however, only 4 of these used TPE as the sole treatment intervention.
Mixed connective tissue disease
Mixed connective tissue disease (MCTD) is a complex connective tissue disorder defined by coexisting and overlapping clinical features of SLE, SSc, and dermatomyositis/polymyositis. 59 It is considered to be a distinct disease by most authors. 60 Of the 19 CRs, 6 CRs41,43,47,52,54,56 were about patients diagnosed with MCTD. In all 6 cases, TPE was initiated because of an acute or crisis situation rather than as a general treatment. Improvements were reported in all of these cases, although multiple simultaneous interventions in 3 of these cases make it difficult to determine the role of TPE in observed improvements.
TPE and RP/DUs
Of the reviewed studies, 16 discussed improvements in RP and DUs following TPE treatments; 4 studies were confounded by simultaneous use of drug therapies and were excluded from further analysis. A commonly reported finding was that a single course of a small number of weekly TPE had major impact on both RP and DU as well as blood flow and microvascular patency. These findings are discussed later in this article.
Effects of long-term TPE
Only a small number of studies have examined the efficacy of long-term TPE on patients with SSc. The 2001 Cozzi study 16 compared pre- and post-TPE laboratory markers reflecting disease activity in a group of 28 Italian patients who received regular TPE combined with D-penicillamine over a 6-year period (mean 33 months) against a control group of 25 SSc patients who received D-penicillamine alone. Significant improvements in clinical scores and laboratory markers only occurred in the TPE treatment group even though at pre-treatment the TPE group had worse laboratory measures and clinical scores than the control group.
A second Italian study 20 summarized the results of long-term treatment of 97 SSc patients using TPE as an adjunct treatment in addition to D-penicillamine or an immunosuppressant. While the authors rated TPE efficacy as either “excellent” or “good” in 52.4% of the patients, the simultaneous use of adjunct treatments make it impossible to determine to what extent these positive effects are attributable to TPE.
Szekanecz et al. 49 followed a male patient with dcSSc for 11 years. The patient received a combination of regular TPE treatments combined with IVIG during the first year and was maintained on a reduced frequency of TPE/IVIG during the 10-year follow-up period. Unfortunately, because of the simultaneous use of TPE and IVIG, it is impossible to determine whether the observed improvements were from TPE, IVIG, or a synergistic combination of both.
Hertzman et al. 43 treated a 12-year-old patient diagnosed with mixed connective tissue disease (MCTD) with an initial series of 10 TPE treatments over a 5½ week period, resulting in significant improvement in nodular lesions and complete elimination of hand swelling. TPE was reduced to one TPE every 3 weeks, and the patient remained asymptomatic at 2-year follow-up with no other treatment intervention.
A 2017 very long-term (22-year) CR 40 documented the effects of regular TPE as the sole systemic intervention in a patient with rapidly progressing anti-centromere-positive lcSSc. TPE was administered in a pulsed protocol (one TPE treatment per week for 4 weeks and 8 weeks with no TPE, and the procedure was repeated). All symptoms (except for very mild residual Raynaud’s), including reduced diffusing capacity for carbon monoxide (DLCO)/valveolar volume (VA), disappeared after 2–3 years. The patient remains in excellent health with continued regular TPE treatments on the original pulsed protocol (approximately 370 to date); however, discontinuing or reducing TPE treatment frequency led to an eventual return of GI symptoms in two attempts.
TPE complications
Of the 46 papers, 11 reviewed for this article described complications directly related to the use of TPE. There were two main types of complications: (1) venous access issues and (2) short-term side effects directly associated with the TPE procedure. There were no reported fatalities associated with TPE, and short-term side effects were generally minor and usually did not prevent TPE from being completed. In one early study, 21 4 patients (out of 40) had allergic reactions. This primarily occurs only when fresh frozen plasma is used instead of sterilized albumin. In a small percentage of the cases, venous access difficulties prevented TPE from being performed using the preferred method of peripheral venous access, leading to cessation of TPE. In other cases, implanted central venous catheters were used for short-term TPE or an arteriovenous fistula was surgically created for long-term TPE.
TPE safety and venous access issues are discussed more fully later in this article. Table 7 lists all of the reported TPE-related complications in the reviewed articles.
TPE complications.
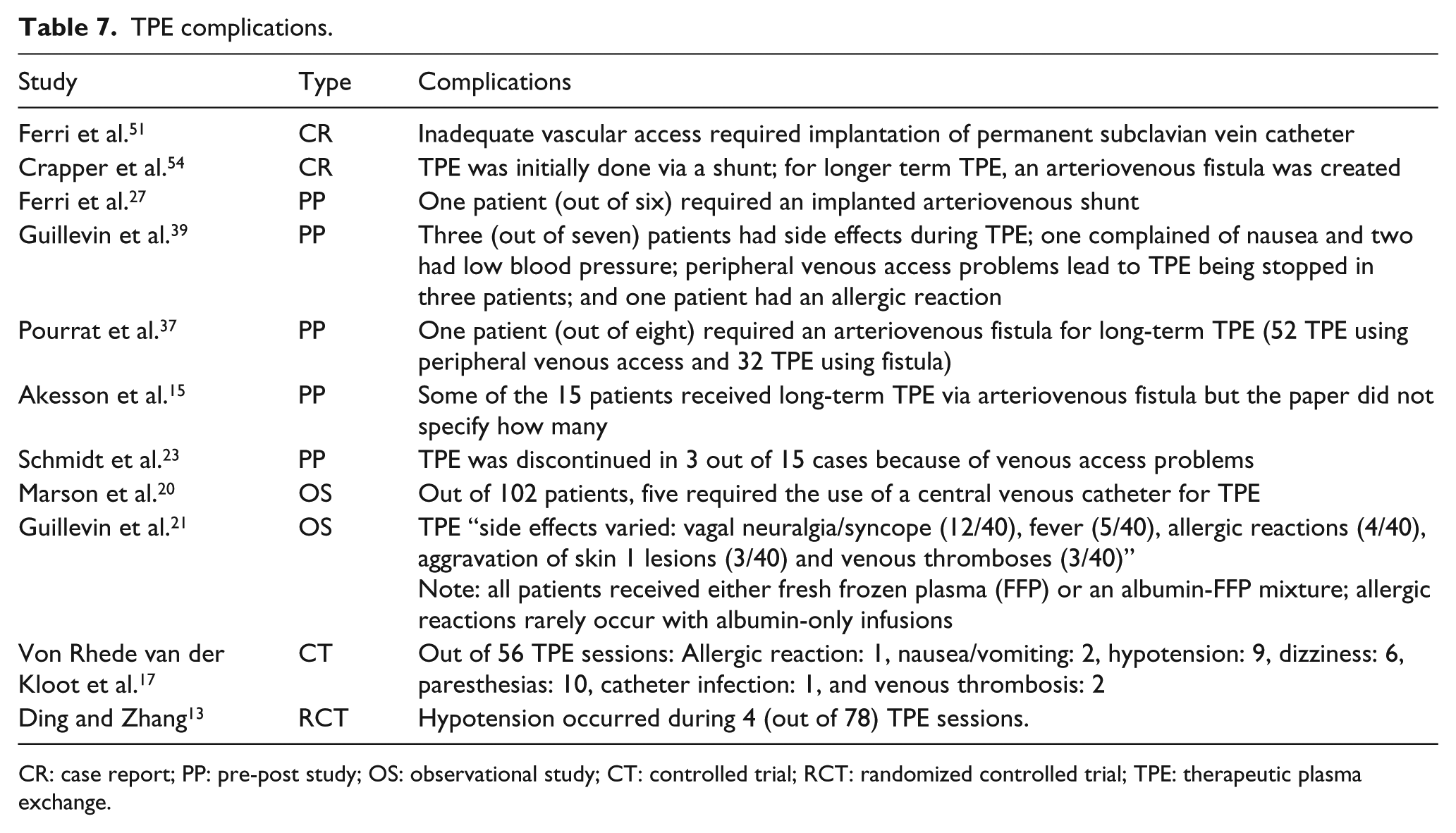
CR: case report; PP: pre-post study; OS: observational study; CT: controlled trial; RCT: randomized controlled trial; TPE: therapeutic plasma exchange.
Summary of results
In almost all studies, the majority of patients receiving TPE showed improvements in both symptoms and laboratory markers, whether in short-term treatment of crisis situations or from long-term administration of regular TPE.
Many patients experienced significant improvement in Raynaud’s symptoms and demonstrated initial healing of digital ulceration after just three to four weekly treatments.
While the effects of even a few TPE treatments often lasted for several months, only continued long-term treatments resulted in stabilization of symptoms or, in one recent CR, sustained remission over a 22-year period.
Venous access problems occurred in a minority of patients receiving long-term TPE, leading to cessation of TPE treatments in some cases and switching to central venous access in other cases.
TPE was very well tolerated by almost all patients. Adverse events were rare and, in almost all cases, mild, with no reported deaths.
Discussion
While TPE was introduced in the 1950s, it was not until 1976, when the Haemonetics Model 30 Apheresis system became commercially available, that clinicians began to try TPE as a potential treatment for more than 100 diseases.3,61 Early successes of TPE, such as the unprecedented reversal of clinical symptoms in patients with Waldenstrom macroglobulinemia and as a mainline treatment for Goodpasture syndrome and myasthenia gravis, have stood the test of time and clinical research. In contrast, using TPE as a treatment for diseases such as rheumatoid arthritis (RA) and SLE nephritis has been shown to be ineffective in clinical trials despite early reports of successes with individual patients. Currently, TPE for treating SSc is classified as a Category III treatment by the ASFA. 7 Category III treatments are defined as “optimum role of apheresis therapy is not established; decision-making should be individualized.”
While there have been (at least) 46 published studies on the use of TPE as a treatment for SSc, none of the published studies reviewed for this article meet the rigor of a well-designed, RCT. Of the studies, 21 used more than one simultaneous treatment intervention, making it impossible to isolate out the effects of TPE versus other co-treatments. Out of the 25 studies that used only TPE as a systemic treatment intervention, only 10 of these studies received our highest rating on our level of evidence grading scale. (Notably, 10 other studies where TPE was used in conjunction with at least one other simultaneous treatment intervention demonstrated clear treatment benefit and received a Grade I rating.) It is clear that additional, well-designed studies are needed to evaluate fully the efficacy of TPE treatments in different SSc patient populations. However, the consistency of the findings showing significant clinical benefit from TPE treatments with very low risk suggests that TPE may be an appropriate treatment option to consider even as these additional studies are being done.
Issues with interpretation of study results
Single-group pre-post studies with no control group
While the “gold standard” for clinical treatment research is RCTs, studies such as pre-post studies can be very valuable and, if done correctly, can strongly suggest a causal relationship between a treatment and any changes in symptoms, 62 especially for SSc treatment studies. Unlike diseases such as multiple sclerosis or lupus, SSc is a disease which is steadily progressive and does not go into remission without an intervention. Because of this, any objective changes in laboratory markers or symptoms following the introduction of TPE are likely to be a result of the intervention as long as there are no confounding co-treatments.
Skin scores as outcome measures
The Modified Rodnan skin score (MRSS) is a commonly used objective measure of skin thickness that is frequently used as one of the primary outcome measures in clinical trials of SSc treatments. About two-thirds of dcSSc patients show significant spontaneous reduction in skin thickness starting a year or two after initial diagnosis for reasons that are not fully understood. It is important to note, however, that there are no corresponding spontaneous improvements in internal disease markers. 63 This means that if a study includes early-stage dcSSc patients, improvements in MRSSs following TPE (or any other intervention) cannot necessarily be attributed to the treatment(s) used in the study.
When does TPE fail to work in patients with SSc?
Guillevin et al. 39 tried TPE treatments in seven patients with severe diffuse SSc after failure of other treatments. Disease duration at time of initial TPE averaged 8 years. In three patients, TPE treatments had to be stopped because of venous access problems. In the remaining four patients, only one showed benefit: improvement of articular and cutaneous symptoms. This suggests that TPE may not be effective in late stages of dcSSc.
Capodicasa et al. 46 tried TPE in two patients in SRC. While brief improvement was seen in one patient, the authors concluded that TPE would need to be started earlier to be potentially effective. In contrast to all other reports reviewed in this article, this study used membrane TPE instead of centrifugal TPE. Also, ACE inhibitors are now employed as the treatment of choice for treating SRC.
Kfoury et al. 50 tried intensive TPE on an 85-year-old patient admitted because of SRC with the rare complication of thrombotic thrombocytopenic purpura. Intense TPE starting with 1 week of daily TPE treatments increasing to twice a day for an additional week had no effect, and the patient died shortly after cessation of TPE and all medications secondary to pulmonary and cardiac conditions related to SRC.
While TPE was not effective in all patients in studies with overall positive outcomes, few data were presented about patients who failed to respond to TPE treatments. Nevertheless, most authors clearly felt that TPE would be most effective if started early in the disease process.
TPE and mixed connective tissue disease
No clinical trial or other large-scale study of TPE as a potential treatment for MCTD has been done to date. While most of the six MCTD CRs reviewed for this article were focused on the use of short-term TPE to deal with an acute issue, such as renal failure or central retinal vein occlusion, one paper 43 followed a 12-year-old MCTD patient who went into remission after 5½ weeks of TPE (10 treatments in total) and remained in remission with regular maintenance TPE at the 2-year follow-up. While MCTD has overlapping symptoms of SLE, it is interesting to note that TPE was not effective in patients with SLE in a short-term RCT. 64
TPE and RP/DUs
Treatment of RP and DU in SSc is challenging and, in some cases, inadequate to prevent progression to gangrene and eventual digit amputation. One of the more surprising findings in 12 of the papers reviewed here17,22,24–28,30,31,33,44,47 was the fact that three or four TPE weekly treatments often led to complete cessation of Raynaud’s attacks and healing of even long-standing DU. These effects were long-lasting, with RP not returning for 6 months or longer, and in one study, 22 patients had no return of DU during at 3-year follow up.
Standard treatments for RP and DU in SSc are focused on improving distal blood flow by either increasing vascular dilation or reducing vasoconstriction or vasospasm. Since TPE treatments are not known to directly increase vasodilation or reduce vasoconstriction or vasospastic activity, these results raise the possibility that an entirely different mechanism of action may be involved in the observed improvements in RP and DU healing following TPE.
Why does TPE show positive results?
Reduction of potential circulating pathogenic factors
Many antibody-mediated diseases are due to IgG antibodies (~150 kDa). Blood plasma and extravascular extracellular fluid within the body contain about 45% and 55% of total IgG, respectively. 65 Thus, the single blood volume TPE treatment could theoretically remove ~30% of circulating IgG. Due to extravascular to intravascular circulation during a TPE treatment, the actual removed amounts of IgG are somewhat higher than expected. 66 Nevertheless, within 2 days, plasma IgG levels return to about 70% of pre-TPE levels. 67
The long-lasting effects of TPE in SSc patients suggest that the mechanism of action may be independent of the reduction of circulating antibodies. Specifically, several studies have documented 6-month (or longer) beneficial effects following a single series of four TPE/week treatments. These favorable effects on both laboratory markers and clinical symptoms cannot be easily explained by short-lived reductions in circulating antibodies.13,22,29 Also, when comparing the effects of standard PE with “placebo plasma exchange (PPE),” where patient’s cellular blood elements were re-mixed with the patient’s own separated plasma (instead of replacing the plasma with 4%–5% sterilized albumin), McCune et al. 28 noted that “There appears to be no difference between plasma and placebo exchange as measured in the vascular laboratory.”
Is blood rheology the key?
Over the past 42 years, many published papers have documented that blood rheology is abnormal in patients with SSc. Individual papers have commented on or measured differing aspects of this abnormal rheology, including elevated whole-blood viscosity (WBV), increased plasma viscosity (PV), decreased RBC deformability, and abnormal RBC aggregation.18,22,25,29,31,68–79 It is important to note that abnormal rheology is not uncommon in autoimmune diseases. It has been documented in RA 80 and SLE. 81 However, TPE does not improve clinical symptoms in RA 82 or SLE, 64 suggesting a different mechanism of action in RA and SLE pathogenesis as compared to SSc pathogenesis.
The potential role of RBC aggregation in SSc pathogenesis
In 1979, Kahaleh et al. 83 noted that “Many, if not all, of the manifestations of scleroderma can be explained on the basis of functional and structural vascular compromise after repeated vascular insults, subsequent healing of vascular walls with proliferative vascular response, and luminal narrowing.” This is still a commonly accepted viewpoint. 84 Several different potential mechanisms for this initial endothelial damage have been proposed, including viral triggers, cytotoxic T-cell involvement, and anti-endothelial antibodies. 85 However, none of these proposed endothelial damage mechanisms have been consistently demonstrated to be universal in SSc. For example, anti-endothelial antibodies are not universally found in patients with SSc and are also found in other autoimmune diseases, including SLE, RA, and Sjögren’s syndrome. 86
Hypothesis
Abnormally clumped red blood cells may be a significant component of the etiopathogenic processes in SSc, potentially contributing to the vascular damage cited above (see Figure 1).
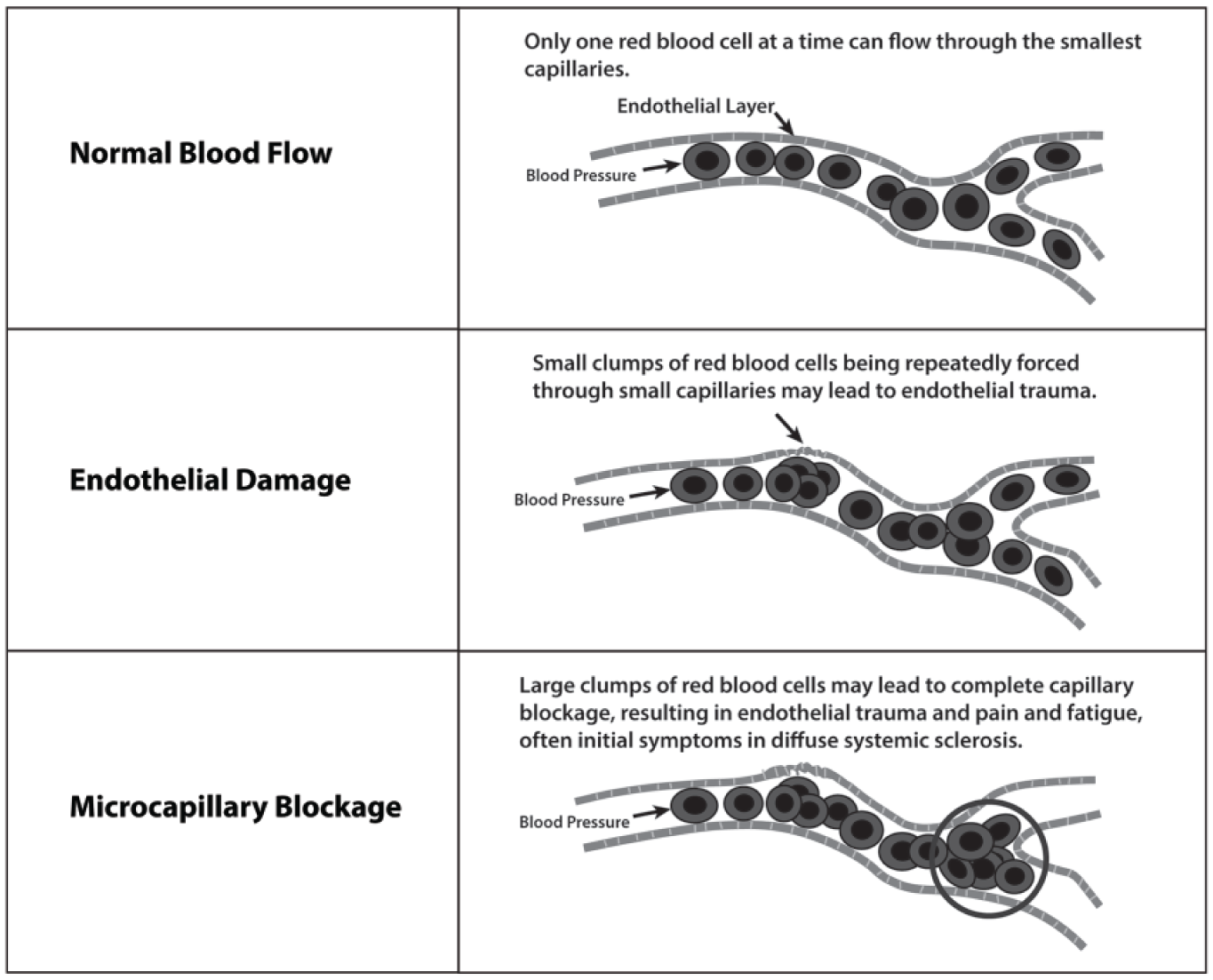
Potential Impact of RBC Aggregation on Endothelial Integrity.
A full examination of the research on abnormal blood rheology in SSc and the potential role of RBC aggregation in SSc pathogenesis is beyond the scope of this review paper, but merits future study.
Issues/concerns about the use of TPE for treating SSc
Safety and complications
While TPE is generally not used for treating SSc currently (at least in the United States), it is a widely used procedure for many autoimmune disorders, for example, myasthenia gravis, Guillain-Barré, chronic demyelinating polyneuropathy, and Goodpasture’s syndrome. This broad usage of TPE prompted several large-scale studies to assess TPE safety and complication rates.
Cid et al. 87 reviewed the efficacy and safety of TPE in 317 patients and 2730 procedures over an 11-year period. Observed adverse events occurred in only 3% of procedures. In all cases, the adverse events were mild and transient, and patients were able to complete the scheduled TPE treatment. Similarly, in a study of more than 20,000 therapeutic apheresis procedures performed in Sweden, 88 mild adverse events requiring no intervention occurred 1.5% of the time, moderate events not requiring cessation of treatment occurred 2.8% of the time, and severe events requiring cessation of treatment occurred 0.8% of the time. There were no fatalities.
The most severe complications in TPE occur with fresh frozen plasma as the replacement fluid. Almost all studies of TPE for treating SSc used sterilized 5% albumin, which has a much better safety profile because of substantially reduced risk of anaphylactic-type events.
The most common short-term problem with TPE is hypocalcemia, usually presenting as mild paresthesias or perioral tingling from the use of citrate as an anti-coagulant. Prophylactic use of oral calcium supplements is usually adequate to prevent or minimize TPE-associated hypocalcemia. Some patients may experience mild hypotension, muscle cramps, or mild headaches from hypovolemia especially with lower concentrations of albumin than the recommended 5% solution.
Vascular access
The safest way to perform TPE is using regular peripheral venous access. Venous access problems were discussed in several of the reviewed articles and were often the reason for discontinuation of TPE. While the exact percentage of patients who would require alternatives to peripheral venous access for long-term TPE is not clear, the data indicate that most patients can undergo long-term TPE using normal peripheral access. Khatri and Kramer, 89 summarizing the results from more than 60,000 TPE treatments, indicate that peripheral venous access is successful in about 75% of the procedures performed at their clinic. However, two new venous access techniques are now available that should increase the likelihood of long-term peripheral venous access: (1) vein illumination technology such as VeinViewer™ and AccuVein™ and (2) ultrasonic-guided peripheral venous cannulation. 90
For patients who cannot undergo normal peripheral venous access, there are a number of alternatives that are available. Central catheters are not a good option for most patients for long-term TPE because of the significant infection risk. Alternatives such as surgically created fistulas or implantable vascular-access devices (ports), such as PowerPorts™ or Vortex™, may be better options for very long-term use of TPE if peripheral venous access is not an option.
Cost
Winters et al. 91 did an analysis of TPE cost and determined that each treatment cost a little under US$1200 when TPE was performed using albumin. Average Medicare reimbursement rates (2015) are about US$1140 plus the cost of albumin, which varies depending on the size of the patient. Several studies suggest that between 12 and 18 treatments per year may be sufficient to control SSc symptoms. For instance, the 16 TPE treatment/year protocol discussed in Harris et al. 40 translates into an annual cost of about US$20,000 per year.
A recent study of the annual cost of modern biologic drugs now commonly used to treat RA and other autoimmune conditions 92 indicated that the lowest price biologic—Humira (adalimumab)—was about US$21,000 per year. Other biologics were somewhat higher. This suggests that annual costs for long-term TPE, while significant, are similar to standard pharmacological options used for other autoimmune diseases.
IVIG, which is being increasingly tried as a treatment for SSc93,94 is much more expensive than TPE. A typical treatment regimen in these early studies used a dosing of 2 g/kg monthly. Using data from Winters et al., 91 this works out to more than US$10,000 per month for a typical 70-kg patient, that is, approximately US$120,000 per year.
Summary and conclusion
While the preponderance of evidence reviewed in this article suggests that long-term TPE may offer a low-risk and cost-effective way to control and, in some cases, reverse SSc symptoms and signs, the overall level of evidence is not high. Only 25 of the 46 reviewed studies used TPE as the sole systemic intervention, and only 10 of these studies received our top grade: “Effectiveness of treatment can be clearly determined.” Of these 10 studies, 5 were pre-post studies with no control group; 4 were CRs; and 1 was a clinical trial (quasi-experimental study).
However, in contrast to current immunosuppressive treatments that carry significant risk, long-term TPE appears to be safe, well-tolerated, and associated with only very few, mostly minor side effects. While TPE is not an inexpensive procedure, annual costs are similar to modern pharmaceuticals commonly used to treat SSc and other autoimmune diseases.
The published research that we have reviewed for this study suggests that TPE provides clinical benefit to a wide variety of SSc patients; however, without a clear understanding of exactly how TPE works on a molecular level, we currently have no way of knowing which patients are appropriate candidates for TPE and what protocol should be followed to produce the best possible outcomes. For example, it is entirely possible that patients with slower progressing lcSSc might benefit from a reduced frequency of TPE than patients with faster progressing dcSSc.
The current ASFA guidelines suggest that clinicians should make individual decisions on the suitability of TPE as a treatment for their patients with SSc. If clinicians do decide to try TPE on an individual basis, it is important that they also try to extract as much useful research data as possible from any such individual trials. We have prepared a document that may be a useful starting point for clinicians who are considering trying TPE. This document is available directly from the corresponding author.
Proposed research
Out of the 46 studies reviewed for this article, 33 were done prior to 2000. The equipment now used for TPE has fewer side effects than earlier generation systems. In addition, newer techniques and equipment are now available that can greatly increase success rates for long-term use of TPE. What is lacking is a well-designed clinical trial of TPE using modern equipment and improved venous access techniques. Any future clinical trial should use tools like nailfold capillaroscopy to directly monitor vascular changes. We believe that the studies reviewed here provide strong support for conducting such a trial.
It is also important to better understand the mechanisms of action in TPE. If we can fully understand how TPE works, then we may be able to develop new, non-invasive treatment approaches that provide the same benefit without requiring TPE equipment that may not be readily available to all patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.